Calcium homeostasis and the parathyroid gland
1/38
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
39 Terms
Give an overview of the skeleton’s functions
Mechanical: support and muscle attachments
Protective: for vital organs and marrow
Metabolic: ion homeostasis, especially calcium and phosphate
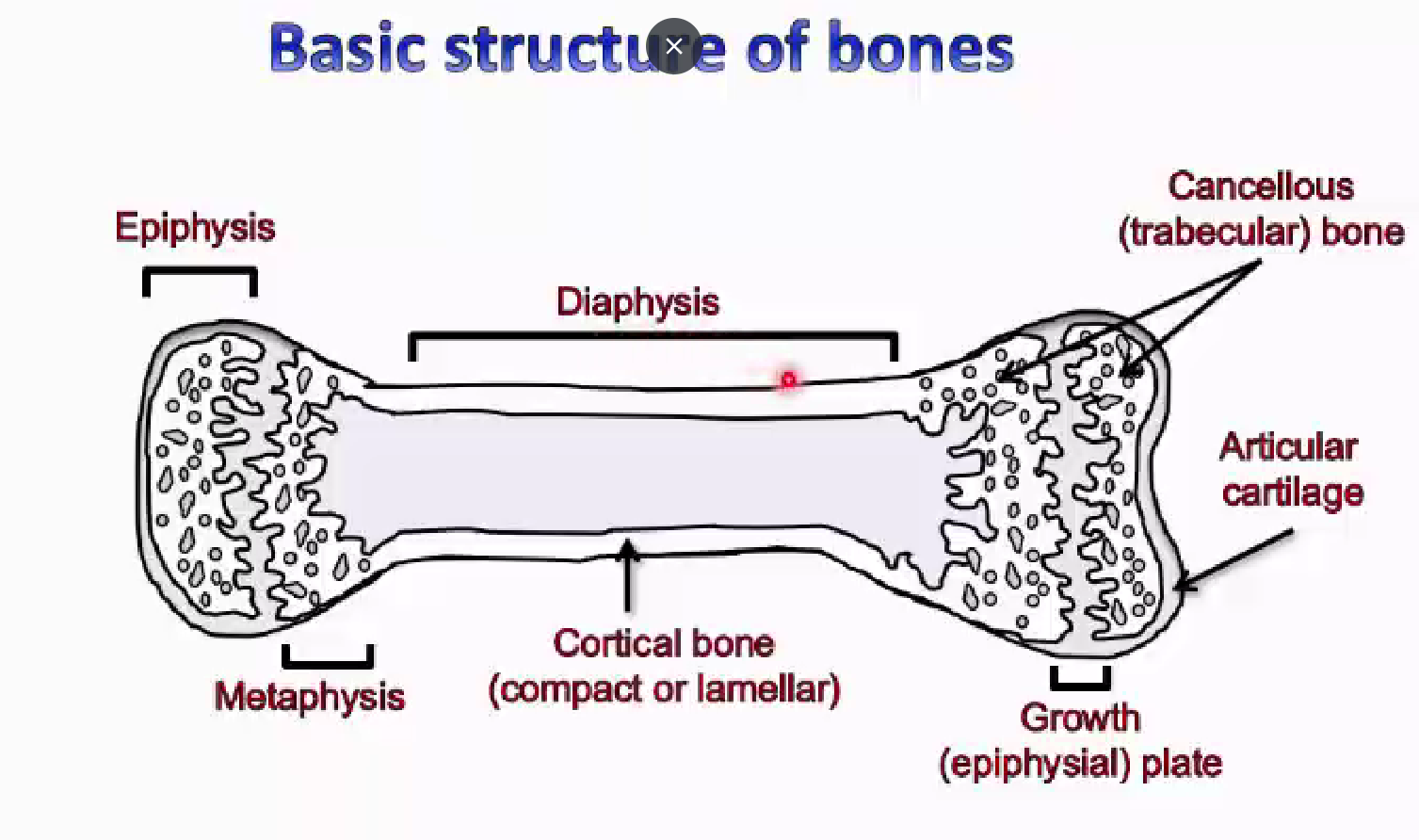
