2410 exam 3
1/79
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
80 Terms
Recognizing patients experiencing impaired perfusion: Subjective
- Pain ( OLDCARTS)
• due to impaired blood flow to the myocardium or pulmonary emboli. ( usually sign of MI NOT HF)
• pt. will report a precipitating event, such as physical exertion, exposure to cold temperatures, or emotional stress
- Dyspnea on exertion (DOE)
- Orthopnea - discomfort in breathing while lying flat.
• How many pillows do you need?
- Paroxysmal nocturnal dyspnea (PND)
- Dizziness or fainting (Syncope & Near-Syncope)
• headache, numbness, and confusion
Recognizing patients experiencing impaired perfusion: Objective
- Edema
- decreased CO, tachycardia, dyspnea, hypertension
- Capillary refill greater than 2 seconds indicates poor perfusion + Clubbing
- JVD are expected
- reduced urine output
- elevated BNP
- Pale mucous membranes, rubor, diaphoresis, cool skin, cyanosis, pallor, no hair on legs.
- Ankle-brachial index (compare BP in arm to ankle to assess for perfusion problems)
- Gallops, murmurs, rubs.
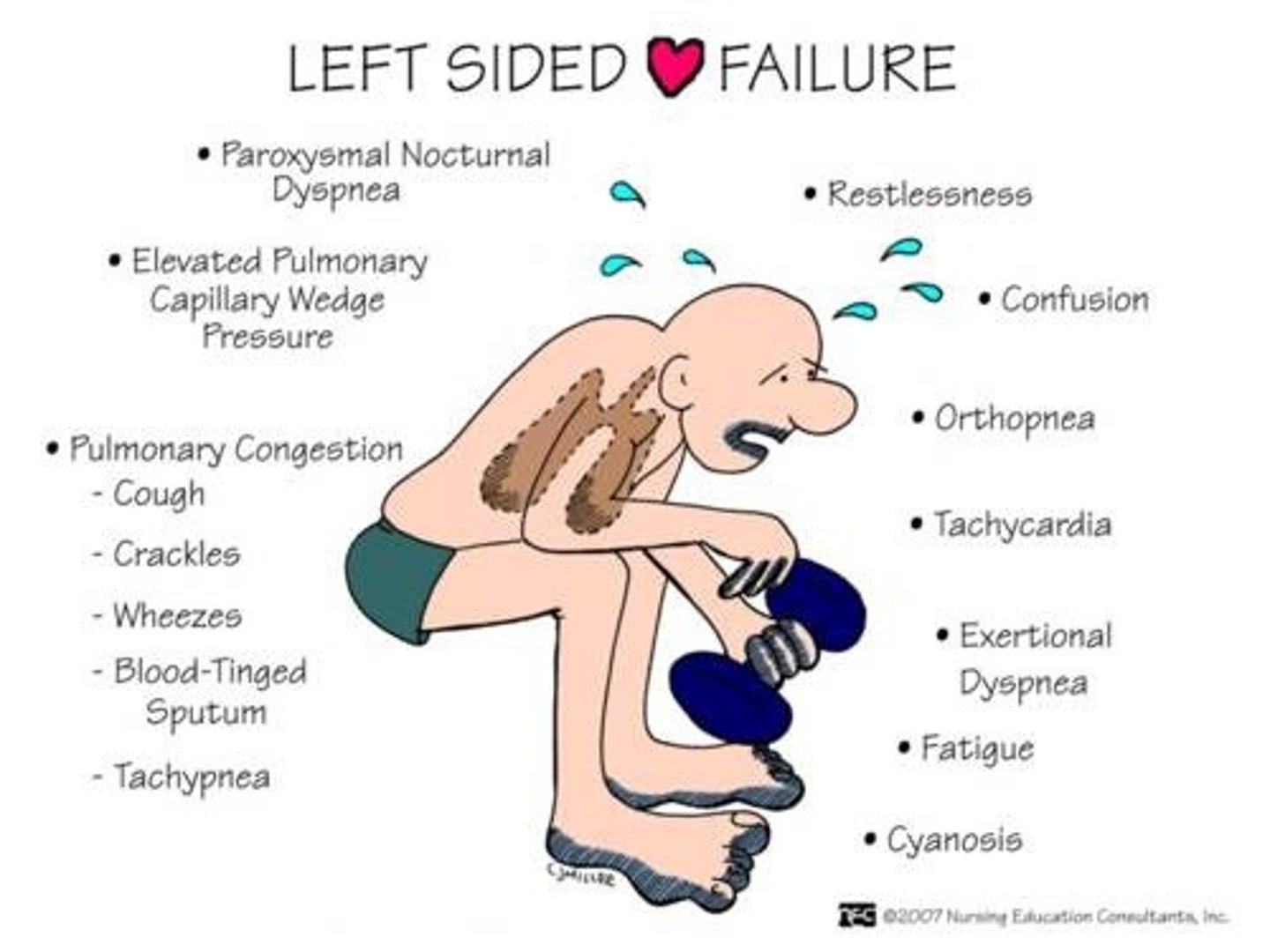
Left-sided heart failure
HF ( HEAVY FLUID)
- Fluid backs up into the Lungs (Left Side)
- inability of the LV to empty adequately during systole or fill adequately during diastole.
