Exam 3
1/115
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
116 Terms
what is TBI
injury to brain from mechanical force(damages tissue) that alters brain function
who is at risk for TBI
older aged adults
males
alcohol use
previous TBI
etiology of TBI
fall contact 35%
traffic accidents 17%
struck by/against 16.5%
unknown 12%
assault 10%
other 9%
types TBI
diffuse or focal
what is diffuse TBI
widespread (reach other areas)
concussion, diffuse axonal injury, blastwh
what is focal TBI
direct impact
contusion, penetrating, hematomas
what is an open TBI
penetrating
skull fx, breach meninges, brain tissue exposed
focal
what is a closed TBI
non penetrating
external force, skull intact, brain injured
usually diffuse but can be focal
impact coup to counter coup
primary injury of TBI
its a DIRECT injury:
contusion-bruising
cerebral laceration-tearing
intracerebral hemorrhage/hematoma
diffuse axonal injury
what hemorrhage is the worst
subdural as its closer to brain tissue
who is likely to get subdural hematomas
older population
severe initial CP
great midline shift
higher incidence of death
secondary injury of TBI
INDIRECT - exacerbate neuronal damage(hours-days after primary)
inflammatory
vascular changes
edema(incr ICP)
parenchymal changes
TBI imaging?
CT is best used and MRI after stabilize injury
indications for CT for TBI
vomiting, headaches, altered mental state, loss consciousness, intoxication, post trauma seizures/amnesia, basal skull fx, facial injury
poor prognostics for TBI
eye dilation not reactive
absent motor responses
recovery from TBI
continued recovery decreases assistance needed
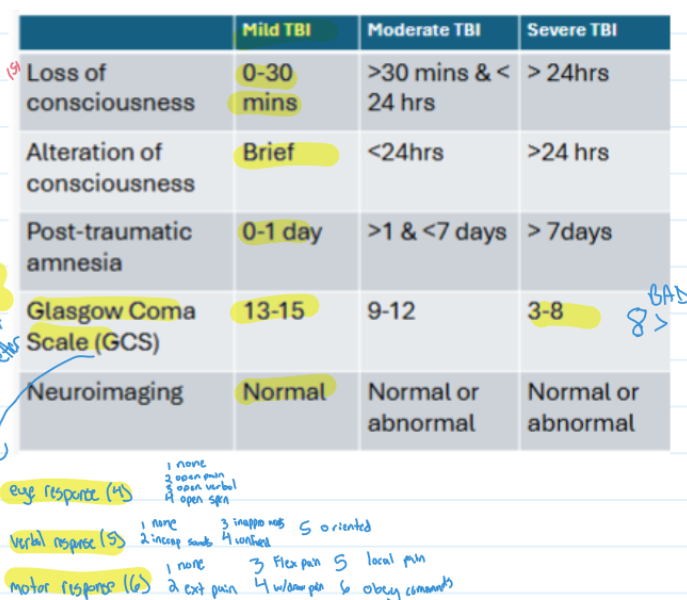
know table of mild, mod, severe TBI
terms if consciousness: alert
awake, looks around, responds in meaningful manner to verbal instructions/gesturesterms if consciousness:
terms if consciousness: coma
unarousable and unresponsive, doesnt open eyes to deep pain
terms if consciousness: stupor
unresponsive except to vigorous stimuli, may attempt to verbalize to vigorous stimuli, open eyes to pain
terms if consciousness: confused
disoriented to time, place, person, memory difficulty, difficulty with commands, exhibits alteration in perception of stimuli, may be adjusted
terms if consciousness: delirium
confusion of circumstances, may hallucinate or act as if in dream like state, conversation may not make sense, often acute ICU setting, emergence from coma
terms if consciousness: lethargic
drowsy, oriented when awake but if left alone will sleep, loud voice needed to keep awake and engaged
CM of TBI physical
loss altered levels consciousness
seizures
hemiparesis(CL)
ataxia
impaired balance
cranial n deficits
abnorm posturing
CM TBI abnorm posturing/reflexes
decerebrate- extend (worse as below red nucleus)
decorticate - flex
TBI CM for cognitive/behavioral
memory deficits
difficulty with attention, reasoning and concentration
personality changes
impulsivity, irritability, and aggression
depression and anxiety
Rancho levels of cognitive functioning(levels of cognitive recovery)
level 1 vs 10
1=total assist
10=independent
CM TBI brain regions
frontal- CL hemiparesis, mood/behavior change
temporal- CL hemiparesis, visual/memory changes, seizures
parietal- CL sensory deficits, R-L discrim difficulty
early acute med manage of TBI
prevent hypotension (SBP >90)
prevent hypoxemia (o2 sat >90)
prevent elevated ICP (<20)
NOT USE - steroids, hypothermia/hyper-ventilation
monitor ICP indications
if GCS 3-8
unilat/B motor posturing
abnorm CT
>40yo
SBP>90
whats EVD- external ventricular catheter drain
allow accurate measurement/drainage of CSF
whats IPD- intraparenchymal devices
inserted into cortical-subcortical brain region
allows ICP monitoring with collapsed ventricles
what to do to avoid hematoma to prevent secondary injury and central herniation
