Neural Control of GI Motility and Function
1/48
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
49 Terms
Major GI sphincters
Lower Esophageal Sphincter(LES), pyloric valve, ileocecal valve, internal/external anal sphincters.
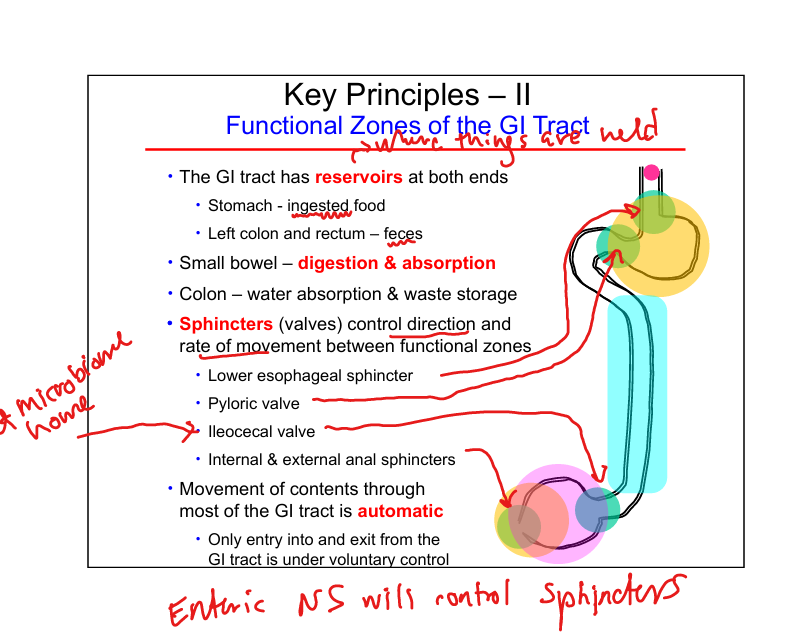
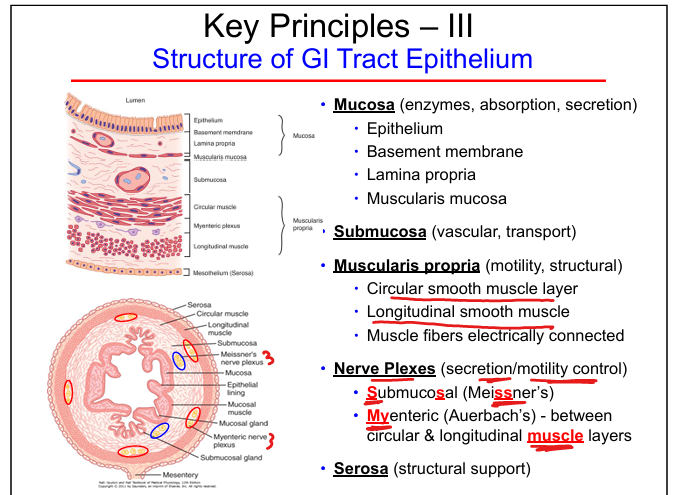
Layers of GI tract
Mucosa, submucosa, muscularis propria (circular + longitudinal), nerve plexuses(Submucosal and Myenteric), serosa.
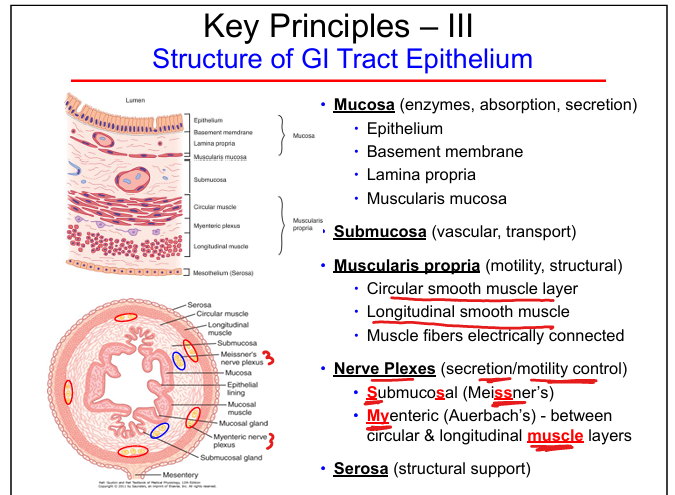
Function of mucosa
Secretion, absorption, enzyme activity.
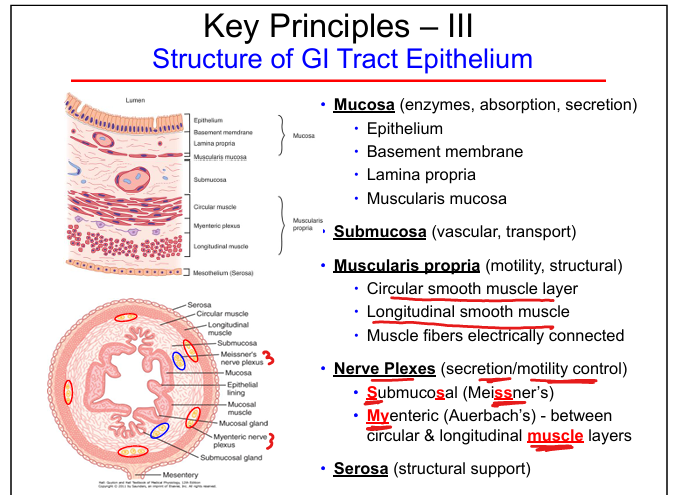
Function of submucosa
Vascular supply, transport, glands.
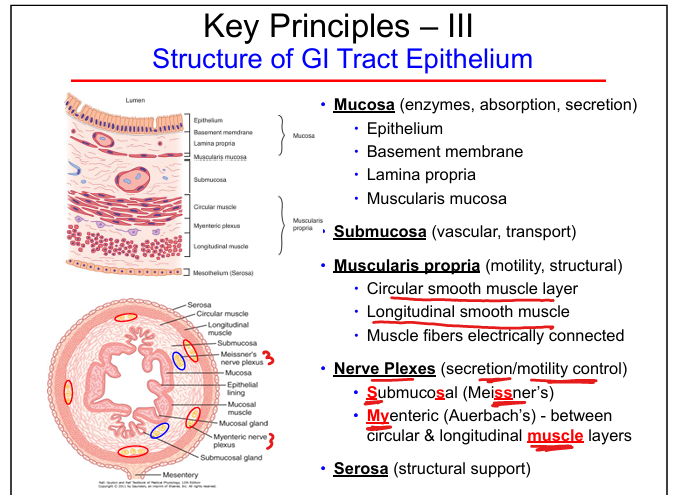
Function of muscularis propria
Motility; circular + longitudinal smooth muscle.
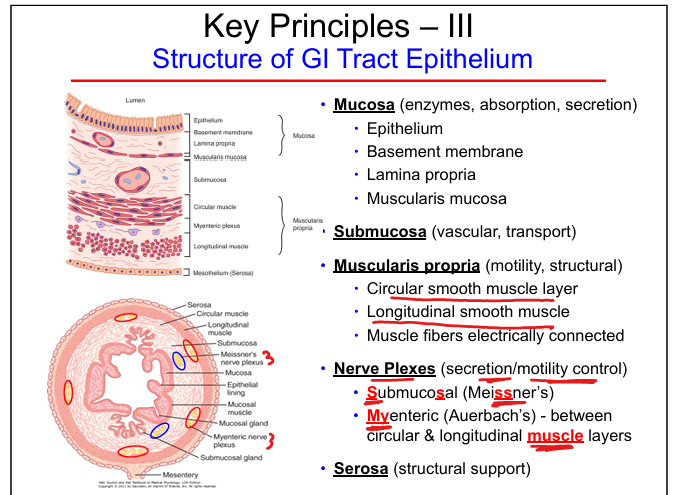
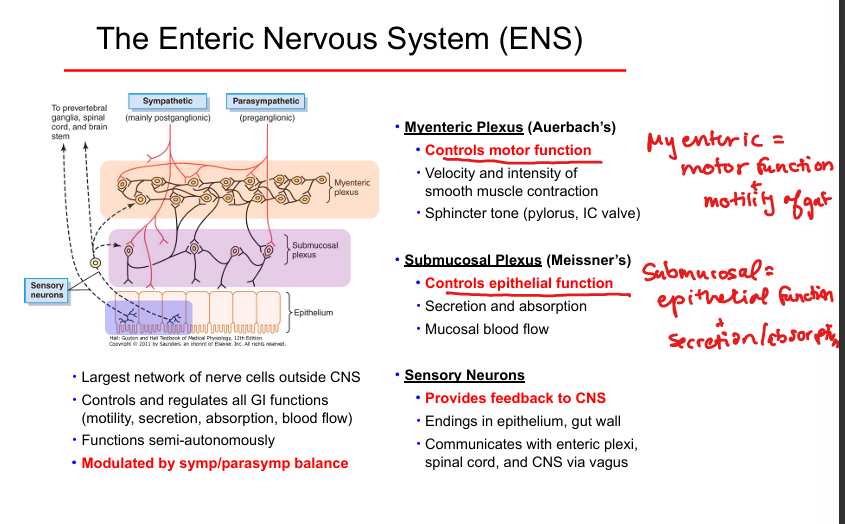
Myenteric plexus (Auerbach’s)
Controls motor function: contraction strength, peristalsis, sphincter tone.
