Week 8 Cardiac muscle - BIPN100
1/45
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
46 Terms
tetanus toxin
• Binds to the presynaptic membrane of the motor neuron and travels retrogradely to the spinal cord!
• Blocks Inhibitory interneuron NT release
• Leads to continuous muscle spasm
botulinum toxin
• Inhibit AcH release at the NMJ via damage to the SNARE protein-
• Vesicles don’t fuse to release AcH
cardiac muscle
striated but smaller, branched, uninucleat. cells joined by intercalated disks. involuntary
the heart, cardiac muscle
1. arrangement of ventricular muscle allows contraction to squeeze the blood upward from the apex of the heart.
2. smaller fibers than skeletal muscles. Typically a single nucleus.
3. Intercalated disks: desmosomes to physically connect adjacent cells; gap junctions to electrically connect adjacent cells
4. T-tubules are larger than in skeletal muscle and branch within the myocardial cell.
5. SR is less elaborate than in skeletal muscle
6. More mitochondria! Mitochondria occupy ~30% of the cell volume!
what are top and bottom of heart called:
top - base
bottom - apex
the heart is encased within a membrane fluid-fileld sac:
the pericardium
myocardium:
the muscular middle layer of the wall of the heart and has excitable tissue and the conducting system
what occupies the bulk of the heart?
ventricles
what attaches to the base of the heart?
arteries and veins
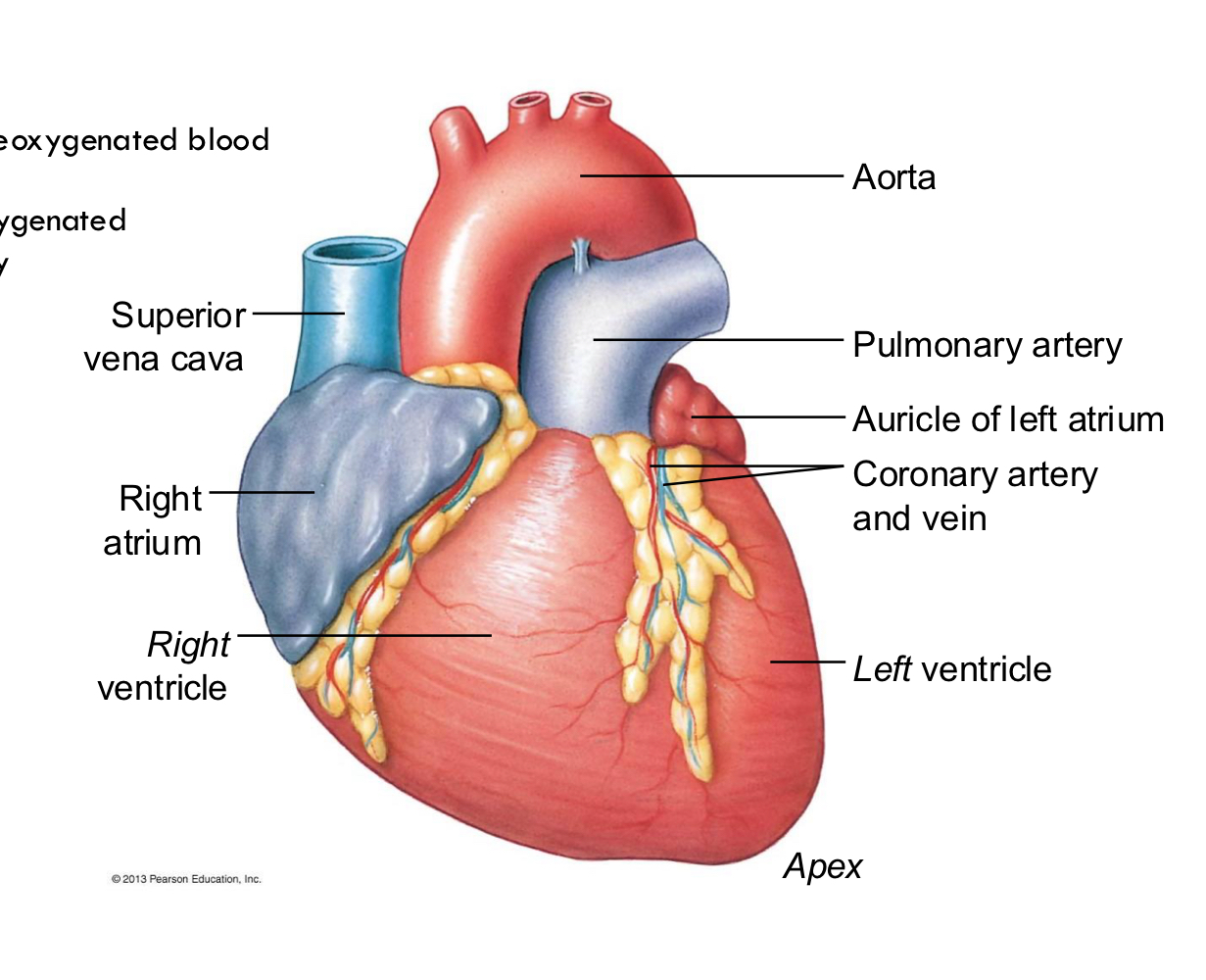
veins:
carry deoxygenated blood into the heart
aorta:
pumps oxygenated blood out to body
pulmonary system:
pulmonary artery: carries deoxygenated blood from heart to lungs
pulmonary blood: oxygenated blood from lungs back to heart
intercalated disks:
Join the muscle cells together, gap junctions
contractile cells:
In the walls of myocardium of atrium and ventricles,
