Water Soluble Vitamins
1/134
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
135 Terms
Thiamin = Vitamin ____
Vitamin B1
Riboflavin = Vitamin ____
Vitamin B2
Niacin = Vitamin ____
Vitamin B3
Pantothenic acid = Vitamin ____
Vitamin B5
Pyridoxine = Vitamin ____
Vitamin B6
Biotin = Vitamin ____
Vitamin B7
Folate = Vitamin ____
Vitamin B9
Cobalamin = Vitamin ____
Vitamin B12
Ascorbic acid = Vitamin ____
Vitamin C
List all the B vitamins in order:
TRN Past Palmer on Brady For Coffee
Thiamin (B1) - methylation
Riboflavin (B2) - methylation
Niacin (B3) - methylation
Pantothenic acid (B5)
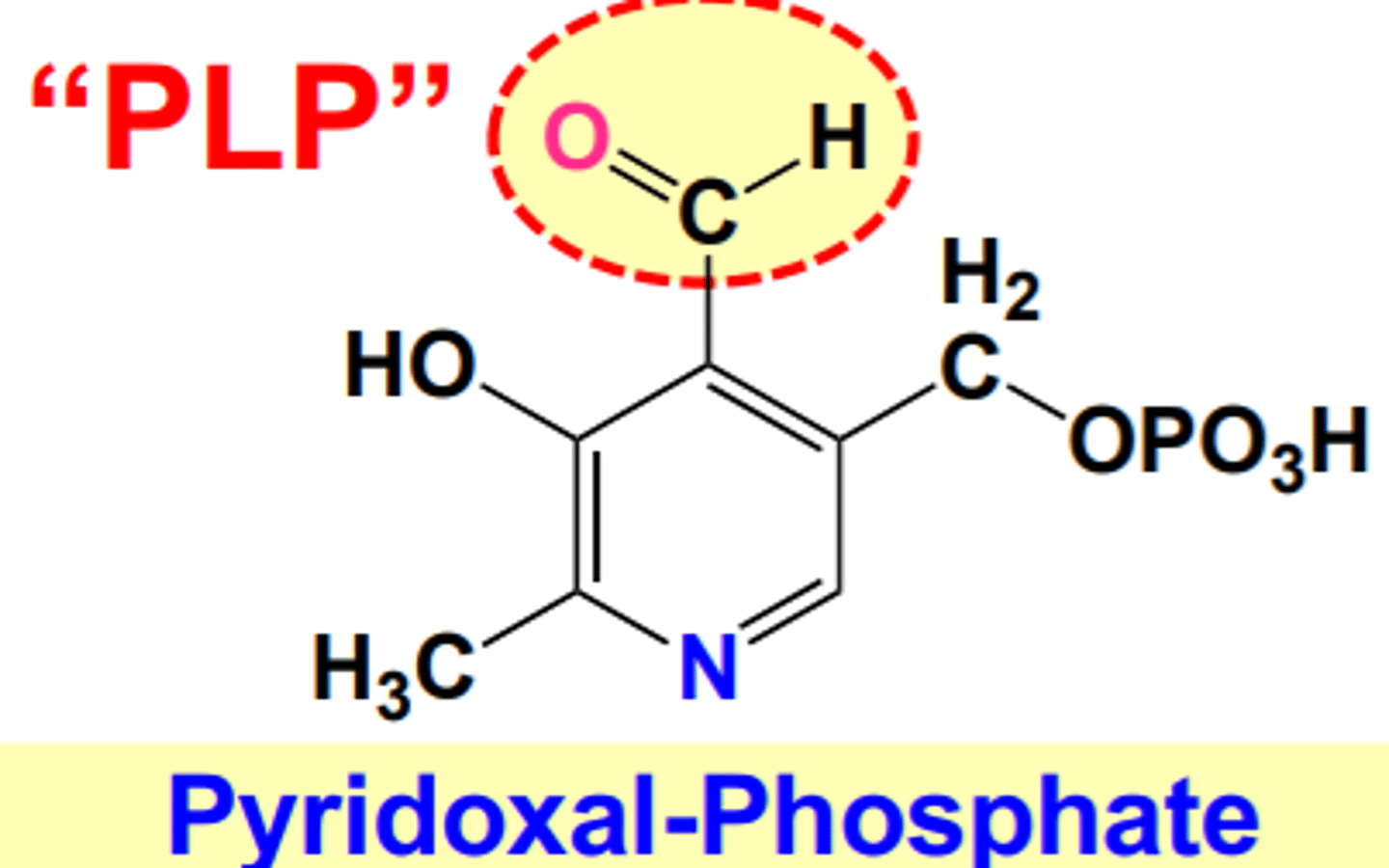
Pyridoxal phosphate (B6)
Biotin (B7)
Folate (B9)
Cobalamin (B12)
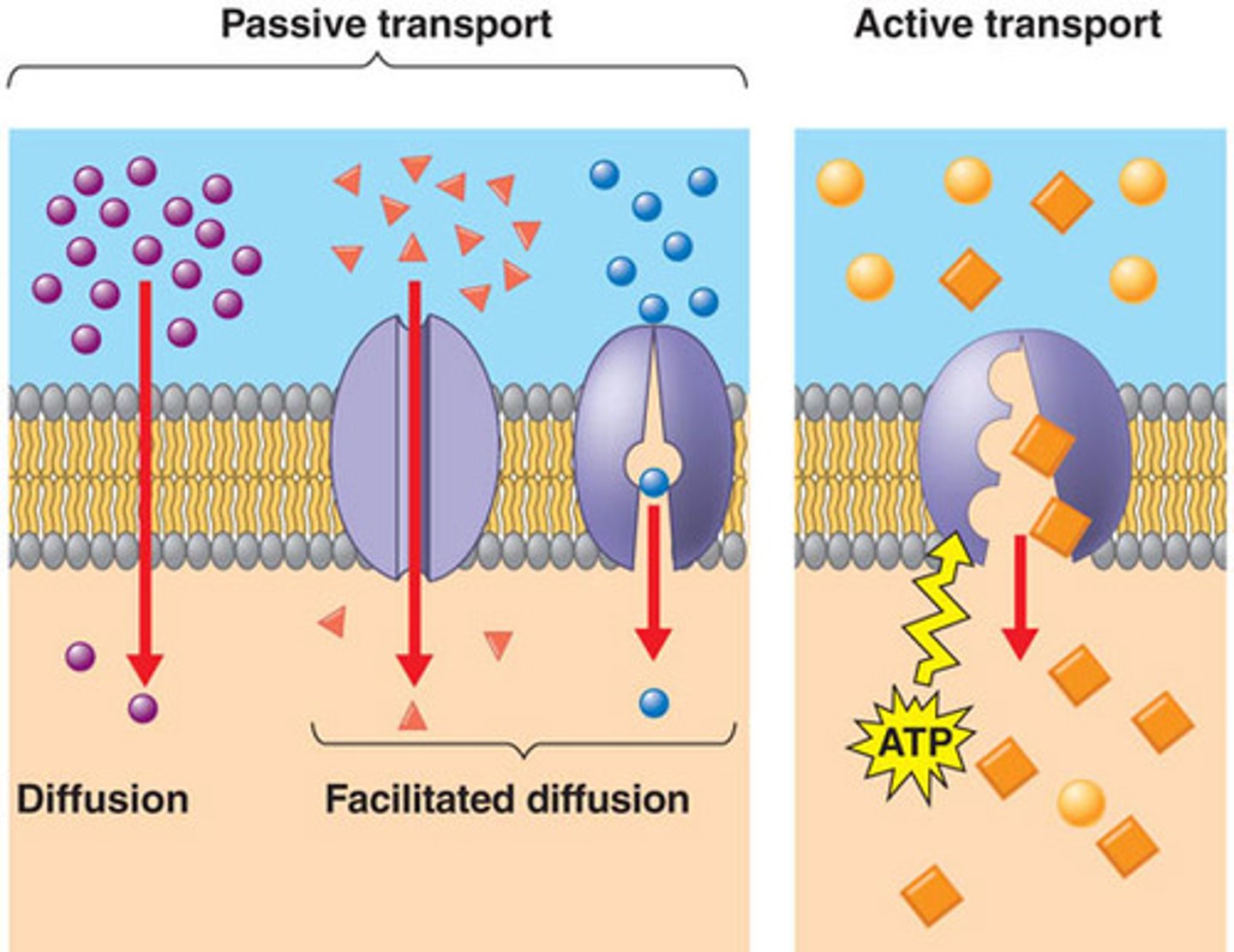
All water soluble vitamins, except B12 are absorbed via:
How is vitamin B12 absorbed?
Facilitated diffusion
B12 = Receptor mediated endocytosis
(T/F): All vitamins are absorbed more at higher one time doses.
False; vitamins are absorbed more at lower doses because it doesn't saturate carrier proteins
Water soluble vitamins are unstable due to:
1) Basic pH - vit. C, vit. B1
2) Water - vit. C, vit. B1, vit. B2
3) Heat - vit. C, vit. B1, vit. B5
4) Oxygen - vit. C
5) Light - vit. B2
6) Freezing - vit. B5
(Functions) Ascorbic acid (Vit C)
1) Antioxidant (donate H or electrons to reduce free radicals in cells)
2) Prevent nitrosamine formation; which are carcinogenic compounds in processed meat
3) Coenzyme; for absorption of non-heme iron & maintain iron and copper in reduced state
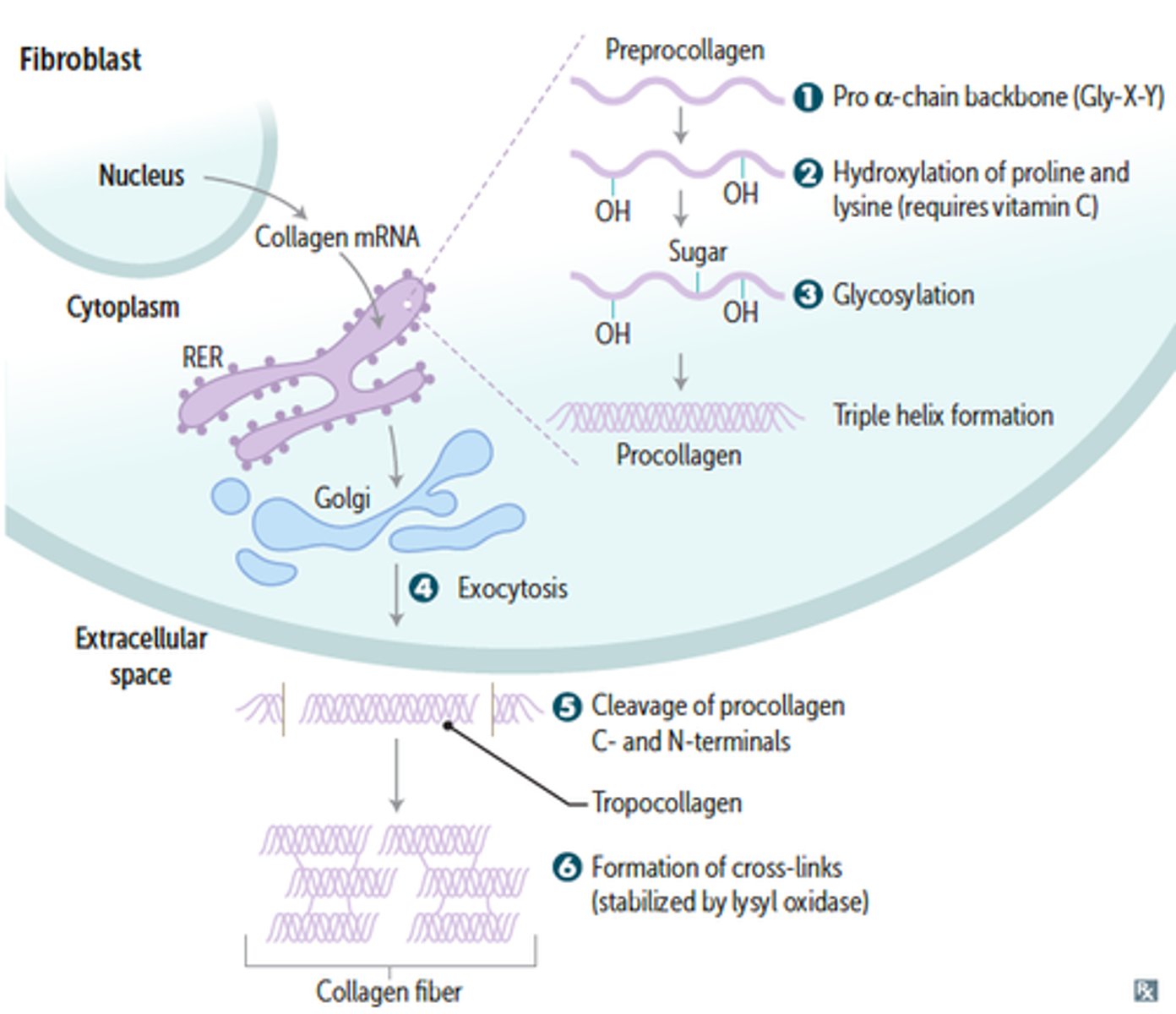
3) Coenzyme; for collagen synthesis via hydroxylation (proline & lysine --> hydroxyproline & hydroxylysine)
4) Required for conversion of dopamine to norepinephrine
5) Vit. C --> Vit. E (can regenerate vitamin E)
Vitamin E is found where in the cell?
Vitamin C is found where in the cell?
Vitamin E = Plasma membranes
Vitamin C = Cytosol the fluid part of cytoplasm
(T/F): Nearly ALL reactions use vitamin C to maintain either iron or copper in a reduced state in order for the enzyme to work.