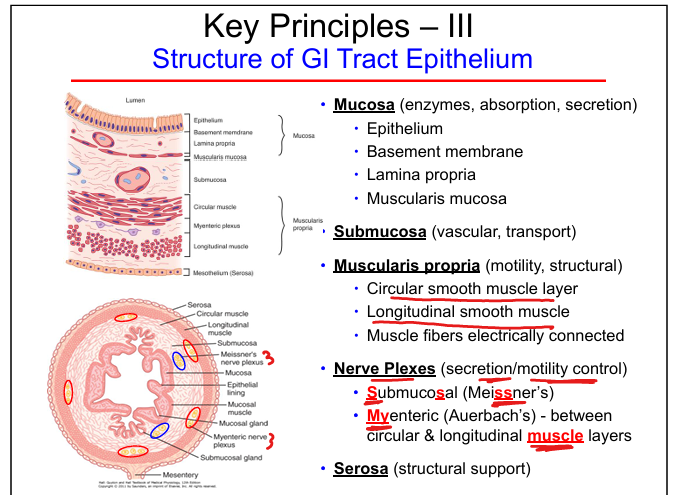
Submucosal plexus (Meissner’s)
Controls secretion, absorption, mucosal blood flow.
ENS role
Regulates motility, secretion, absorption, blood flow; largest nerve network outside CNS.
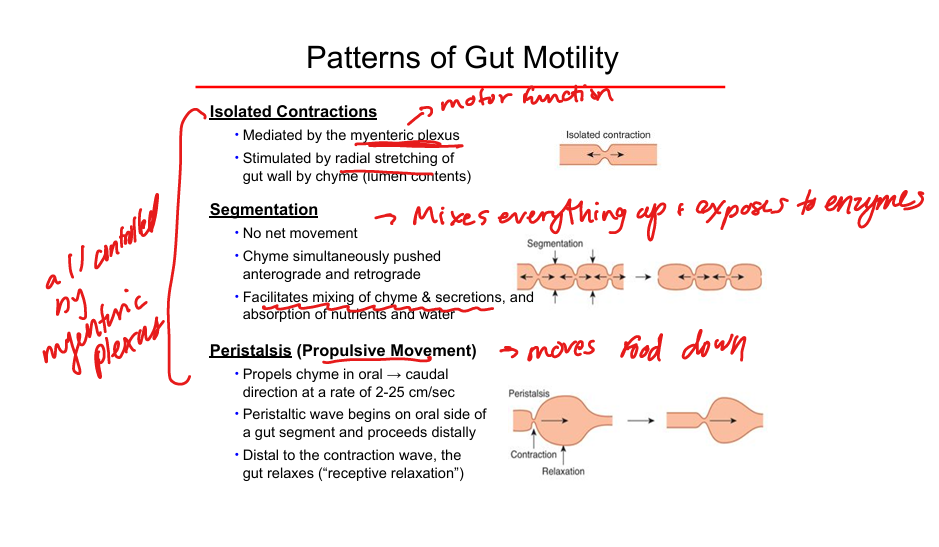
Isolated contractions
Small, localized contractions for mixing; mediated by myenteric plexus.
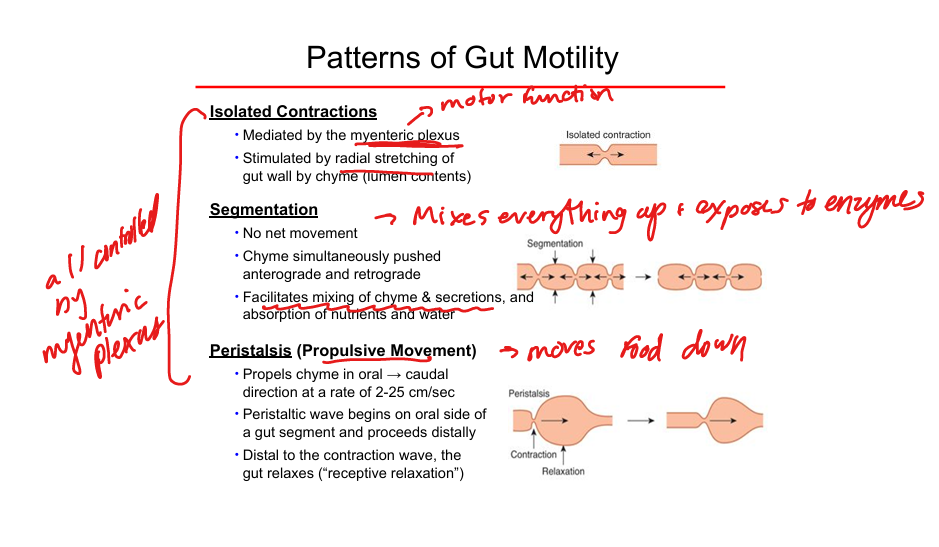
Segmentation
Mixing movement; no net propulsion; enhances digestion and absorption.
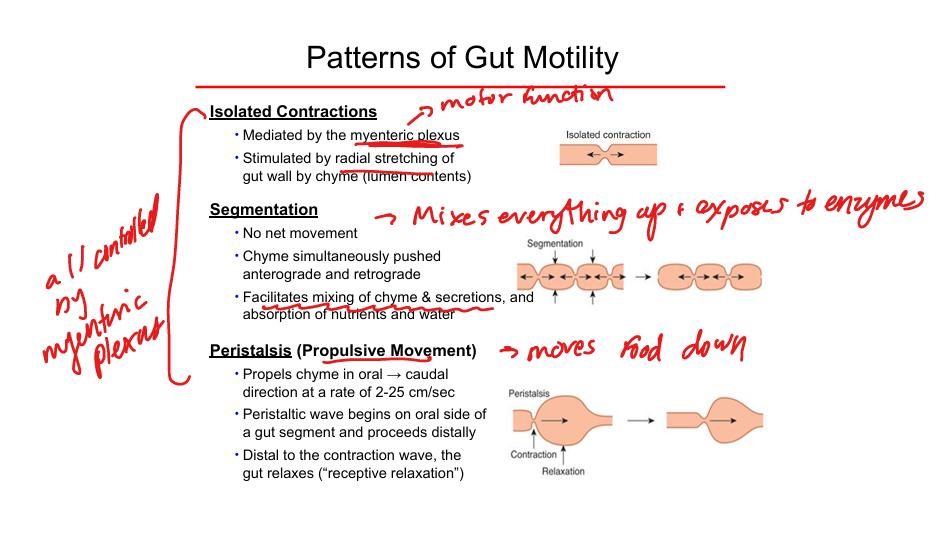
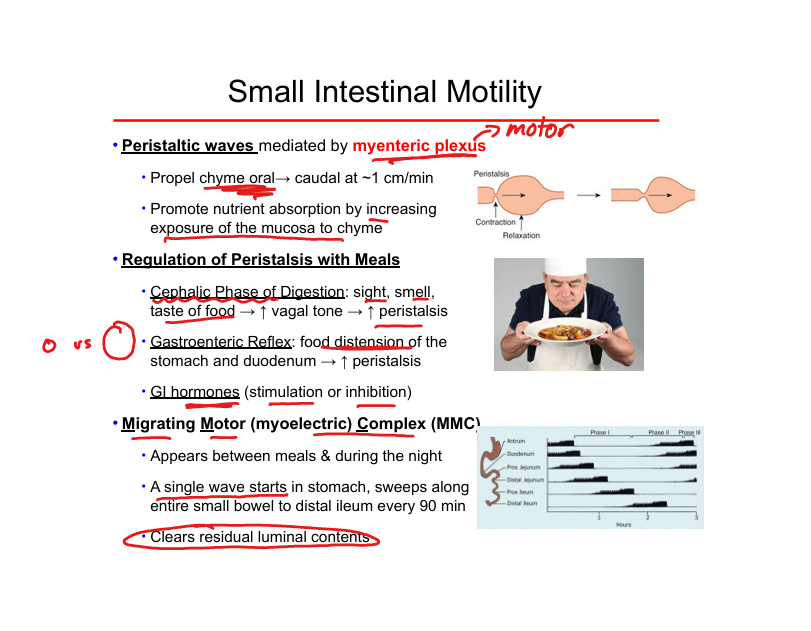
Peristalsis
Propulsive movement; oral → caudal; contraction followed by receptive relaxation.
