ANAT2012 - Module 8 Brain Injury
1/88
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
89 Terms
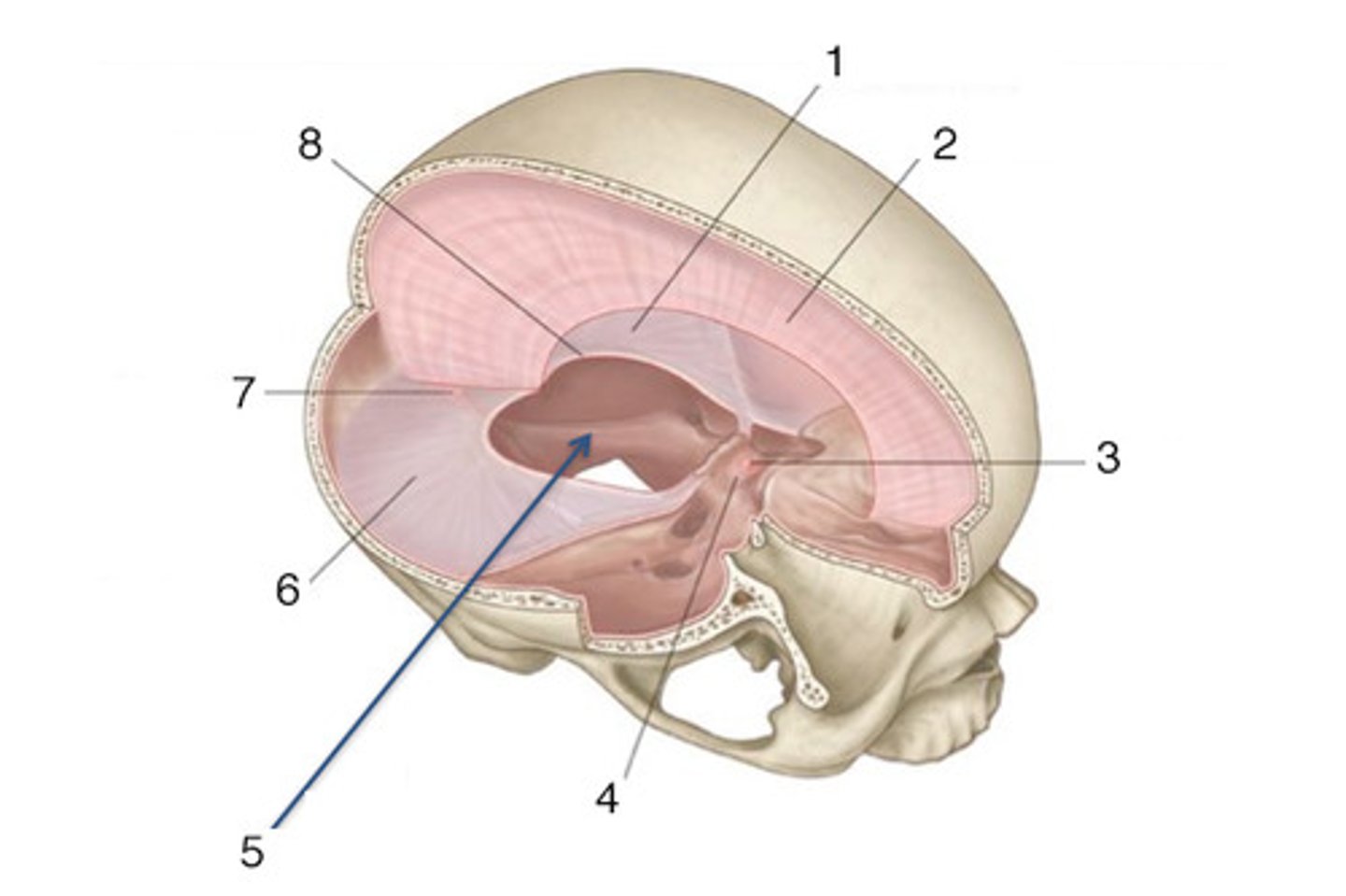
2 types of dura mater
periosteal and meningeal
3 purposes of dural folds
1. partially separate intracranial compartments
2. hold them together
3. restrict movement
describe falx cerebri
- fold of dura mater that dips into the longitudinal fissure and divides cerebral hemispheres
- acts as a seatbelt -> if left hemisphere moves, falx cerebri reduces movement of right hemisphere

describe tentorium cerebelli
separates cerebral cortex (supratentorial) from cerebellum (infratentorial)

what is tentorial notch
- anterior free edge of tentorium cerebella
- encircles midbrain
- allows cerebellum and midbrain to communicate
purpose of CSF for brain
provides buoyancy and cushioning of mechanical forces. Brain would be distorted by its own weight if not suspended in CSF
describe brain's storage mechanisms for glucose
is not effective - requires continuous and copious blood supply
where can fluid leak throughout brain interstitial space
1. fluid leaks across BBB and enters interstitial space
2. fluid flows into choroid plexus which creates CSF, then flows into ventricles
3. CSF from ventricle flows across ependymal lining into interstitial space
4. CSF flows into spinal cord through subarachnoid space
describe texture of brain tissue (4 points)
1. inhomogeneous
2. cells include neurons, glia, grey/white matter
3. ECM composed of 70% interstitial fluid and various fibres/cells
4. fibre direction and length is inhomogeneous as well
describe the 2 ways external loading to head may affect intracranial contents
1. direct contact - displacing or deforming skull, has high focal connective energy and low cranial momentum (e.g. fixed head + blow)
2. differential motion - motion between skull/dura and intracranial contents. Has low kinetic energy and large momentum (rotation, tensile, and shear forces)
describe linear impact to head
- in line with centre of gravity of brain
- doesn't cause rotation of brain inside skull
- skull absorbs more stress, more likely to fracture, less likely to damage brain
describe oblique impact to head
- more common
- produces both linear and rotational kinematics
- causes diffuse axonal injury where axons snap by shear impacts
what is poroelastic
brain is poroelastic - it is a porous, fluid-saturated solid
what is the resistance to fluid flowing throughout brain and why
high resistance - very low permeability of fluid vessels
what is a bulk modulus - does the brain have high or low bulk modulus
