MMSC 409 exam 1
1/164
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
165 Terms
immunohematology
the study of the immune aspects of hematology to provide safe therapeutic blood products to patients
-antigens, antibodies, agglutination, hemolysis and blood groups
antigen (Ag)
a substance that is recognized by the body as being foreign, which causes an immune response
-in blood banking Ags are mainly (but not exclusively found on the RBC membrane
-the reaction of Abs against foreign Ags in transfused blood is a common cause of transfusion reactions
antibody (Ab)
a protein substance that is secreted by plasma cells in response to an antigen
-Abs will only respond to the Ag that they are sensitized against
-Abs are found in the serum
-commerical Abs can be used for lab testing
-donated blood needs to be screened for Abs that will cause an attack of recipient cells
hemolysis
the disruption of the RBC membrane, causing release of hemoglobin into the plasma
-lysis of RBCs
-immunological transfusion reactions in the body can cause this process to occur
agglutination
the clumping of RBCs (or other particulate) due to interaction of antibodies with their corresponding antigen
-clumping that is caused by the interaction of antibodies
accuracy in blood banking
it is important that testing in blood banks and transfusion labs are 100% accurate to avoid severe transfusion reactions due to incompatability
-donated blood units need to be typed properly to ensure they are given to the right patient
-recipients need to be typed properly to ensure they recieve the correct units of blood
blood test at donor collection facility
-ABO and Rh typing
-infectious disease testing: syphillis, hepatitis B & C, AIDS/HIV, HTLV I & II, west nile virus, Chagas disease (T. cruzi)
-ABO and Rh types reconfirmed
blood test at transfusion center
-reconfirmation of ABO type (make sure it matches the label)
-pre-transfusion testing on patient: ABO, Rh type, antibody screen, crossmatch
American Red Cross (ARC)
provides many benefits to members
-disaster relief
-rare donor registry (find rare blood types)
-reference alb services
Food and Drug Administration (FDA)
regulates all blood component manufacturers, distributors and medical laboratories in the US
-provides licensure to all blood collection centers, and approves all methods and products used for blood collection
-blood and blood products are pharmaceutricals and biologics
-center for biological evaluation and research (CBER) functions under them to control blood collection and manufacturing of pharmacueticals
AABB
-write stands that blood collection centers and transfusion centers must follow for testing
-voluntary accreditation of either people or facilities
-writes technical manuals
-ensures that standards for CMS (medicare and medicaid) are met
college of American pathologists (CAP)
-voluntary accreditation of clinical laboratories
-administer proficiency testing for clinical laboratories
Joint Comission
offer voluntary inspection and accreditation of institutions or specific units within an institution
past blood banking issues
-multiple blood groups: even with knowing about ABO there were still transfusion reactions going on that lead to discovery of other blood groups
-circulatory overload: people who only needed 1 component of blood were given whole blood that gave an overload of cells and volume, leading to production of apheresed products
-blood storage and expiration: blood that was collected would expire really quickly so research was need to figure out what would extend the shelf life
RBC membrane
-phospholipid bilayer containing glycolipids and immunoproteins
-semipermeable
-integral proteins extend from the outside through the bilyaer and into the cytoplasm
-peripheral proteins are present on internal side of the bilayer forming the cytoskeleton
-protein cytoskeleton is a mesh that supports the bilayer
-spectrin is present in cytoskeleton and promotes flexibility of the RBC
spectrin