- Usually from MI, CAD, ACS
- ↓ EF < 45% == (Normal is 55-60%)
• (<30% = implantable cardioverter defibrillator (IDC) candidate)
LSHF clinical manifestations
- Pulmonary edema
- Dyspnea or Orthopnea
- Pulmonary congestion (Crackles), dry cough
- Blood tinged sputum- pink
- Cyanosis, confusion, restlessness, tachycardia
- S3 heart sound gallop
- Weakness
- Elevated pulmonary capillary wedge pressure
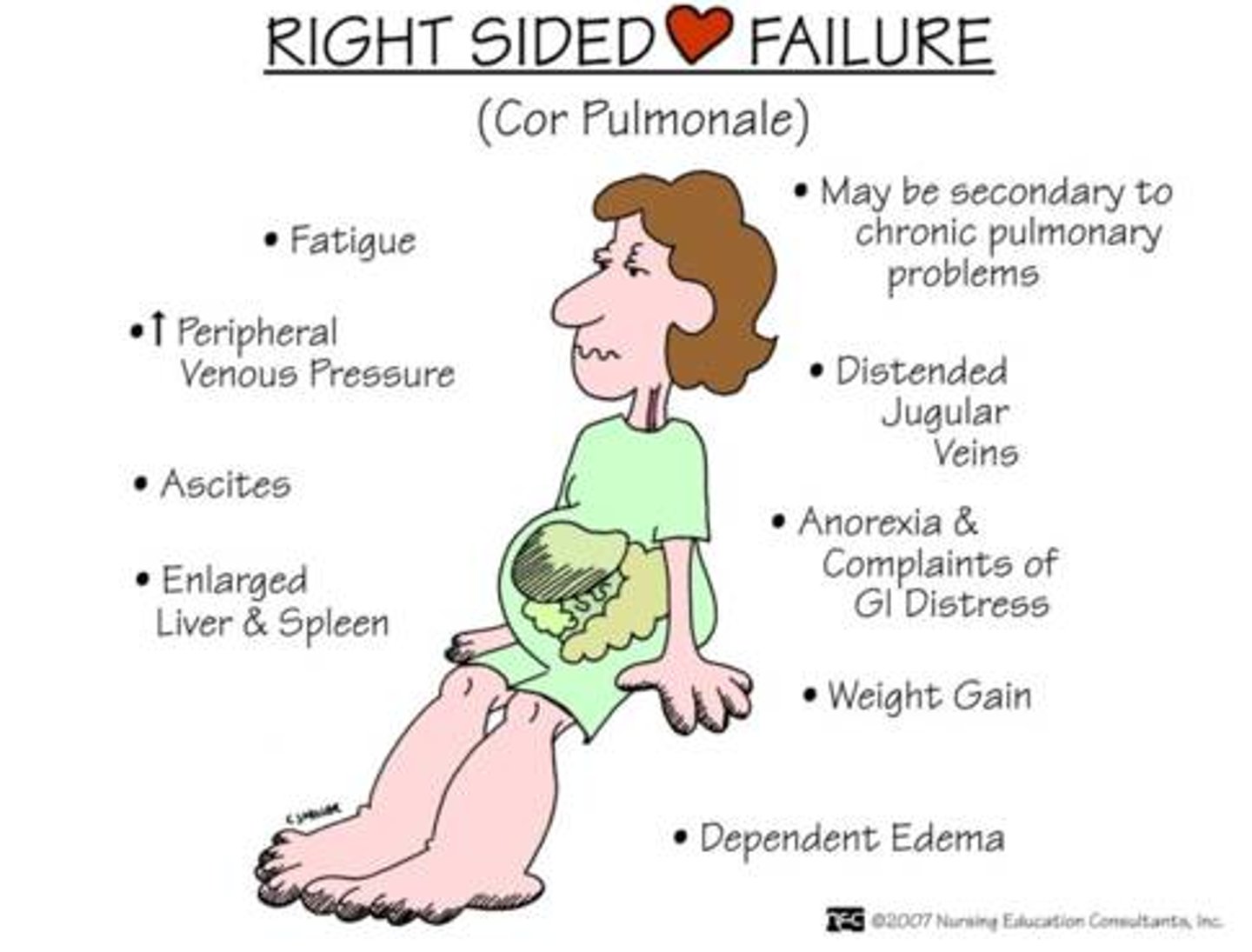
Right-sided heart failure
HF ( HEAVY FLUID)
- Fluid RIGHT backs up into the body. ( Right SIDE)
- Right ventricle doesn't empty effectively
- Most common cause is left-sided heart failure, causes right ventricle to work harder
- Other causes COPD, Smoking, or Obstructive Sleep Apnea
- Pulmonary hypertension (Cor pulmonale) may result
RSHF clinical manifestations
- Peripheral edema
- Weight gain early
• 3 ib IN 1 DAY Report
- JVD
- Fatigue
- Hepatomegaly
- Abdominal ascites (bloating )
- Nausea/ Anorexia- feeling like they don’t wanna eat.
- fluttering or prominent pulsations
- murmus
- Increased peripheral venous pressure
Diagnostics/Labs used to determine heart failure
- BNP ↑
- Hypo/hyperkalemia are sometimes side effects of some cardiac medications
- BUN/ creatinine ↑
- LOW H&H: HF resulted from anemia
- Urinalysis and ABGs
- Chest x-rays
- Echocardiogram
- EKG (ECG)
- Invasive hemodynamic monitoring:
BNP
- hormone secreted by cardiomyocytes in heart ventricles in response to fluid overload/stretching,
• 100- 300 suggest HF
• > 300; mild HF
• > 600; Moderate HF
• > 900; Severe HF