decompress with craniotomy or craniectomy(for diffuse BI or delayed bone replace)
indications for epidural hemorrhage TBI
on CT volume >30cc/>15mm
indications for subdural hemorrhage TBI
on CT thickness is >10mm and shift midline >5mm
GCS drops 2+
ICP >20
abnorm pupillary response
postop craniotomy/craniectomy
head bed =/>30
craniectomy=MUST wear helmet ALL time out of bed
lifting/exercise limit unitl DR says so
avoid things incr ICP
pharmacologic management of TBI
analgesics/anticonvulsants=decr pain/prevent seizures
neuroprotective drugs= reduce secondary injury(Ca channel blockers)
sedatives/anxiolytics= manage pain, agitation, anxiety
common side effects- sedate, confuse, dizzy, hypotension
TBI complications
post-traumatic epilepsy(seizures post injury, needs meds)
hydrocephalus- abnorm accumulation CSF > incr ICP (incr ICP> life emerg)
autonomic dysfunction- dysregulation HR, BP and temp control
what are red flags for PT TBI
>ICP/brain edema
acute/unstable fx(cervical spine)
severe/uncontrolled seizures
signs of ICP incr
headache, nausea, elevated BP, decline mental state, double vision, shallow breathing, non-reactive pupils, seizures, alter consciousness/coma
ELEVATE Head Bed -30
what to consider for TBI
dysautonomia(paraoxysmal symp hyperactivity)
executive function(need simple instruct)
judgement deficits
perceptual deficits
behavioral deficits
communication deficits
what us a stroke
the loss of neurological function bc impaired blood flow in the brain
-disrupt of cerebral flow that leads to ischemia/hemorrhage and lead to neuronal injury
nonmodify and modify risk stroke
modify: >55yo, gender, family history/genetics
nonmod: hypertension, afib, diabetes, dyslipidema, obesity, sedentary, birth control >35yo, smoking, cocaine use
types of stroke
TIA, hemorrhage, ischemic
what is TIA
transient ischemic atttack
focal neurologic symptoms resolves in 24hrs
what is ischemic stroke
can be thrombosis, embolism and majority of cases!!
what is hemorrhage
intracerebral/subarachnoid - less common
difference btw hemorrhage and thrombosis/embolism
hemorrhage is blood loss and psi where thromb/emb is block flow
imaging for stroke
CT very common- could have false negatives
MRA- see arteries and detect blood flow
MRI- soft tissue BEST OPTION (1st for stroke centers)
what does doppler US for strokes do
show carotid a. stenosis, post brain circulation and periph a.
NONINVASIVE
what does the arteriography and digital subtrction angiography do for strokes
xray carotid
DSA
INVASIVE
whats prognosis depend on for stroke
amt of neural damage
time onset symptoms
level cogn involvement
if someone has a stroke how likely are they to have another one
25% more likely
stroke sign BE FAST
Balance lost
eyesight changes
face drooping
arm weakness
speech difficulty
time call 911
CM of stroke
hemiparesis/plegia
impaired balance and coordination
cognitive and perceptual deficits
aphasia
dysarthria
visual disturbances
left brain damage cm of stroke
paralyzed right side
speech/language deficits
behavioral -slow/cautious
memory deficits(language)
right brain damage cm of stroke
left paralyzed
spatial/perceptional deficits
behavioral- quick/impulsive
memory deficits(performance)
whats a major branch of anterior circulation - stroke
middle cerebral artery (69%)
where does MCA supply
hands and mouth
with occlusion to MCA what can result
hemiplegia more in UE
hemisensory
hemianopsia
MCA occlusion if someone has L damage then what is affected
global aphasia
ideomotor apraxia
if R MCA occluded what could be an issue
L neglect(unilateral neglect)
what does the ACA supply afffect
LE
if ACA occluded what result in
CL hemiparesis/sensory loss more in LE
ideomotor apraxia
what PCA supply
vision and pain/sensory
PCA peripheral occlusion cause
visual deficits
memory deficits
if R PCA affected what side body
left!