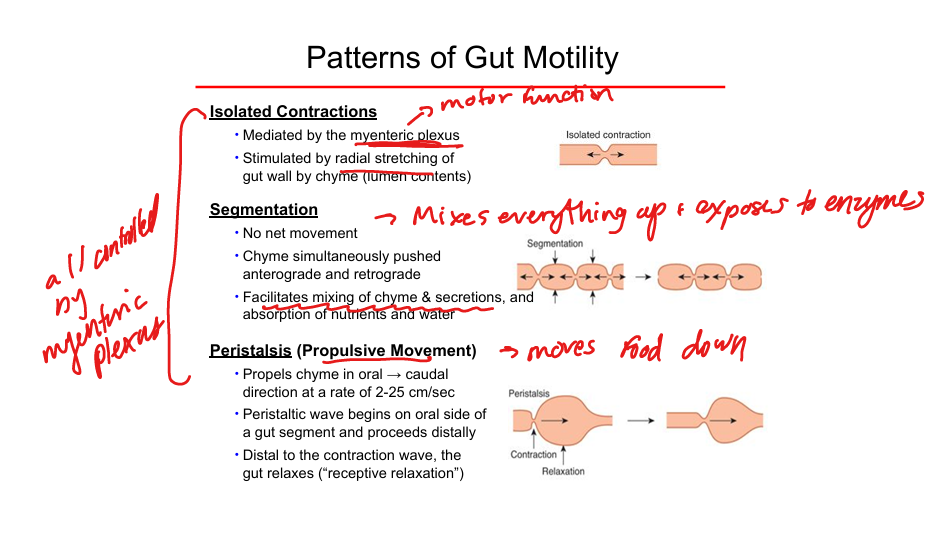
Trigger for peristalsis
Radial stretch of gut wall by chyme.
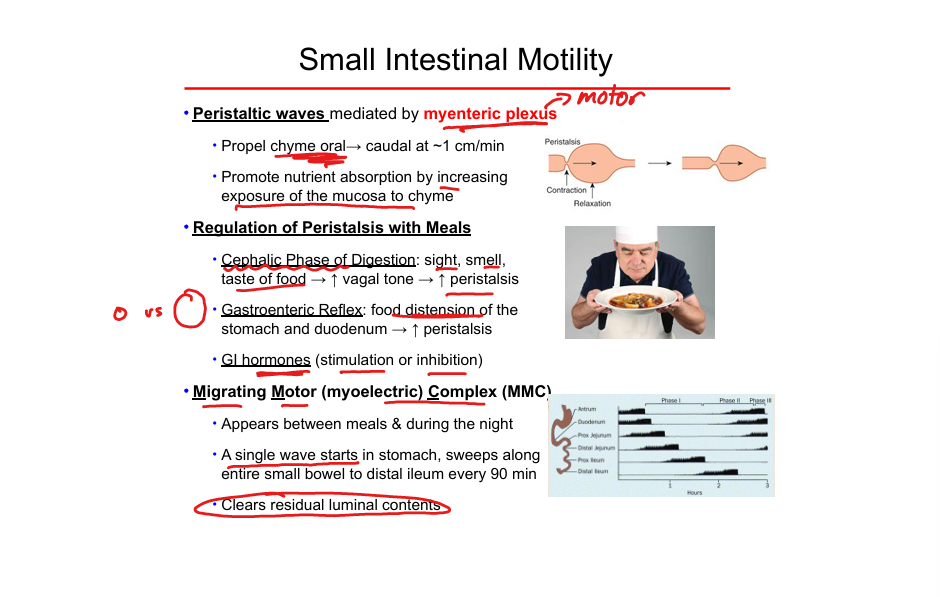
Migrating Motor Complex (MMC)
Fasting motility pattern; sweeps stomach → ileum every 90 min; clears residual contents.
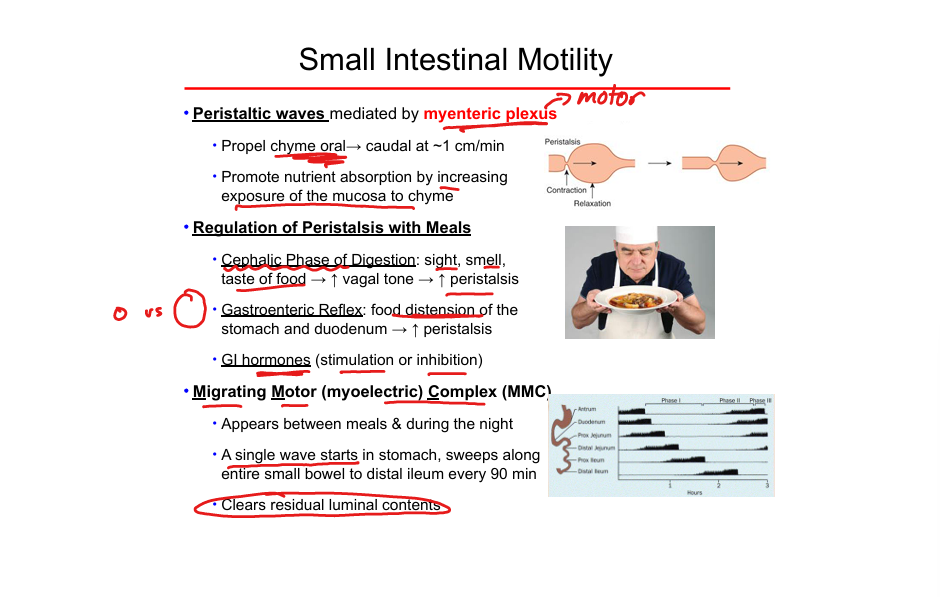
Gastroenteric reflex
food distension of the stomach + duodenum= inc peristalsis
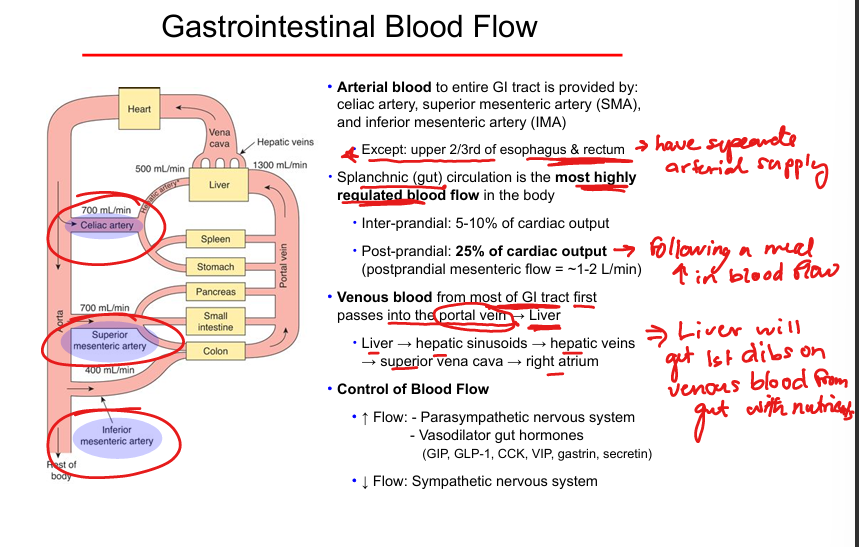
Arterial supply of GI tract
Celiac artery, SMA, IMA.
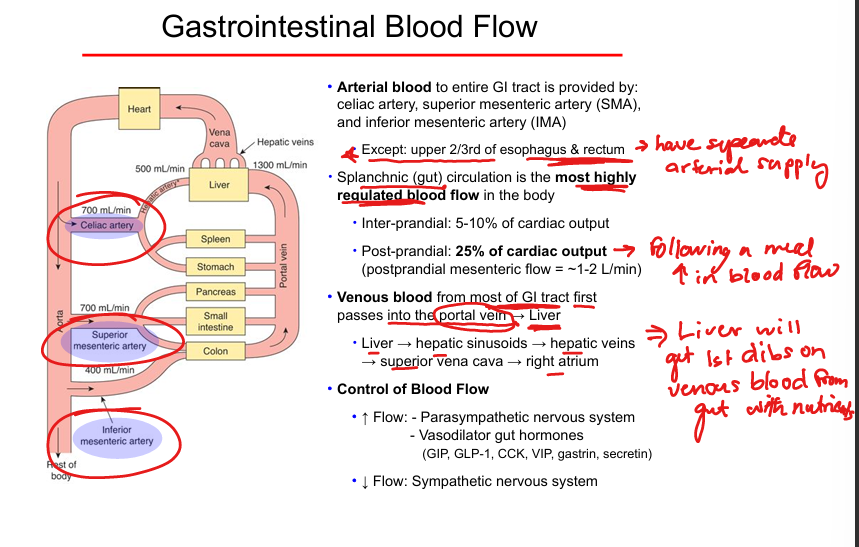
Portal circulation
Venous blood from GI → portal vein → liver → hepatic veins → IVC.