an important protein the cytoskeleton of RBCs that is phosphorylated by ATP so that the cell remains flexible
deformability
flexibility of the RBC membrane
-spectrin proteins are responsible for keeping RBC flexible
-RBCs need to be flexible so they are able to pass through small blood vessels
-RBCs that lose this ability (low ATP= nonfunctional spectrin) will be broken down in the spleen
permeability
ability of molecules to pass in and out of the RBC membrane to maintain Na+ and K+ concentrations
-ATP powered pumps transport K+ into the cell and Na+ out of the cell
-if ions become imbalanced (low ATP=non functional pumps) the cells become dehydrated and rigid and are removed from circulation
hemoglobin
protein in RBCs composed of 2 alpha chains and 2 beta chains that is responsible for gas exchange
-carries O2 to tissues
-when B chains spread apart it allows 2,3 DPG to bind and causes release of O2 from the protein and into the tissues
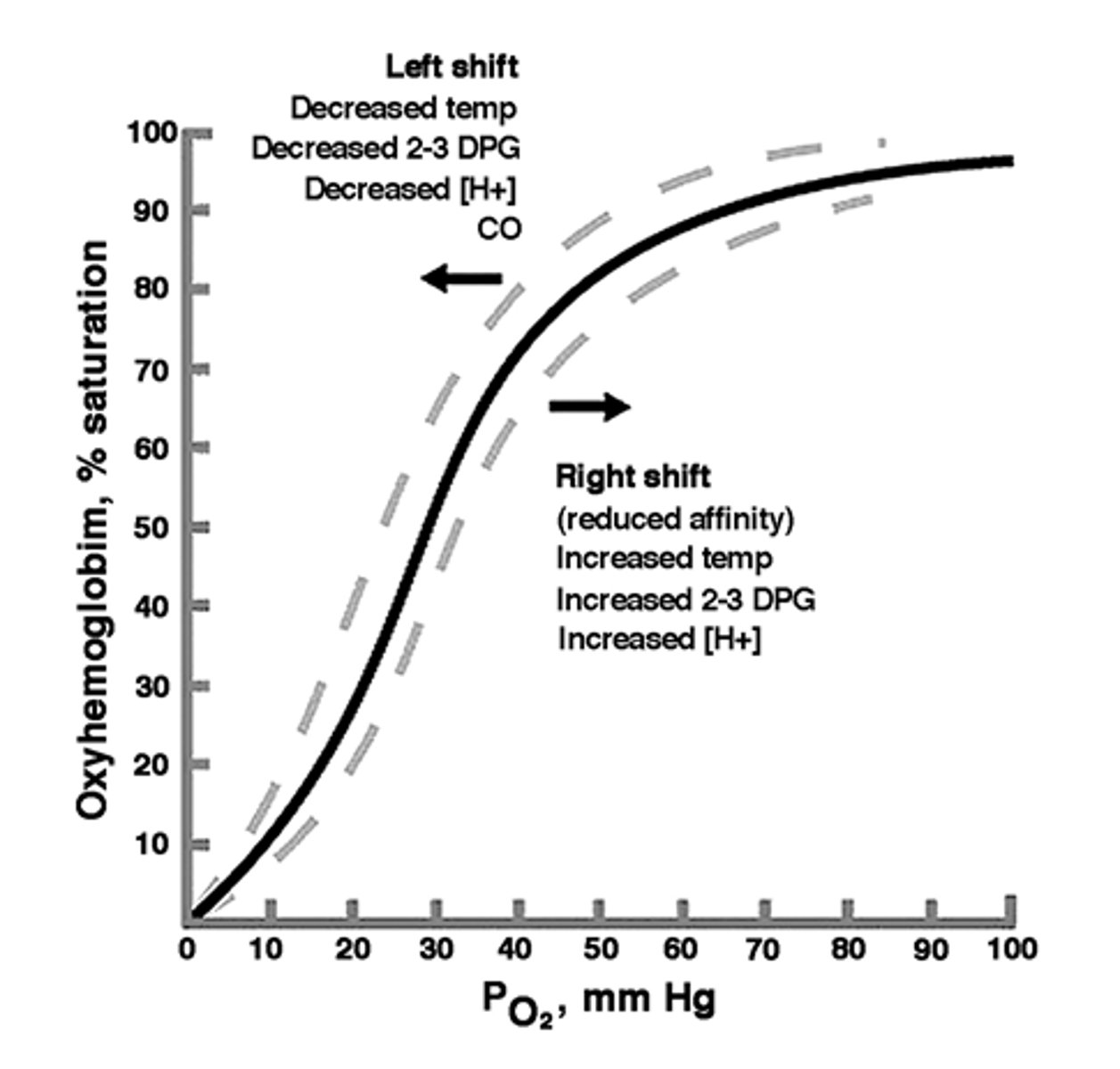
oxygen dissociation curve
a graph that associates the % saturation of oxygen on the hemoglobin molecule with a particular pressure of O2
-the % of oxygen that is being released into tissues is equal to 100% minus the % oxygenation of hemoglobin (the amount of O2 the hemoglobin holds on to)
2,3 DPG
a molecule that binds to the beta chains of oxyhemoglobin and forces the oxygen on the hemoglobin to be released into tissues
-high concentrations will increase O2 delivery to tissues
-low concentrations will decrease O2 delivery to tissues (increased O2 carrying capacity of hemoglobin)
right shift
MORE oxygen delivery to tissues
-hemoglobin is more weakly bound to O2 (decreased oxygen carrying capacity)
-high temperatures
-high 2,3 DPG
-low pH (acidic)
left shift
LESS oxygen delivery to tissues
-hemoglobin is more strongly bonded to oxygen (increased oxygen carrying capacity)
-low temp
-low 2,3 DPG
-high pH (basic)
left (fill in the blank)
stored blood can undergo a (left or right) shift of the oxygen dissociation curve due to the fact that 2,3 DPG has been depleted during storage
-causes decreased delivery of oxygen to tissues
additive solutions
additive solutions are used with RBCs to keep them viable after they have been removed from plasma and offer other benefits
-longer shelf life: provide nutrients so RBCs are able to survive longer
-production of more products: removing RBCs from whole blood and storing them in solution makes it possible for platelets and plasma to be used as separate therapies
-easier transfusions: RBCs that are in solution instead of plasma is less viscous and easier to transfuse than whole blood
anticoagulant
additive that is used to store RBCs and prevent clotting
ACD-A, CPD, CP2D
anticoagulants that are used for storage of RBCs in whole blood
-contain citrate, monobasic sodium phosphate and dextrose
-expiration: 21 days
-store at 1-6 C
citrate (sodium citrate or citric acid)
an ingredient of anticoagulants which chelates calcium to prevent clotting
monobasic sodium phosphate
a buffer that is present in anticoagulants to maintain storage levels of 2,3 DPG so that stored RBCs maintain their ability to deliver oxygen
dextrose
an energy substrate that is present in anticoagulants to provide a substrate for glycolysis so stored RBCs maintain ATP production (remain flexible and able to maintain electrolyte concentrations)
CPDA-1
anticoagulant solution used to store RBCs in whole blood for extended time
-contains sodium citrate, monobasic sodium phosphate and dextrose
-expiration: 35 days (increased time is a big benefit)
-storage 1-6 C
adenine
an additive to anticoagulant solutions that allows for increased production of ATP in stored RBCs
-allows for longer storage times
AS-1, AS-5, AS-7
additive solutions used to store RBCs
-contains mannitol, saline, adenine and glucose
-expiration 42 days
mannitol
additive solution ingredient that protects against hemolysis in stored RBCs
-present in AS-1, AS-5 and AS-7
AS-3