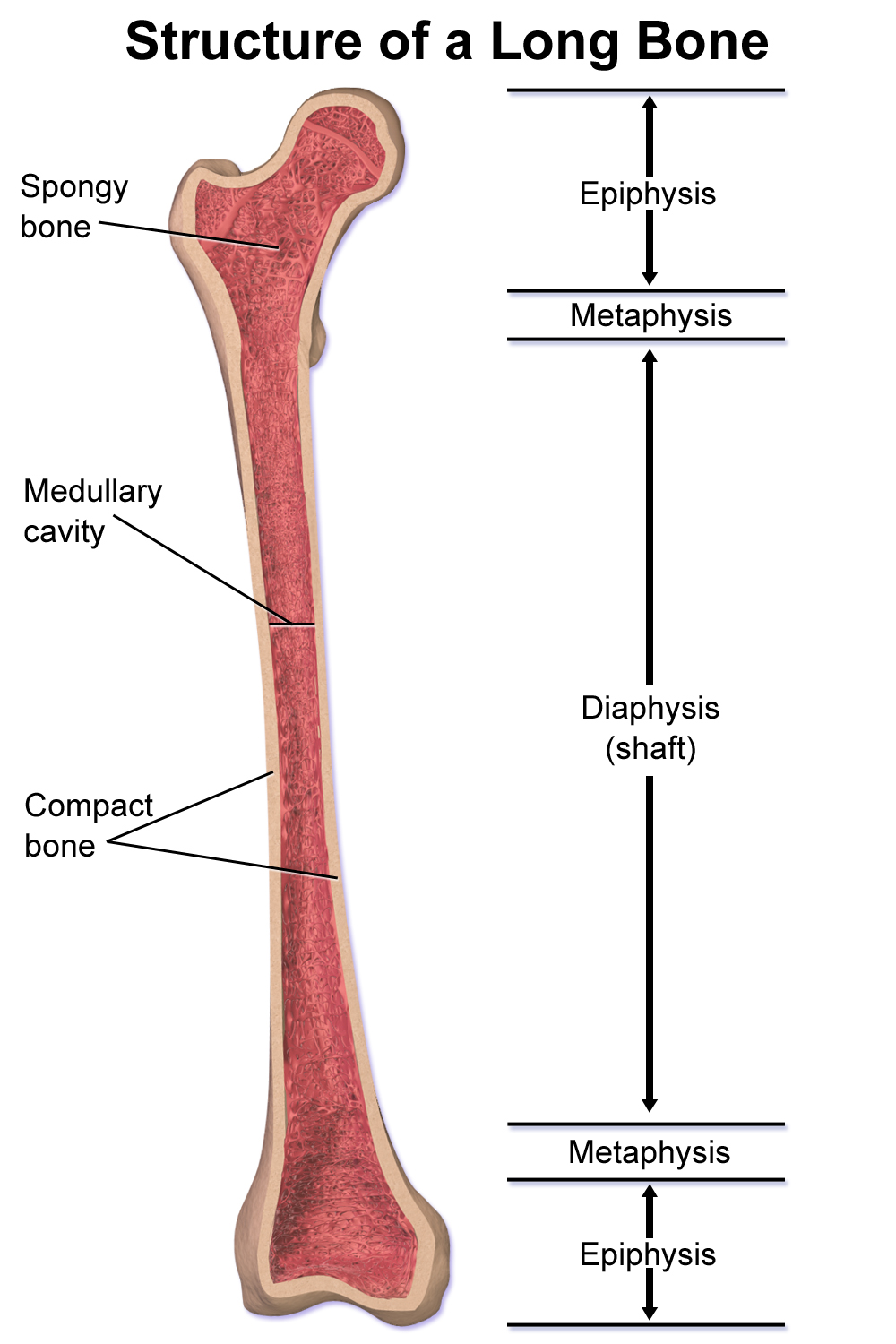
Epiphysis
The ends of a bone, the round parts
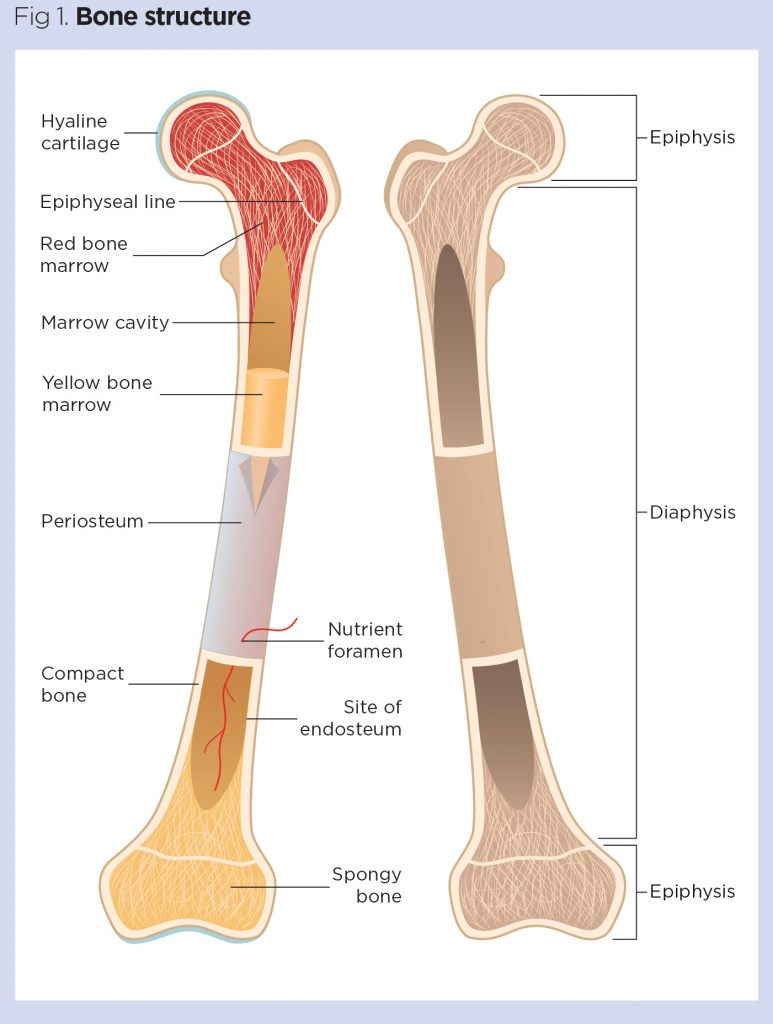
Metaphysis
The middle bit between the epiphysis and the diaphysis (shaft)
What is cancellous bone
Trabecular bone
Includes the epiphysis and metaphysis
Lateral loading, strength under pressure. honeycomb like.
large surface area- much easier to access calcium and phosphate than cortical bone
individually weak, collectively strong
diaphysis
the length of the bone (shaft) before the round bits (in between the epiphysises)
made up of cortical bone (compact or lamellar)
strong under compression, basic protection
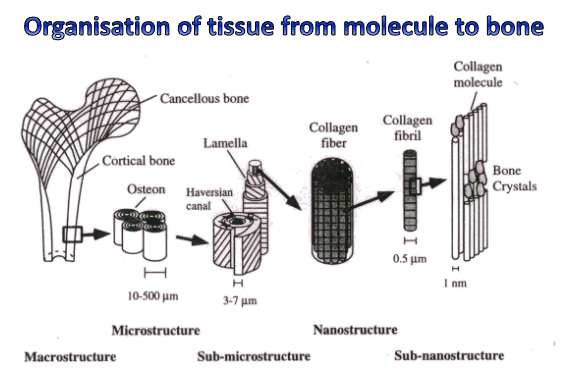
what is bone made of?