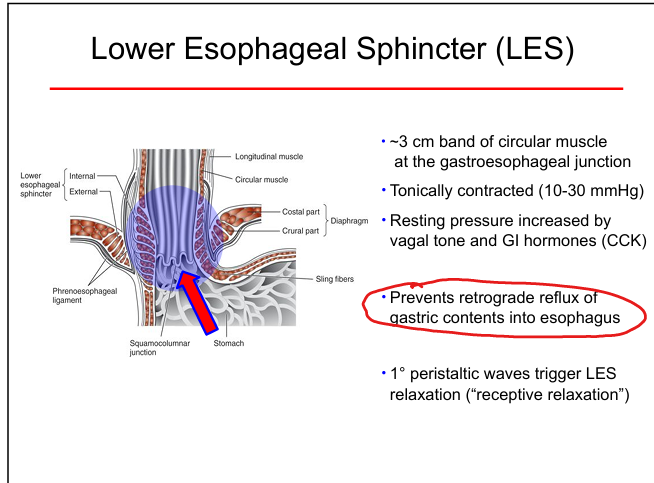
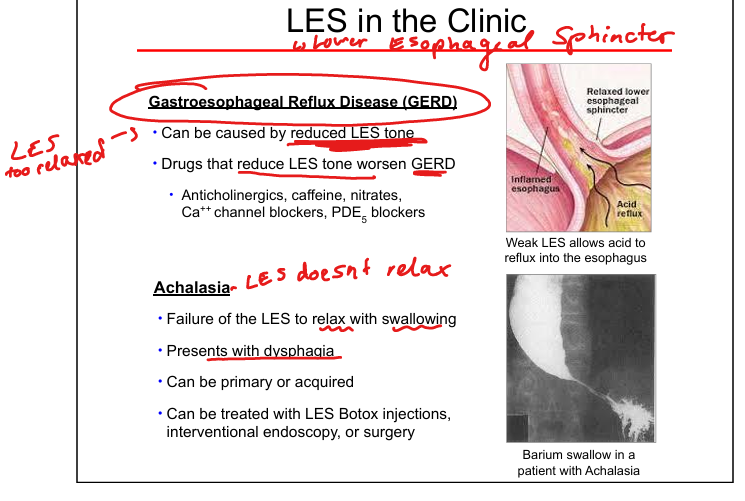
Lower esophageal sphincter (LES) function
Prevents reflux; tonically contracted at 10–30 mmHg.
Decrease LES tone
Anticholinergics, caffeine, nitrates, CCBs, PDE inhibitors.
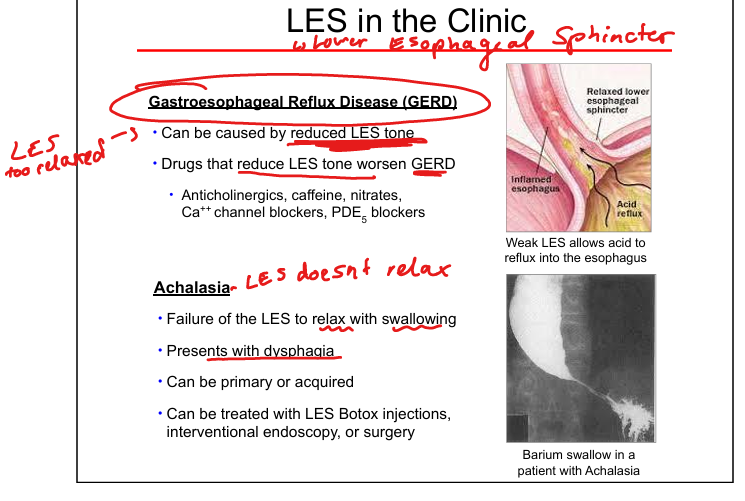
GERD mechanism
Weak LES → acid reflux.
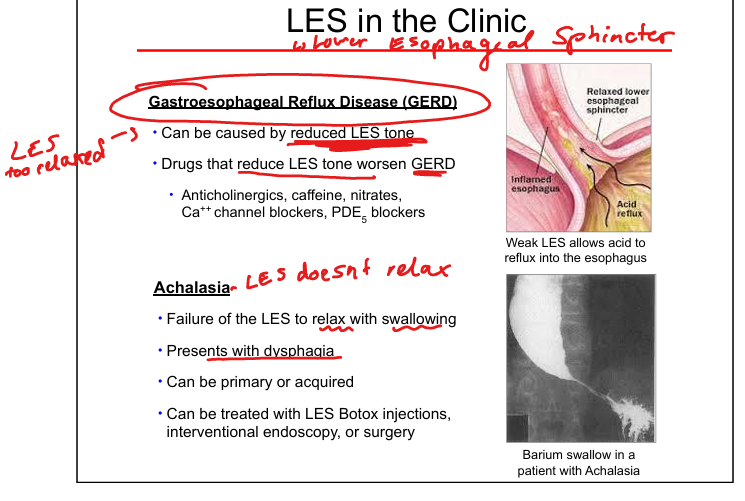
Achalasia mechanism
LES fails to relax → dysphagia; treated with Botox, dilation, surgery.
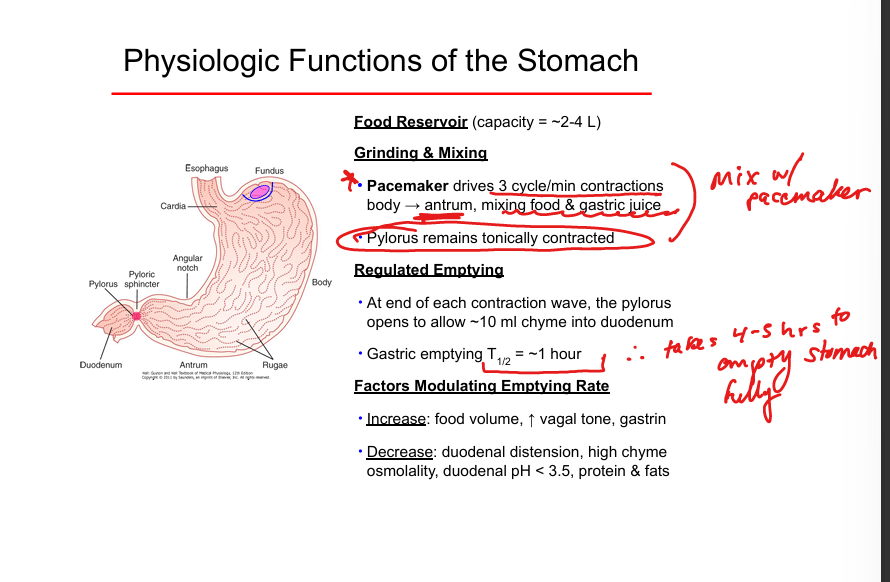
Gastric emptying
~10 mL per contraction; full emptying ~4–5 hours.
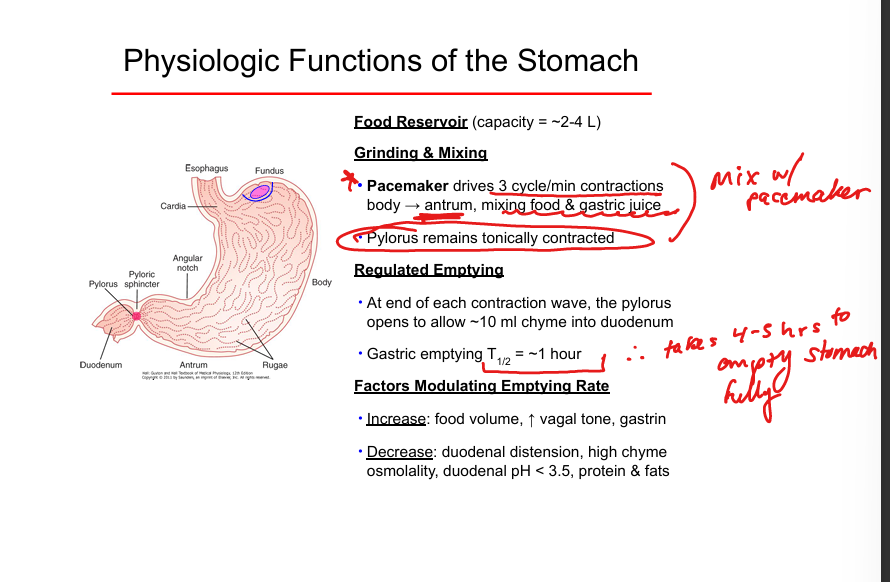
Increase gastric emptying
Food volume, vagal tone, gastrin.
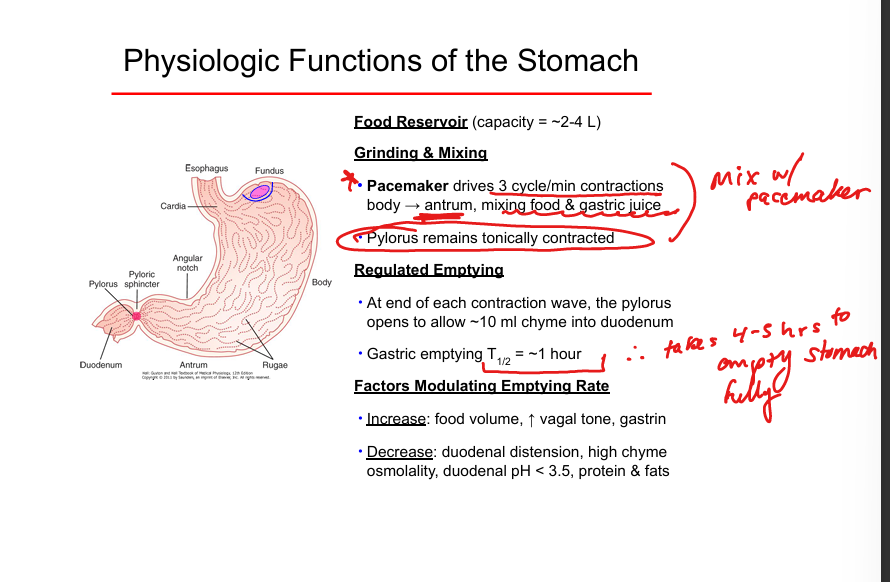
Decrease gastric emptying
Low duodenal pH, high osmolality, fats, proteins, distension.