if object is equally pressured on all sides, how much pressure is required to change the volume.
brain has high bulk modulus = doesn't change volume easily
does brain have high or low compression modulus
very low = extremely soft/compliant (<5 kPa)
does brain have high or low shear modulus
very very low shear modulus (<1kPa), extremely sensitive to shear. When different layers of tissue move differentially to each other, fine connections (axons) between them break easily
is brain viscoelastic
yes , except for infants who are insensitive to the strain rate
is white matter or grey matter stiffer (in general)
white matter (in general) but it depends on direction of force because white matter fibres run in many different ways.
is grey matter anisotropic
no
do smaller or larger brains tolerate greater acceleration/deceleration forces better
smaller brains
what is an acquired brain injury
any brain injury that occurs after birth (not congenital) - can be trauma, stroke, tumour, poison, infection, anoxic episodes
definition of traumatic brain injury (TBI)
traumatically induced structural and/or physiologic disruption of brain functions a result of external force
4 clinical signs of traumatic brain injury (TBI)
1. consciousness - loss or decreased level
2. memory - any loss of memory for events immediately before or after injury
3. mental state - altered (e.g. confusion, slowed thinking)
4. neurological deficits - weakness, balance, visual, speech, sensory
2 main categories of traumatic brain injuries
diffuse and focal
4 types of diffuse traumatic brain injuries
1. concussion
2. diffuse axonal injury
3. blast (e.g. explosion)
4. abuse head trauma/shaken baby syndrome
3 main types of focal traumatic brain injuries
1. contusion
2. haematoma
3. penetrating (e.g. knife through skull)
5 types of haematoma
1. epidural
2. subdural
3. subarachnoid
4. intracerebral
5. intraventricular
5 classification schemes for TBI
1. primary or secondary injury
2. focal, multifocal, or diffuse
3. physical mechanism
4. symptoms/severity
5. pathoanatomy - relate where lesion of brain is to symptoms
likely injuries from linear impact
skull fracture, contusion, epidural haematoma (force is absorbed by skull)
likely injuries from oblique impact
DAI, contusion, subdural/intracerebral hematoma (force absorbed by brain and rotation)
what are primary vs secondary TBIs
primary = what immediately happens to skull or brain
secondary = consequences caused by primary injuries that can occur minutes to weeks after injury.