- BNP can also indicate pulmonary embolism, renal failure, and acute coronary syndrome.
EKG (ECG) with HF
Can show dysrhythmias, acute infarction, myocardial ischemia, old MI injuries
Invasive hemodynamic monitoring: with HF
swan ganz catheter
- ↑ Central venous pressure (CVP) OVER 8 NOT Great
- ↑ pulmonary wedge pressure (PAWP)
- ↑ pulmonary artery pressure (PAP)
- ↓ CO
- ↓ venous oxygen saturation (SvO2)
Nursing implications: HF
- ** Furosmide/ Burosmide Priority
- HOB elevated
- Oxygen ( high flow mask)
- Push Morphine+ Furosmide
- End NA+ & fluids
- Look for clearer lung sounds + decreased HR
- Question ANY IV fluids *
Nutritional teaching HF
-Restrict fluid intake (1000 mL)
- Restrict sodium
- Dash diet
- No foods high in K+ ( Green leafy vegetables)
HF home management
-Diet (low NA+ Fluids) - No packaged foods or OTC medicine
-Risk for falls ( change position slowly)
-BP & BNP ( should not be increasing)
-Elevate the legs
-Daily weights (report gain. weight of 3 lb in 1 days)
-Stocking or Ted hose
DR BEDS
ACE inhibitors- Lisinopril
1st choice
- for left ventricular dysfunction, lower BP and increase blood to the heart (does not affect HR)
- Blocks RASS system
- hypotension, Cough, Hyperkalemia, angioedema (AIRWAY Risk) & renal insufficiency
ARBS- Losartan
2nd Choice
- Lower BP ( does not affect HR)
- prevent vasoconstriction
- Promote afterload reduction and vasodilation
- Blocks RASS system
- ARBs do not typically cause a cough
- hyperkalemia- avoid green leafy veggies
betablockers
- decrease cardiac output, HR, and BP
- s/e: bradycardia, bronchospasms, Bad for HF, Blood sugar masking.