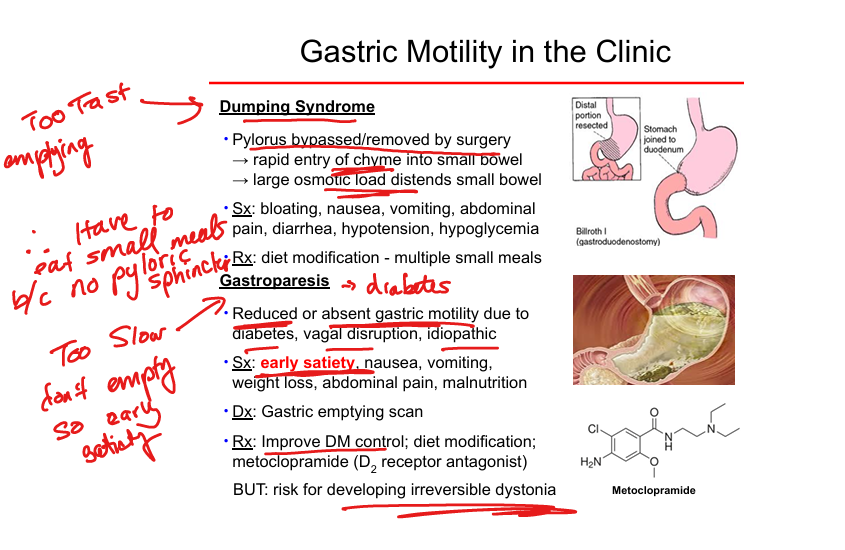
Dumping syndrome
Rapid emptying after pylorus bypass; nausea, diarrhea, hypotension; treat with small meals.
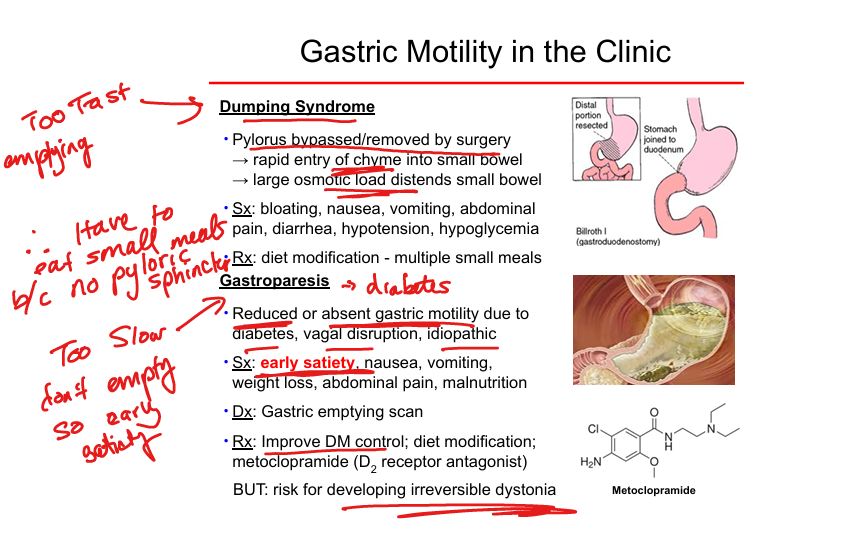
Gastroparesis
Delayed emptying and gastric motility due to diabetes/vagal injury; early satiety, nausea; treat with metoclopramide or DM control.
Small bowel peristalsis; Mediated by?
Propels chyme ~1 cm/min; increases mucosal exposure. Mediated by myenteric plexus
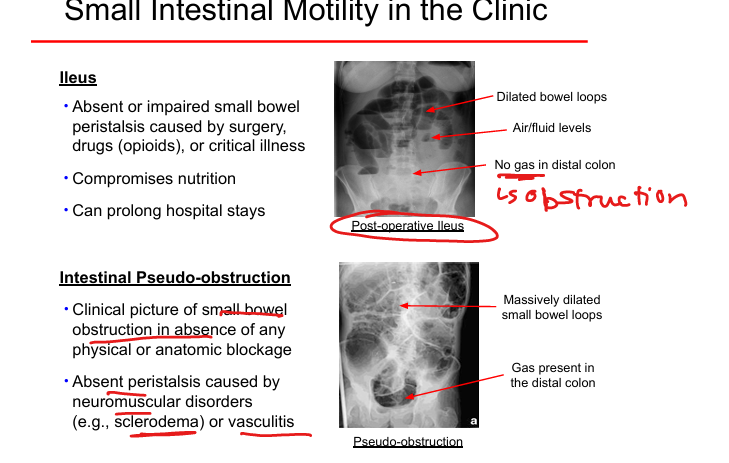
Post-Operative Ileus
Absent peristalsis due to surgery, opioids, critical illness.
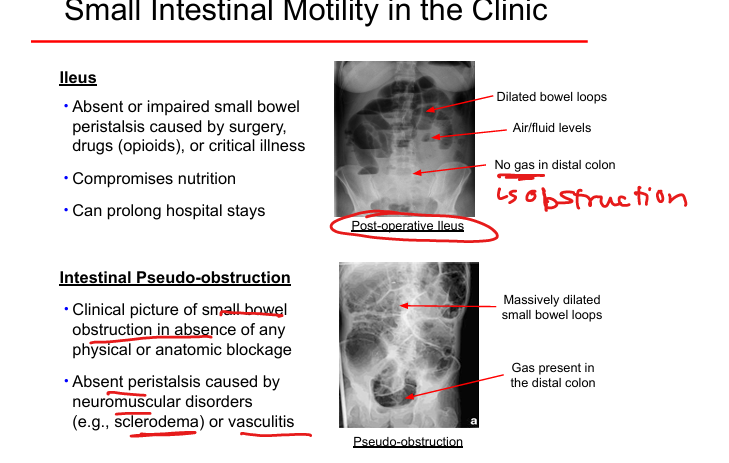
Intestinal pseudo‑obstruction
Obstruction‑like symptoms without blockage; due to neuromuscular disease(sclerodema) or vasculitis.
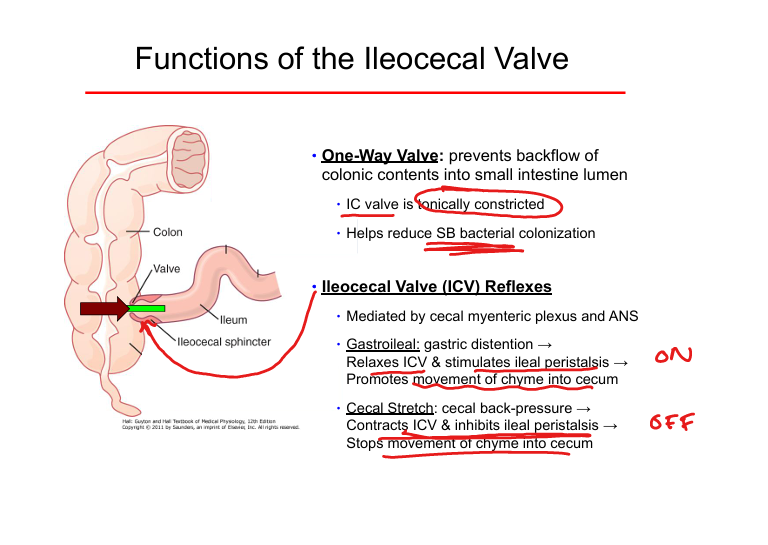
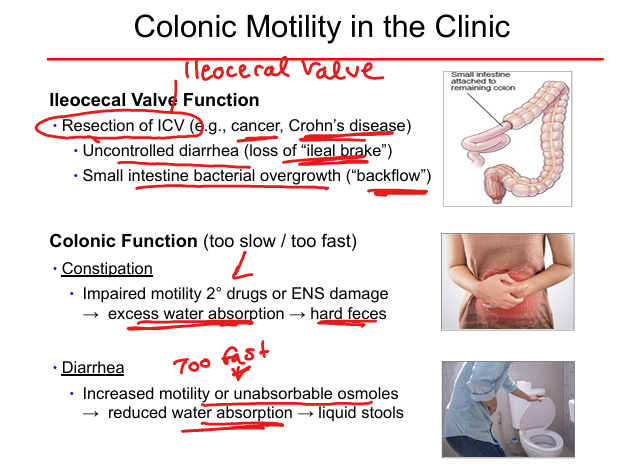
Ileocecal valve function
Prevents colonic backflow; reduces bacterial overgrowth.
