Equine diseases of the head & neck 2
1/60
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
61 Terms
What are the important components of the anatomy of the nares/nostrils?
Alar folds

Supported by alar cartilages —> keep nostrils open
need to be as wide as poss during exercise
Facial nerve
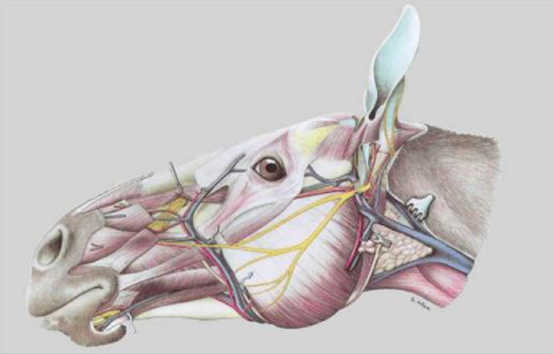
Nasal diverticulum (false nostril)
List some examples of nasal disorders
Trauma —> lacerations
Facial nerve paresis / paralysis
Nasal atheroma
Alar fold collapse
What can cause facial nerve paresis?
GA / recumbency where pressure over facial nerve
Iatrogenic e.g. surgery of face
Most often temporary paresis, will resolve with time
What are the clinical signs of facial nerve paresis / paralysis?
Facial swelling
Asymmetry
Reduced airflow
Nasal stertor
+/- facial distortion
Poor performance
How is facial nerve/paresis diagnosed?
Observation
Palpation
How do you deal with lacerations of the nares?
Precise anatomical repair important
Minimal debridement —> good blood supply, preserve the tissues
2/3 layer closure
Monitory for rubbing of suture
What are the problems with chronic scarring following lacerations of the nares?
Performance limiting (reduced nasal flow)
Cosmesis may be important (show horses)
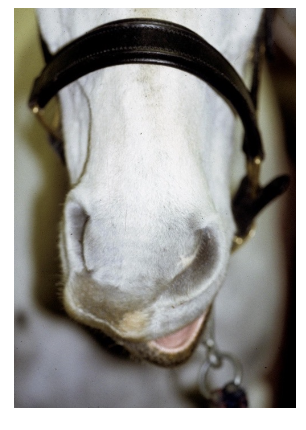
What is an epidermal inclusion cysts /nasal atheroma?
Cyst within nasal diverticulum (false nostril)
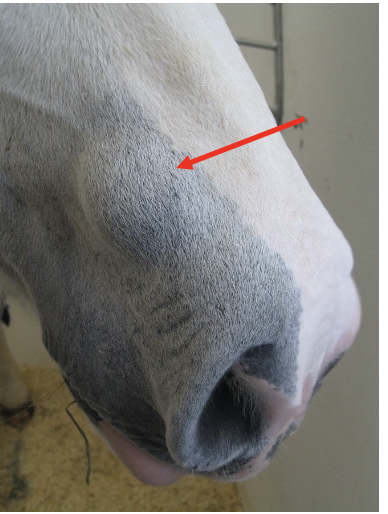
What are the clinical signs of nasal atheroma?
Non-painful swelling at nasoincisive notch
What is the diagnosis, tx & prognosis of nasal atheroma?
Dx —> History, visual appearance, histopathology.
Tx —> surgical removal (usually under LA + standing sedation)
Prognosis —> excellent with surgical removal; likely to recur with simple drainage.
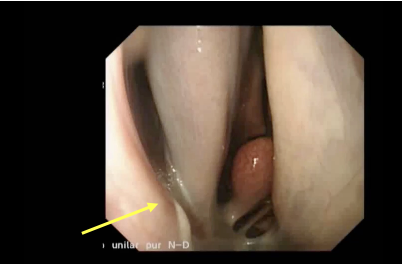
What is alar fold collapse?
Flaccid or redundant alar folds
Respiratory tract noise at exercise
Exercise intolerance in performance horses
Pathogenesis = Unknown
How is alar fold collapse diagnosed and treated?
Dx —> fluttering sound at exercise (ddx laryngeal/ soft palate disorders) temporary sutures
Tx —> can resect folds
What separates the nasal passages?
Nasal septum & vomer bone
Describe the anatomy of the dorsal and ventral conchae
Thin scrolls of cartilage and bone
Divide nasal passage into 3 meati:
Dorsal
Middle
Ventral
Form conchal sinuses caudally
What are the key anatomical features of the nasal passages?