specialised connective tissues
extracellular matrix which can calcify
collagen fibres with a preferential orientation (follow specific orientation structure)
some non-collagenous proteins essential to bone function (regulators)
calcification occurs with the formation of hydroxyapatite crystals- calcium phosphate crystals incorporate into bone to give it its structure
how does bone remodelling work
in trabecular bone- cycles of remodelling
constantly eating away and replacing- catabolic clearance, anabolic laying down of new bone
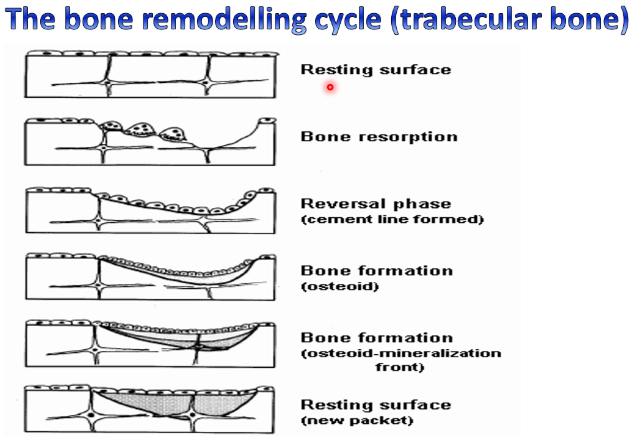
osteoclasts
responsible for bone resorption (munch through the bone, bone clearing)
found in contact with calcified bone surface in lacunae
multinucleated
produce acids to resorb mineral and enzymes to resorb matrix (markers)
attach to bone with integrins
osteoblasts
Bone formation, lay down collagen (aid calcification + produce matrix constituents)
created when collagen structure calcifies over time and some of the osteoblasts left behind become osteoblasts
bone lining cells
initiate bone remodelling
osteocytes
mechanosensing, orchestrates microfracture repair (sense damage)
created when the collagen calcifies and some of the osteoblasts left behind become them
communicate with osteoblasts to fix damage
significance of calcium
essential for:
nerve innervation of muscle + muscle contraction
bone mineral deposition
blood clotting
nerve impulse transmission
hypocalcemia symptoms
muscle spasms
cramps
seizures
paresthesia (pins and needles/tingling/numbness)
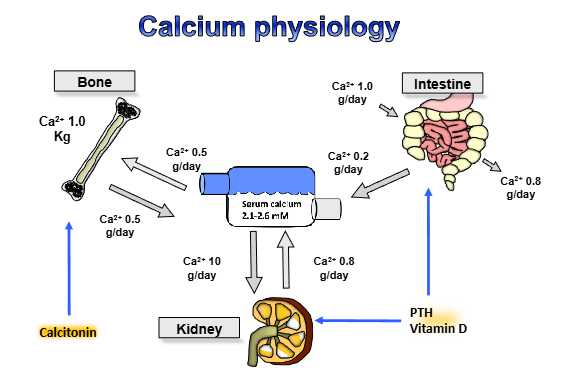
Outline the calcium cycle
about a gram a day is taken in, about 0.8 grams are lost
0.2 grams go to serum
within the serum, can turn into bone ( ½ a gram liberated from bone a day, ½ a gram taken up- homeostasis)
lose 1 gram/day in urine, then 0.8 grams reabsorbed from kidneys
what do the parathyroid glands do? (generally)
regulate calcium and phosphate levels
secrete PTH (parathyroid hormone) in response to low calcium and high phosphate
have g-protein coupled receptors
what does PTH do?
increases calcium reabsorption in renal distal tubule
increases intestinal calcium absorption via action of vitamin D
increases calcium release from bone (stimulates osteoclast activity, enhancing bone resorption)
decrease phosphate reabsorption
outline the structure of PTH
84 amino acids but biological activity in the first 34 amino acids
gets cleaved into smaller peptides
has an n-terminal and a c-terminal
assayed (measured) by two site assay
PTH receptor expressed primarily in bone, kidney, cartilage
outline PTH function in the kidney
stimulates production of the active form of vitamin D- 125D3
increases distal tubular reabsorption of calcium + inhibits PO4 reabsorption
outline the negative feedback mechanisms involved in PTH
PTH transcription (mRNA production) inhibited by 1,25D3 (vitamin D)
PTH translation (mRNA —> protein synthesis) inhibited by increased serum calcium
once calcium released, should feedback to parathyroid to stop production of PTH
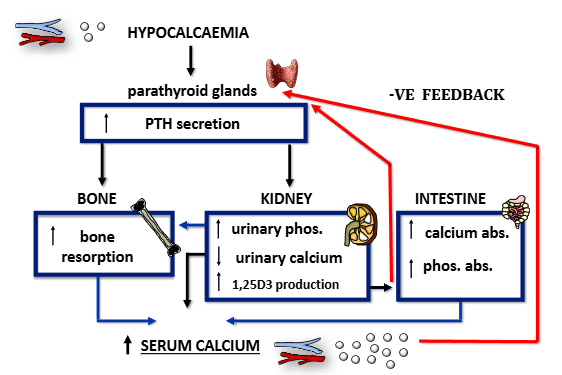
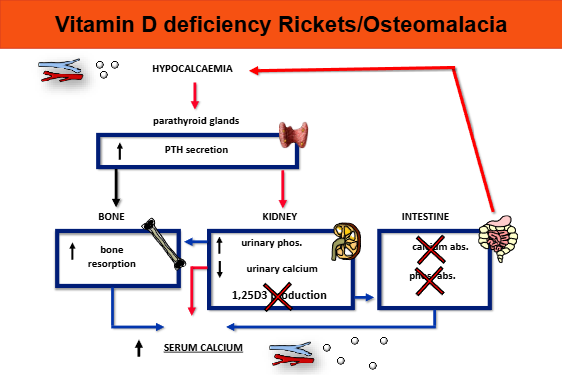
How does PTH work to rectify hypocalcaemia?