responsible for generating force. Contraction increases pressure in the
chamber
do cardiac cells need motor neuron input?
no they are self-excitatory
autorhythmic cells:
self generate action potentials and serves as a pacemaker
sinoatrial (SA) node:
initiates the cardiac cycle by generating an action potential (pacemaker)
electrical conduction in myocardial cells
SA node- main pacemaking center Autorhythmic cells spontaneously fire APs. Depolarizations of the autorhythmic cells spread through gap junctions to adjacent contractile cells.
cardiac refractory period:
much longer refractory period prevents tetanus in your heart
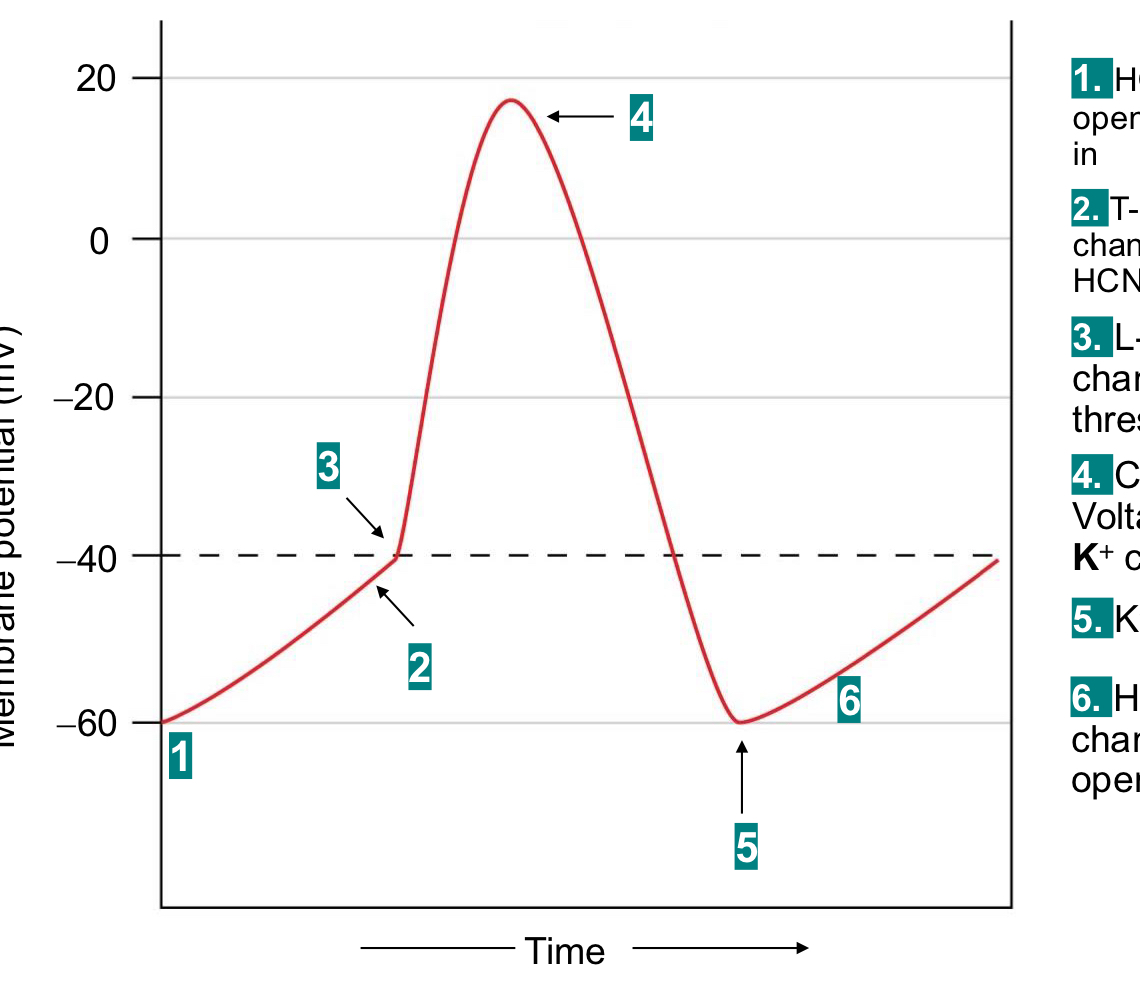
pacemaker action potential
The pacemaker potential gradually becomes less negative until it reaches threshold, triggering an AP
The pacemaker cells in the SA node will typically fire about 100 times per minute