True
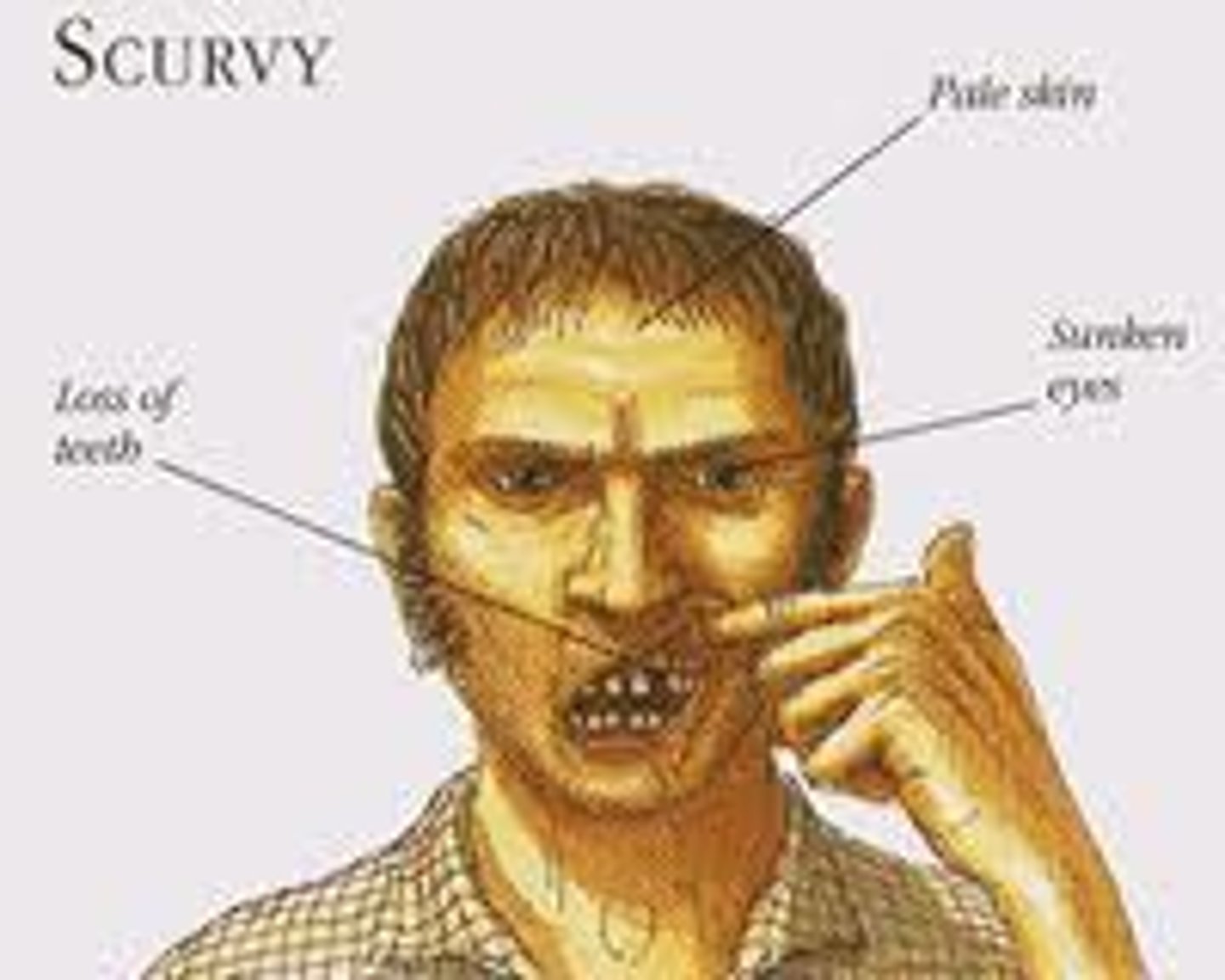
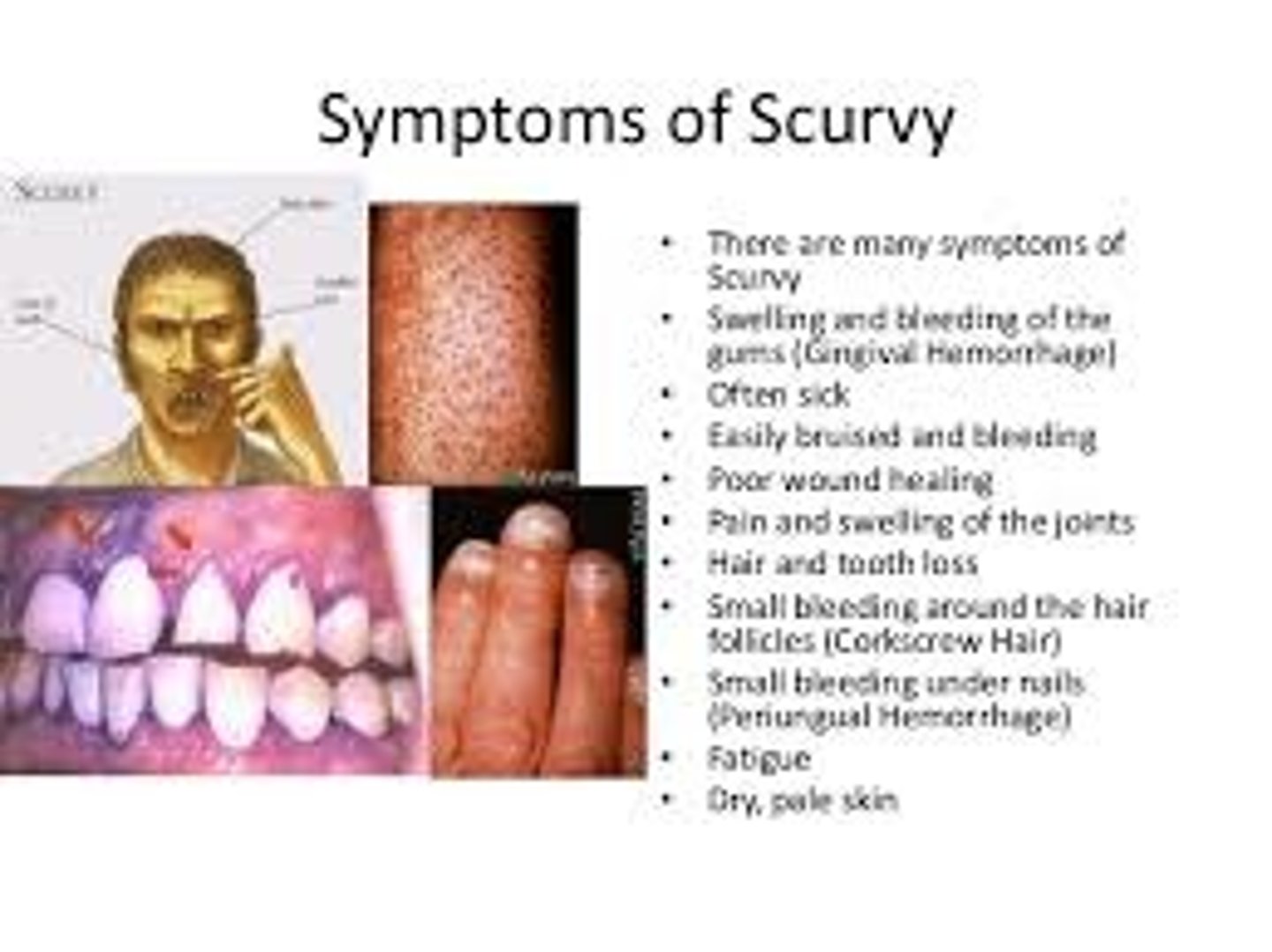
(Deficiency Name) Ascorbic acid (Vit C)
Scurvy
What are the four H's of Scurvy?
1) Hemorrhagic signs - poor wound healing
2) Hyperkeratosis of fair follicles - corkscrew hairs
3) Hypochondriasis - psychological manifestations
4) Hematologic - impaired collagen synthesis & decreased iron absorption

(Deficiency Symptoms) Ascorbic acid (Vit C)
1) Easy bruising
2) Pinpoint hemorrhages (Petechiae)
3) Bone fracture / Bone & teeth pain
4) Bleeding gums
5) Corkscrew hairs
(Toxicity Symptoms) Ascorbic acid (Vit C)
(Mainly from supplement use)
1) Osmotic diarrhea
2) Kidney disease - high vitamin c intake increases absorption of oxalate (kidney stones)
3) Impaired iron metabolism - iron toxicity
What are two contraindications for someone to supplement with vitamin C?
1) History of kidney stones
2) High iron levels
(Sources) Ascorbic acid (Vit C)
1) Bell peppers
2) Citrus fruits / fruit juices
3) Broccoli
4) Dark leafy green veggies

Vitamin C Requirements
Women = ____________ mg
Men = ____________ mg
Smokers = ____________ mg
Women = 75 mg
Men = 90 mg
Smokers = RDA + 35 mg
What population requires more vitamin C in their diet?
Smokers

What are the two types of Thiamin (B1)?
1) Thiamin Pyrophosphate (TPP) / Thiamin Diphosphate (TDP) - 80%
2) Thiamin Triphosphate (TTP) - 20%
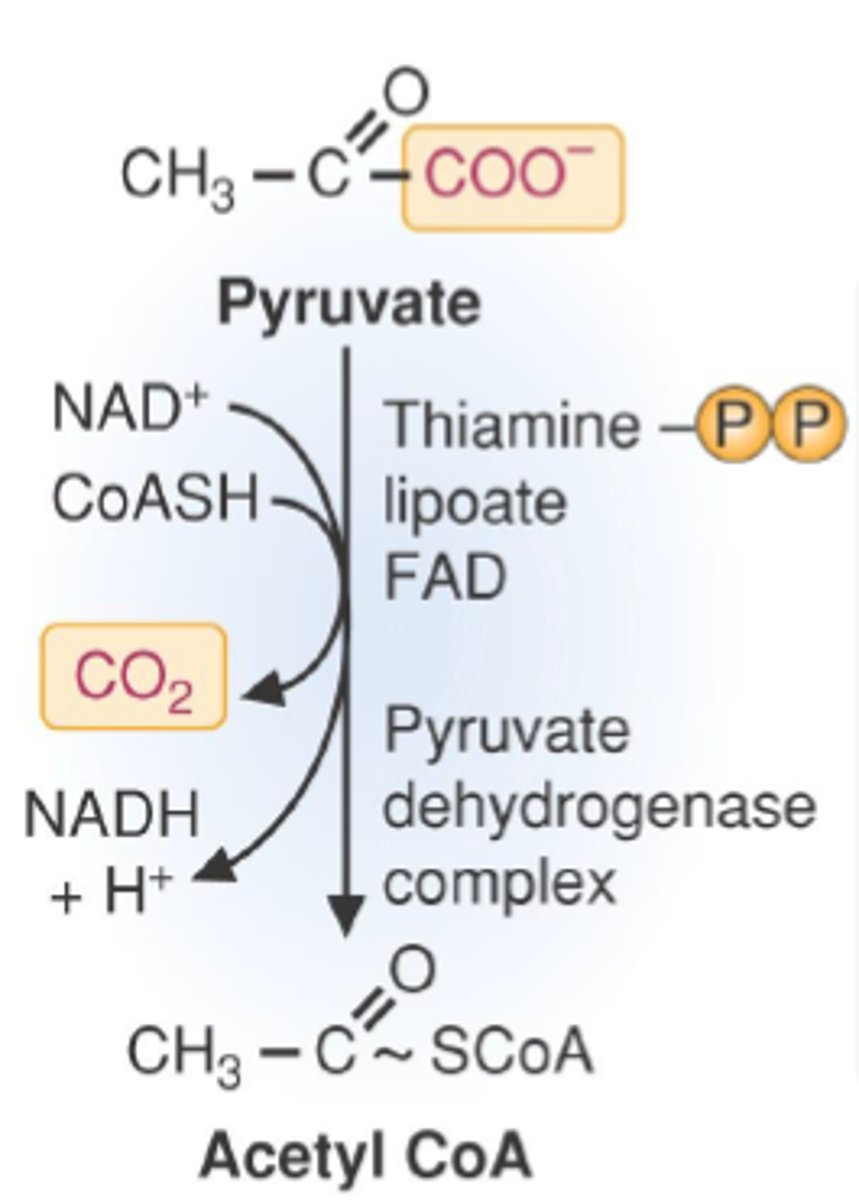
(Functions) Thiamin (B1)
1) Co-enzyme (TPP / TDP); energy production (pyruvate to acetyl CoA) dehydrogenase rxn
2) Non-coenzyme (TTP); Nervous system
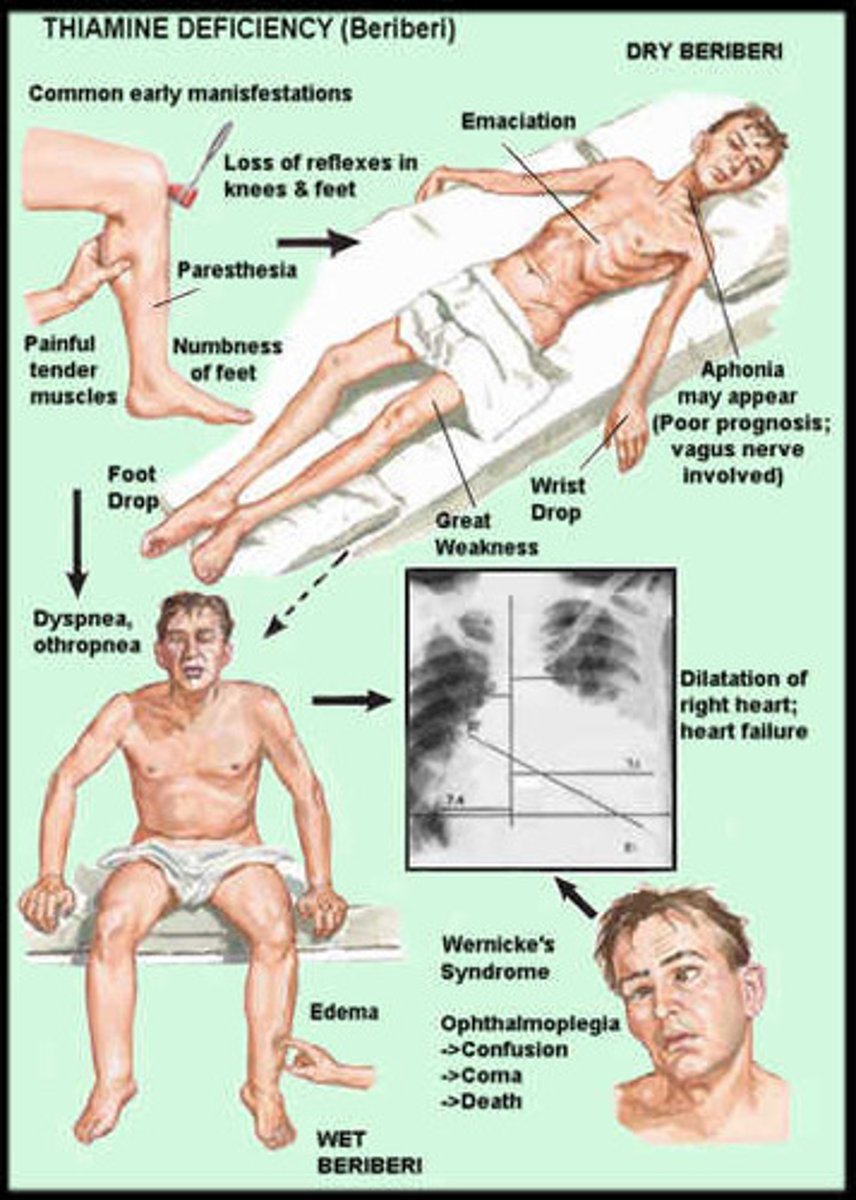
(Deficiency Name) Thiamin (B1)
Beriberi & Wernicke-Korsakoff syndrome
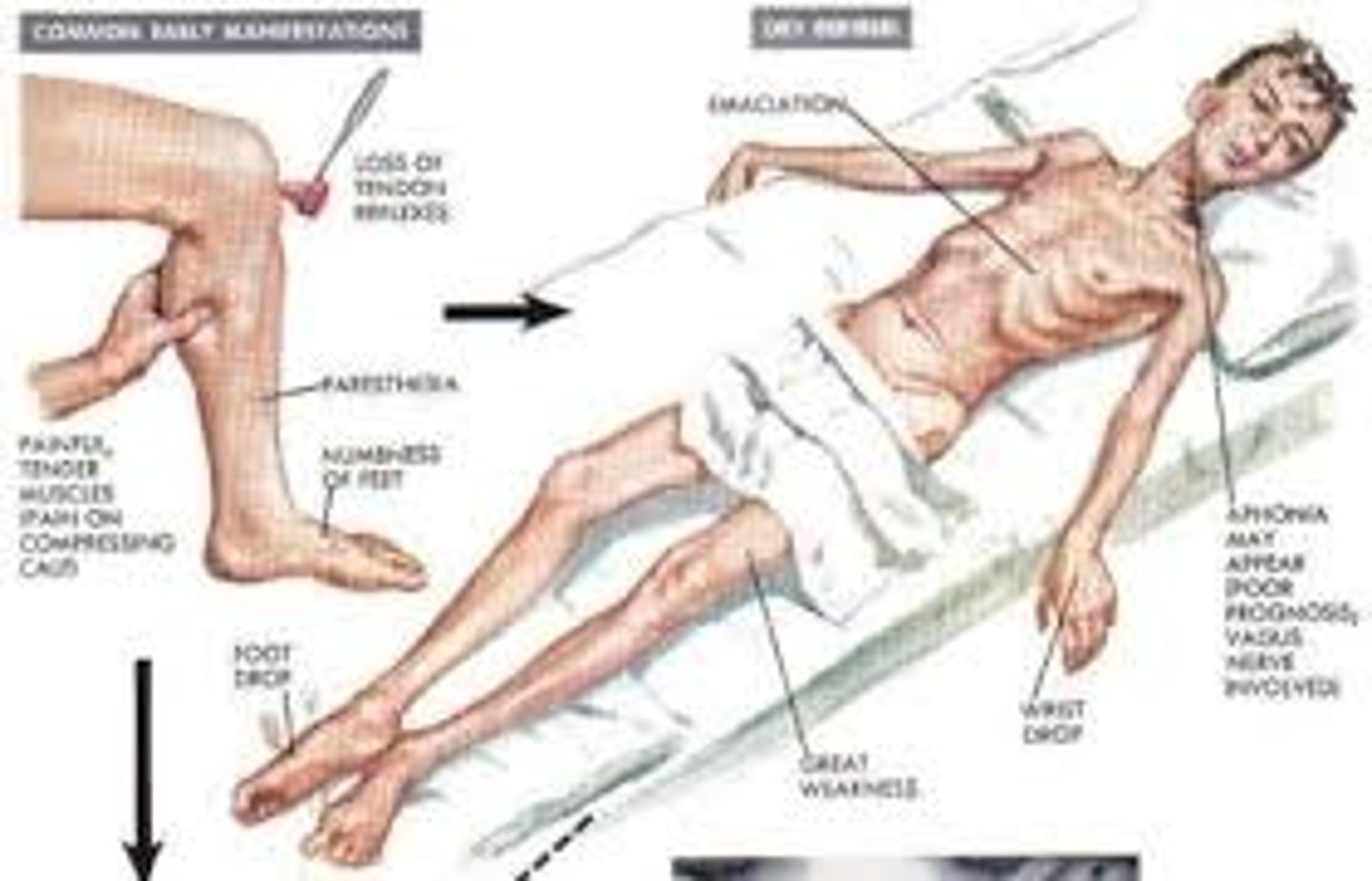
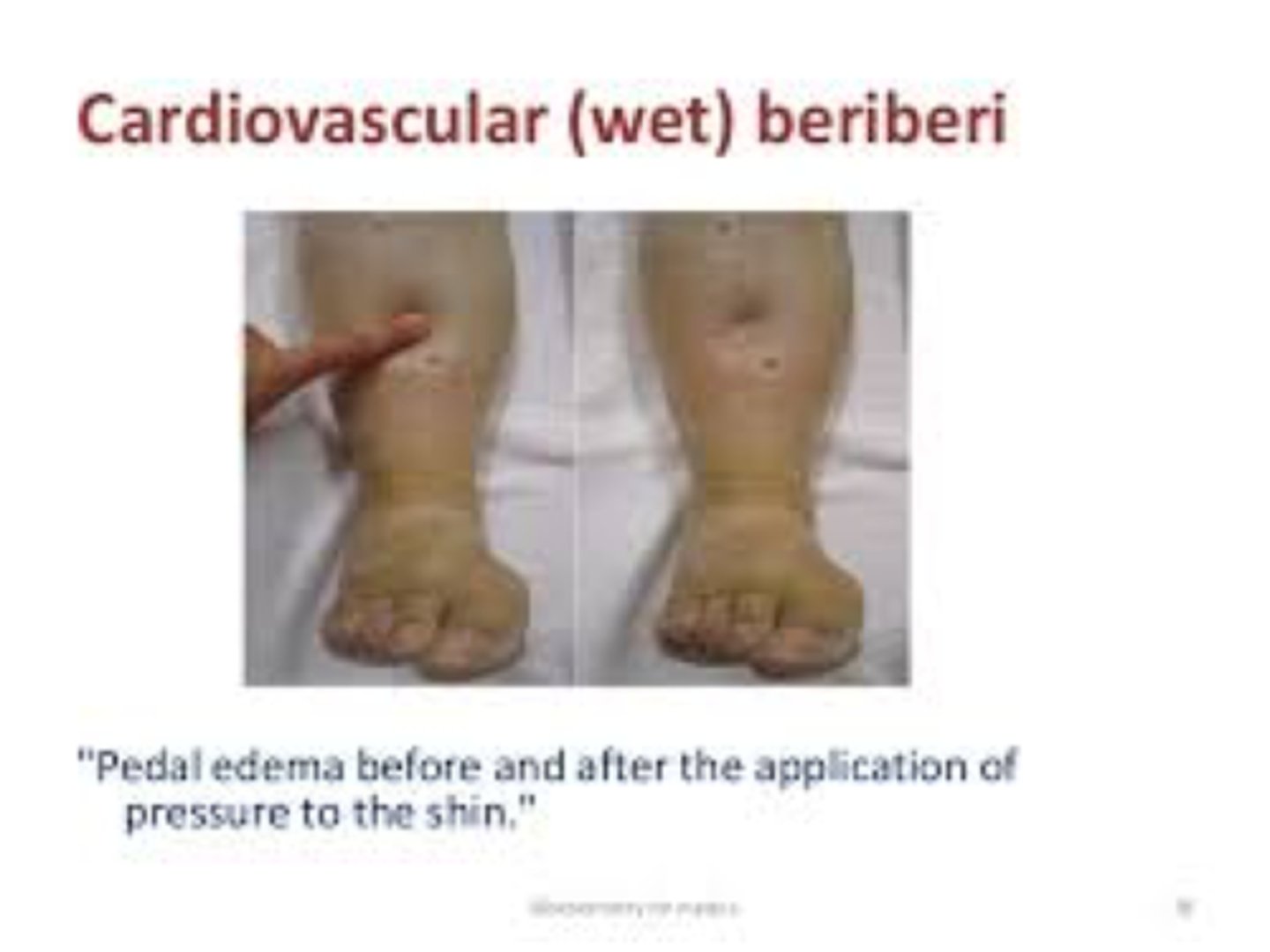
What are the three types of Beriberi?