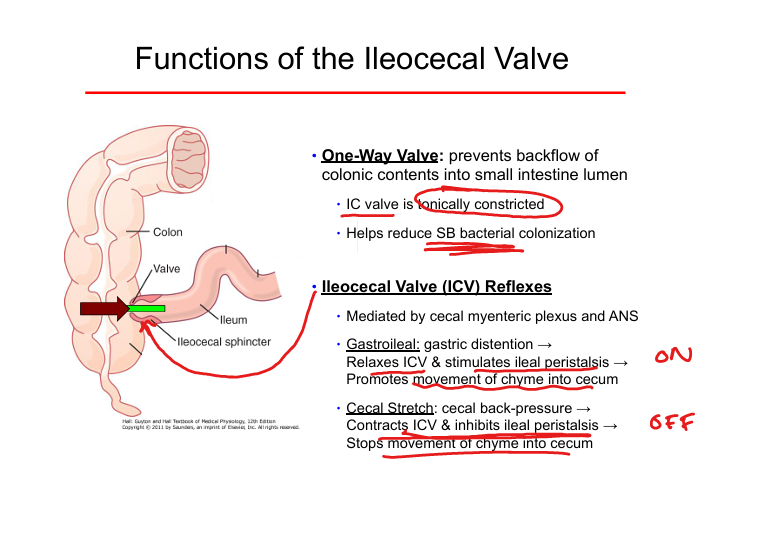
Gastroileal reflex
Stomach distension → relaxes ICV → promotes ileal emptying.
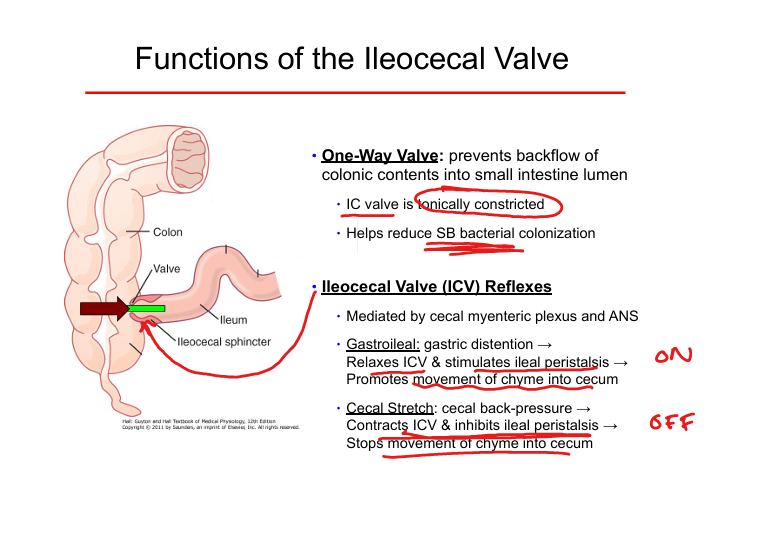
Cecal stretch reflex
Cecal distension → contracts ICV → inhibits ileal peristalsis.
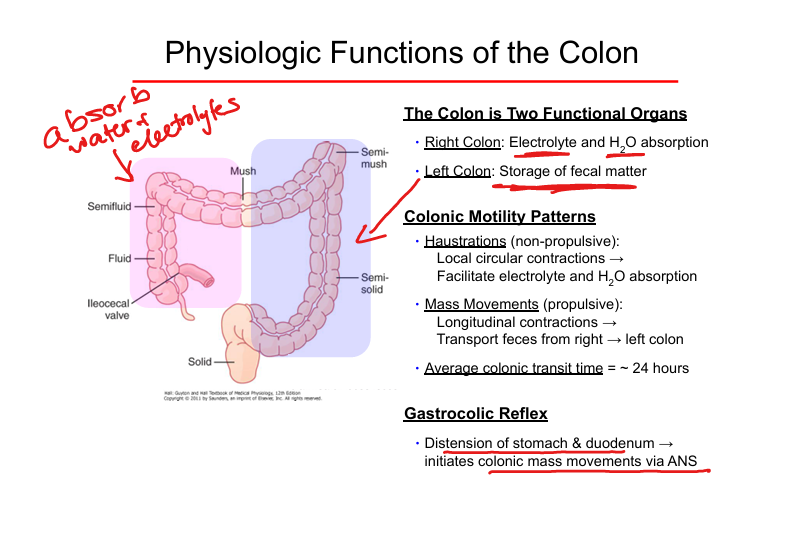
Right colon function
Water and electrolyte absorption.
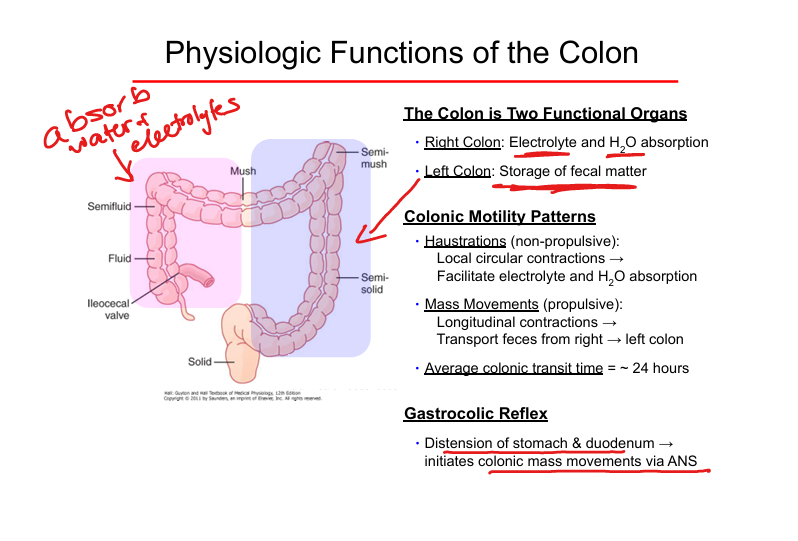
Left colon function
Fecal storage.
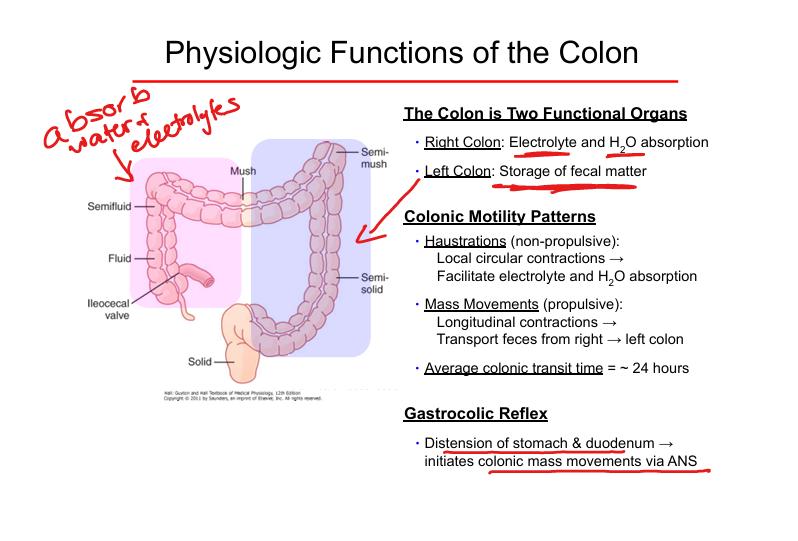
Haustrations
Non‑propulsive mixing contractions.
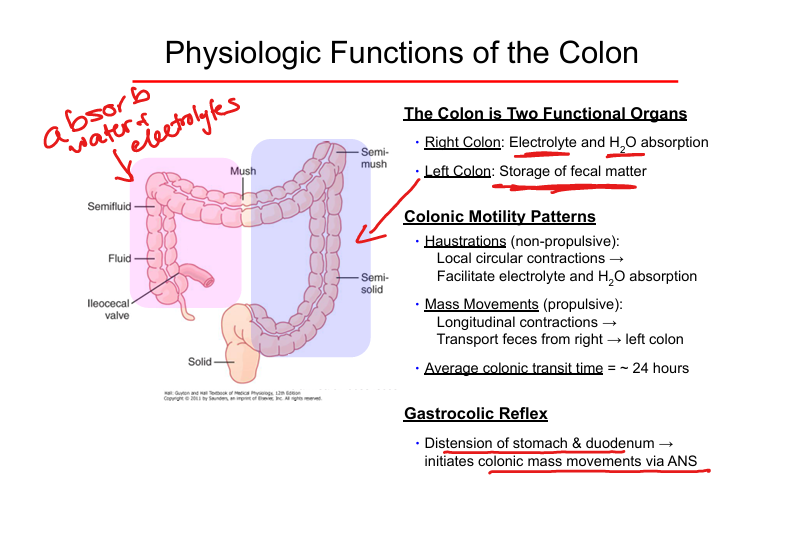
Gastrocolic reflex
Stomach distension triggers colonic mass movements.
Ileocecal Valve resection effects
Diarrhea, Small Intestine Bacterial Overgrowth (SIBO), loss of ileal brake. (often due to cancer or crohn’s disease)
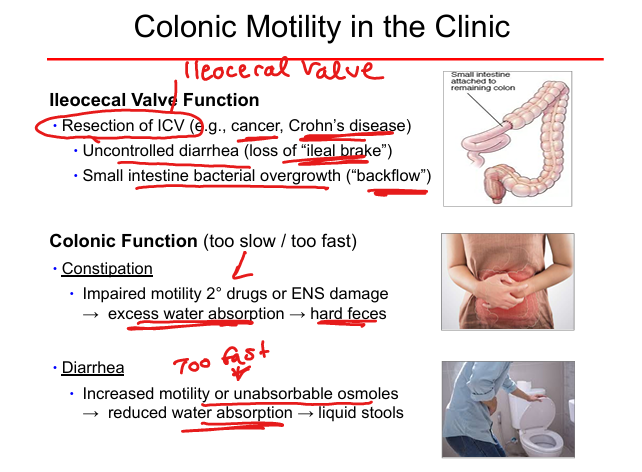
Constipation mechanism
Slow transit, ENS damage, excessive water absorption.