heart rate directly related to the slope of the pacemaker potential
ion channels that drive a pacemaker potential:
1) HCN channels open, allow Na+ in
2) t-type Ca2+ chennels open, HCN channels close
3) L-type Ca2+ channels open (L = lasting/large curent)
as the membrane depolarizes, HCN channels start to close
4) Ca2+ channels close, voltage gated K+ channels open
5) K+ channels lcose
6) HCN channels open
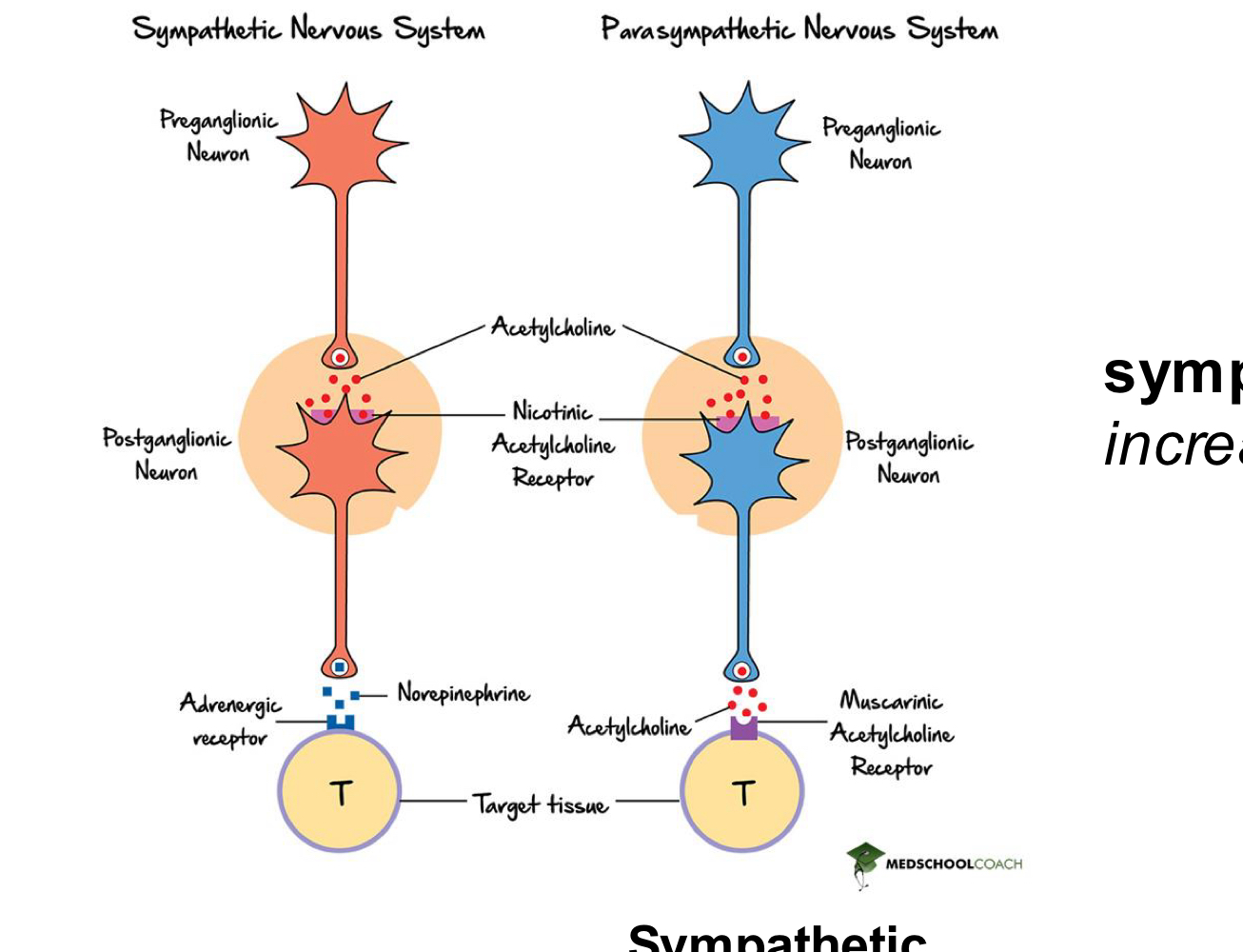
parasympathetic activity:
decreases heart rate
from ACh and mAChR Gi on heart
sympathetic activity
increase heart rate
bc of beta adrenergic cells and norepinephrine Gs
autorhythmic cells:
spontaneously fire APs
depolarizations of the autorhythmic cells spread through gap junctions to adjacent contractile cells
intercalated disk anatomy/function
desmosomes (major cell adhesion junctions)transfer force from cell to cell
gap junctions allow electrical signals to pass rapidly from cell to cell.