additive solution that is used for storage of RBCs
-contains citrate & phosphate, saline, adenine and glucose
-expiration: 42 days
citrate and phosphate
2 ingredients that are used together to prevent hemolysis of RBCs in additive solution
-used in AS-3
storage lesion
a loss of viability and function due to biochemical changes that occur in stored blood
storage lesion (RBCs)
-% of viable cells decrease
-glucose and ATP decrease
-lactic acid increases, leading to more acidic pH
-2,3 DPG decreases, leading to left shift in O2 dissociation curve (less oxygen delivery to tissues)
RBC lifespan
120 days
fetal (fill in the blank)
________ hemoglobin has a higher affinity for O2 than adult hemoglobin
-this means that it binds O2 more stably, and does not release it into tissues as easily
expiration of whole blood
35 days
methemoglobin
hemoglobin that is in the ferric state and can no longer carry O2
-undergoes methemoglobin reductase pathway to go back to ferrous state an be able to carry oxygen again
donor interview
is conducted to promote the safety of the donor and the recipient
-history and personal info screening are taken via UDHQ (uniform donor history and ID verification)
-ID of the donor is obtained
-required educational info provided to donor
-physical exam is given (general appearance, BP, HR, Hgb/ Hct)
weight for heterologous donation
110 lb
temperature for heterologous donation
37.5 C / 99.5 F or lower
pulse for heterologous donation
50-100 BPM
blood pressure for heterologous donation
180/100 or lower
hemoglobin (Hgb) for heterologous donation
-male: 13 g/dL or higher
-female: 12.5 g/dL or higher
hematocrit (HCT) for heterologous donation
38% or higher
questions to protect donor
-time period since last donation
-past deferral for reasons of their own health (vitals out of range that would endanger their health)
-health history: surgery in the last 12 months, history of heart/lung/ liver disease, history of cancer, abnormal bleeding tendencies, unexplained weight loss
-medications: drugs, meds, antibiotics, aspirin in the last 3 days
-pregnancy in the last 6 weeks/ ever
questions to protect recipient
-permanent deferrals
-indefinite/ permanent deferrals
-temporary deferrals
permanent deferral
confirmed HBsAg test (confirmed hepatitis B)
indefinite/ permanent deferral
-hepatits or AIDS
-antibodies to hepatitis B (anti-HBc)
-hepatitis C infection
-tests positive for HIV, HCV, HTLV or T. cruzi
-previous donation that gave recipient hepatitis or AIDS
-sexual risk of AIDS (sex workers, gay men)
-IV drug abuse
-CJD risk factors (brain tissue transplant, use of bovine insulin, receive HGH)
-parasitic infections (babesiosis, Chagas disease, Leishmaniasis)
-leukemia or other cancers
-Tegison medication (causes birth defects)
5 year deferral
cancer in the last 5 years
3 year deferral
-malaria
-immigrant from malaria endemic country
-acitretin (causes birth defects)
12 month deferral
-recipient of blood/ blood products/ clotting factors
-close contact with viral hepatitis or AIDS
-sexual partner of someone on permanent deferral
-inmate of prison/ mental institution
-needlestick exposure
-HbIG recipient (given in cases where HBV is a high risk)
-piercings/ tattoo
-accupuncture
-treatment for syphilis or gonorrhea
-travel to malaria endemic country
-rabies shot
-transplant or graft recipient
-cocaine use
4 week deferral
-german measles (rubella) immunization
-proscar & accutane (birth defects)
2 week deferral
immunizations for small pox, measles (rubeola), mumps, yellow fever or polio (SABIN)
whole blood collection
-select collection bag with desired anticoagulant
-ensure proper ID of patient
-prepare venipuncture site: scrub with iodine (clears normal flora of skin) and let dry completely
-draw donor blood
-mix blood and anticoagulant constantly (can be done by machinery)
-do not leave donor unattended
-when sufficient volume has been collected, draw pilot tubes of blood
-make integral segments
-give donor post-collection instructions