- Aruptly stopping can cause rebound hypertension, tachycardia, or rebound angina
Diuretics
- Furosemide (Lasix) & Hydrochlorothiazide promote fluid excretion.
- WATCH FOR HYPOKALEMIA***
- s/s include irregular pulse, muscle weakness
- Consume foods high in potassium (orange juice, bananas)
- spironolactone: avoid foods high in K+
Nitrates
- vasodilator prevents coronary artery vasospasm, reduces preload & afterload, decreases cardiac 02 demands
- s/e: orthostatic hypotension, HEADACHE, nausea & vomiting
- avoid drugs that treat erectile dysfunction, no viagra!
Digoxin
- reduce preload and afterload, reduces HF symptoms, increases myocardial O2 consumption & slowing of HR
- s/e: abdominal pain, anorexia, nausea & vomiting, visual disturbances (yellow or green vision)
- monitor serum K+, Mg, and Ca+, renal & hepatic function
- therapeutic digoxin level: 0.5 - 2ng/mL, draw immediately before next dose is due
- Does not affect BP
Endocarditis causes
disease of the endocardial layer of the heart & heart valves. Impacts aortic and mitral valves.
- dental work, systemic infections, surgery, IV drug use, central venous catheters)
Endocarditis: Clinical manifestations
- Fever, malaise, fatigue
- Roth spots - eye exam
-Osler nodes- OW! painful
-Murmurs
- Janeway's lesions (just jane, not painful)
-Anemia/ Anorexia
-Nail bed hemorrhages
-Emboli
Endocarditis Diagnostics
- Positive Blood Cultures definitive diagnosis: staph/ strep
- ECG - ST elevation (diffusion & widespread)
- Echo: look for change in valve moment
- Labs: elevated CRP, troponins, leukocytosis
- Tx: long term antibiotics
Rifamin for prosthetic valves, if doesn't work- surgery
Pericarditis Clinical manifestations
- inflammation of the sac surrounding the heart
- Precordial pain - sharp, severe, worse with inspiration and often radiating down the shoulder
- Hear a Friction/Rub
- dyspnea with hiccups
Pericarditis: Cardiac tamponade - EMERGENCY
- can lead to Cardiac tamponade
Becks TRIAD
- JVD
- Muffled heart tones/ distant heart sounds
- Hypotension
N/A: Auscultate blood pressure for pulsus paradoxus TX: IV fluids
Echocardiograms
Ultrasound of the heart
- Best tool for DIAGNOSING HEART FAILURE
Transthoracic Echocardiogram (TTE)
- Evaluates size, shape, and motion of heart and measures ejection fraction.
- Noninvasive test takes up to 1 hr.
- Lie on left side and remain still
Transesophageal Echocardiogram (TOE)
- Passed through mouth into esophagus to provide images of heart
- Informed consent; NPO for 6 hr prior
- may be sedated
- Monitor for return of gag reflex; keep HOB at 45.
Stress test
- Pre:
• Consent signed
• Wear comfortable clothes
• Fast for 2-4 hrs before
• hold b-blockers for 24 hours before the test
• avoid caffeine-containing foods 24 hours before the test
- Intra
• Apply 12 lead
• Report Chest pain, SOB, or dizziness
- Post
• Check BP
Acute Coronary Syndrome
spectrum of conditions resulting from thrombus formation in the coronary arteries
- Range from unstable angina, NSTEMI, STEMI
• unstable angina: No necrosis
• NSTEMI: partial necrosis
• STEMI: Transmural necrosis- ST elevation AKA heart attack
Acute Coronary Syndrome MONA
- Morphine sulfate (priority in managing pain for ACS!)