gap junctions in heart =
intercalated disks maybe idk
action potential of a cardiac contractile cell steps:
0. Na+ channels open
1. Na+ channels inactivate/close, fast K+ channels open (brief!) then close
2. Ca2+ channels open – and stay open (long!); fast K+ channels close
3. Ca2+ channels close; slow K+ channels open
4. Resting potential
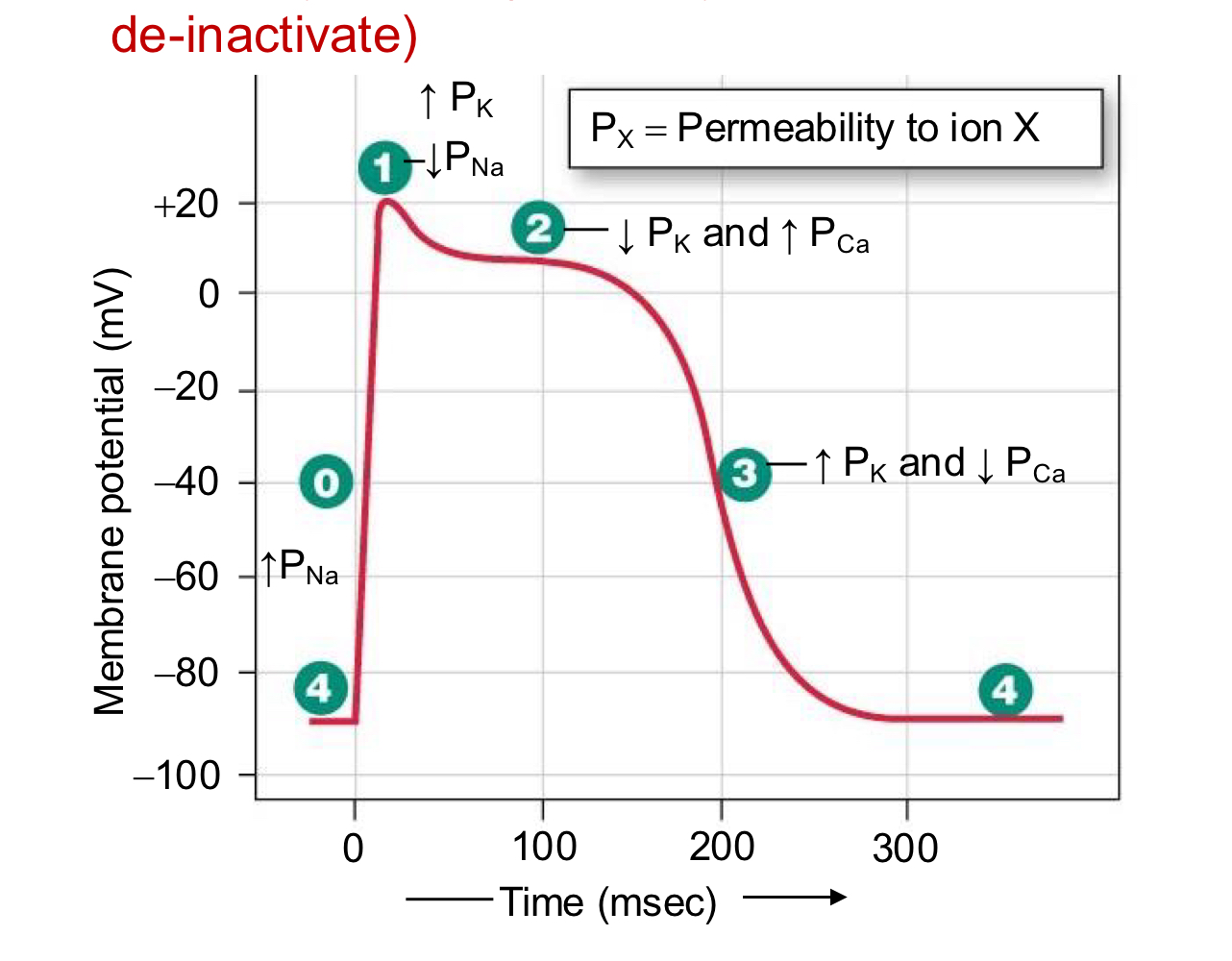
more about APs of cardiac contractile cells:
plateau potential: NO summation of twitches due to long absolute refractory period (drive by Ca2+, which does not allow the Na+ channels to de-inactivate)