Sinuse drainage angle
Where paranasal sinuses drains into nasal passages
Usually 2-3mm —> can't directly access paranasal sinuses in normal horse using nasal endoscope
Ethmoidal turbinates
What are the congenital disorders of the nasal passages?
Wry nose (nasal septal deviation)
Choanal atresia (rare)
Membrane that should not be present is → severe airway blockage
What are the acquired disorders of the nasal passages?
Trauma (iatrogenic common)
Progressive ethmoid haematoma (PEH)
Fungal rhinitis
Foreign bodies (rare)
What are the clinical signs of diseases of the nasal passages?
Nasal Discharge
Abnormal resp noise (altered flow of air?)
Dyspnoea
Malodorous smell —> e.g. fungal infection
Facial / nasal Distortion
Head Shaking
Snorting / rubbing nose
What can cause nasal trauma in a horse?
Epistaxis (nose bleed)
Kick/ blunt trauma
Iatrogenic
Trauma during nasogastric intubation / endoscopy common
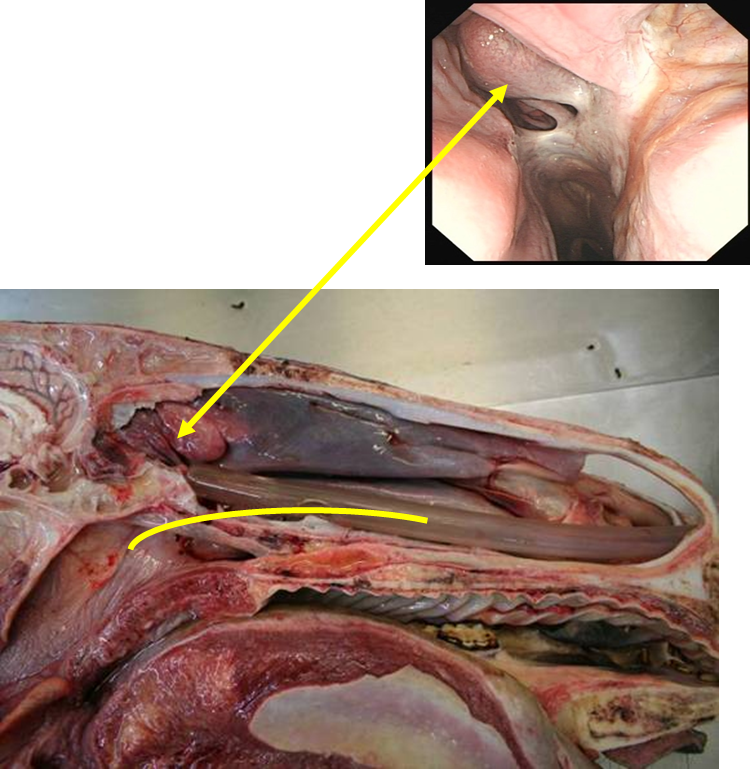
How do you avoid iatrogenic trauma of the nose?
Ensure tube placement in VENTRAL meatus not middle meatus (more likely to traumatise ethmoturbinates)
Use smooth tube
Lubricant on end of tube
Do not force tube when meet resistance
Haemorrhage will stop in 5-10 mins if ethmoturbinates traumatised
What are progressive ethmoid haematomas?
Encapsulate non-neoplastic mass
Unknown aetiology
Locally invasive (does not metastasise)
Grows into nasal passages / paranasal sinuses
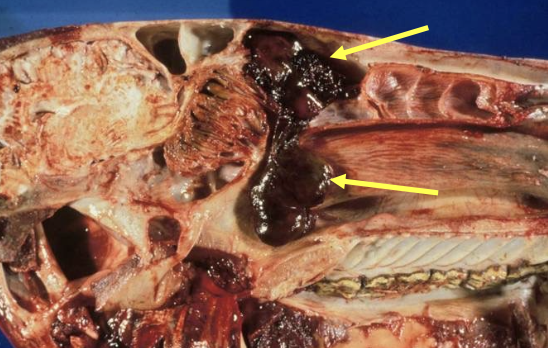
What are the clinical signs of progressive ethmoid haematomas (PEH)?
Epistaxis (nasal passages / sinuses)
Usually intermittent
Often slightly brown/red colour
+/- Facial swelling (sinuses)
How do you diagnose PEH?
Nasal PEH:
Endoscopy —> characteristic yellow/green lesion on ethmoid
+/- computed tomography
Sinus PEH:
Radiography
Sinoscopy
CT
Assess cribiform plate
Possible intracranial extension (formalin contraindicated for tx —> find out whether extends into sinuses / brain before using)
Check both sides —> often bilateral
How do you treat PEH?