1) Dry beriberi = peripheral neuropathy, bilateral tender calf muscles, symmetrical foot drop (often due to low thiamin + high carb intake)
2) Wet beriberi = enlarged heart, rapid heartbeat, peripheral edema, & high blood pressure
3) Acute beriberi = chronic infant deficiency* (2-5 months of age); breast fed mothers with poor thiamin intake
(Deficiency Symptoms) Thiamin (B1)
1) Peripheral nerves numbness and paralysis - Dry beriberi
2) Enlarged heart / Peripheral edema - Wet beriberi
3) Brain of infants - Acute beriberi
(Toxicity Symptoms) Thiamin (B1)
Rare
100x RDA given by IV
(Sources) Thiamin (B1)
1) Yeast
2) Meat, especially pork
3) Whole grains
4) Enriched cereals
5) Legumes

Anti-thiamin factors:
1) Water (thiamin absorbed and then lost in water)
2) Heat & basic pH
3) Raw shellfish and freshwater fish (thiaminases)
4) Tea, coffee, blueberries, red cabbage (Phenolic acids =. thiaminases)

What is Wericke-Korsakoff Syndrome?
Chronic thiamin deficiency in alcoholics (decreased thiamin intake, absorption, and utilization)
Symptoms: Psychosis, delirium, ataxia of gait & stance, Anorexia, vomiting, enlarged heart, tender calf muscles

What population(s) are at risk for Thiamin (B1) deficiency?
1) Alcoholics
2) Older adults (decrease absorption)
3) HIV/AIDs patients
4) Diabetics
5) Gastric bypass patients
What is the most common nutritional deficiency in alcoholics?
Thiamin (B1)
A patient that is a daily coffee consumer and who also loves to eat raw sushi is at a higher risk of ____________________ deficiency.
Thiamin (B1) deficiency, due to raw fish and coffee containing thiaminase compounds
Thiamin deficiency = Beriberi

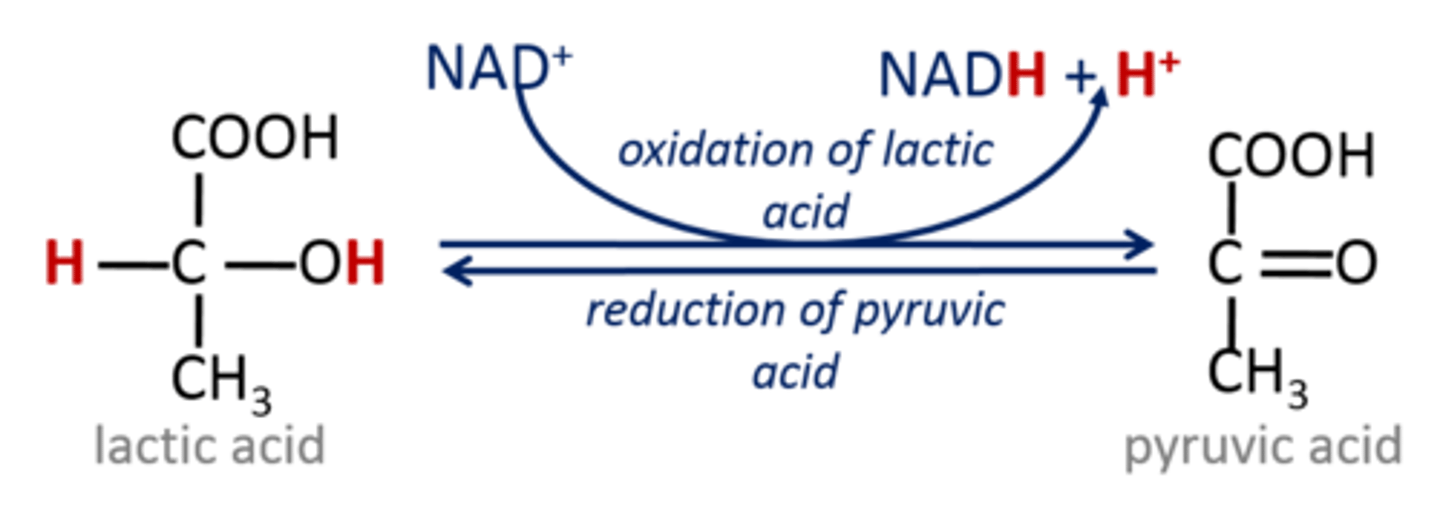
What B vitamins are coenzymes for dehydrogenases?
Thiamin (B1)
Riboflavin (B2)
Niacin (B3)
(Functions) Riboflavin (B2)
1) Coenzyme for dehydrogenase for redox reactions (FAD & FMN) --> utilized in the ECT, 1st step in beta-oxidation (fat breakdown), and TCA/Krebs cycle
2) Synthesis of niacin (B3), folate (B9), B6
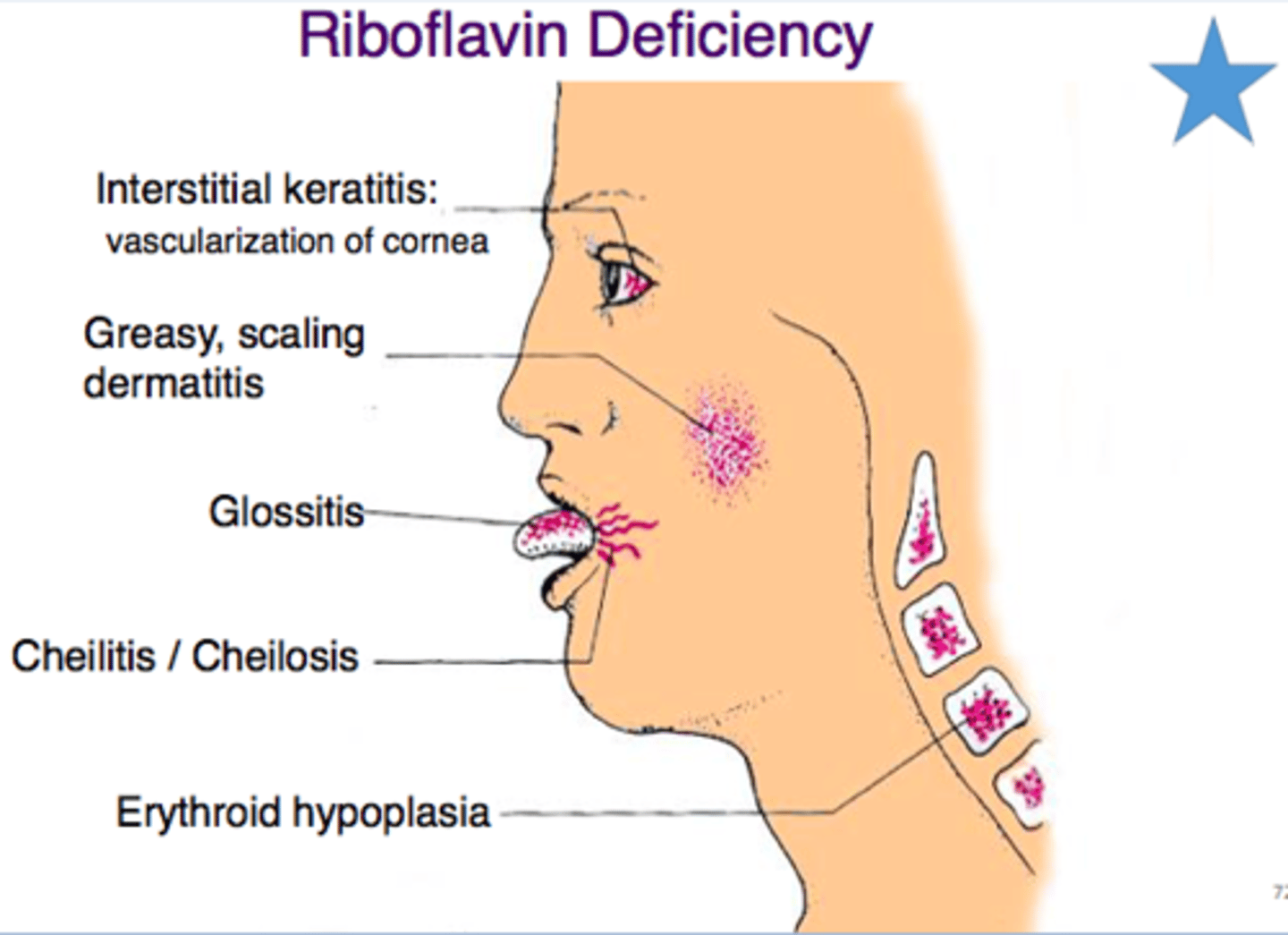
(Early Deficiency Symptoms) Riboflavin (B2)
1) Photophobia - light sensitivity
2) Burning/itching eyes
3) Soreness of mouth
(Deficiency Name) Riboflavin (B2)
Ariboflavinosis
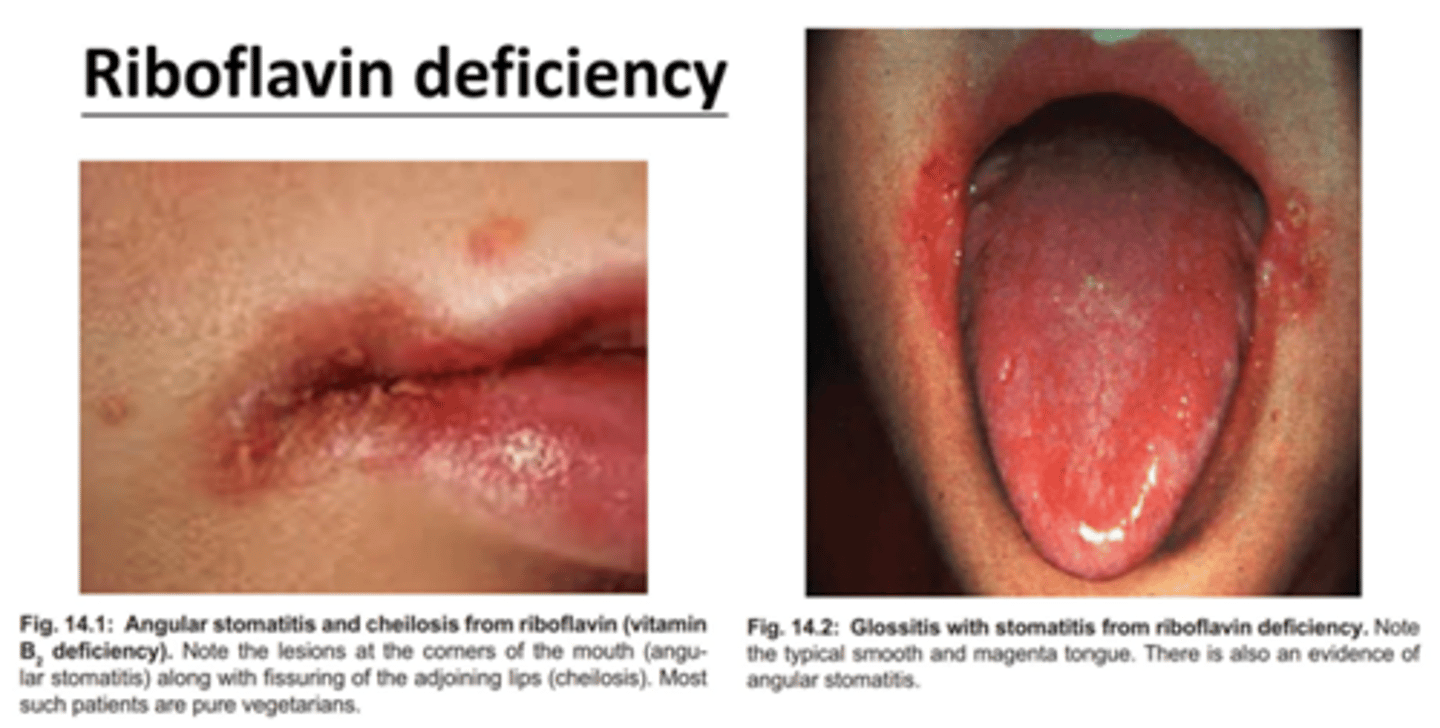
(Ariboflavinosis) Riboflavin (B2)
1) Cheilosis - cracking of mouth
2) Angular stomatitis - painful sores at the corners of the mouth
3) Glossitis - inflammation of the tongue
4) Magenta tongue - specific to Ariboflavinosis
5) Photophobia & Corneal vascularization
(Toxicity Symptoms) Riboflavin (B2)
No toxicity; 400mg has been shown to be an effective dose for treating migranes
(Sources) Riboflavin (B2)
1) Cow's milk (1 glass = 0.5mg)
2) Enriched grains/cereal
3) Almonds
4) Eggs
5) Meat
6) Soybeans

What population(s) are at risk for Riboflavin (B2) deficiency?