rise is due to voltage gated Na+ channels
plateau driven by Ca2+
repolarization due to K+
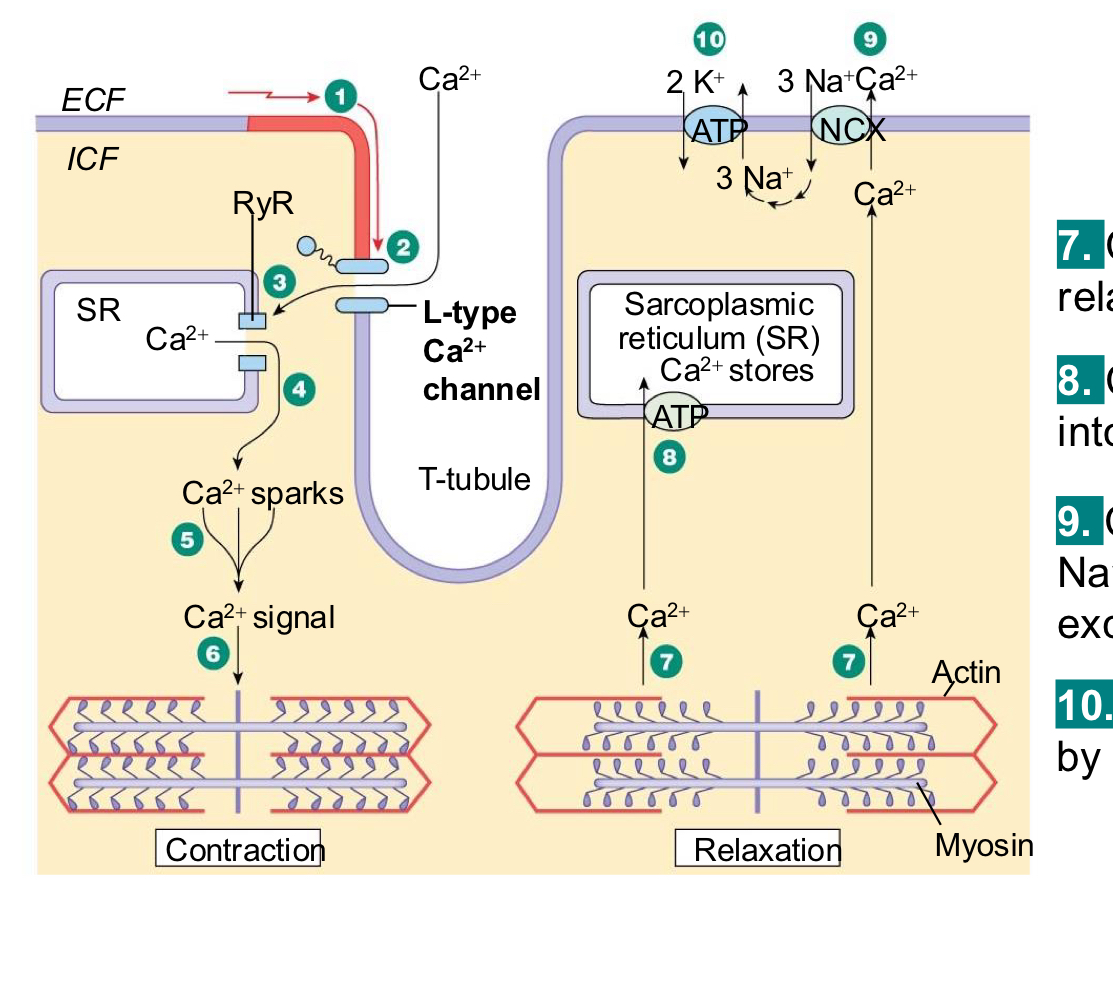
excitatory-contractile coupling in cardiac muscle
1. AP propagates via gap junction VGCCs (L-type)open. Ca2+ enters for plateau phase.
3. Ca2+ gates RyR and induces Ca2+ release
4. Ca2+ release from SR causes spark
5. Summed Ca2+ sparks create a Ca2+ signal.
6. Ca2+ binds troponin… initiates contraction
7. Ca2+ unbinds troponin, relaxation occurs
8. Ca2+ pumped back into the SR for storage.
9. Ca2+ is exchanged with Na+ by the NCX (Ca2+ Na+ exchange) antiporter.
10. Na+ gradient maintained by the Na+ -K+ -ATPase
cardiac muscle AP stuff
refractory period is almost as long as the entire muscle twitch
long refractory period (due to Na+ channels being inactivated) in a cardiac muscle prevents tetanus. NO SUMMATION!
skeletal muscle
refractory period is very short compared to the development of tension
repetitive stimulation will summate
electrical conduction in myocardial cells:
SA nodes to gap junction to contractile cells
autorhythmic cells spontaneously fire APs
depolarization of the autorhythmic cells spread through gap junctions to adjacent contractile cells
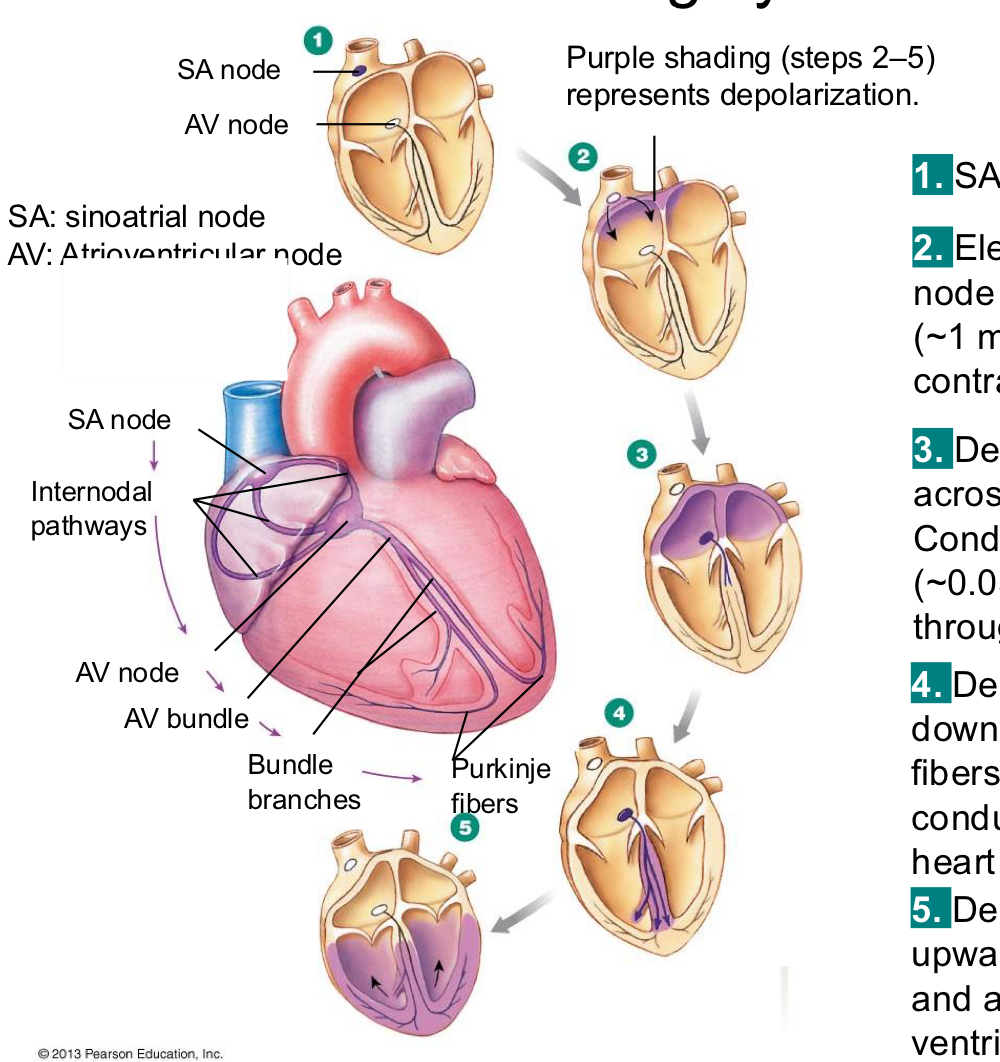
the conducting system of the heart:
1) SA node depolarizes
2) electrical activity goes rapidly to AV node via internodal pathways and tells the atria to contract
3) depolarization spreads more slowly across atria. Conduction slows through AV node. wave of contraction through the atria
4) depolarization moves from AV node down the septum through the purkinje fibers rapidly through ventricular conducting system to the apex of the heart