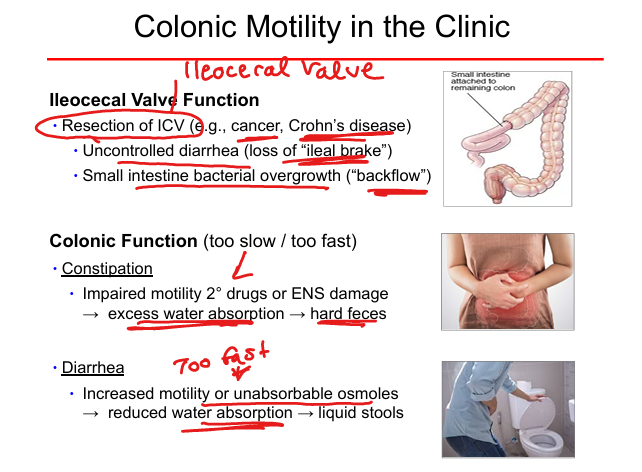
Diarrhea mechanism
Fast transit or unabsorbable osmoles.
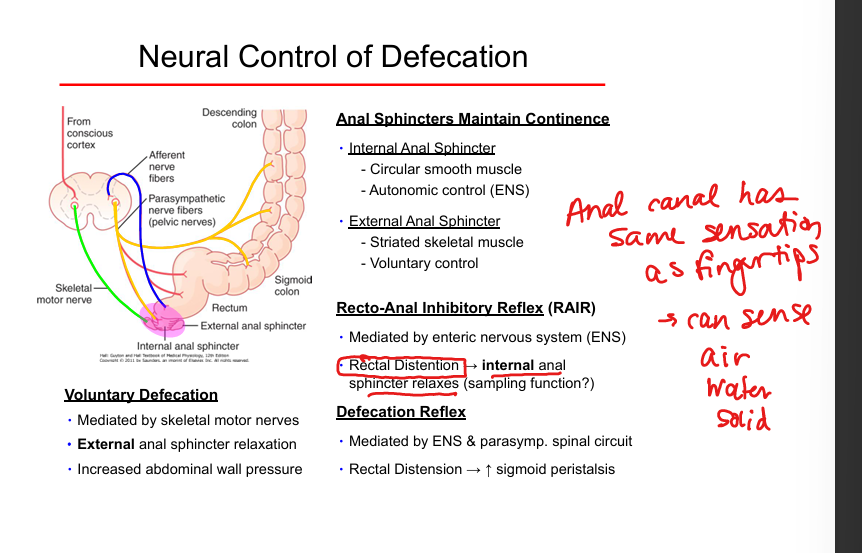
Recto‑anal inhibitory reflex (RAIR)
Rectal distension → Internal anal sphincter relaxation.
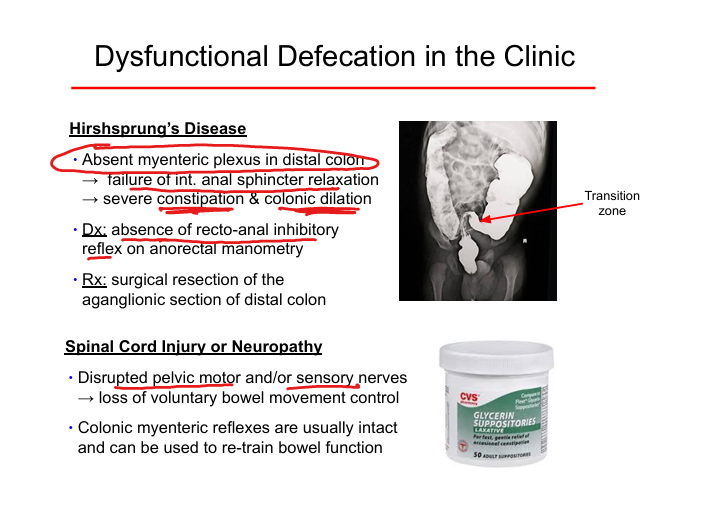
Hirschsprung disease
Absent myenteric plexus in distal colon → no recto-anal inhibitory reflex(no internal anal sphincter relaxation) → severe constipation.
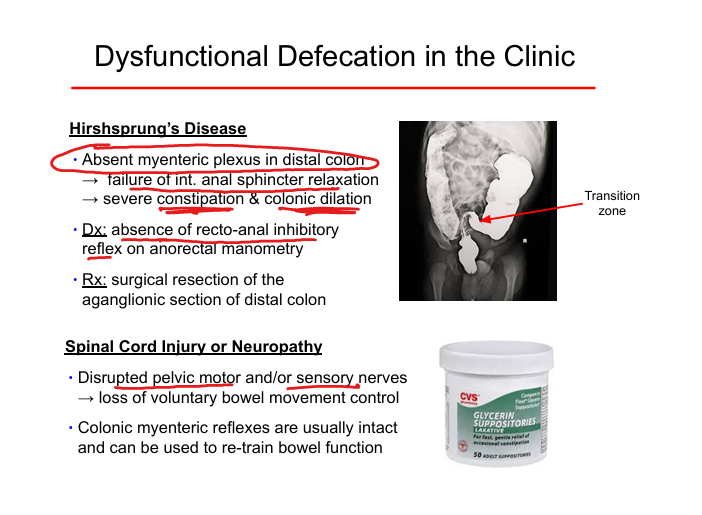
Spinal cord injury effect
Loss of voluntary control due to disrupted pelvic motor/sensory nerves; ENS reflexes intact; bowel retraining possible.
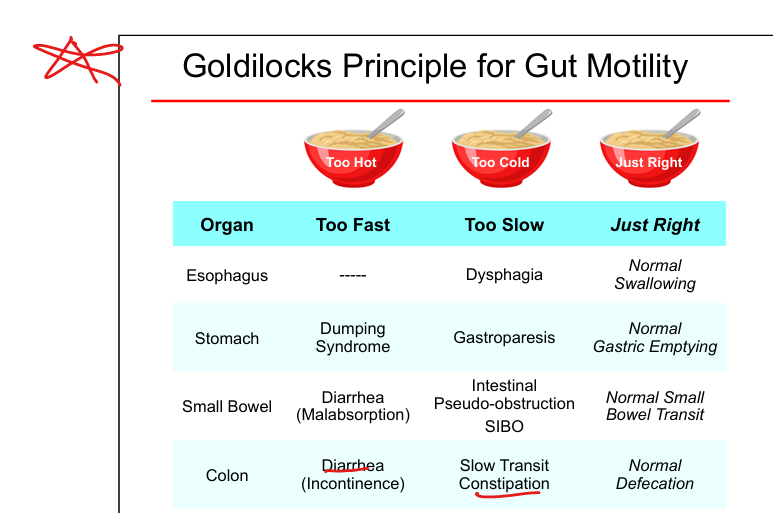
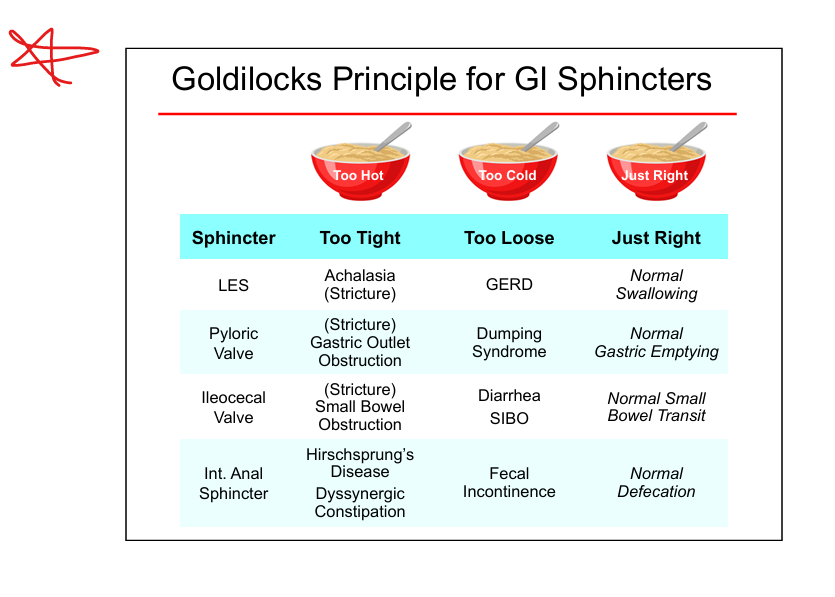
Goldilocks: LES
Too tight = achalasia; too loose = GERD.