- Oxygen
• administer at 2-4L/min
- Nitrates
• Sublingual Can repeat every 5 minutes x 3
• Can have side effects- hypotension (Contraindicated), severe headache (have some Tylenol on hand)
- Aspirin
• relieve acute pain and restore coronary blood flow
• Administered with Nitroglycerin at the onset of chest pain.
• There is a risk for bleeding and bruising
Acute Coronary Syndrome EKG
- OBTAIN 12 LEAD ASAP TO DETERMINE IF PATIENT HAD MI
- ST depression & T wave inversion = Ischemia/ Unstable Angina
- ST elevation = Injury/ NSTEMI
- ST elevation + widened & deep Q wave = Infarction/ STEMI
- Pathologic Q waves often accompanies STEMI, indicative of COMPLETE CORONARY OCCLUSION
Ischemia
lack of blood flow
Infarction
death of tissue; no blood flow
Acute Coronary Syndrome Chest Pain
- report chest pain that is not relieved by rest or nitroglycerin.
• heavy/ dull
• jaw/ arm/ shoulder
- CALL 911
- IMPLEMENT MONA
- obtain 12 LEAD EKG
- lasting > 20 minutes is highly suggestive of MI
Unstable angina
- new in onset, worse at rest.
- first clinical sign of CAD.
- unpredictable and must be treated immediately
- ST depression and/or T wave inversion
Lasts more than 20 minute
Stable angina
- occurs intermittently over a long period
- provoked by physical exertion, stress, or emotional upset.
- resolved by resting, calming down, using sublingual nitroglycerin
- pt describe a pressure, heaviness, or discomfort in the chest.
lasts less than 15 minutes
Cardiac cath lab
if the patient has chest pain + ST elevation, take them straight to the cardiac cath lab to confirms diagnosis and extent of heart
Reperfusion- cath lab
- uses PTCA for door-to-balloon to restore coronary perfusion in cases of MI
• TX FOR Acute Coronary Syndrome
- pharmacological interventions used only for STEMI include
• thrombolytic agents (alteplase, reteplase & tenecteplase) to dissolve clot and open artery
-high risk for stroke
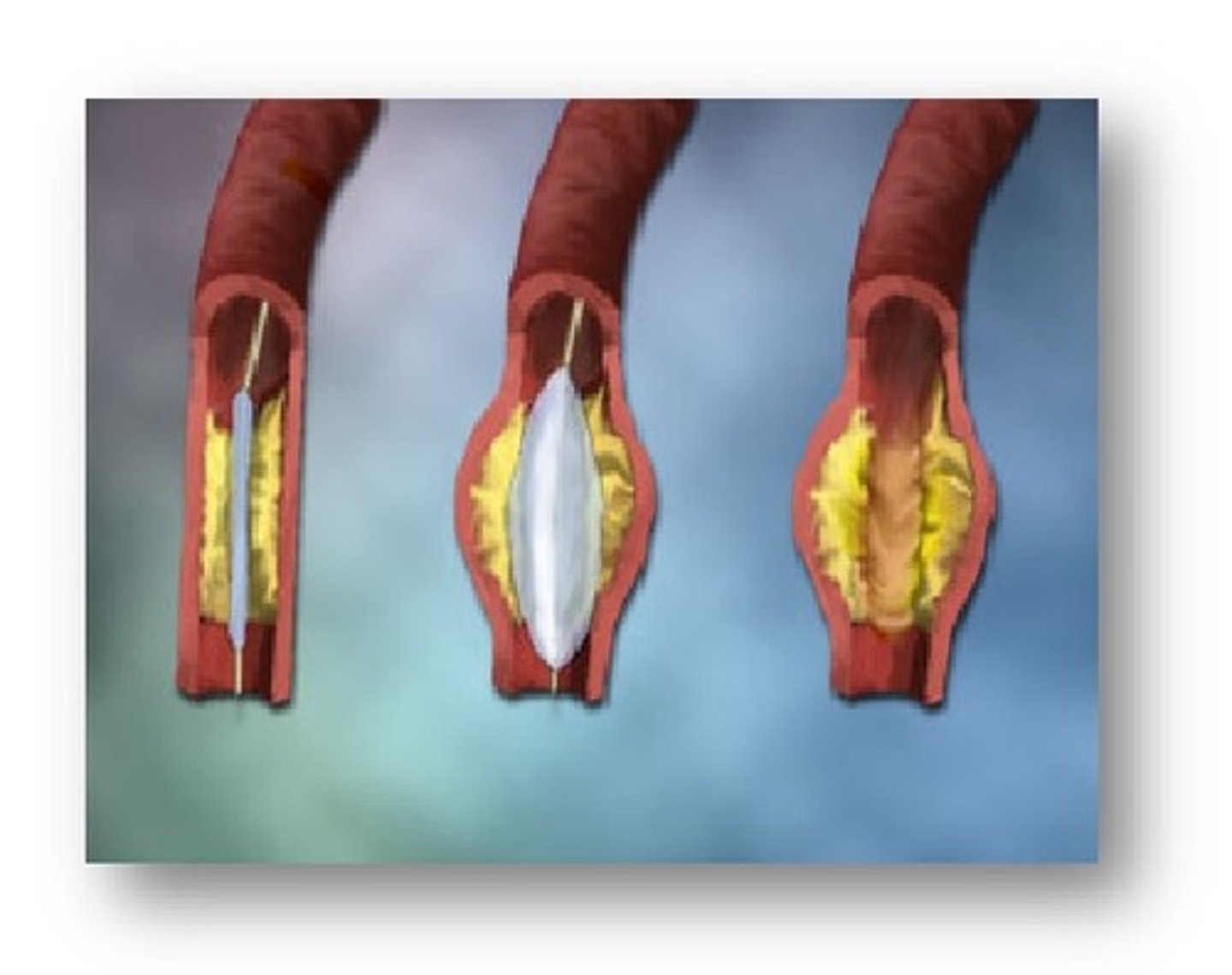
Percutaneous Transluminal Coronary Angioplasty (PTCA)
- balloon/stent to restore coronary artery blood flow when arteries are narrowed or clogged.