5) depolarization wave spreads upward from the apex and a wave of contraction from the ventricle
the conducting system of the heart
change in speed allows the muscle contraction to catch up
all autorhythmic but entrained by the SA node at the top
if you ablate the SA node, the intranodal pathways are still pacemaking cells
the cardiovascular system
closed loop circulatory system
1. Blood enters the heart from the body through the vena cava, into the right
atrium. Right atria contracts.
2. Blood goes into the right ventricle, right ventricle contracts, blood goes into the
lungs.
3. The pulmonary circulation from the lungs, it returns to the left side of the heart, into
the left atrium, and then from the left atrium down into the left ventricle, and then the left ventricle into the body.
4. The atria are contracting together. The ventricles are contracting together.
5. Atria contract → ventricles contract
what the cardiovascular system does (purpose of blood):
• A pump (the heart)
• Some tubes (the vasculature)
• Some liquid (the blood)
• Distribute nutrients, water, and gases
• Facilitate communication among cells
• Remove cellular waste
one-way flow through the heart is ensured by:
two sets of valves
tricuspid
cusp of right AV valve, 3 flaps anchored inside the ventricle
semi lunar
inside the pulmonary artery or aorta, ensure unidirectional flow of blood
bicupsid/mitral
2 flaps, anchored inside the ventricle
during ventricular contraction:
the AV valves remain closed to prevent blood flow backward into the atria
pressure in ventricles is very high during this