what are examples of primary TBIs
skull fracture, cerebral laceration, contusion, haemorrhage, BBB compromise, DAI, necrotic cell death
what are examples of secondary TBIs
- cerebral blood flow deregulation
- increased intracranial pressure + oedema
- hypoxic ischaemia
- neuroinflammation
- excitotoxicity / Ca2+ influx
- neuronal death
what can occur after secondary traumatic brain injuries
neurobehavioral deficits e.g. cognitive disfunction, sleep disorder, seizure, psychosis
what is diffuse axonal injury (4 points)
1. leading cause of morbidity from TBI
2. axons are vulnerable: viscoelastic (rapid deformation = brittle), being highly aligned in tracts (anisotropic), and can only strain 6-7%
3. under highly tensile stress, axons can snap (axotomy) which damages connections/communication in brain
4. occurs more with unrestricted head because it allows rotational acceleration which increases tissue deformation and axonal tension
how does vascular haemorrhage occur
tearing of blood vessels, expanding and filling potential or true spaces. Potential spaces = epidural and subdural spaces. True spaces = subarachnoid space
haemorrhage vs haematoma
haemorrhage = active bleed that is currently bleeding
haematoma = pool of blood, usually clotted, sitting within brain
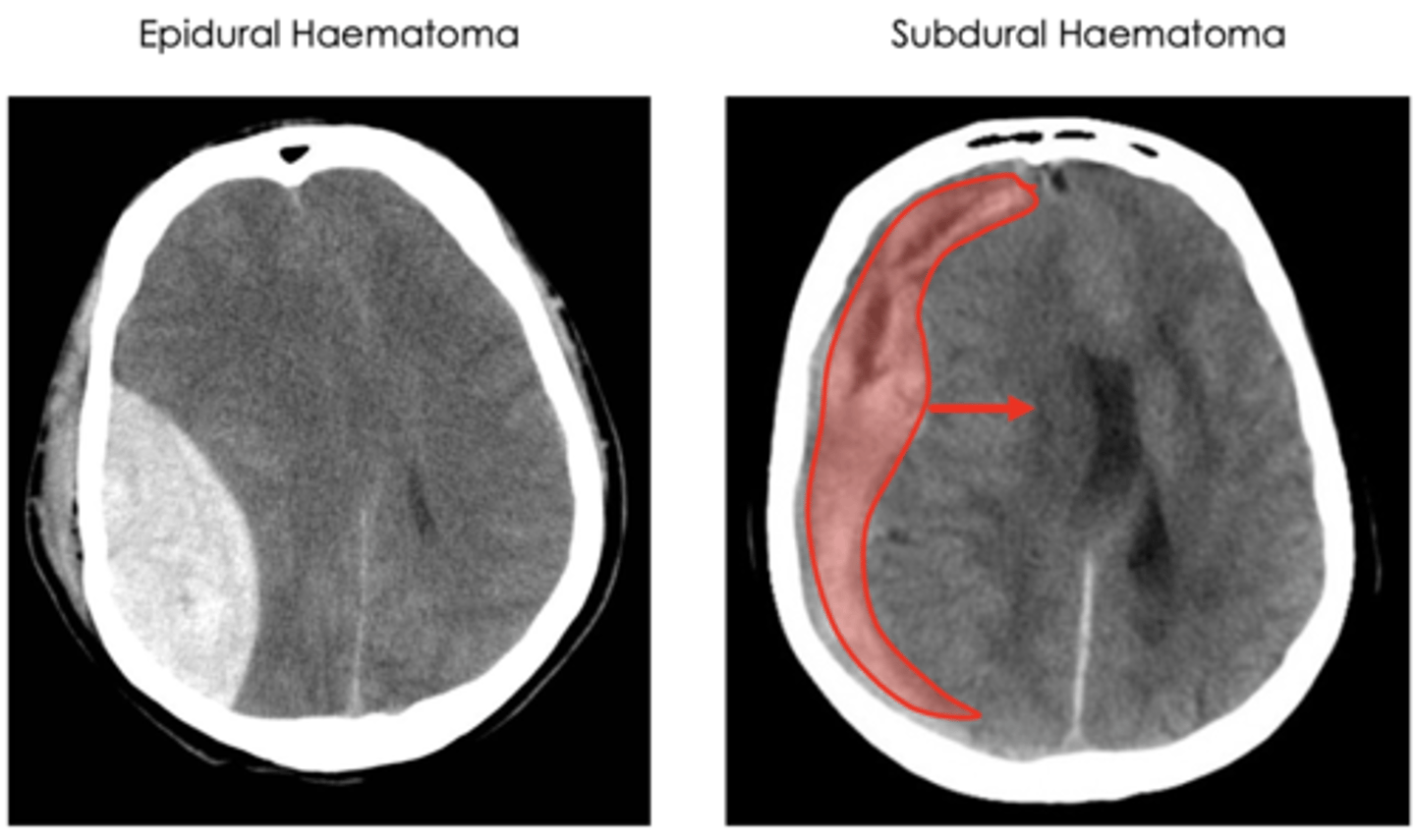
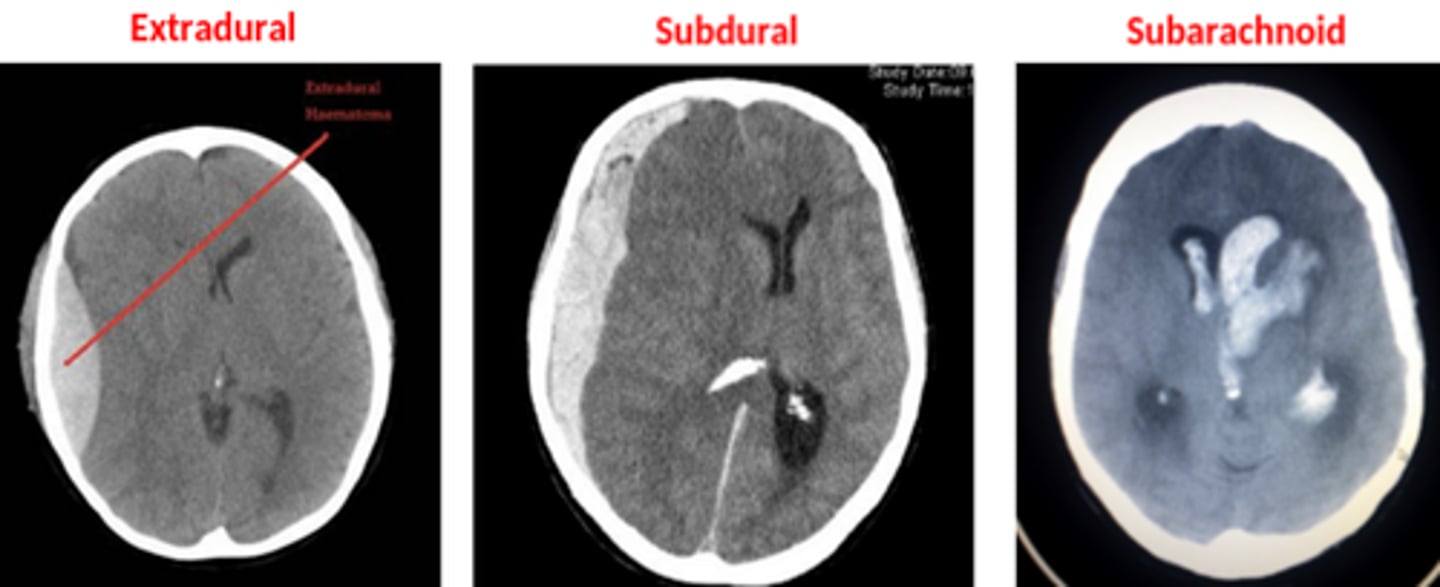
describe an epidural haematoma (common MOI, imaging results, treatment)
- occurs with skull fracture which slices and ruptures the L/R middle meningeal artery - pressure from bleed separates dura from bone
- shows biconvex haemorrhage on x-ray because expansion of blood is contained by tight adherence of dura mater to skull
- treated with prompt surgical evacuation
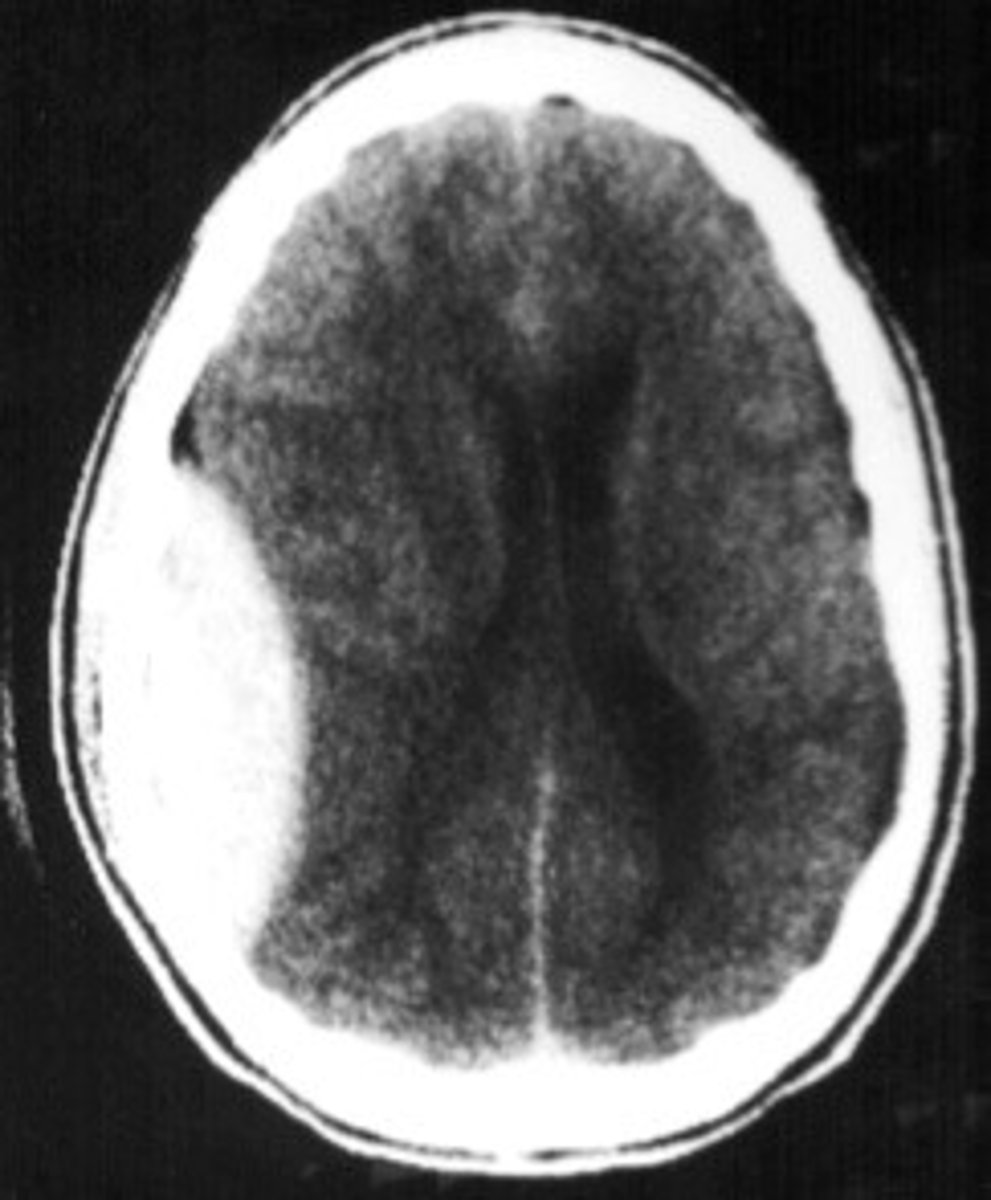
describe a subdural haematoma (common MOI, imaging results, treatment)
- occurs with violent shaking of head which snaps bridging veins between dura mater and subarachnoid space, haematoma causes mass effect midline shift of brain
- classified with crescent-shaped haematoma not contained by dura, but is contained by falx cerebri and tentorium cerebelli