In nasal passages
Intra lesional formalin —> CT first
+/- Laser excision/ ablation if small
PEH within the sinuses
Sinus flap surgery
Treat sinusitis
Remove lesions +/- laser
(recurrence common)
What are the types of fungal rhinitis?
Primary (Uncommon in UK)
Secondary
Fungal disease 2° to bacterial sinusitis common
What are the clinical signs of fungal rhinitis?
Unilateral purulent/haemorrhagic nasal discharge
+/-Malodorous smell
Occasionally nasal stertor
How do you diagnose and treat fungal rhinitis?
D —> endoscopy and fungal culture
Tx —> removal of fungal plaques and necrotic bone, topical antifungal treatment (Eniloconazole lavage)
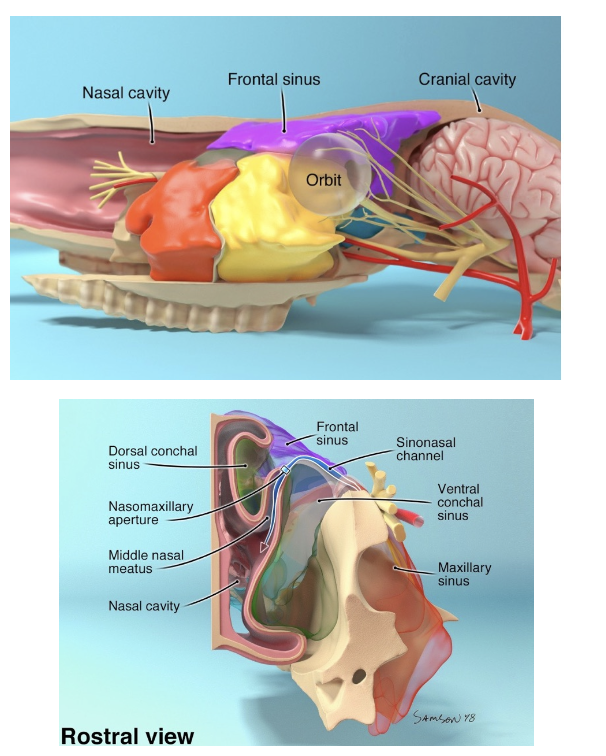
How many paranasal sinuses are there and how many groups?
7 pairs of paranasal sinuses
2 functional groups
No communication between groups
Sinuses within each group share drainage into the nasal passages
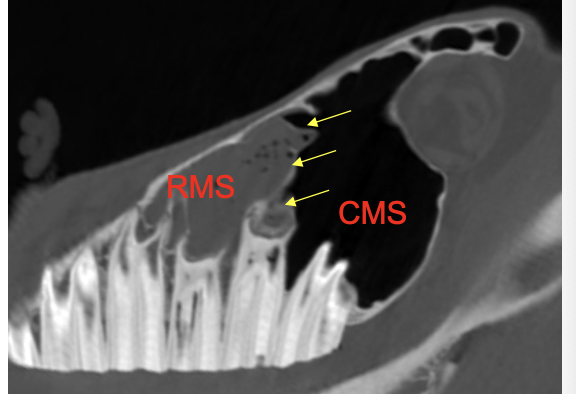
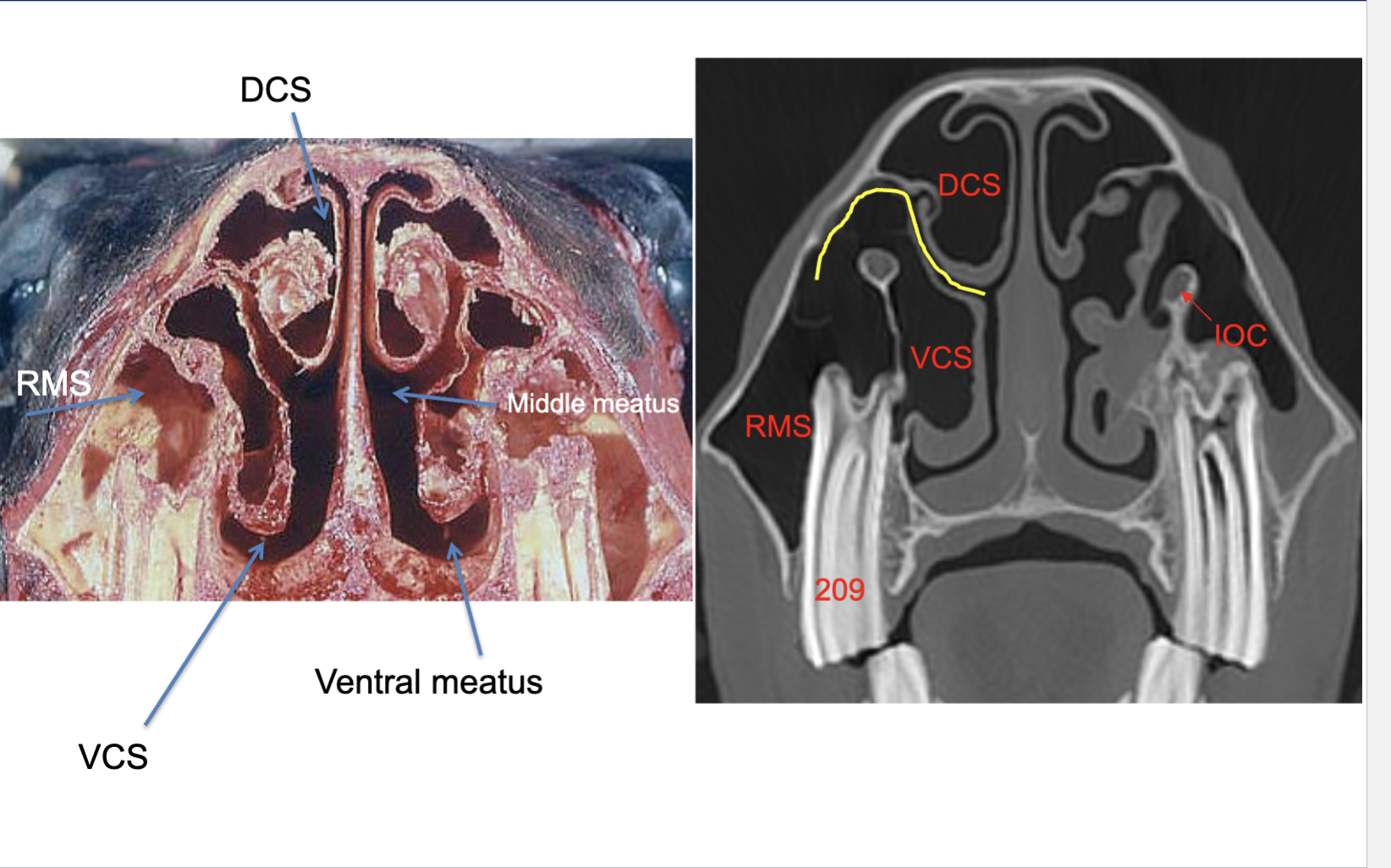
What are the groups and names of the paranasal sinuses?
Rostral group (2 sinuses)
Rostral maxillary (RMS)
Ventral conchal (VCS)
Caudal group (5 sinuses)
Caudal maxillary (CMS)
Frontal (FS)
Dorsal conchal (DCS)
Sphenopalatine (SP)