1) Lactose intolerance & Paleo diet (low dairy intake = milk is a good source)
2) Pregnant & Lactating women
3) Diabetes
4) Stress
5) Hypothyroidism

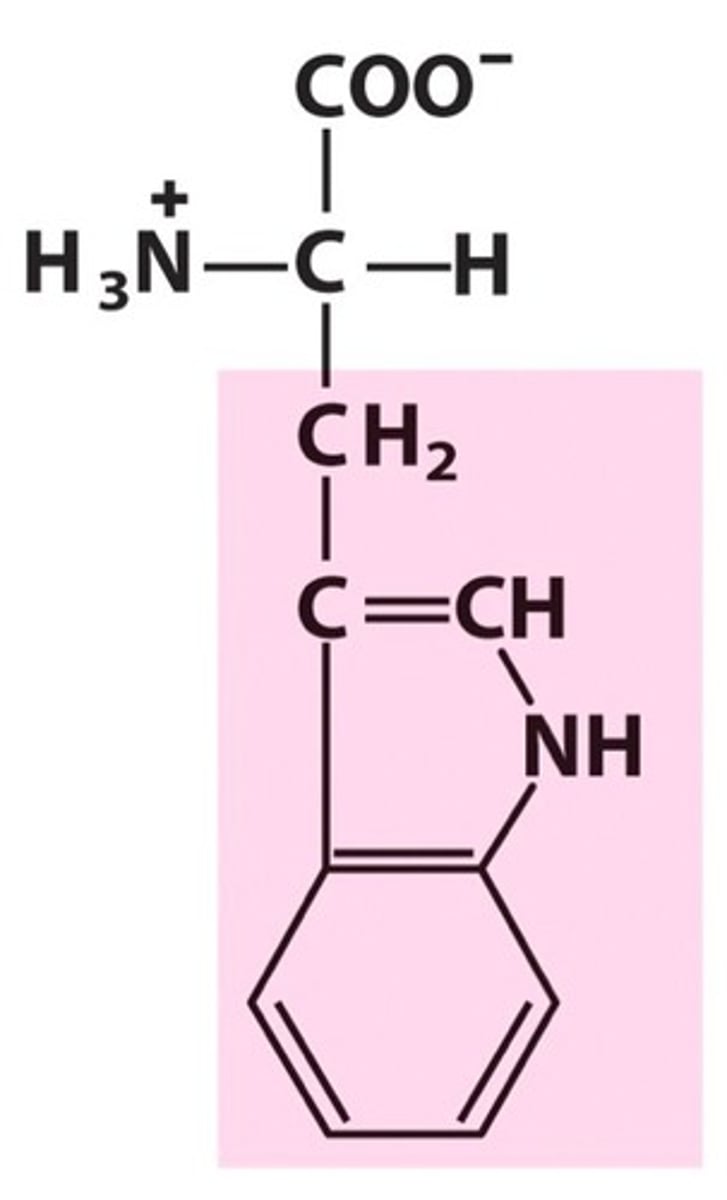
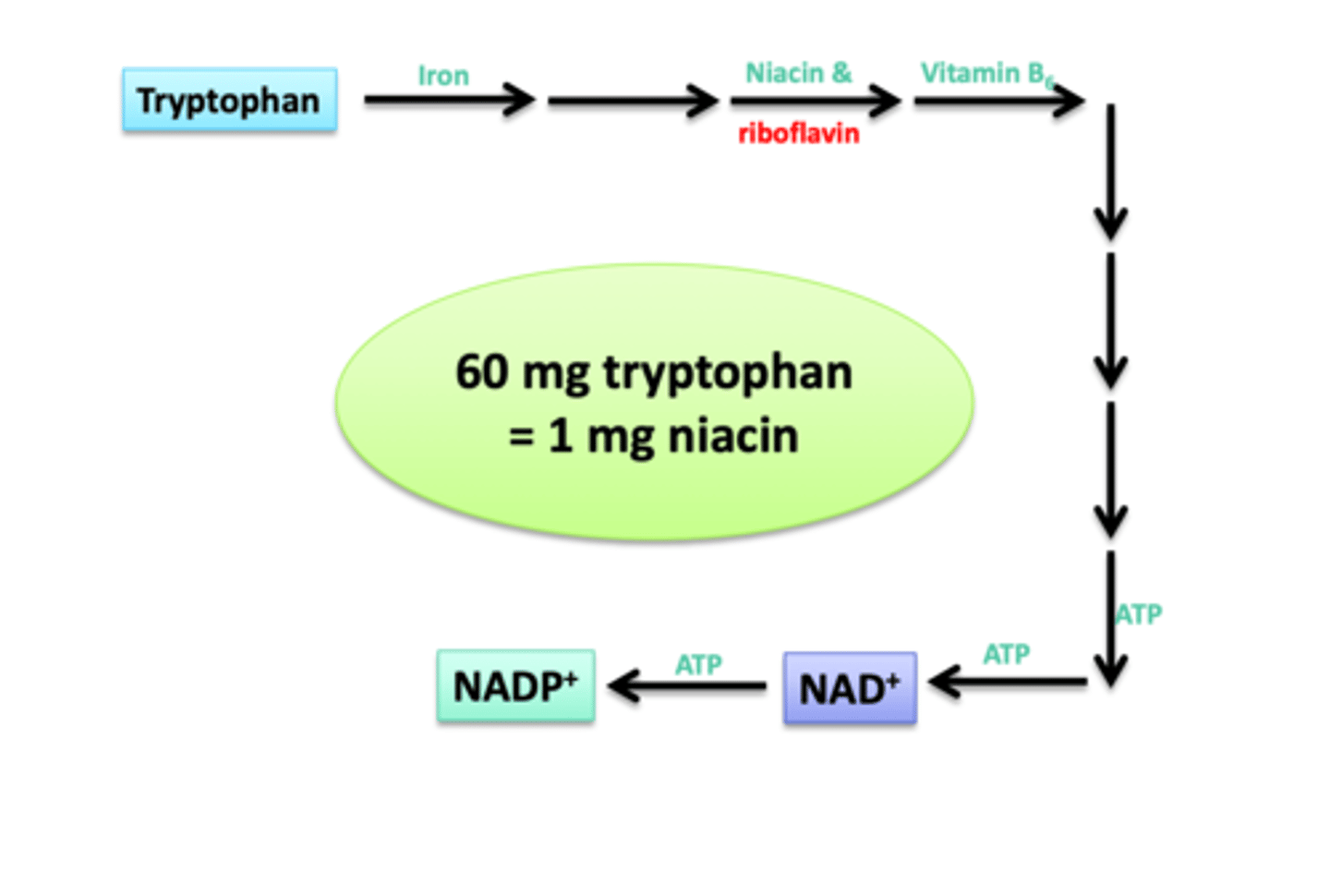
Niacin (B3) is made from...
Tryptophan (A.A.)
(Functions) Niacin (B3)
1) Coenzyme for dehydrogenase for redox reactions (NAD & NADP)
NAD --> glycolysis, TCA/Krebs, beta-oxidation, ethanol metabolism
NADH --> fatty acid synthesis, cholesterol & folate synthesis, 2nd step in beta-oxidation
2) Noncoenzyme - ADP-ribose transferase reactions / DNA repair & Chromatin remodeling
(Deficiency Name) Niacin (B3)
Pellagra
Dr. Joseph Goldberger ('filth parties')
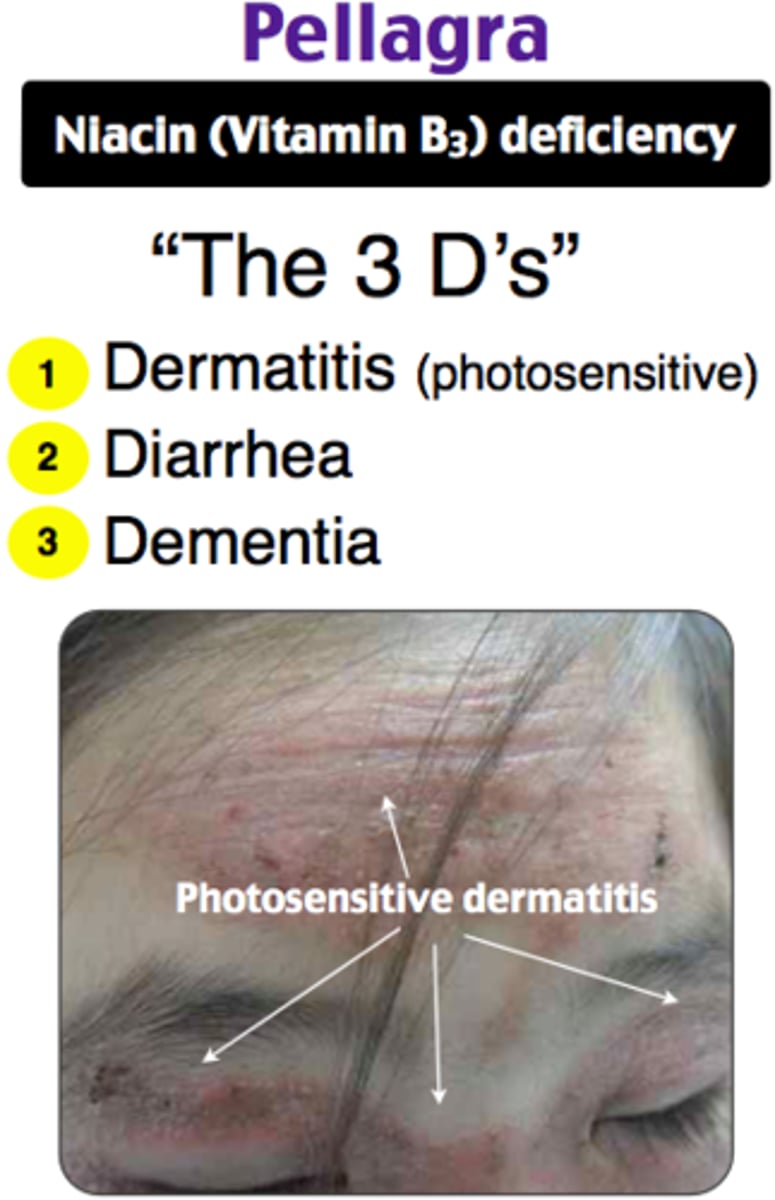
(Deficiency Symptoms) Niacin (B3)
3(4) D's
1) Dermatitis - sunburn on face, neck & extremities
2) Dementia - headache, memory loss, confusion, disorientation
3) Diarrhea - inflammation of mucus membrane of mouth & GI tract (glossitis, cheilosis, angular stomatitis)
4) Death
Additionally mouth issues found in Ariboflavinosis (Cheilosis - cracking of mouth, Angular stomatitis, Glossitis - inflammation of the tongue)

Pellagra was common in the Southern US with diet of
3 M's
1) Meat (Pork back fat)
2) Meal (Cornmeal)
3) Molasses
(Toxicity Symptoms) Niacin (B3)
1) Vasodilation/hot flashes (flushing from histamine)
2) Heartburn
3) Liver damage
4) Gout
5) Impaired blood glucose

(Sources) Niacin (B3)
High protein foods
1) Chicken, Pork, Beef, Fish
2) Enriched grains/cereals
3) Coffee
What population(s) are at risk for Niacin (B3) deficiency?
1) Malabsorptive patients
2) Alcoholics
3) Patients with HIV
4) Chemotherapy
5) Older patients
___ mg of tryptophan = ____ mg of niacin
60:1
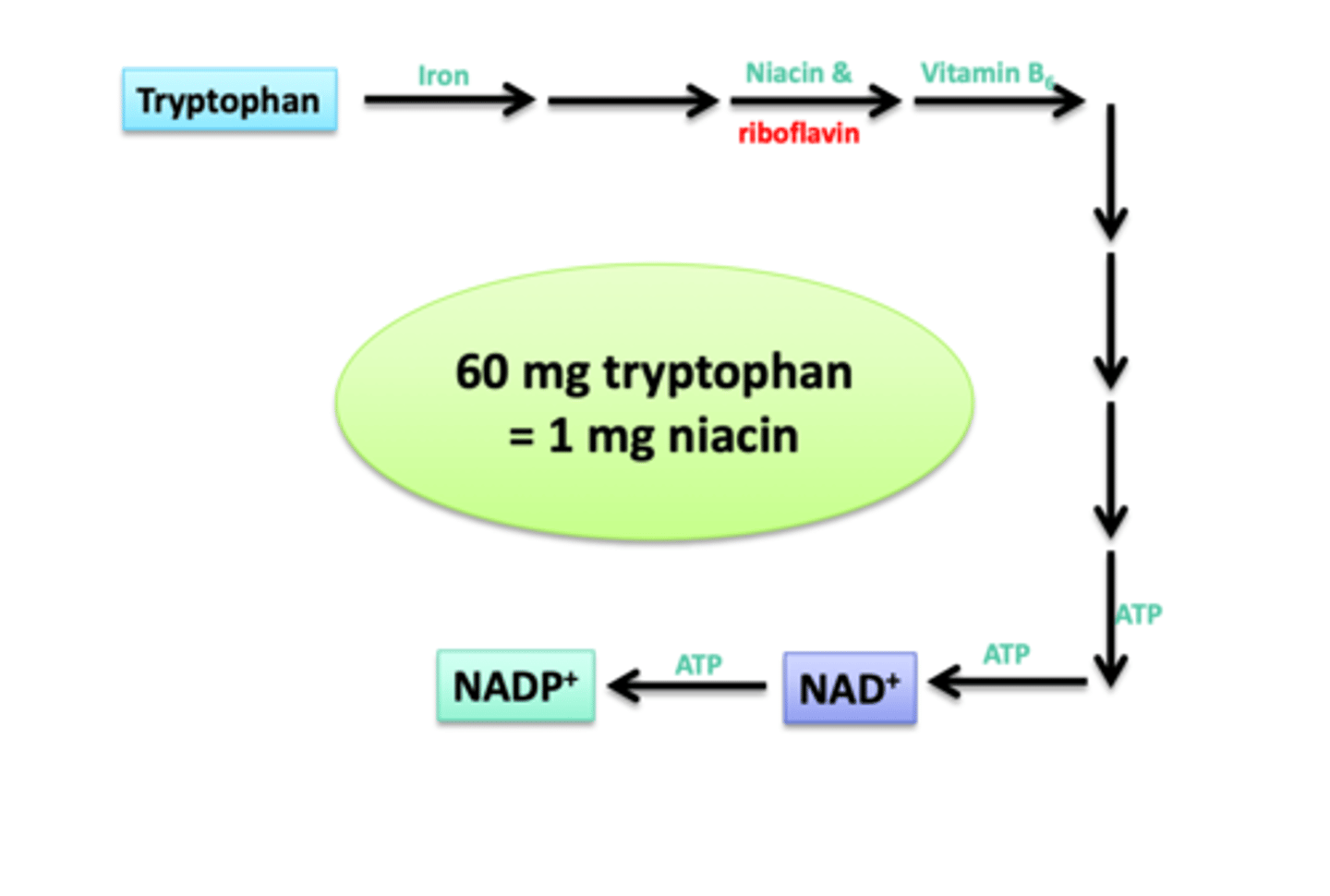
What B vitamins are required to convert Tryptophan to NADP?