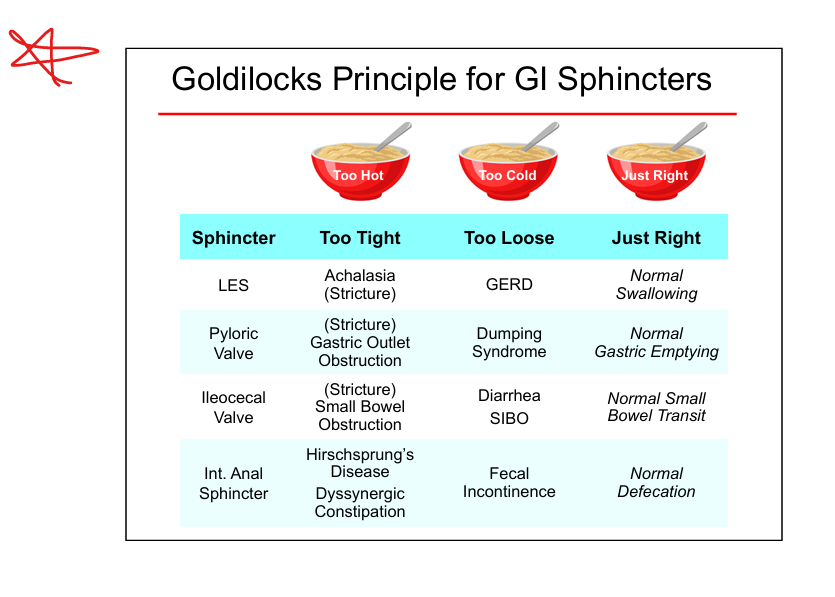
Goldilocks: pylorus
Too tight = gastric outlet obstruction; too loose = dumping syndrome.
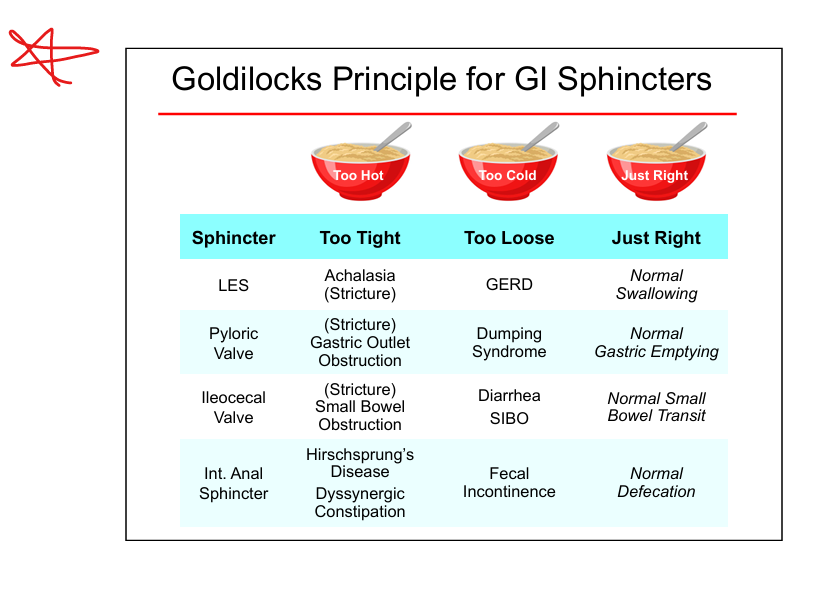
Goldilocks: Ileocecal valve
Too tight = SBO; too loose = diarrhea/SIBO.
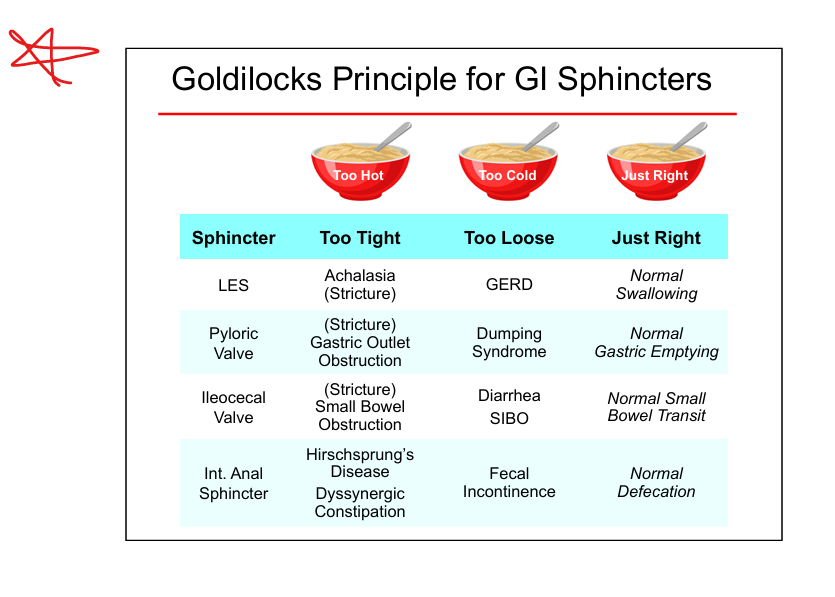
Goldilocks: internal anal sphincter
Too tight = Hirschsprung/dyssynergia; too loose = incontinence.
Too fast = dumping syndrome; too slow = gastroparesis;
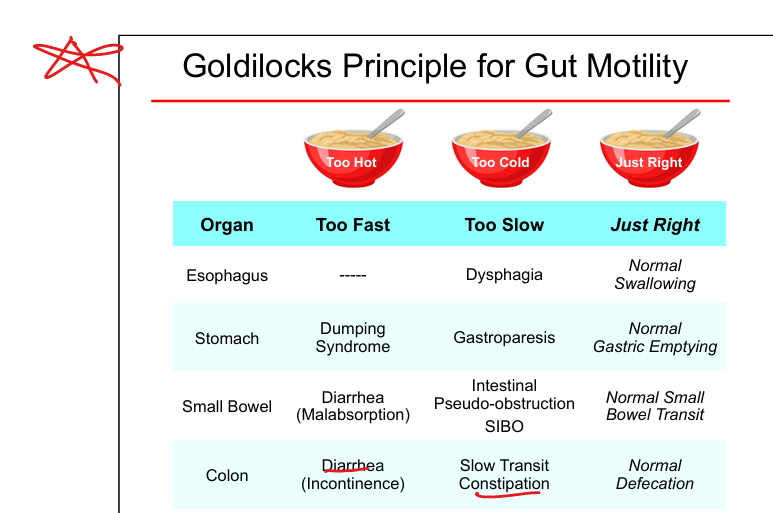
Too fast = diarrhea/malabsorption; too slow = pseudo‑obstruction/SIBO;
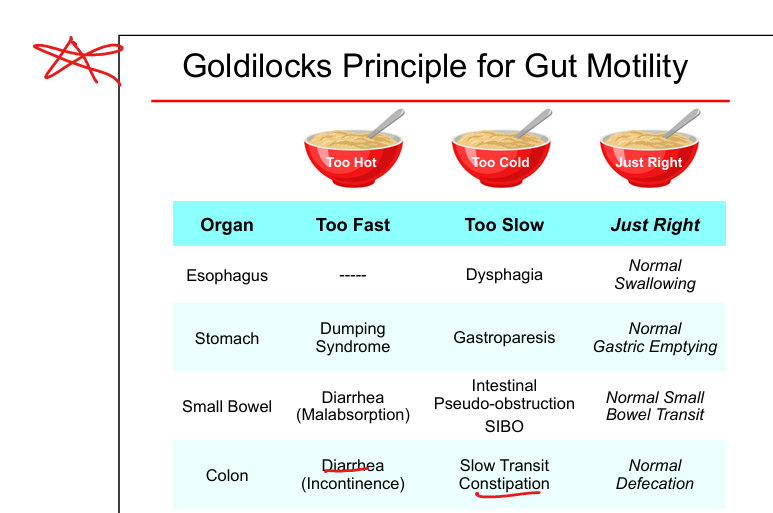
Too fast = diarrhea/incontinence; too slow = slow‑transit constipation;
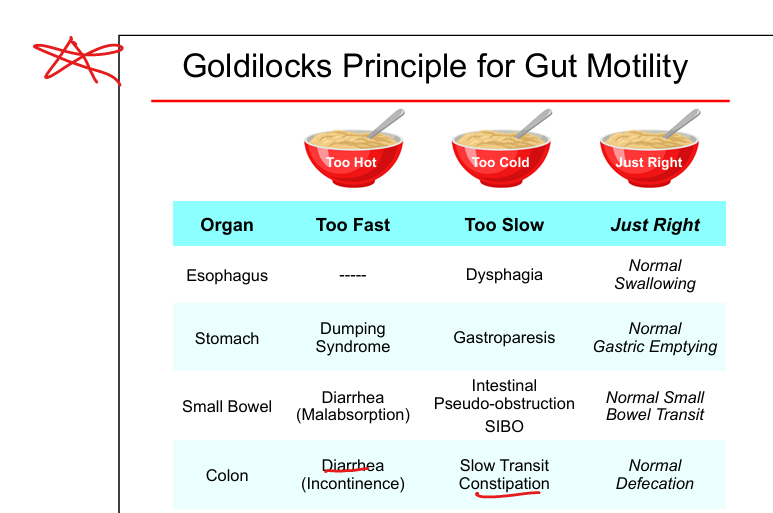
Too slow = dysphagia; too fast is uncommon;