Ethmoid sinus (ES)
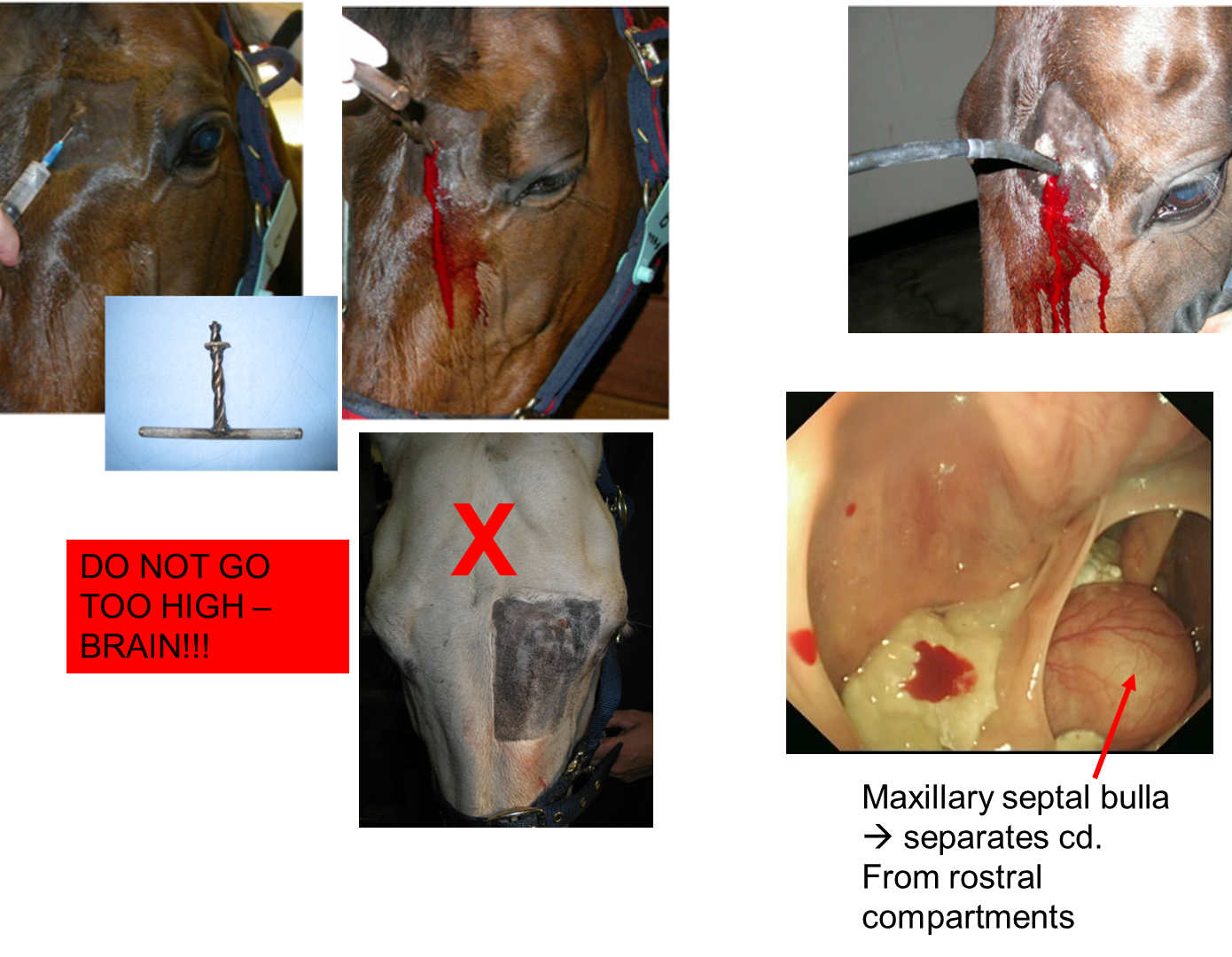
What are the key anatomical points regarding the paranasal sinuses?
Proximity to other structures
May cause disease in these e.g. intrasinus PEH can extend into brain
Disease may extend from these structures
Periapical regions of teeth → 2° sinusitis
Rostral & caudal groups separated by oblique bony septum
Important when performing flushing of sinus compartments
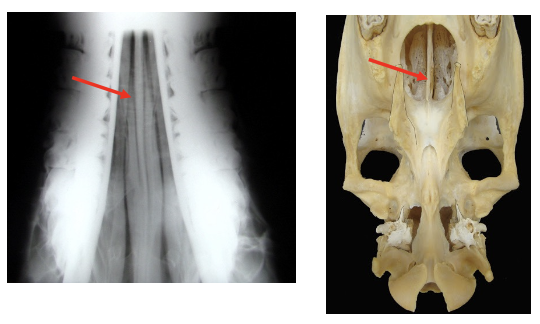
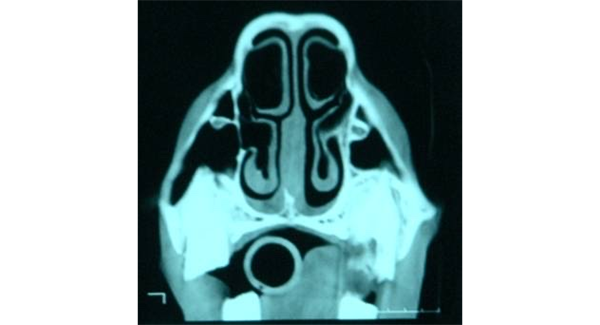
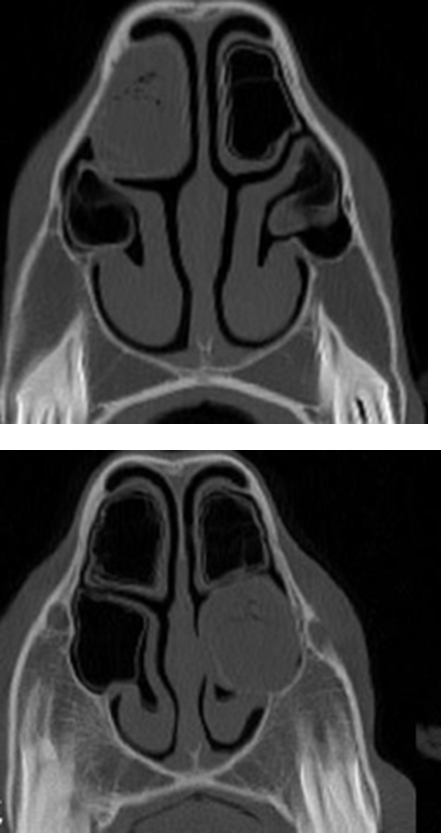
What is being indicated in these images?