donor processing tests
-ABO typing: forward and reverse type
-Rh type: weak D test
-serum antibody screen: manufactured pooled screening units are used on donor units to look for clinically significant non-BO Abs
-if there are clinically significant Abs present, use the RBCs and discard plasma that contains the Abs
infectious disease tests (donor processing)
-hepatitis B and C
-HTLV I and II
-HIV
-syphilis
-west nile virus
-ALT
-T. cruzi
-zika virus
-CMV (positive units can be used just not on immunocompromised)
viral marker tests that require confirmation
if the test is positive will repeat and then use a followup test
-HBsAg: if positive use inhibition test
-anti HIV1: confirm with western blot or gel electrophoresis
-any test that is positive will be retested (not necessarily with a different follow up)
donor unit label
-volunteer or paid donor
-component contained inside (RBCs, plasma, etc.)
-ABO and Rh
-unusual test results of the unit
-anticoagulant type and amount
-volume of blood
-ISBT donor number (country, collection site, year and number of collection all included by this)
-expiration date
-storage temp
-instructions/ precautions for use
autologous blood donation
donation of blood unit for yourself
-donor and recipient are same person
-blood collected for future use in surgery (preoperative collection) of elective surgeries
-can be done if someone has a rare blood type
autologous donation requirements
-prescription from physician
-no weight limit, can do low volume collection if < 100 lb
-no age limit
-Hgb: at least 11 g/dL
-HCT: at least 34%
-time period: 3 days since last donation
autologous donation donor processing
-ABO and Rh testing to confirm that types match
-1st unit (if many are collected) will be tested for hepatitis B and C, syphilis and HIV (if positive label as biohazard)
-labeling is the same as heterologous, but says "for autologous use only"
directed donor blood donation
the recipient of the blood chooses the donor
-done for elective surgery if recipient cannot donate blood for themself
directed donor requirements
-ABO and Rh compatibility of donor and recipient
-donor meets physical and history requirements for heterologous donation
-need prescription
directed donor donor processing
-same tests are performed as heterologous donation
-labeled normally with " for designated recipient" with recipient's ID
irradiation
a process that is used to inactivate any remaining WBCs (lymphocytes) that are present in a directed donor blood donation
-prevents transfusion associated graft vs. host disease
-required for 1st or 2nd degree relatives
apheresis
a method of blood collection in which whole blood is withdrawn, a desired component is separated and retained and the remainder of the blood is returned to the donor
apheresis types
-plateletpheresis: platelets are collected
-leukapheresis: granulocytes
-plasmapheresis: plasma
-erythrocytapheresis: RBCs
-HPC apheresis: hematopoietic progenitor cells
apheresis requirements
-meets all criteria for heterologous donation
-sufficient time since lsat donation
-no bleeding/ fluid retention problems
-asprin free for 3 days
-platelet count above 150,000 per uL
-WBCs above 4,000 per uL
-serum protein 6 g/dL or higher
double red donation requirement
-male: 130 lb, 5 ft 1 in
-female: 150 lb. 5 ft 5 in
-HCT: 40% or higher
heterologous whole blood donation frequency
8 weeks
-RBC mass needs to be replenished
autologous whole blood donation frequency
3 days (as long as hemoglobin is fine)
double red cell donation frequency
16 weeks
-RBCs need to replenish
plasmapheresis donation frequency
4 weeks
-plasma protein levels need to return to normal
plateletpheresis donation frequency
at least 2 days
-count must be over 150,000 / uL again
gene
unit of inheritance within a chromosome
locus
specific location of a gene within a chromosome
-the site on the chromosome where the gene is present
allele
one of 2+ alternative forms of a gene that can occupy the same locus on a chromosome