parathyroid glands increase PTH secretion
increased bone resorption
increase in urinary phosphate, decrease in urinary calcium, increase in 1,25D3 production
increase in calcium absorption in intestine, increase in phosphate absorption
serum calcium raises, feeds back to parathyroid glands to stop production of PTH
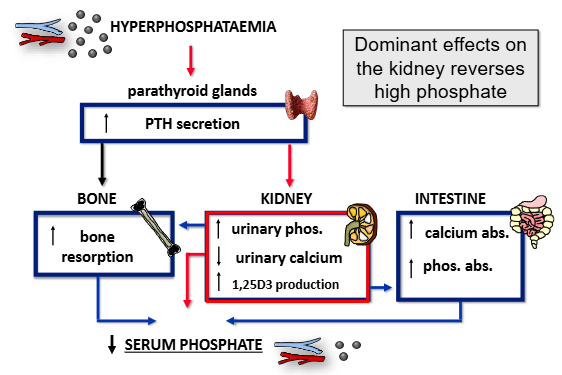
how does PTH work to rectify hyperphosphataemia?
same as hypocalcaemia, but pay attention to the kidneys- increase in urinary phosphate, decrease in urinary calcium, increase in 1,25D3 production
calcium supersedes this system
functions of vitamin D
increases calcium and phosphate absorption in intestines
important in osteoblast differentiation/osteoclastogenesis to increase bone remodeling
deficiency in vitamin D or calcium —> osteomalacia (low mineral content)
technically a steroid hormone
how do we get vitamin D3?
UV radiation and diet (eggs, fish)
UV radiation converts 7-dehydrocholesterol in skin —> vitamin D3
outline the process through which vitamin D turns into 1,25D3
vitamin D3 from light + diet go to blood, then liver
liver converts to 25-hydroxyvitamin D3 (inactive)
in the kidneys, D3 + PTH = 1,25D3
outline calcitonin
produced by thyroid c-cells (parafollicular)
released in hypercalcaemia, inhibits bone resorption by acting on osteoclasts (osteoclasts have calcitonin receptor, calcitonin turns them off)
not essential to life
‘i’m going to protect bone’ hormone
outline the production of calcitonin
example of alternative splicing (look at you knowing what that means :)
two calcitonin gene products from a single gene and primary RNA transcript- calcitonin and calcitonin gene-related peptide
outline how the parathyroid rectifies serum hypercalcaemia
reduction in PTH secretion as instructed by parathyroid glands
calcitonin acts on bone to reduce bone resorption
reduction in urinary phosphate and 1,25D3 production, increase in urinary calcium
reduction in calcium and phosphate absorption in the intestines
list the metabolic bone diseases (that you need to know)
hyperparathyroidism
rickets/osteomalacia
renal osteodystrophy
osteoporosis
what is primary hyperparathyroidism?