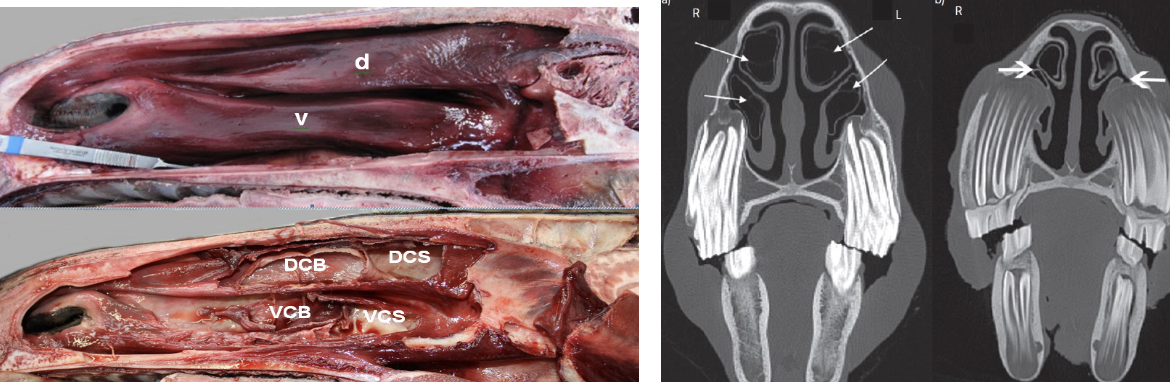
Conchal bullae —> air filled but can become infected
then form dorsal & ventral conchae
List the diseases of the paranasal sinuses
PRIMARY SINUSITIS
SECONDARY SINUSITIS
PAI / fungal
SINUS CYSTS
SINUS PEH
NEOPLASIA
TRAUMA
What is the most common presentation of paranasal sinus disease?
NASAL DISCHARGE
FACIAL SWELLING
What are the clinical signs of paranasal disease?
Predom unilateral nasal discharrge (may be bilateral if bilateral sinus dx)
nature of discharge —> serous / purulent / mucopurulent / haemorrhagic
Facial swelling
Facial deformitiy
Decreased nasal airflow
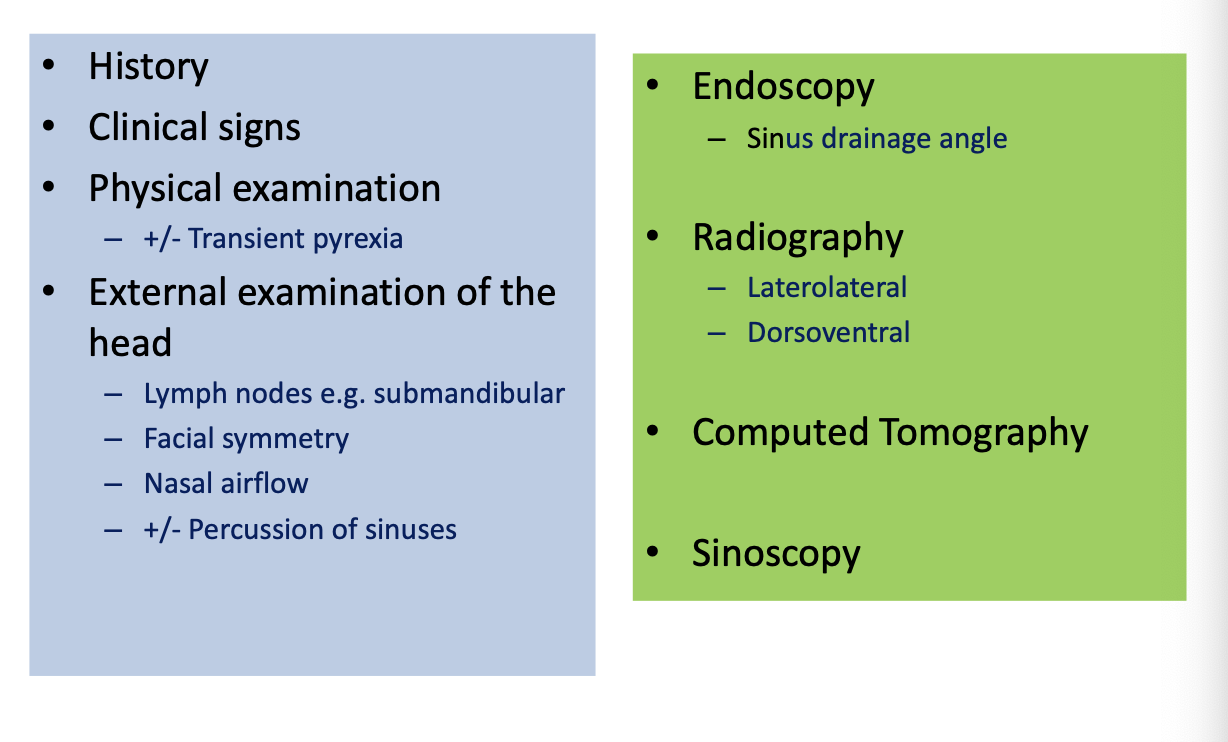
How is disease of the sinus diagnosed?
What causes primary sinusitis?
Prev. URT infection
Streptococcus spp most commonly
What causes secondary sinusitis?
1. Dental disease (60% of 2°)
2. Sinus cyst
3. PEH
4. Neoplasia
5. Fungal sinusitis (rare)
MUST treat sinusitis & primary cause of sinusitis
How is sinusitis diagnosed?
Endoscopy —> visualise purulent material coming from sinus drainage angle
Rads:
fluid line on lateral view,

radiodensity in sinuses on DV views
poor sensitivity for identifying cause of 2° sinusitis
CT —> gold standard, teeth = greater sensitivity, useful for pre op planning
How is 1° sinusitis treated?
Antimicrobials
Culture & sensitivity to rule out strep equi
One course only
e.g. trimethoprim sulphonamides for 7-14d
Poor response indicated further infection
Do not try diff antibiotics —> resistance
NSAIDs e.g. phenylbutazone
Feed from ground (encourage drainage)
Dust free management —> reduce URT inflam
Turn out as much as possible —> drainage & reduce inflam
Surgical draiange if does not respond (most mild, acute cases respond)