PCA central occlusion causes
thalamic pain
pain and sensory impairs
CL hemiplegia
involuntary movements
webers syndrome
which artery supply CM is webers syndrome
PCA central!!
what kind of a stroke is webers syndrome
PCA or midbrain stroke
what does webers syndrome affect
ipsilat cn3(occul palsy)
CL hemiparesis
sometimes ataxia(red nuc) or rigidity(sn)
goals for acute medial management - stroke
improve cerebral perfusion
maintain oxygenation
maintain BP/CO
medical manage ischemic stroke-acute
tPA/TNK- admin within 3 hrs
surgical manage ischemic stroke-acute
mechanical thrombectomy- clot remove within 6hrs
surgical bypass for revascularization
carotid endarterectomy- plaque removed, for stenosis 60-90%, reduce risk CVA 55%
angioplasty/stents- open up blocked artery
medical and surgical manage of hemorrhagic stroke-acute
endovascular - prevent rupture by block contrib flow
surgical clipping stop bleed
bypass for revascularization
stroke- pharmacologic manage
anticoagulants/anitplatelets-aspririn/warfarin
thrombolytics-TNK/tPA
antihypertensives and statins- beta blockers, Ca channel blockers
cautions with stroke pts
decr in sight to deficits of R brain stroke
fall risk
psi injuries
contraindications to pts with stroke
TNK/tPA-not start PT 12-24hrs from administration
BP monitoring!!!
PT measures for pt post stroke
10 m and 6MWT
functional gait assessments
5 times sit - stand and ABC scale
Berg balance scale
etiology of meningitis
inflammation of meninges of brain/spinal cord
pathogenesis of meningitis
infection carried by blood products/other fluids causing damage to cerebral capillary organisms
blood brain barrier fails prevent entry infectious organisms
what is most common cause meningitis type of inflammation
viral/aseptic meningitis
what is aseptic meningitis
contamination of CSF by virus/fungus(enteroviruses, herpes simplex virus 2, epstein barr virus, systemic lupus erthematosus, intracranial tumors)
occurs days-weeks after exposed
where is bacterial meningitis
organisms in mucosal surfaces in upper respiratory tract- sinusitis, otitis, mastoiditis
whats neonatal meningitis
birth canal transferred to infant from mother- ecoli, listeria, group b streptococcus
CM of meningitis
fever, headaches - stiff/painful neck(nuchal rigidity)- kernigs/brudzinskis signs
pain lumbar area and post thigh
cranial n palsies and deafness
changes in mental status/behavior
fever
late disease process CM of meningitis
focal neurological signs- weakness, visual disturbance, aphasia
meningitis medical management
blood test/lumbar puncture determine bacterial/viral
CT brain inflammation
treatments- antibiotics, IV fluids, steroid meds
hospital stay- few days-weeks
etiology of encephalitis
inflammation of grey matter
-mosquito/tick(west nile)
-herpes simplex virus(skin contact, resp droplets)
pathogenesis of encephalitis
cerebral edema destroys n cells causing intracerebral hemorrhage and brain damage
CM of encephalitis
headache, nausea, vomiting- altered consciousness(coma)
fever
agitation
focal neurologic signs- hemiparesis, apraxia, ataxia, disorder limb movement, visual disturbances, aphasia
seizures common
diagnosis encephalitis
CT or MRI - brain inflammation
lumbar puncture- infection/autoimmune antibodies
blood/urine - viruses
EEG- brain electrical activity
treat encephalitis
mobility restrict
incr fluid intake
autoinflamm(steroids)
antivirals/IVIG/plasma exchange
follow up therapy
PT for CNS infections - primary vs secondary
recognize when refer to MD/PCP = primary
secondary= treat complications of weakness, impaired balance, AS, motor coordination
types CNS inflammation
meningitis and encephalitis
classify neoplasms
names by cell origin
primary v secondary
benign v malignant
histologic grade
anatomic location
childhood v adult
grade
grade
grade
grade