- a femoral introducer/sheath
• Complications: hematoma, pseudoaneurysm, infection over femoral artery, kidney injury from contrast dye. Ask about allergies to iodine/shellfish
Cath lab Pre
- Check for allergies to iodine or shellfish
- Assess for underlying kidney disease( expect Dialysis)
- Patients will need hydration pre & post-procedure
- Consent must be obtained prior to the procedure
- Mark pulse sites
Cath lab Post
- Monitor site for bleeding (bruising on back, side or perineum) & chest pain
- **will see TACHYCARDIA & DECREASED URINE OUTPUT FIRST**
- Frequent neurological assessments; mentation, hand grasps
• signs of stroke
- Leg needs to remain straight and immobilized (no restroom)
Cardiogenic Shock (Pericardial Tamponade)
life-threatening; heart suddenly can't pump enough blood to meet your body's needs
- BECKS TRIAD:
• JVD
• Muffled or distant heart sound
• Low blood pressure
Hypertension Assessment
- Palpate pulses at major sites ( Radial, Dorsal)
- Assess blood pressure in both arms
- Check temperature differences in lower extremities
- Capillary refill
- Assess for bruit with Doppler or stethoscope
- Check for family history of Coronary Artery Disease (CAD)
- Ask about life stressors
Hypertension Risk factors
smoking, obesity, sedentary lifestyle, genetics, age, poor diet
Low HDL + High LDL , Diabetes
Hypertension Signs/symptoms
-Often labeled the "silent killer" due to lack of symptoms
- (Most common symptom is Headache)
-Fatigue, palpitations, angina, dizziness, SOB
HF PADS
Hypertension Common medications
- Diuretics
- Adrenergic inhibitors
- Directvasodilator
- Calcium channel blocker
- ACE inhibitors
- ARBs
Hypertension: Medication regimen compliance
- Take BP at home
- Follow-up with PCP every 3 months
- Restrict sodium intake
- Don't suddenly stop drugs
Peripheral Arterial Disease: risk factors
- Atherosclerosis, CVD, Diabetes, Hypertension, high cholesterol, Smoking
- African Americans are affected more than any other group
Peripheral Arterial Disease: Signs/symptoms
- Cool to touch, white, hairless & Shiny, pulseless, report more pain.