What is the most freq cause of 2°sinusistis?
Dental dx
Why does dental disease cause secondary sinusitis?
Close proximity of alveolar bone to maxillary sinuses
Upper 08/09s —> Rostral Maxillary Sinus (RMS)
Upper 10/11s —> Caudal Maxillary Sinus (CMS)
How is 2° sinusitis diagnosed and treated
D:
Rads insensitive
CT gold standard
Tx:
Removal of infected tooth
Management of sinusitis
In what animals are paranasal sinus cysts seen?
Young horses most common but can see in all ages
Aetiology unknown —> filled with yellow, viscous fluid
What do paranasal sinus cysts cause?
Erosions & distortion & they expand
Nasal passage deformity
Facial swellings

What are the clinical signs of paranasal sinus cysts?
Facial swelling
Reduced nasal airflow (can be subtle to detect)
Nasal discharge
Nasal stertor
How are paranasal sinus cysts diagnosed and treated?
D:
Rads
Sinoscopy
CT
Tx —> surgical removal via trephine portals / sinus flap
What signs are associated with sinus neoplasia?
Facial swelling
+/-nasal discharge, head shaking
May not be detected until extensive growth has already occurred
What are the common types of sinus neoplasia?
SCC
Adenocarcinoma
Fibro-osseous tumors
Myxoma (benign tumour of heart)
How is sinus neoplasia diagnosed and treated?
D:
Rads / Sinoscopy
CT
Tx:
Usually too extensive to treat
Debulking and radiotherapy uncommonly performed (costs/ facilities)
What is sinus trauma caused by?
Direct trauma e.g. running into tree
How is sinus trauma diagnosed and treated?
D:
Clinical signs
Radiography
+/- US and CT
Tx:
Removal/ stabilisation of bone fragments
Flushing of sinuses to remove blood / purulent material
What are the trephine sites for sinoscopy?