Niacin (B3), Riboflavin (B2), and B6 (Vitamers)
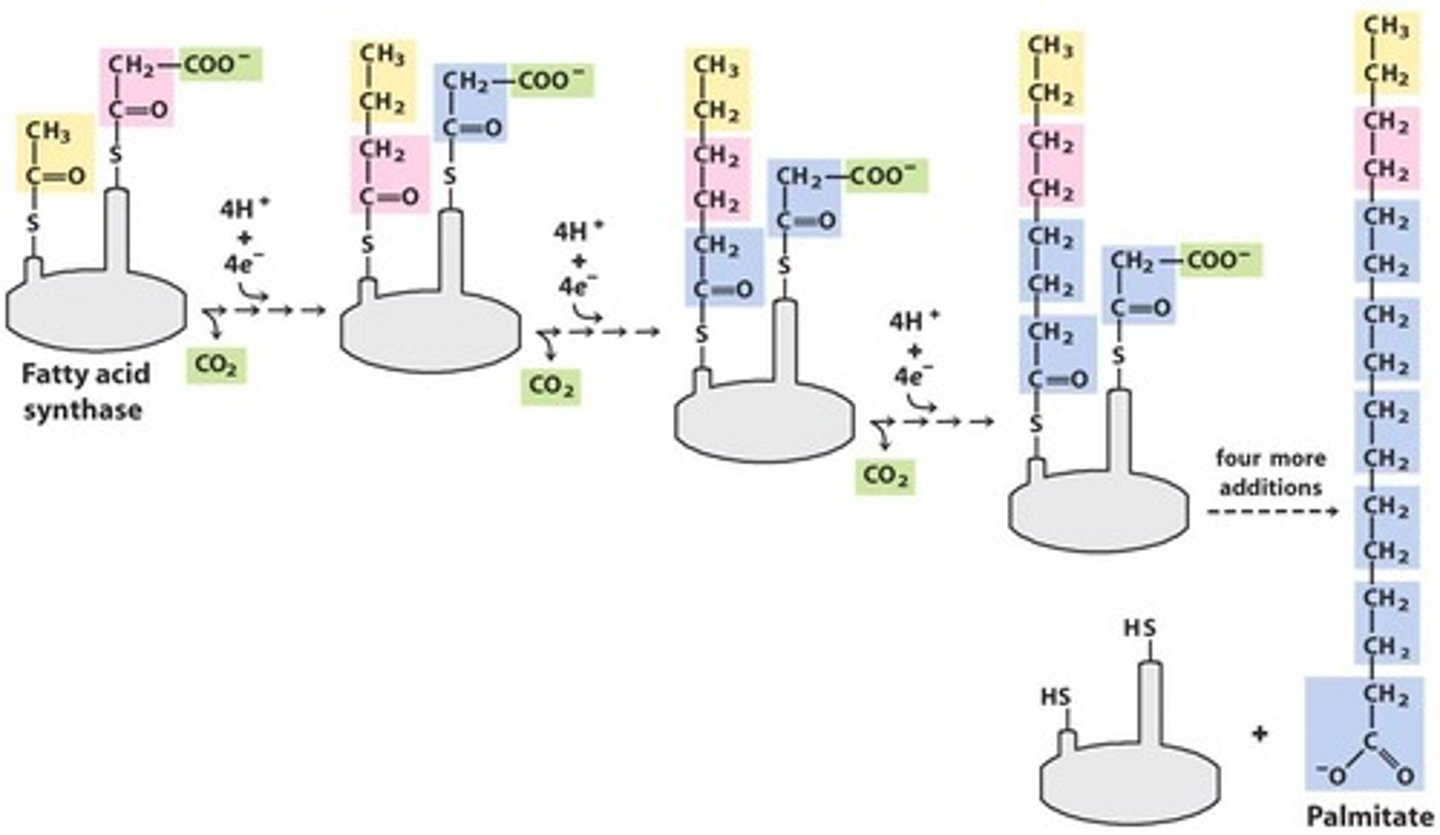
(Functions) Pantothenic acid (B5)
1) Coenzyme - part of Coenzyme A (CoA)
CoA --> metabolisms of carbs & lipids, synthesis of fatty acids & cholesterol, phospholipids, neurotransmitters, sphingolipids (nerves), and heme
2) Carrier protein (ACP) - Acyl-carrier protein in Fatty Acid Synthase
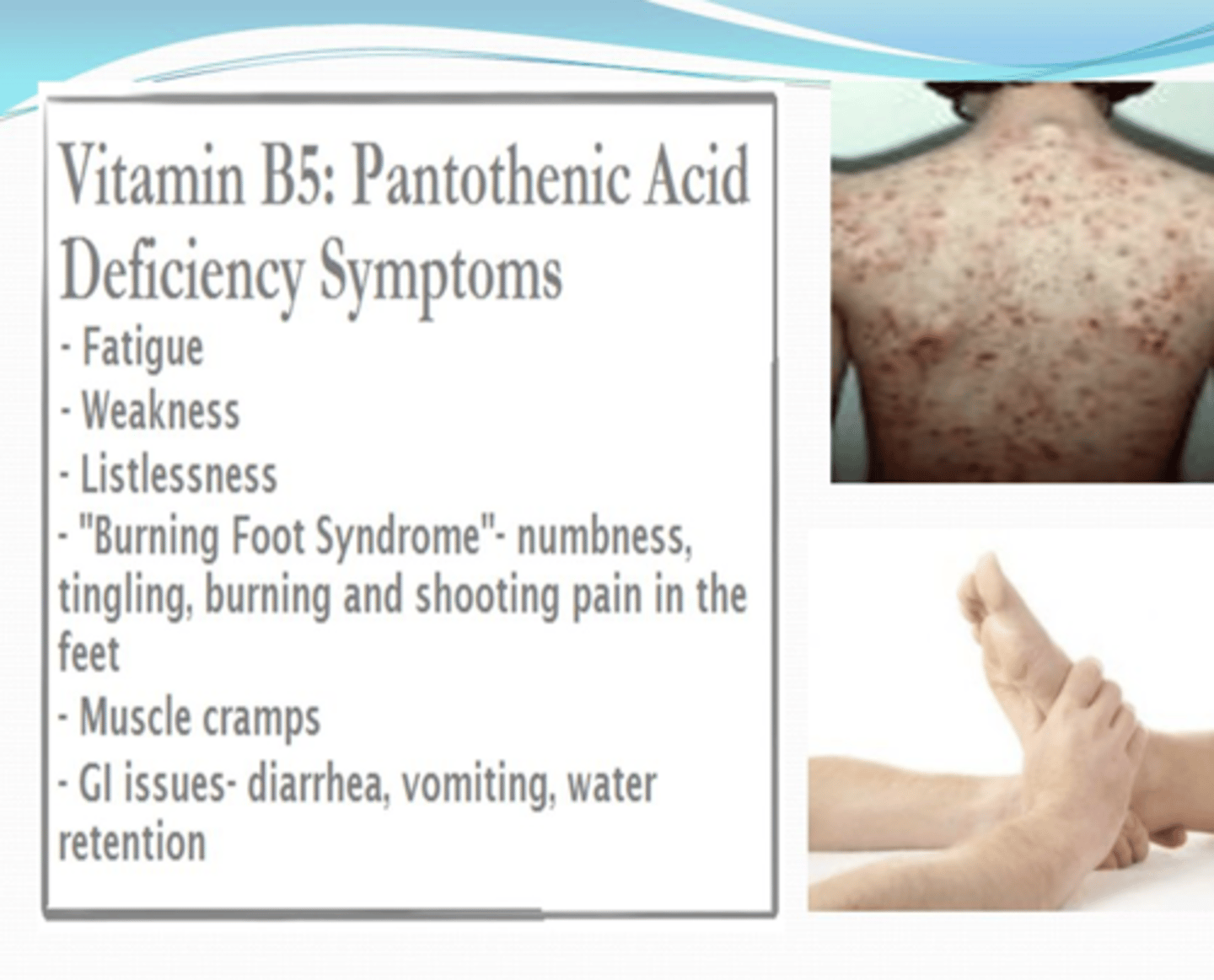
(Deficiency Name) Pantothenic acid (B5)
Burning Foot Syndrome
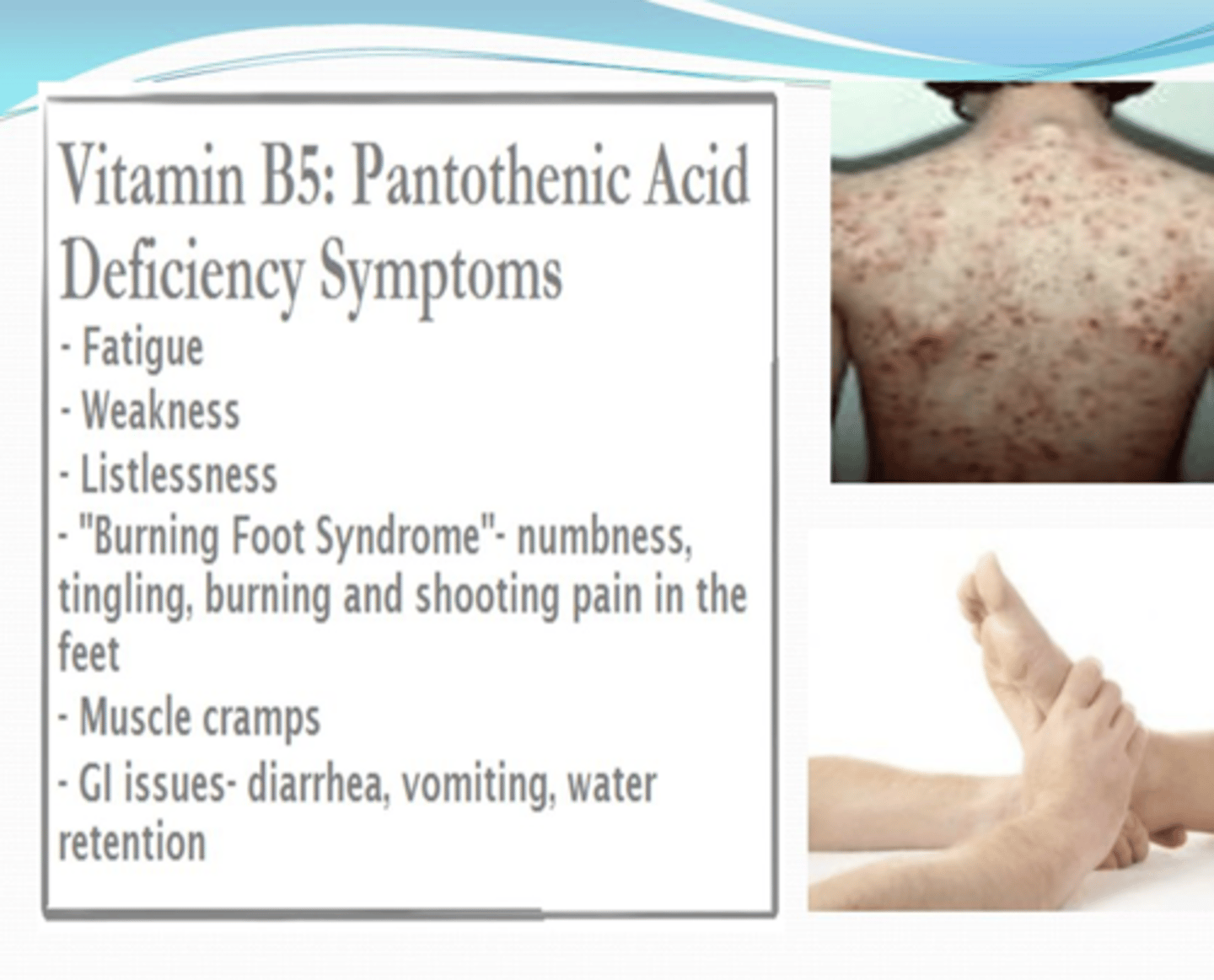
(Deficiency Symptoms) Pantothenic acid (B5)
-Very rare; results in dysfunctional lipid synthesis and energy production
-Depression, fatigue, insomnia, burning sensation in the feet and hands, numb toes and weakness
(Toxicity Symptoms) Pantothenic acid (B5)
None
(Sources) Pantothenic acid (B5)
All over in the diet
1) Meat & Poultry
2) Egg yolk
3) Milk
4) Whole grains
5) Seeds
6) Veggies
Destroyed with cooking and freezing
(Functions) Pyridoxal phosphate (B6)
1) Coenzyme - Pyridoxal Phosphate - PLP
1a) PLP --> amino acid metabolism (higher protein intake = higher B6 intake)
1b) PLP --> glycogen degradation,
1c) PLP --> heme synthesis
1d) other = sphingolipids in myelin sheath, and niacin (B3), neurotransmitters (serotonin, epinephrine, norepinephrine, GABA), and histamine
2) Non-coenzyme = Facilitates binding of steroid hormones & transcription factors for gene expression
(Deficiency Symptoms) Pyridoxal phosphate (B6)
RARE
- Dermatitis
- Glossitis - inflammation of the tongue
- Cheilosis - cracking of mouth
- Angular stomatitis - painful sores at the corners of the mouth
- Peripheral neuropathy (unique!)
- Seizures
- Hypochromic microcytic anemia; due to lack of heme synthesis

(Toxicity Symptoms) Pyridoxal phosphate (B6)
Tolerable upper intake level = 100mg --> Nerve damage / Neuropathy (unique!)
(Sources) Pyridoxal phosphate (B6)
1) Enriched cereals
2) Meat & poultry
3) Nuts
4) Grains
5) Seafood
Higher bioavailability from animal than plant
What population(s) are at risk for Pyridoxal phosphate (B6) deficiency?
1) Impaired renal function
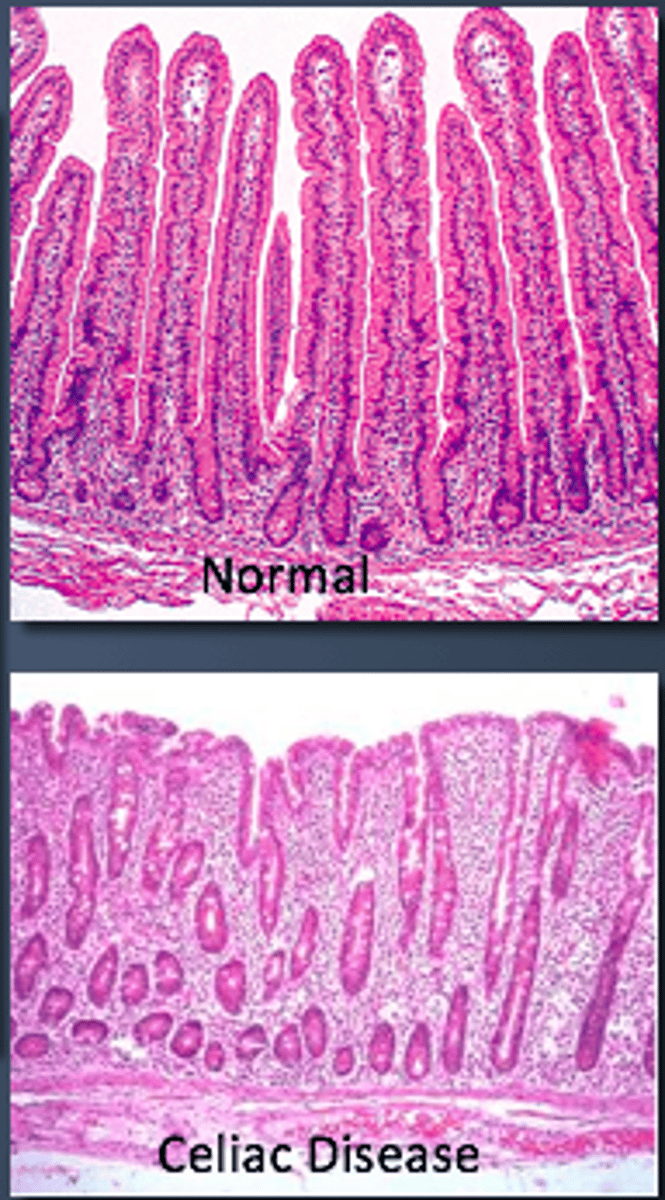
2) Autoimmune conditions - Celiac & IBD
3) Alcoholics
4) Patients on isoniazid (TB med) or corticosteroids
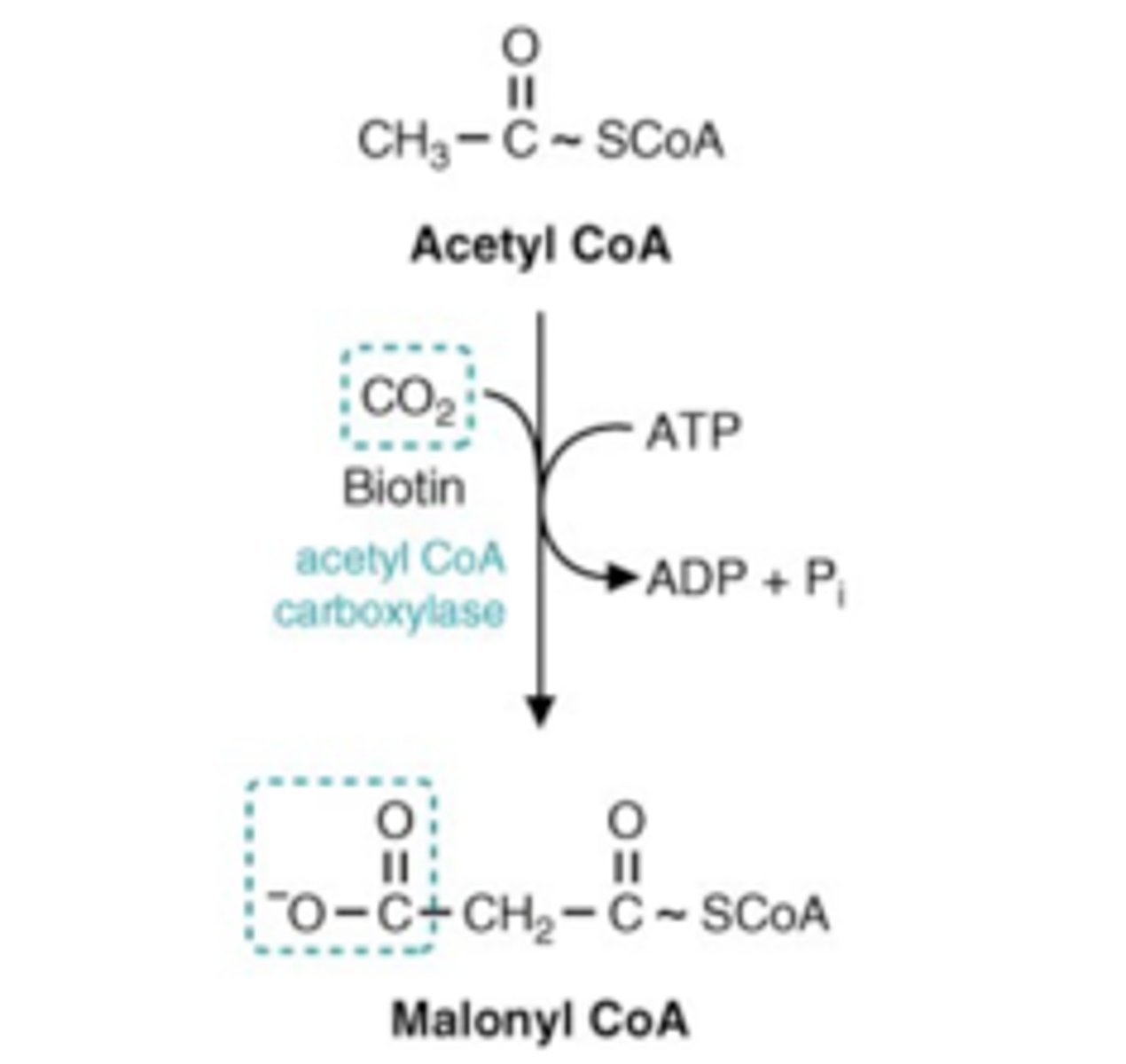
(Functions) Biotin (B7)
1) Coenzyme for carboxylase reactions: committed step in FA synthesis (Acetyl-CoA carboxylase used in Acetyl-CoA to Malonyl-CoA)
1a) Pyruvate carboxylase used in Pyruvate to Oxaloacetate (TCA & gluconeogensis)
2) Non-coenzyme = Transcription/synthesis of several enzymes / gene expression (glucokinase, phosphoenolpyruvate carboxykinase) & histone modification, and cell signaling
(Deficiency Symptoms) Biotin (B7)
RARE; Raw egg white injury
1) Dermatitis
2) Anorexia
3) Depression
4) Alopecia - hair loss
5) Muscle pain
6) Lethargy
7) Hallucinations
8) Ketolactic acidosis

(Toxicity Symptoms) Biotin (B7)
N/A BUT if someone is supplementing with biotin impacts thyroid or Vit. D testing
(Sources) Biotin (B7)
1) Bacteria in L.I.