- Very little drainage, Little tissue granulation (pale/very light pink) OR necrotic/black
Peripheral Arterial Disease: Nursing implications
- Meds, surgery,( revascularization), put a stint. Improve blood flow!
- palpate posterior tibial pulse
- (DON'T USE HEATING PAD), CMS checks
Peripheral Arterial Disease: Teaching – diet, exercise, positioning
- Prevention depends on disease process ( hypertension, high cholesterol) Lifestyle + pt. Education ( Smoking cessation)
- DASH diet, avoid alcohol, nicotine & caffeine
- Exercise- Promotes collateral circulation
- Feet should not be elevated above the heart.
Peripheral Arterial Disease: Home care management
- Exercise regimen
- Always wear shoes to avoid injury
- Use mild soap and room temp water to wash feet/legs
- Avoid alcohol and tobacco
- Apply lubricating lotion to dry areas of legs/feet
pregnancy induced cardiomyopathy
- Monitor for cardiac decompensation 24-48 hours after birth * HIGH RISK AT THIS TIME!!
• Difficulty Breathing - Orthopnea
• Cough - crackles in lung bases
• Irregular pulse
• Edema
• JVD
• Tachypnea
• Cyanosis - low O2 saturation
- Oxygen saturation - optimal positioning (elevate HOB)
- Avoid Valsalva maneuver - use stool softeners**
**ACE inhibitors/ ARBs should not be used
Bleeding/clotting Assessment
- Blood in urine/stool
- Low blood count
- Embolus (Pulmonary)
- Drug therapy (Plavix)
- Joint problems
- Ascites
- Warfarin History
- Skin: Pallor/ Petechiae
- Lethargy/ Fatigue
- Yellow/Jaundice
BLED JAW SLY
Bleeding s/s (hypocoagulation)
- Bleeding gums/nose
- Oozing blood from IV site,
- Blood in stools, emesis, or urine,
- Skin: pallor (too much blood loss), petechiae, purpura
- Hematomas, hemoptysis, , hypotension
- Orthopnea
- Tachypnea, tachycardia
BOB SHOT
Conditions resulting in hypo-coagulation
- Aplastic anemia (body doesn't make enough blood cells
- Thrombocytopenia (decreased platelets)
- Idiopathic thrombocytopenic purpura (platelets greatly reduced)
- Hemophilia (Factor VIII deficiency)
- HIT
Thrombocytopenia (decreased platelets) Contributing factors
- Platelet disorders (ITP, HIT, DIC)
- Leukemia
- Aplastic Anemia
-Trauma
-Enlarged spleen
-Liver disease
-Ethanol use
-Toxins/ drugs (chemotherapy,/Aspirin)
-Sepsis (hepatitis C virus, HIV, cytomegalovirus)
PLATELETS
ITP (idiopathic thrombocytopenic purpura)
Own body attacks platelets and blood can't clot -> leads to bleeding.
* emotional disease (lots of fatigue)
- TX: corticosteroids (e.g., prednisone, methylprednisolone) are used initially to treat ITP
Hemophilia
NO coagulation to stop bleeding.. Love to bleed.
* Hereditary
- Decreased clotting factors
• Deficiency of factor VIII (Von willbrand )
- often caused by liver failure + vitamin k deficiency
Clinical Manifestation of Hemophilia
- Easy bruising (Ecchymosis)
- Hematomas
- Prolonged bleeding after cut or surgery
- GI bleed, nose bleeds, hematuria
-Hemarthrosis- bleeding in jounts/muscles- may need joint replacement of hip/knee
Hemophilia Treatments
- A-B-C's: stop the bleeding
1. Factor VIII infusions (most common)
2. Desmopressin (DDAVP)
hemophilia education
- medical alert bracelet
- Avoiding contact sports
- home administration of factor VIII
- bleeding interventions
- NO MI Injection
- no aspirin
Liver clotting factors
- liver plays a function in formation of Vitamin K
- labs:
• ↑ PT/INR, & PTT time
•. ↓ platelets, H&H
Conditions resulting in hyper-coagulation
- polycythemia
- sickle cell anemia
- factor V Leiden
- DVT
- surgeries
factor V Leiden
- Hormones- it increases your risk for thrombus.