making parathyroid hormone regardless of feedback = raised serum PTH
caused by a parathyroid tumor (usually benign adenoma)
cause hypercalcaemia and low serum phosphate, loss of negative feedback from hypercalcaemia
treatment = surgery
clinical features of hyperparathyroidism
Symptoms caused by electrolyte imbalance
Neuro: lethargy and confusion
Renal: thirst/polyuria, renal stones (caused by lots of calcium going through kidneys)
GI: constipation, pancreatitis
Rheumatic: joint pain, fracture
Neuropsychiatric: depression
Cardiac: hypertension
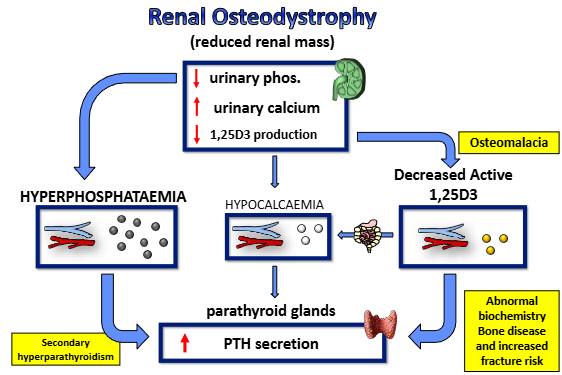
outline secondary hyperparathyroidism
caused by renal disease
increased phosphate, decreased activation of vitamin D- kidneys can’t absorb Ca2+ or produce VD
absorbing less calcium in digestive tract, parathyroid gland compensates by producting more PTH
loss in bone content as calcium lost in urine + not absorbed in diet
treatment with phosphate binders or vitamin D analogues
outline tertiary hyperparathyroidism
long-standing secondary HPT —> irreversible parathyroid hyperplasia
usually seen when renal disease corrected
elevated PTH over extended period —> enlarged parathyroid
use of endocrine glands heavily over time = build up, disuse of endocrine glands over time = atrophy
outline vitamin D/calcium deficiency
—> osteomalacia (low mineral content) due to lack of mineralisation of osteoid
intestinal calcium absorption capacity decreases with age + vitamin D levels are low in the elderly
softer bone, more likely to break or pseudofracture
low vitamin D —> low intestinal calcium absorption
outline osteomalacia
Rickets when affects growing skeleton- osteomalacia when affects adult skeleton
bones unduly soft, loss of calcium from bones
rickets: osteoid at growth plate is weak —> bow legs, growth plate expands to compensate (swollen koints)
as it grows longer, without calcification, compression from body weight = bendy bones
osteomalacia —> bone pain and pseudofractures
causes of rickets and osteomalacia
dietary/lack of sunlight
inherited (rarely)
calcium + vitamin D supplementation highly effective in reducing fractures, their actions reduce PTH levels and prevent osteoclast mediated bone resorption
outline renal osteodystrophy
reduced renal mass- ‘knackered kidney’
reduction in urinary phosphate, increase in urinary calcium, reduction in 1,25D3 production (unable to secrete more phosphate, therefore higher serum levels)
leads to hyperphosphataemia, hypocalcaemia and decreased active 1,25D3
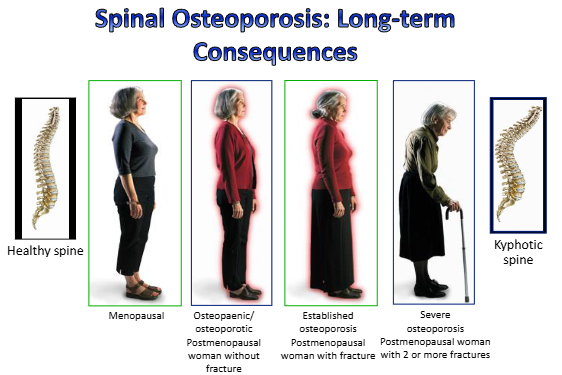
outline osteoporosis
low bone mass, micro-architectural deterioration of bone tissue
increase in bone fragility + susceptibility to fracture
less resistant to compressive force, decrease in bone porosity
osteoporosis
loss of bone mass/density = both mineral and osteoid decreased. normal bone but less of it, increased fracture risk
osteoporosis of aging- males + females have gradual decline in bone density from early adult peak
postmenopausal osteoporosis = rapid decline in female bone density following decline in estrogen at menopause
estrogen deficiency increases bone remodelling rate + degree of bone resorption
treatment = hormone replacement, biphosphonates
draw a bone + its components