2) Nuts
3) Liver
4) Soy
5) Cooked eggs
6) Dairy
What population(s) are at risk for Biotin (B7) deficiency?
1) Infants with biotinidase deficiency
2) People who consume raw egg whites (Avidin)
3) Chronic alcoholics
4) Pregnant / Breastfeeding mothers
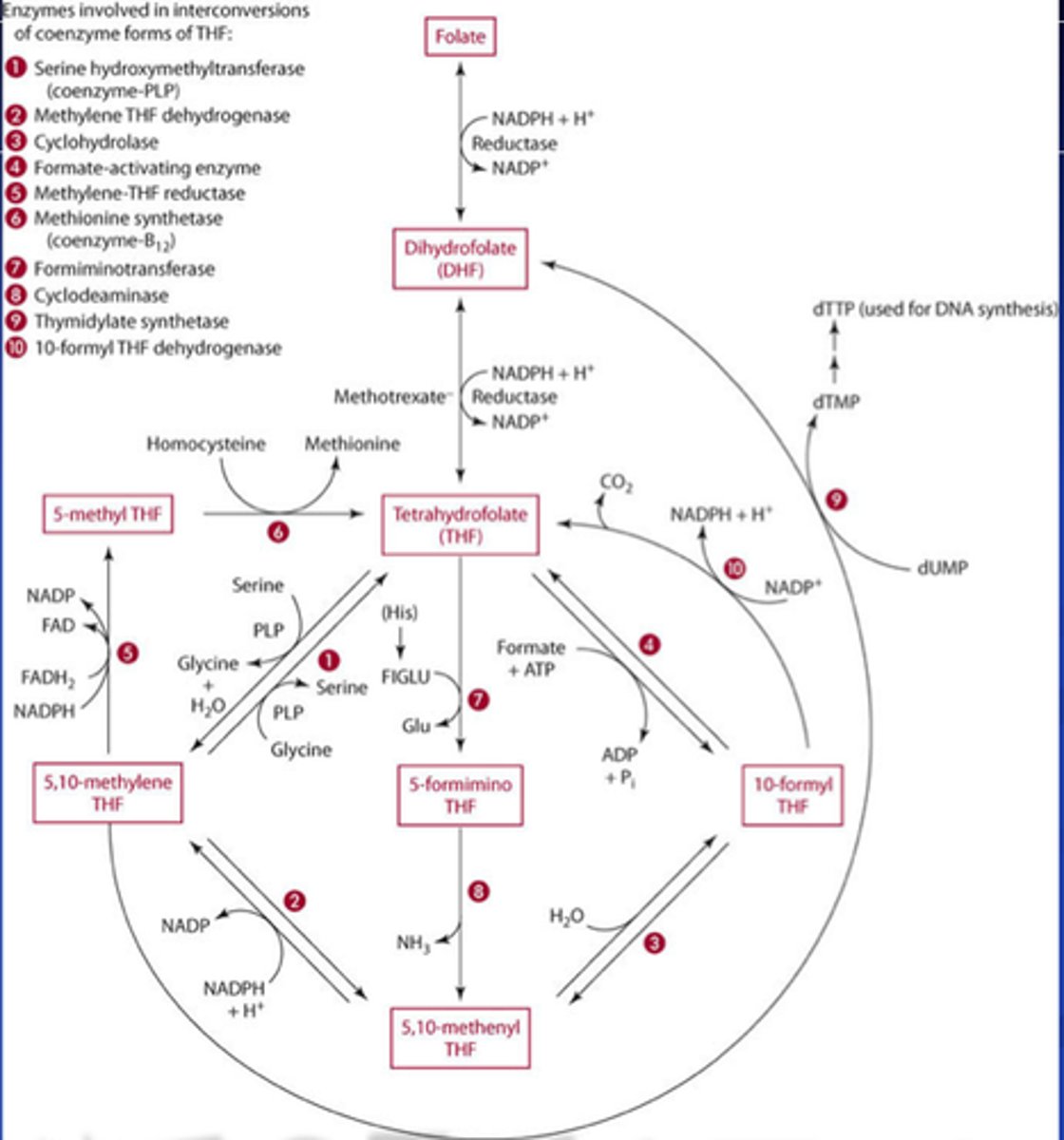
(Functions) Folate (B9)
1) Coenzyme for methylation reactions: Tertrahydrofolate (THF)
1a) THF - 1 carbon metabolism (methylation)
1b) THF - Purine & pyrimidine synthesis aka DNA & RNA synthesis and repair
1c) THF - formation of RBCs & WBCs, and
1d) THF- A.A. metabolism
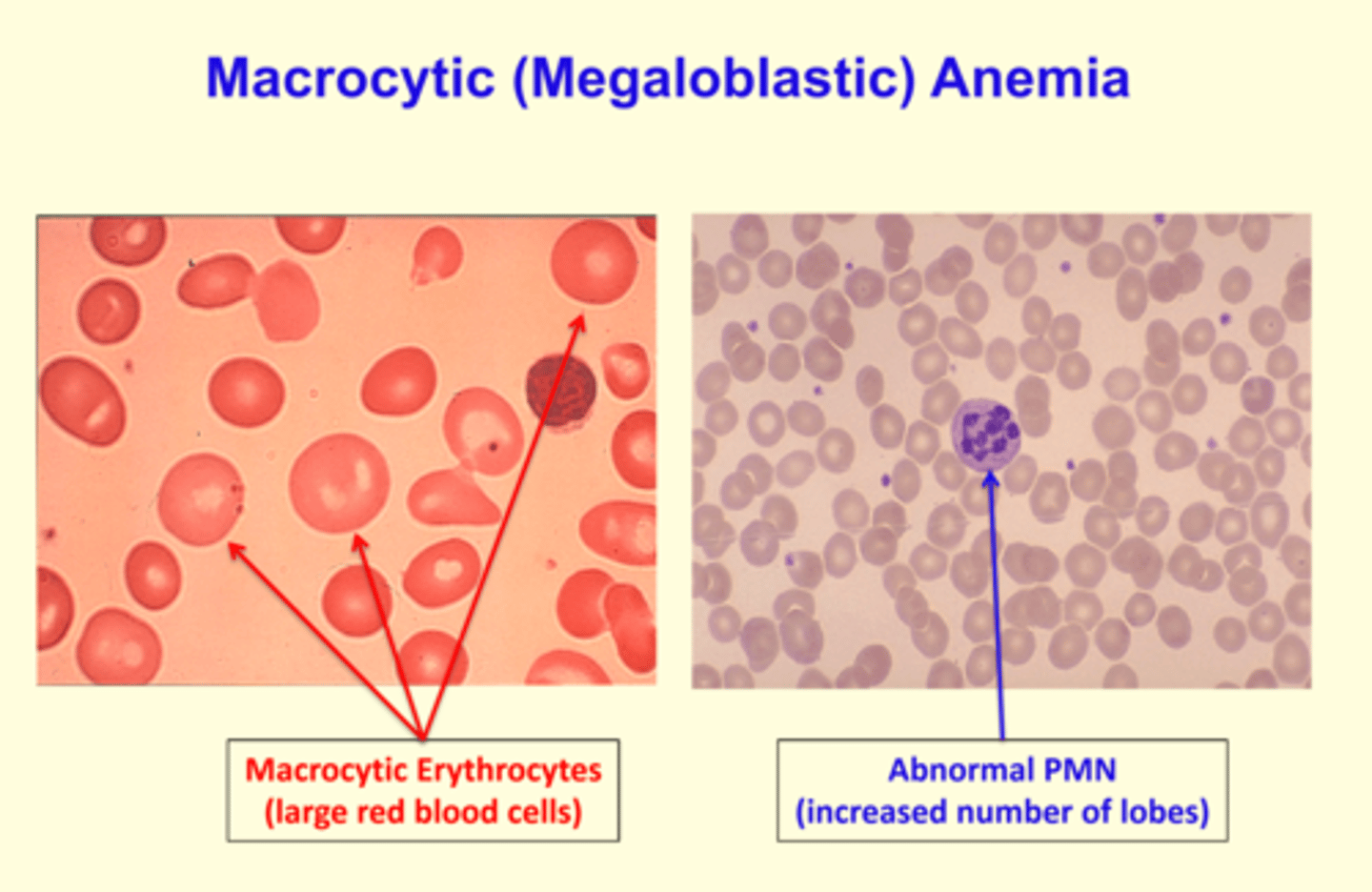
(Deficiency Name) Folate (B9)
Megaloblastic Macrocytic Anemia --> fatigue, headaches, difficulty concentrating, shortness of breath, heart palpitations
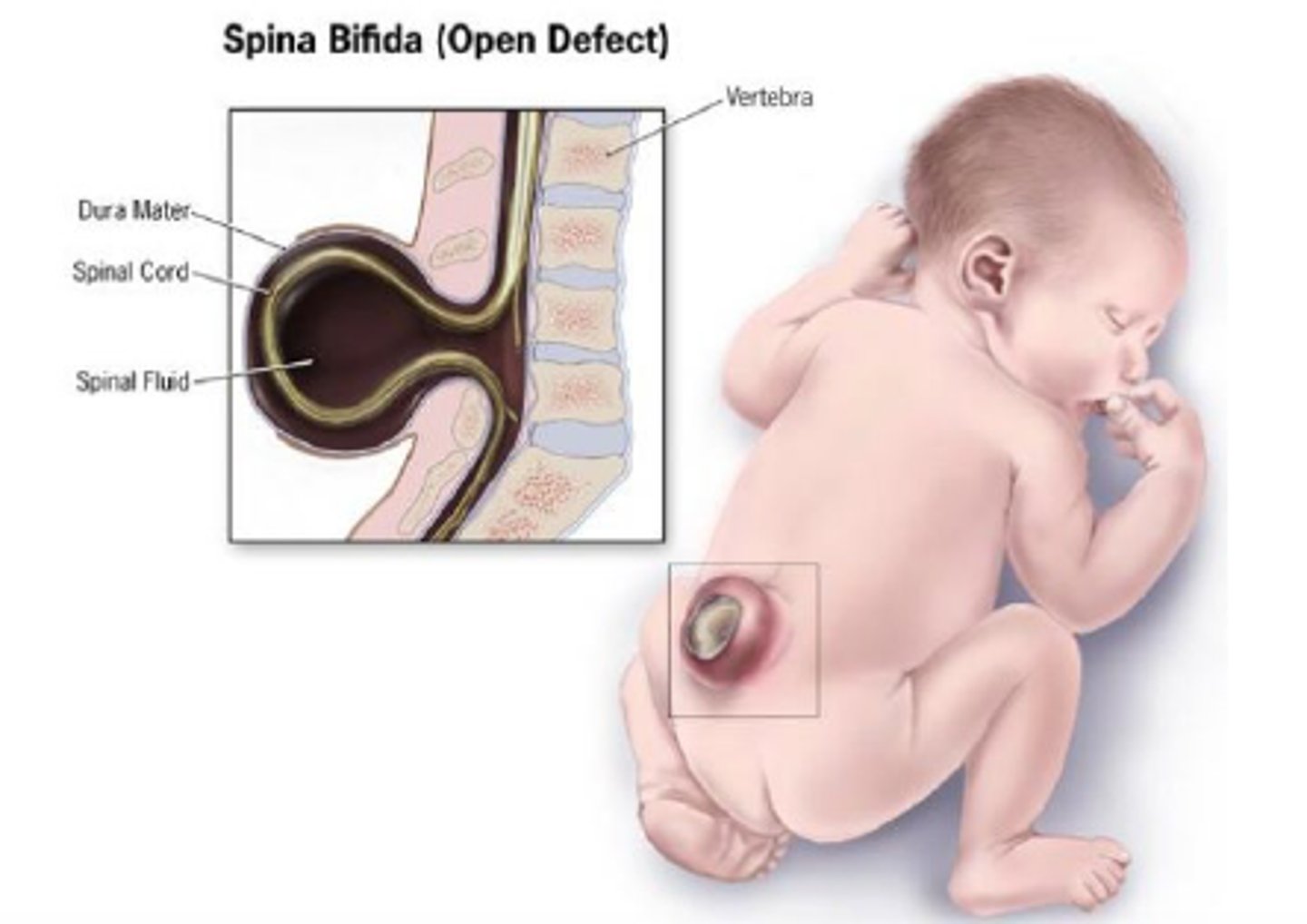
Neural tube defects --> Spina bifida & Anencephaly
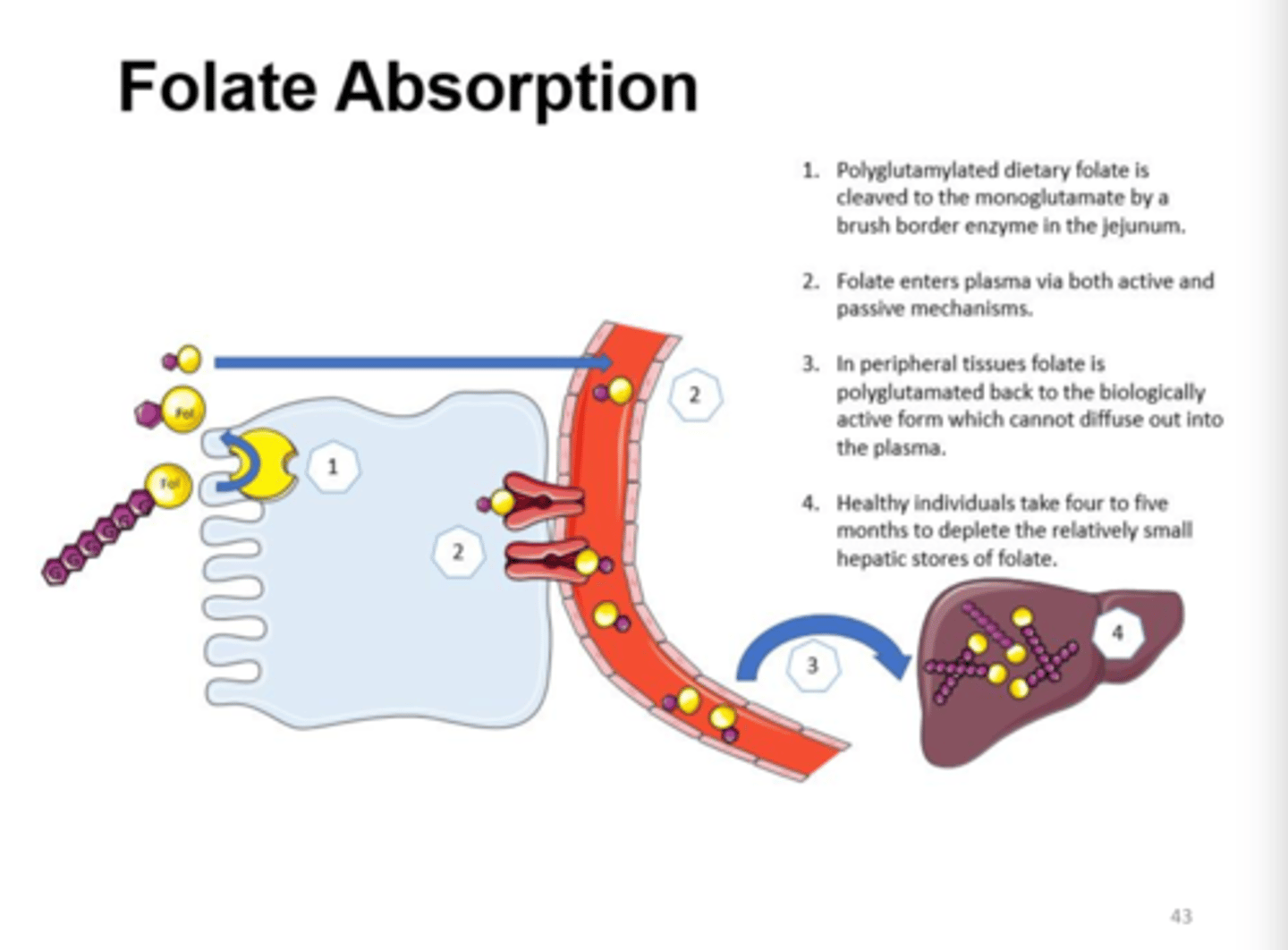
Absorption:
Folic acid =
Folate =
Folic acid = NO digestion
Folate = Folate hydrolase aka glutamate carboxypeptidase II conjugate removes the glutamic acid residues present; and zinc is required for the zinc-dependent enzyme in the brush border for absorption
(Deficiency Symptoms) Folate (B9)
1) Anemia (Megaloblastic) - fatigue, headaches, difficulty concentrating, shortness of breath, palpitations
2) Neural Tube Defects (Spina bifida & Anencephaly)
3) Miscarriage
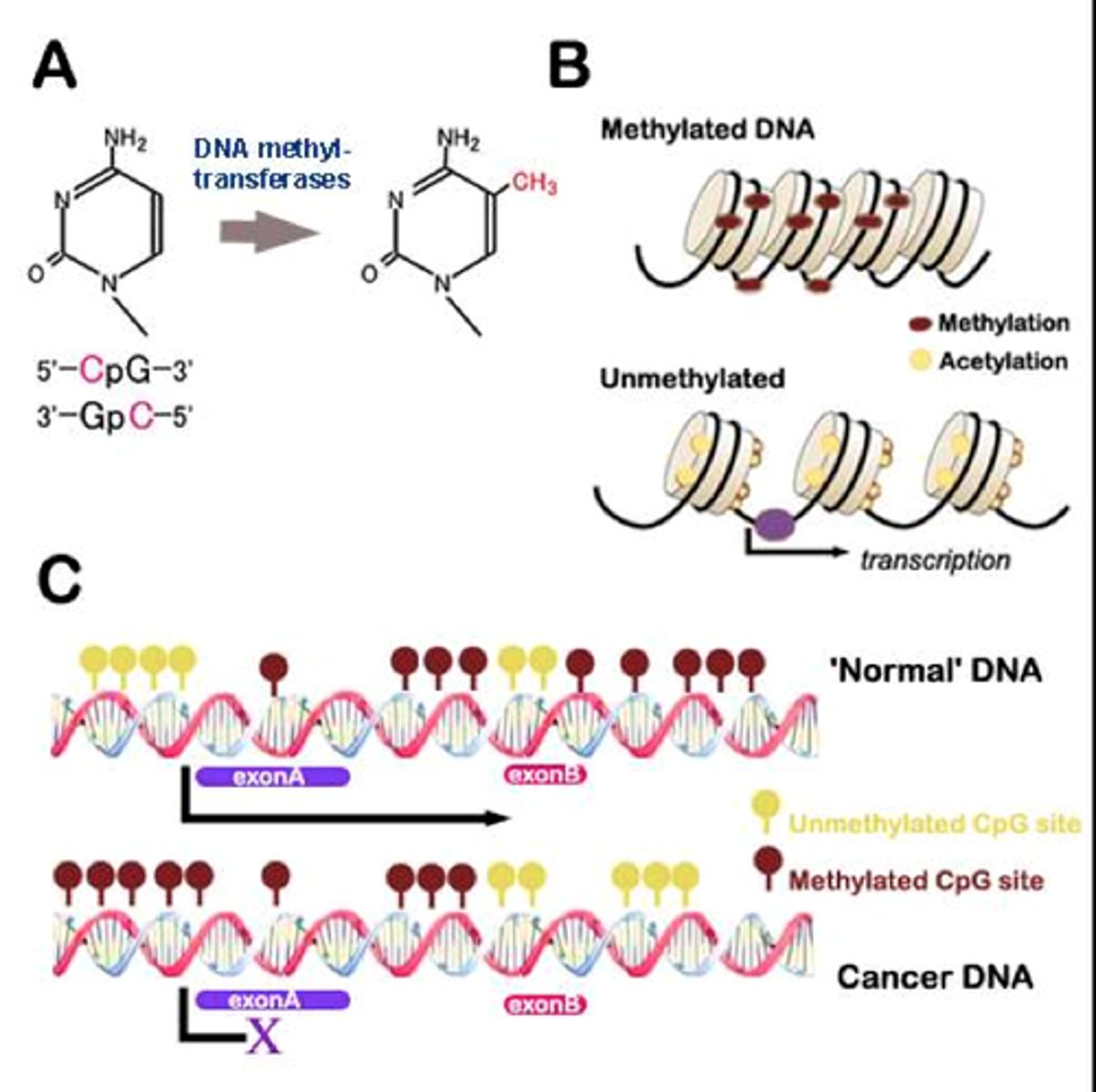
4) Unstable DNA & inadequate DNA repair (causing cancer)
5) Malabsorptive diarrhea; lack of DNA replication in GI tract
(Toxicity Symptoms) Folate (B9)
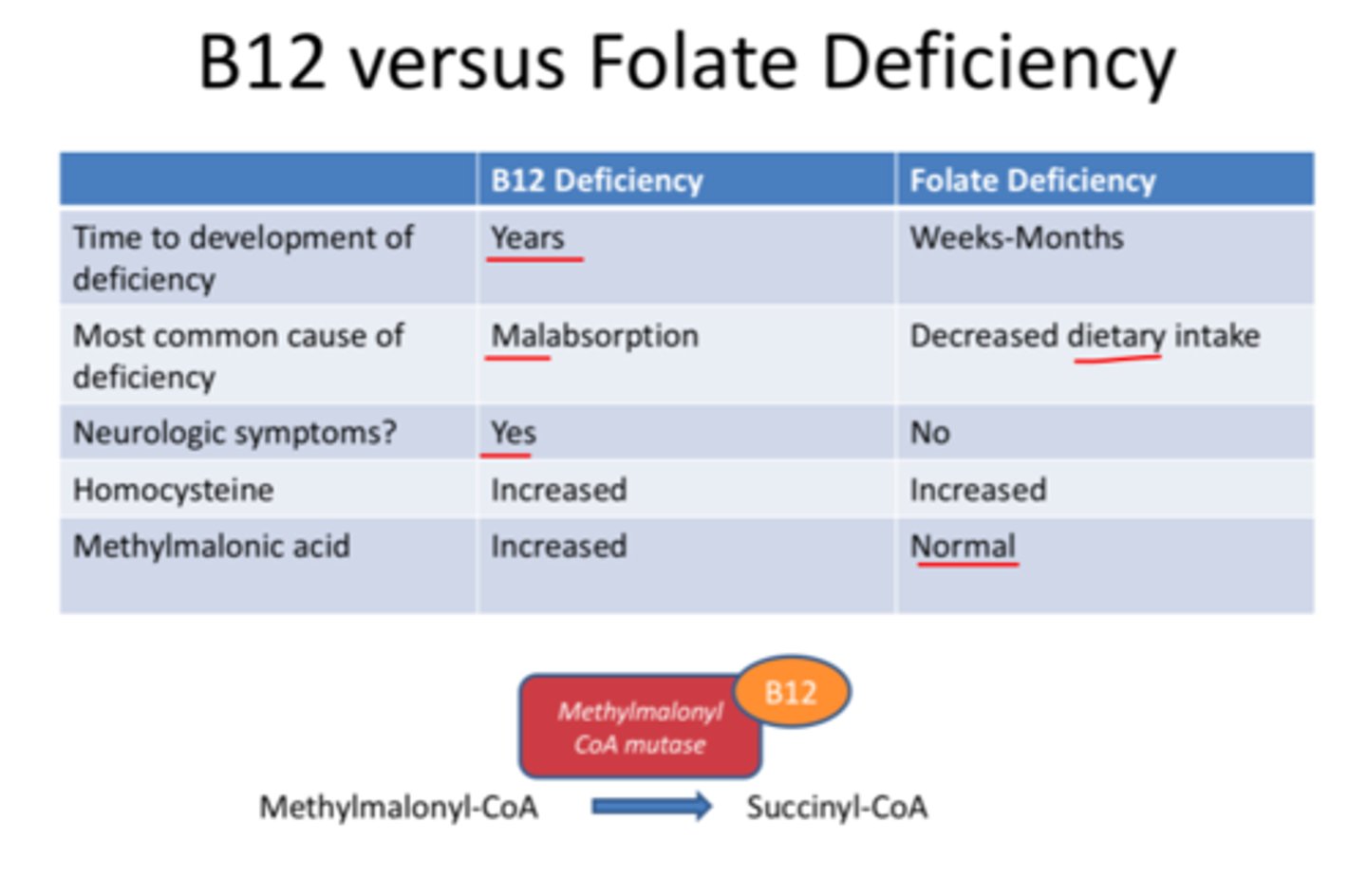
Masks B12 deficiency
1) G.I. distress
2) Irritability
3) Insomnia
4) Zinc deficiency = High supplementation of Synthetic Folic acid will cause zinc deficiency due to folic acid binding zinc in the GI tract. This then can impair Folate absorption because zinc is required to digest Folate