- S/S ( VTE, DVT/ Thrombosis, possible fetal loss )
Hyper Coagulation Contributing factors
- History of blood clots
- Chronic heart failure & AFIB
- Genetics
- Central Venous Catheter
- Overweight
- Smoking
- Cancer
polycythemia
- Blood disorder
• Overproduction of RBCs
- ↑ RBC's, WBC's, Platelets
- look for dizziness, HTN, petechiae, enlarged spleen
- comp. include DVT, stroke, myocardial infarction, and angina pectoris.
polycythemia: management
ABCs
- Aspirin may be used to decrease clots
- Blood letting (Phlebotomy= TAKE BLOOD OUT; TOO MUCH RBC)
- Chemotherapy sometimes prescribed but may also lead to leukemia
- Hydroxyurea may be prescribed. Helps lower blood counts.
sickle cell: management
- affects the shape of all RBC’s, which carry O2 around the body
- Oxygen
- Pain medication (Morphine) !
- Medication Hydroxyurea
- Hydration! 250 mL/hr x 4 hours
- Packed RBCs ( watch for iron toxicity)
- Prevent infections
sickle cell : teaching
- warm compresses, no sports, avoid sick kids!
- Maintain hydration
- Avoid high altitudes
- Keep current on all immunizations
- take folic acid supplements
DIC S/S
- DIC has both bleeding and thrombotic
• Acute: Bleeding episodes (ecchymoses, petechiae, purpura, blood oozing from oral mucosa, sites of trauma, catheters and IV lines,
• Chronic: thromboembolism, tissue hypoxia, infarctions
* kidney damage and oliguria, leading to failure.
Lab values associated with DIC
- D-Dimer-confirms diagnosis: increased
- PT/PTT prolonged
- Thrombin prolonged
- Fibrin split products elevated
- Fibrinogen Levels decreased
- Platelets Reduced
- Decreased Hemoglobin
DIC Treatment
- O2, IV fluids, TX w/ blood thinner initially
- Fresh frozen plasma
• Platelet transfusions
• RBC transfusions
Virchow's triad
DVT CAUSES:
Pulmonary embolism (triad = blood stasis, endothelial damage, hypercoagulation)
Warfarin (Coumadin)
( not safe during pregnancy)
- prevents synthesis of factor VII, IX,X
- Prevents Venous thrombosis & PE
- prevents A Fib
- LABS: monitor INR for therapeutic PT/INR 2-3
• (2.5-3.5 w/high risk embolism)
- antidote: vitamin K
-Complications: Hemorrhage, Hepatitis, Toxicity
Heparin
( safe during pregnancy)
-- Stroke, PE, DVT
- monitor aPTT therapeutic (46- 70 seconds)
• 30 mins before next dose or q4hr if continuous
- PT/INR- The higher the # the higher the chance of bleeding
- monitor platelet count q2-3days: HIT
- antidote: protamine sulfate
- Complications: - Toxicity, Hemorrhage, Epidural/spinal hematoma, HIT
LMW Enoxaparin/Lovenox
- prevent angina, ST elevation in MI. SubQ
- Labs: Heparin anti-Xa to titrate doses, therapeutic range 0.5-1 unit/mL
- Antidotes: protamine sulfate
- Complications: Neurologic damage, HIT, Toxicity
HIT Signs & Symptoms
- Venous thrombosis
- Pulmonary embolism
- Thrombosis to hands and feet
HIT Risk Factors
longer use of heparin, post-surgical thrombo-prophylaxis, being female, exposure to unfractionated heparin.
HIT labs + tx
- Evident by low platelets
- Monitor platelets esp. in first month
- Stop heparin if < 100,000
• tx anticoagulation therapy i.e. agatroban