Ventricular Filling (Diastole)
The ventricles are relaxed and filling with blood.
Open valves:
Tricuspid valve (right atrium → right ventricle)
Mitral (bicuspid) valve (left atrium → left ventricle)
Closed valves:
Pulmonary valve
Aortic valve
Purpose: Blood flows from the atria into the ventricles.
Ventricular Contraction Begins (Early Systole)
The ventricles start to contract, increasing pressure.
Closed valves:
Tricuspid valve closes.
Mitral valve closes.
This closure produces the first heart sound (S1, "lub").
Pulmonary and aortic valves: Still closed initially.
This brief phase is called isovolumetric contraction because all four valves are closed and pressure builds without a change in ventricular volume.
Ventricular Ejection (Systole)
Ventricular pressure becomes greater than the pressure in the arteries.
Open valves:
Pulmonary valve (right ventricle → pulmonary artery)
Aortic valve (left ventricle → aorta)
Closed valves:
Tricuspid valve
Mitral valve
Blood is pumped out of the heart.
Ventricular Relaxation (Early Diastole)
The ventricles relax after ejecting blood.
Pulmonary and aortic valves close, producing the second heart sound (S2, "dub").
For a short period, all four valves are closed (isovolumetric relaxation).
As ventricular pressure falls below atrial pressure:
Tricuspid valve opens.
Mitral valve opens.
The cycle then repeats.
ventricular relaxation:;
pressure in atria is high and low in the ventricle
mitral valve open
left ventricle, dilated
the semilunar valves prevent blood that has entered the arteries from flowing back into the ventricles during ventricular relaxation
semilunar valves closed