Frontal sinus (blue)
Caudal maxillary (orange)
Rostral maxillary (red)
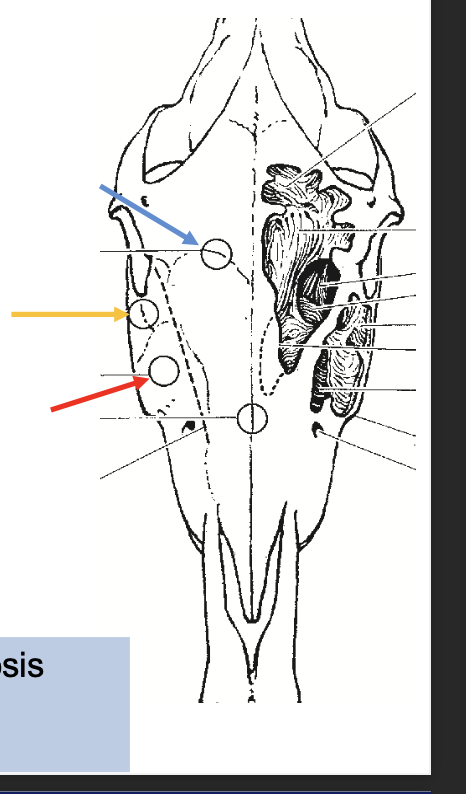
enables access into sinuses for diagnosis (sinoscopy) & tx e.g. flushing
What are sinus flaps?
Used to increase access into sinuses for removal of masses/other treatment
Often performed under standing sedation (avoid GA —> costs/risk, less haemorrhage)
Rectangular, bony flap created

What are the possible sites for sinus surgery?
Maxillary sinus flap
Frontonasal flap
dependent on location of lesion
What are the potential complications of sinus surgery?
Haemorrhage
Infection of the trephine portal / sinus flap
Bone sequestrum formation
Poor cosmesis (white hair)
Recurrence of sinusitis
What is empyaema conchal bullae?
Chronic infection of dorsal or ventral conchal bulla
Relatively newly recognised
Surgical techniques for draiange
What is suturitis?
Perisotitis of the suture line in skull
frontonasal suture most common —> can occur after sinus surgery
Bilateral, firm, swelling in nasofrontal region
May be painful at first
Settle & become non-painful
Usually regresses with time but some can be permanent
What is dentigerous cysts?
Congenital condition —> failure of closure of 1st branchia cleft
Swelling on head —> usually @ base of ear, firm ± discharging sinus tract but can occur elsewhere (rare)
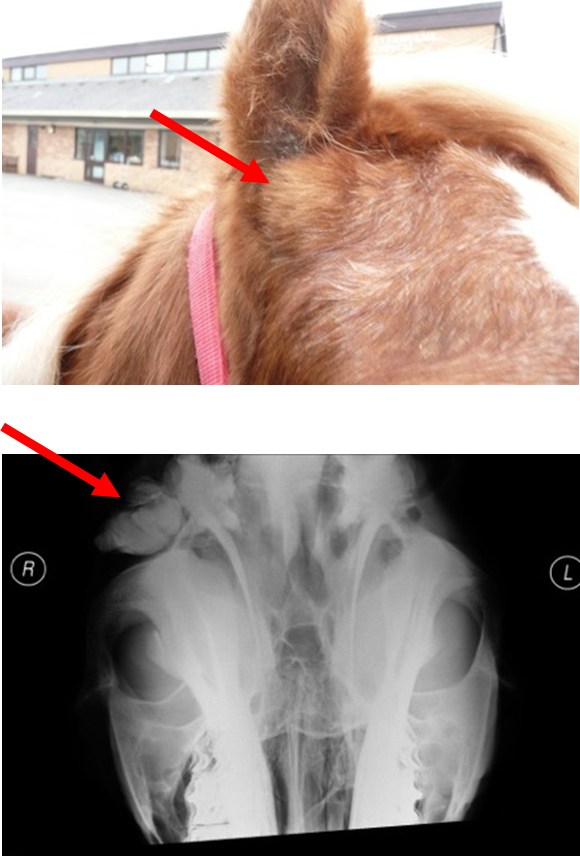
How are dentigerous cysts diagnosed?
Clinical signs, rads, CT
How are dentigerous cysts managed?
Can be left untreated
Usually removal requested cosmetically —> risk of infection developing / problems selling horse
Describe surgical excision of dentigerous cysts
Performed under GA
Advanced & specialist
Prognosis good —> no cyst remnants should be left in situ