-e.g. E and e are alleles for the same locus
homozygous
the same allele is expressed twice
-the same allele was inherited from both parents
-E+ e- or E- e+ would indicate the person has only one of the possible alleles
heterozygous
two different alleles are expressed for the same gene
-different alleles were inherited from each parent
-E+ e+ would indicate the person has both of the possible alleles
genotype
the genetic makeup of a person
-e.g. if the person is Ee or EE or ee
phenotype
the observed expression of a gene
-e.g. if the person is Tt and the T is dominant and expressed and t is recessive not expressed then only the T phenotype is seen
codominance
RBC genes are codominant and therefore the phenotype that is observed is a direct representation of the phenotype
dominant
a trait that will be expressed in the offspring even though it is carried in only one of the homolgous chromosomes
-does not apply to blood genetics
recessive
a gene that in the presence of a dominant allele does not get expressed
-expression only occurs in the homozygous state
-does not apply to blood genetics
codominant traits
a pair of alleles where neither is dominant to the other, therefore they are both expressed
-most of the antigens in blood groups follow this inheritance pattern
antigen dosage (dosage effect)
certain antibodies can have a very strong reaction when tested against a homozygous sample and have a weak or absent reaction when tested against a heterozygous sample
-antibodies give different reaction strength depending on the amount of antigen that is present on a RBC, which differs in homozygous and heterozygous individuals due to codominance of alleles
-e.g. anti-M on a homozygous MM sample will be 4+ agglutination, but will only be 2+ agglutination on a sample that is heterozygous MN
ABO genes
consist of 2 codominant alleles
-A: AO or AA
-B: BO or BB
-AB: AB
-O: OO
amorphic genes
"silent genes" that do not produce a detectable antigen
-the gene that codes for type O blood
-someone who is type AO only produces A antigens
-someone who is OO does not have ABO antigens
units to screen calculation
# units required/ (1- decimal frequency of antigen) * (1-decimal frequency of antigen)
T cells
-involved in cellular immunity
-use MHC molecule compatability to recognize foreign antigenic cells and eliminate them
-protect against viral, fungal and parasitic infections
-cause tissue graft rejection and protection against tumors
-respond to antigens on APCs
B cells
-involved in humoral immunity
-mature into plasma cells to secrete Abs
-have surface receptors that allow them to react to a specific Ag they come into contact with
antibody production
-APCs digest antigens into smaller segments
-Th cells interact with the APC and recognize the Ag
-Th cell activates a B cell to produce a plasma cell that produces Abs
-B cells can become memory B cell and patrol the body for the same antigen that it was sensitized against, and produce Abs again if encountered
innate immunity
nonspecific and nonchanging defenses against infection
-primary defense mechanisms (skin, mucous membranes, biochemical secretions, pH) prevent bacteria from entering the body
-secondary defense mechanisms (phagocytic cells, alternative and lectin pathway of complement, inflammation) help to fight infection in non-specific ways
acquired (adaptive) immunity
defense mechanisms that are able to change and respond to a specific infectious agent
-T cells (Th, Tm) and B cells (Bm and plasma) respond to specific antigens
-Abs form against specific Ags
-classical complement activation responds to Ag-Ab complexes and clears them out
alloantibody
antibodies produced after exposure to non-self antigens in the body
-WBC, platelet or other blood group Ag that are not present in a transfusion recipient that are introduced cause these antibodies to form
-can be a problem in transfusions when the Abs go down to undetectable levels in the plasma and second exposure leads to strong anamnestic response