(Sources) Folate (B9)
Most foods / Green plants
1) Dark leafy vegetables
2) Mushrooms
3) Liver
4) Legumes
5) Enriched grains/cereal
5,10-Methylene THF ---(______________________)------> 5-Methyl THF
Niacin (B3) & Riboflavin (B2)
Methylene THF Reductase (MTHFR)
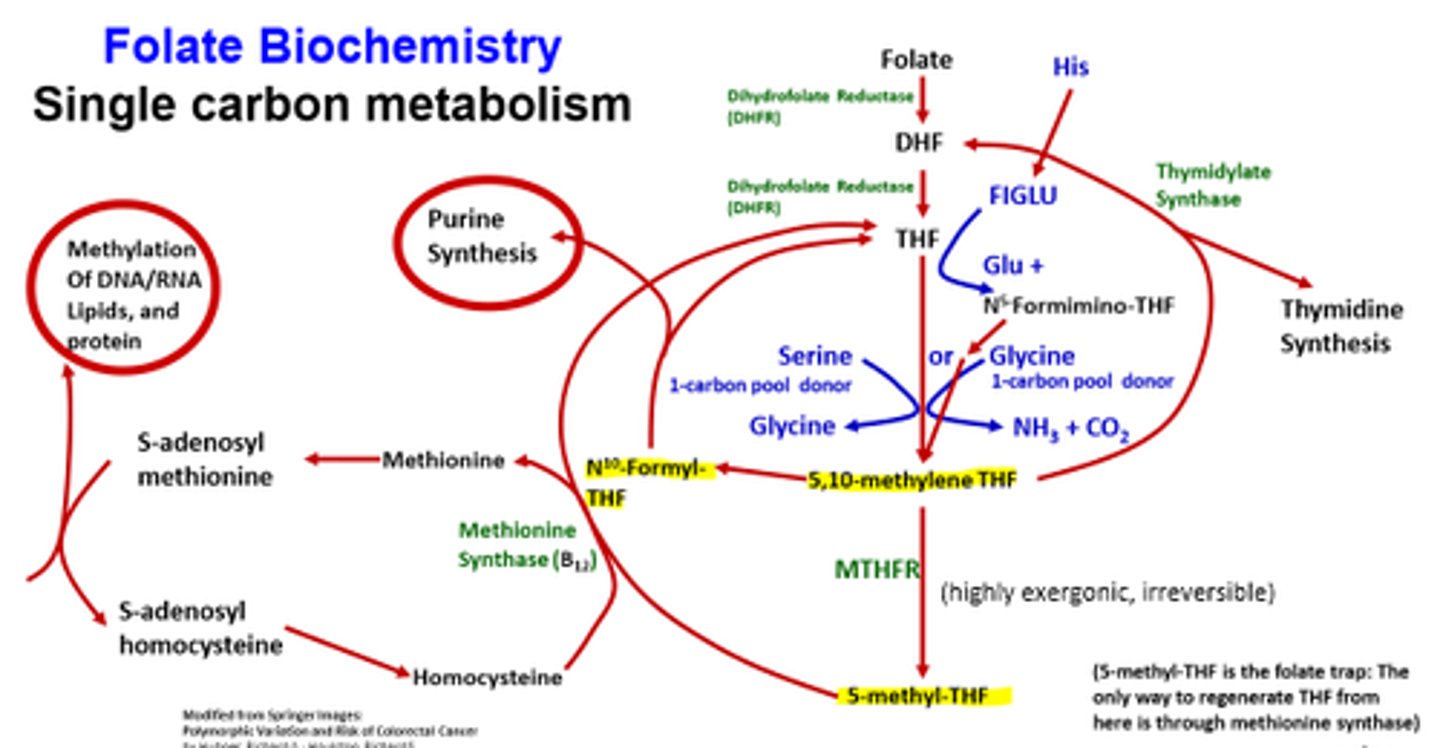
10-Formyl THF =
5,10-Methylene THF =
5-Formimino THF =
5-Methyl THF =
10-Formyl THF = Purine synthesis
5,10-Methylene THF = Pyrimidine synthesis, serine, glycine, & choline degradation
5-Formimino THF = Histidine degradation
5-Methyl THF = Methionine synthesis (from homocysteine)
What population should avoid exceeding the tolerable upper intake of 1000 mcg of Folate?
Pregnant women; excessive amounts above the RDA during pregnancy are associated with low IQ and reduced immune system activity

What population(s) are at risk for Folate (B9) deficiency?
1) Alcoholics
2) Women of childbearing age
3) Malabsorptive conditions
4) MTHFR mutations (5,10-methylene TNF --> 5-methyl TNF)
________________ rely on Folate (B9) for survival.
Enterocytes; folate deficiency can lead to shorter vili height, thinning of GI tract, malabsorptive diarrhea, and glossitis
What are the two active coenzymes for Cobalamins (B12)?
5-deoxyadenosylcobalamin
Methylcobalamin
(Functions) 5-deoxyadenosylcobalamin (B12)
5-deoxyadenosylcobalamin = odd-chain fatty acid metabolism (threonine & isoleucine)
(Functions) Methylcobalamin (B12)
Universal methyl donor for DNA, RNA, hormones, proteins, lipids, and the nervous system / myelin sheath
1) Coenzyme for methylation reactions & Homocysteine removal: convert to methionine using methionine synthase
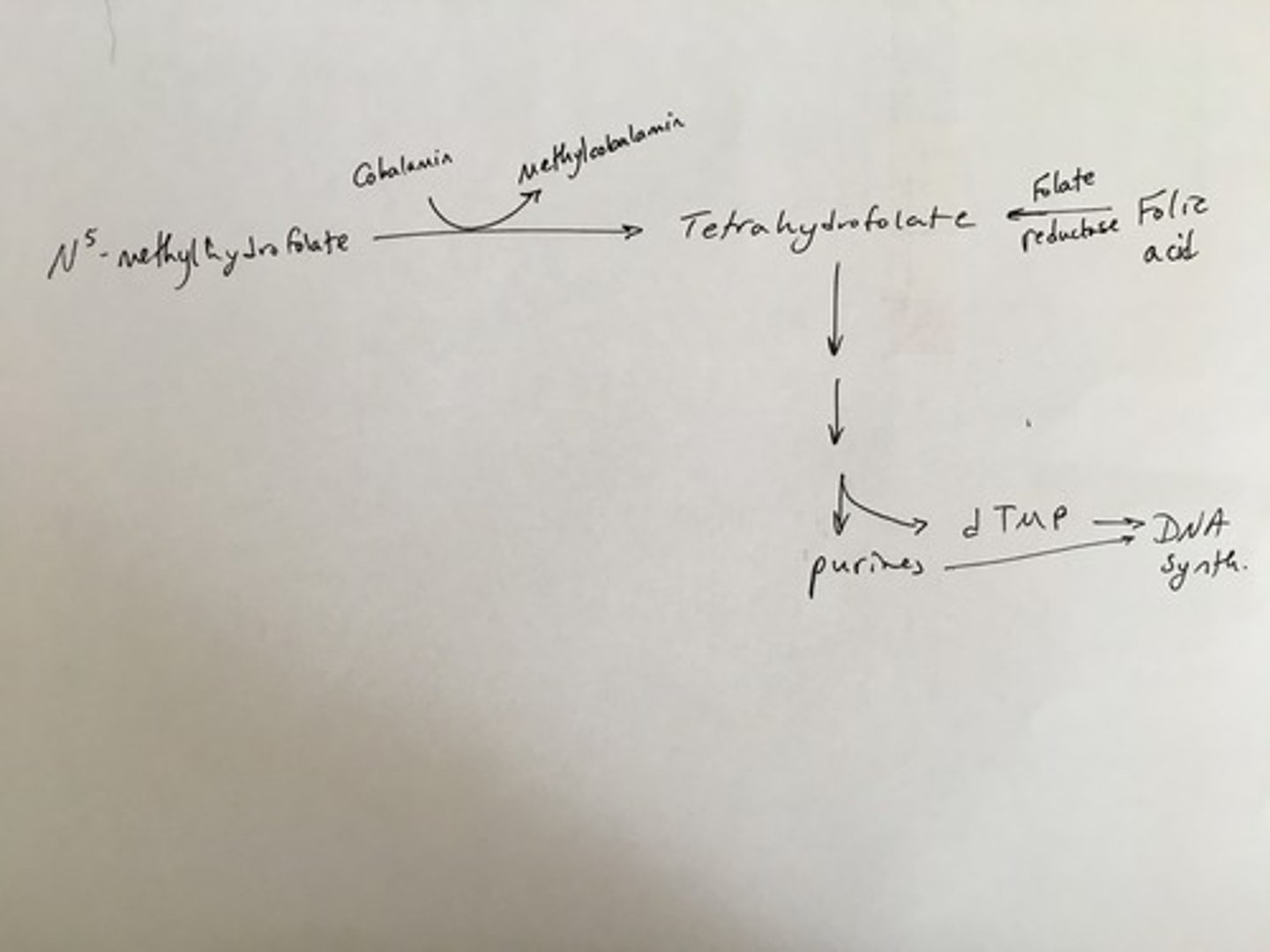
2) Folate pathway (5-methyl THF --(B12)--> Tetrahydrofolate (THF)
3) Heme synthesis
(Deficiency) Cobalamins (B12)
Pernicious anemia; likely due to auto-antibodies for IF
Megablastic anemia
Peripheral neuropathy (unique!)
(Causes of Deficiency) Cobalamins (B12)
1) MC due to poor absorption
2) Zollinger-Ellison syndrome --> too much HCl / low IF
3) Medications --> Histamine blockers, glucophage (metformin), protein pump inhibitors
4) Pancreatic insufficiency --> not enough proteases to release B12 from protein
5) Malabsorptive syndromes --> Celiac's, Crohn's (due to inflammation of ileum where B12 is absorbed), IBS, Cystic fibrosis
(Toxicity Symptoms) Cobalamins (B12)
N/A
(Sources) Cobalamins (B12)
Animals
1) Shellfish
2) Meat & Liver
3) Fish/seafood
4) Dairy (5-10% lost during pasteurization)
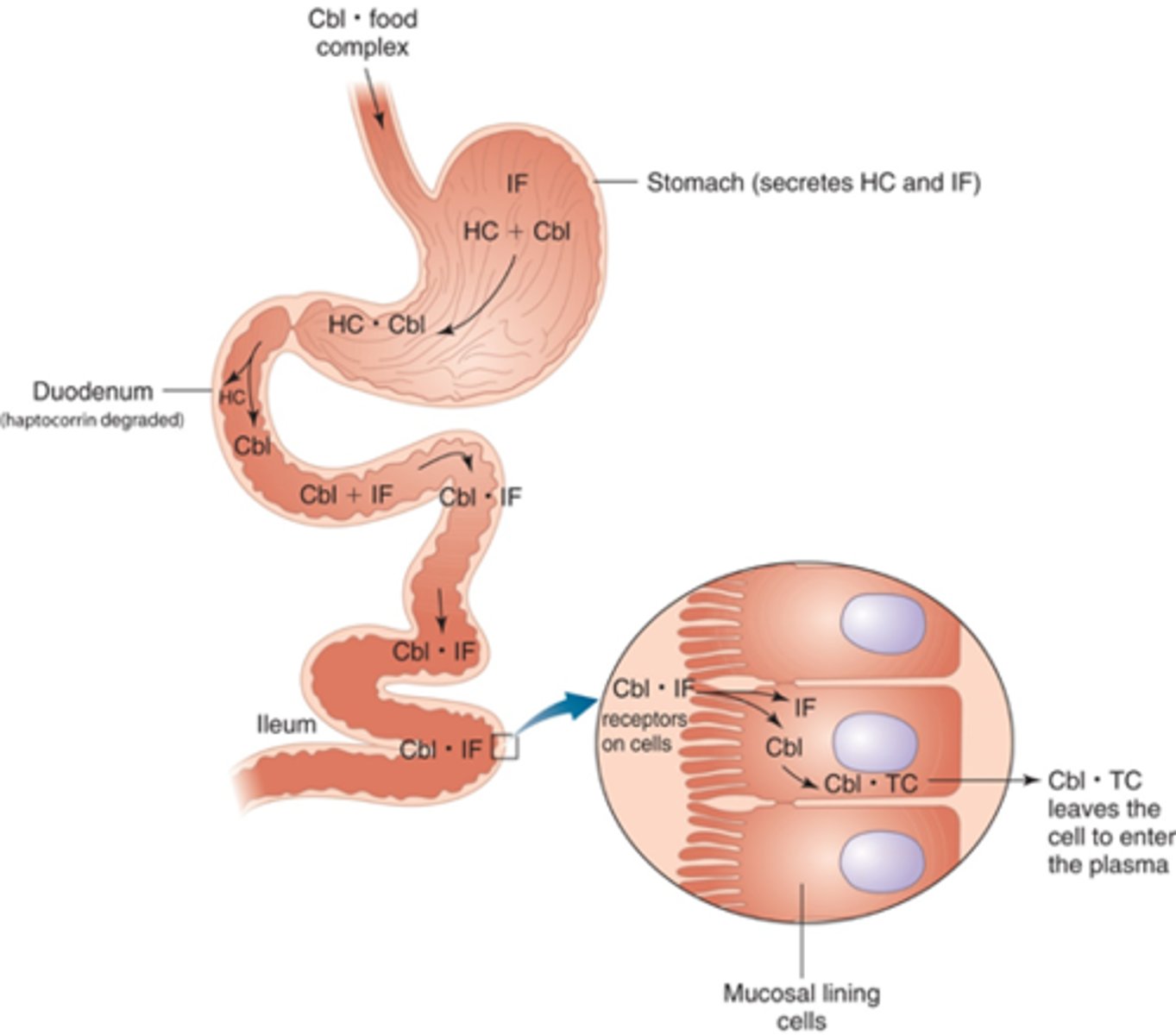
Does Cobalamin (B12) need to be digested?
Yes, B12 is bound to proteins in food. HCl & pepsin in the stomach will break the bond between B12 and protein and intrinsic factor (IF) will bind onto B12. IF receptor in the ileum binds B12-IF complex and absorbs by receptor-mediated endocytosis & some diffusion
Cobalamin (B12) is mainly stored in the liver. Roughly how many years would it take to deplete your B12 storage?
3-5 years
What is the Methylfolate Trap?
Lack of vitamin B12 impairs conversion of folate (B9)
5-methyl THF --> Tetrahydrofolate (THF)
What population(s) are at risk for Cobalamins (B12) deficiency?
1) Strict vegetarians/vegans
2) Elderly/Achlorhydria (decreased HCl)
3) Diabetics (metformin drug)
4) Gastritis (impaired IF release)
5) Zollinger-Ellison syndrome
6) Malabsorptive syndromes --> Crohn's
What population should consider supplementation of Cobalamins (B12)?
+50 years; anyone over age 50 years of age should consume B12-fortified foods or supplement (25-100 mcg/d) due to decreased HCl in the stomach. Low HCl (Achlorhydria) doesn't allow proteins to be broken down which doesn't release the B12
Vitamin B12 deficiency - Megaloblastic Macrocytic Anemia
Due to decreased DNA synthesis; causing fatigue, headaches, difficulty concentrating, depression, shortness of breath, peripheral neuropathy
Folate can get rid of hematologic symptoms, but NOT neurologic symptoms due to demyelination of nerves.
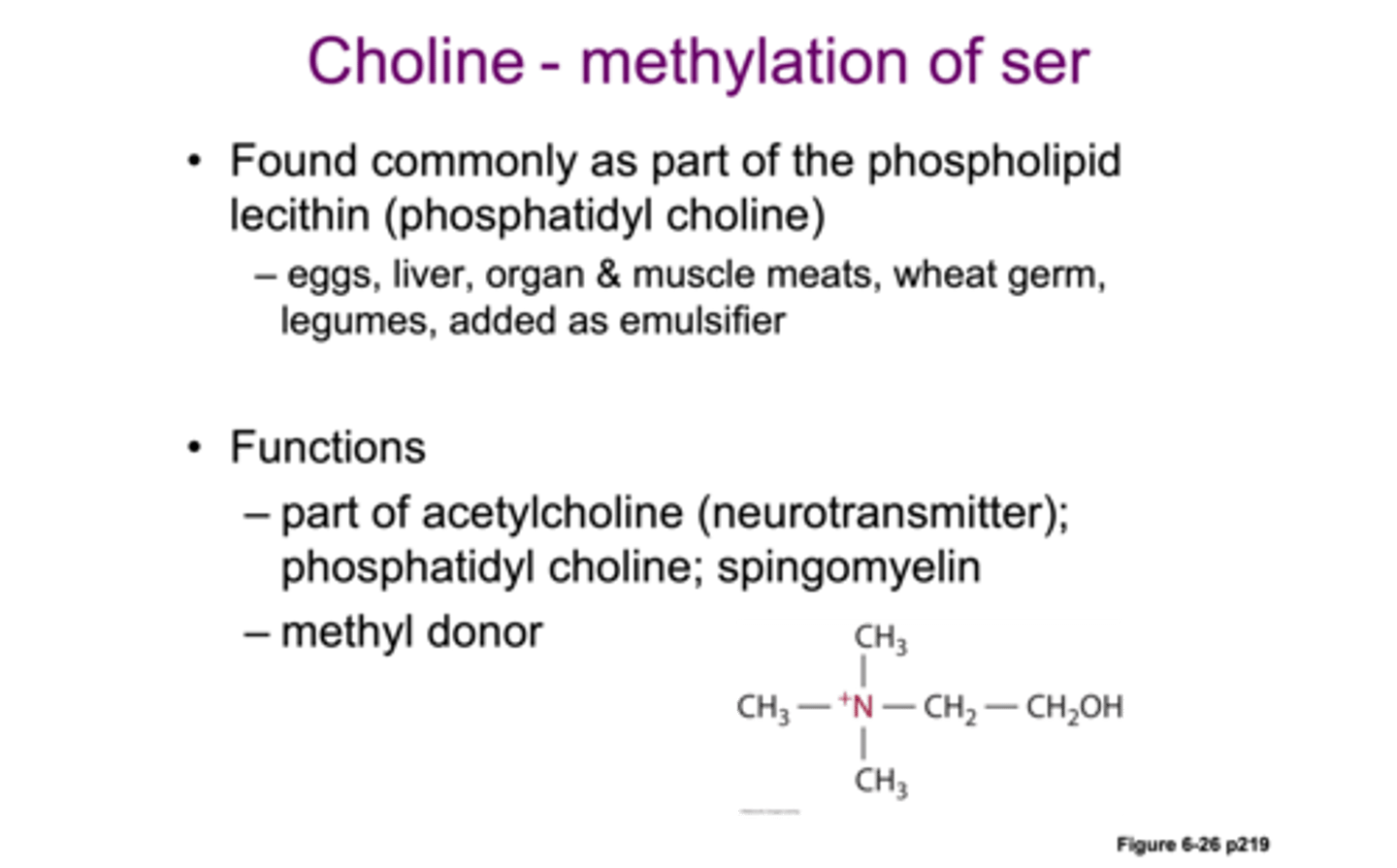
(Functions) Choline
1) cell membrane integrity; Phosphatidylcholine (aka Lecithin) makes up 50% of all the phospholipids in the human body & lipid transport (lipoproteins)
2) Choline = part of acetylcholine & sphingomyelin
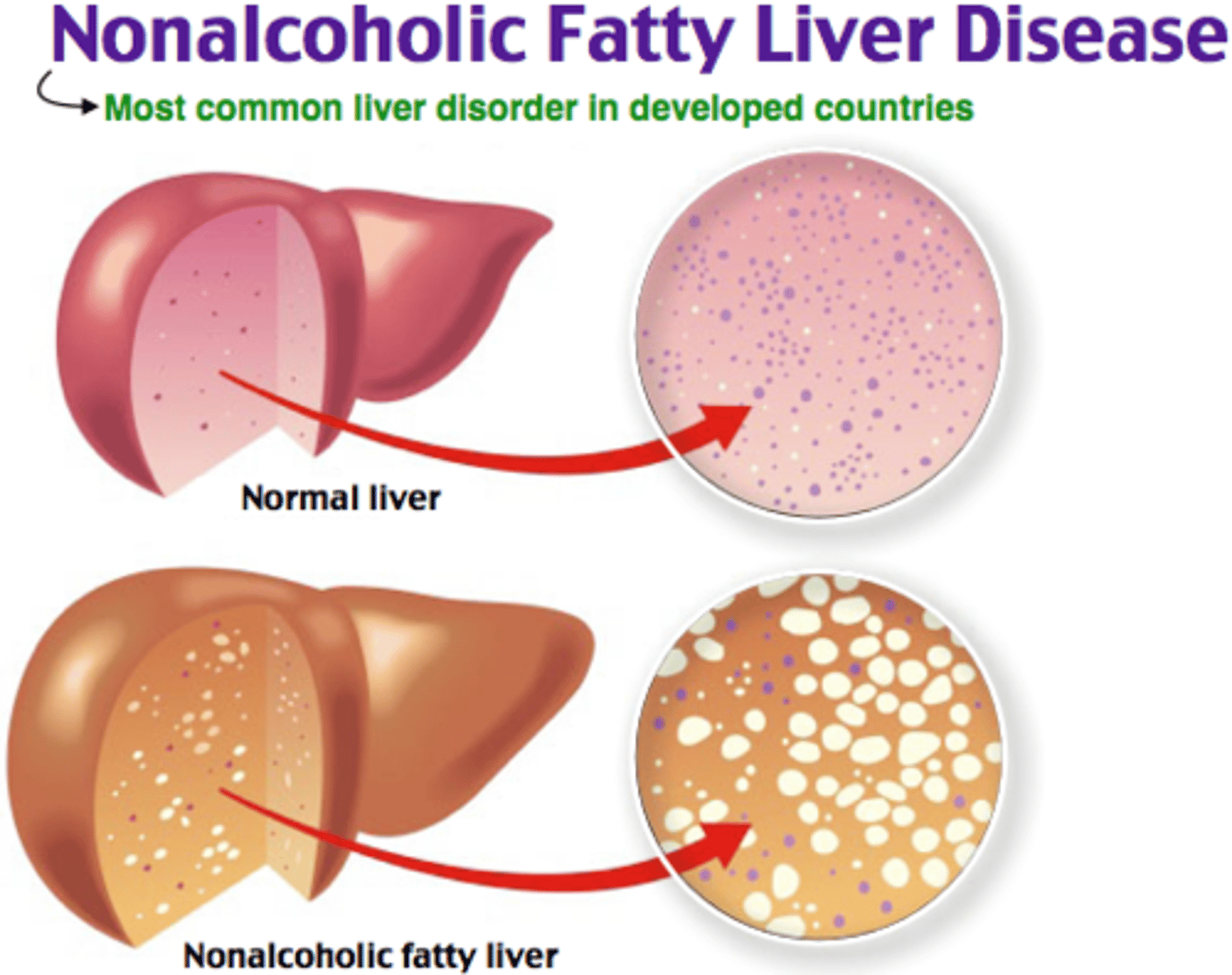
(Deficiency Symptoms) Choline
Choline is required for lipid transport
1) Nonalcoholic fatty liver disease (fat stuck in the liver)
2) Muscle damage (fat stuck in the muscle)
3) Liver damage
(Toxicity Symptoms) Choline
1) Low BP
2) Fishy body odor
3) Excessive salivation & sweating
4) Liver toxicity
5) Cardiovascular disease (Choline --> TMA, TMA gets absorbed and converted into TMAO which has been associated with risk of CVD in some studies)
(Sources) Choline
1) Soy
2) Egg yolk
3) Liver
4) Meats
What population(s) are at risk for Choline deficiency?
1) Pregnant women
2) Genetic conditions (certain SNPs)
What vitamin deficiencies cause neuropathy?
1) Thiamin (B1)
2) Niacin (B3)
3) Pyridoxal phosphate (B6)
4) Cobalamin (B12)
What B vitamins can be produced by gut microbiota?
Riboflavin (B2), Niacin (B3), Biotin (B7), Folate (B9)