describe a subarachnoid haematoma (common MOI, diagnosis, treatment)
- various trauma or stroke causes damage to cerebral arteries, which bleed into subarachnoid space
- most likely caused by rotational acceleration and breakage of vessels
- vasospasm can occur in attempt to reduce blood flow to bleeding vessels, may cause focal areas of ischaemia
- blood mixes with CSF, so can be diagnosed with blood in spinal tap
describe intracerebral haemorrhage and MOI
haemorrhage of small arterioles and capillaries in brain tissue (parenchymal vessels)
- commonly acceleration/deceleration trauma
- disrupts BBB and lets in harmful molecules
what is an inter-ventricular haemorrhage
bleed directly into ventricles of brain
what is a brain contusion
focal surface bruises - cell death, bleeding, oedema of surface brain tissue
which part of brain is most susceptible to contusions
crests of gyri
what other injury is associated with brain contusions
subarachnoid haemorrhage
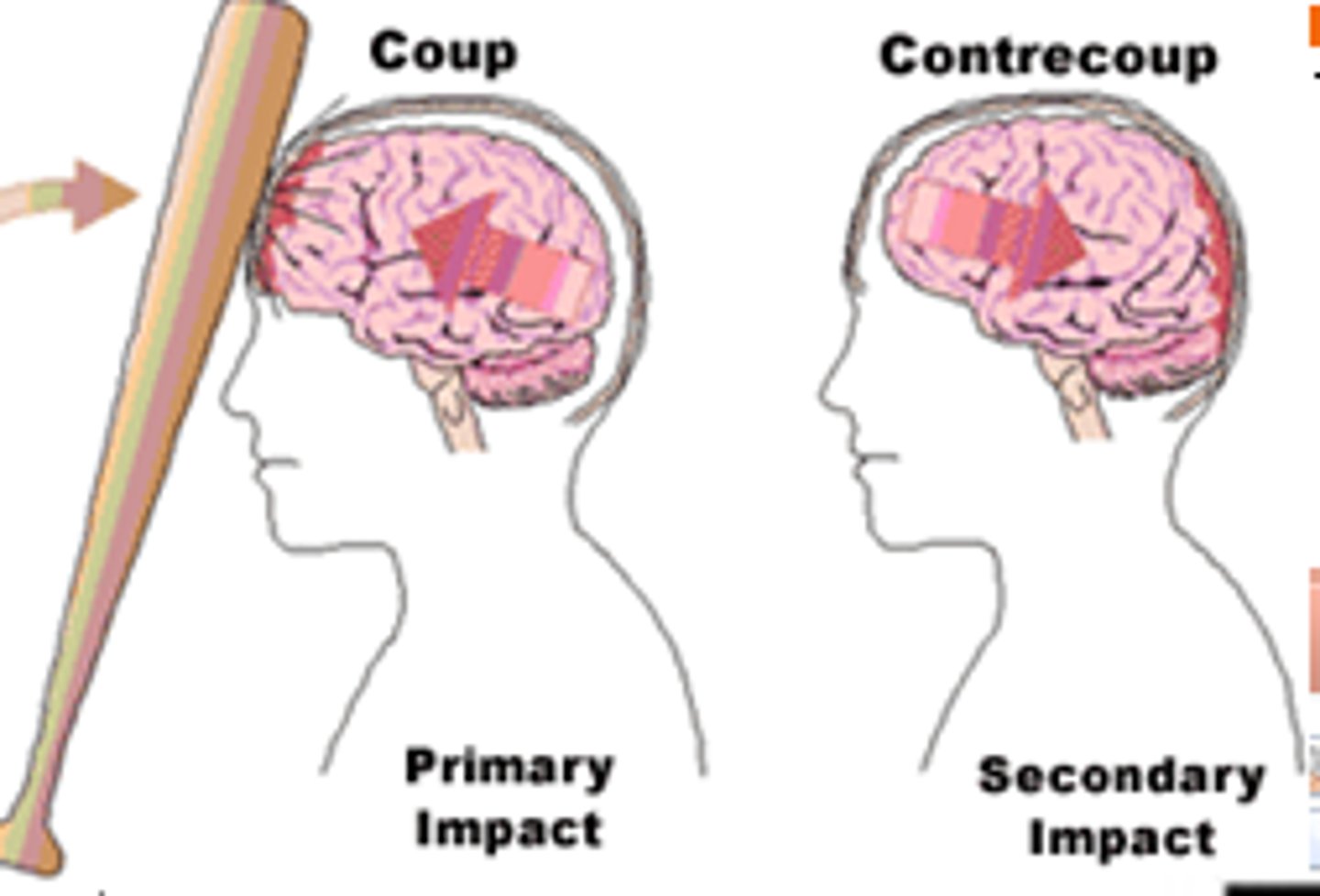
what is a coup and contrecoup
coup = site underneath impact due to compression
contrecoup = site on opposite side of brain where it impacts the skull. Can be used to show direction of impact
what is the preferred imaging modality for acute traumatic brain injuries
unenhanced brain CT scan
advantages and disadvantages of unenhanced brain CT scan
advantages
- CT scans are available, fast
- accurate for detecting intracranial haemorrhage.
- can display mass effect, distinguish brain contusions from haematomas. Excellent for detecting depressed facial and skull fractures
disadvantages
- low resolution - patient with significant deficit could show 'normal' scan
- T2 MRI superior for subacute or chronic contusions
what are the score descriptions for 'eye opening' category on Glasgow coma scale
4 = spontaneous
3 = to speech
2 = to pain
1 = none
what are the score descriptions for 'best verbal response' category on Glasgow coma scale
5 = oriented
4 = confused
3 = inappropriate words
2 = incomprehensible sounds
1 = none
what are the score descriptions for 'best motor response' category on Glasgow coma scale
6 = obeys commands
5 = localises to pain
4 = withdraws from pain
3 = abnormal flexion to pain
2 = extension to pain
1 = none
what GCS score means mild, moderate, and severe
mild = 15-13
moderate = 12-9
severe = <9
what factors affects mortality rate of TBIs
time to regain consciousness. Once >6 hours, chance of survival is much worse
describe a mild GCS TBI
- most common
- lost consciousness <30min
- post-traumatic amnesia <24 hours
- no macroscopic damage
- physical = fatigue, nausea, and altered balance, vision, hearing
- cognitive = attention, concentration, memory, etc
- behaviour = insomnia, irritable, anxious, depressed
what happens if blood flow to brain is reduced from 55mL/min to 20mL/min and even further to 10mL/min
20mL/min = neurons stop generating electrical signals
10mL/min = necrosis and infarct
what is a stroke and what are the two categories
stroke = abrupt vascular insufficiency
categories = ischaemic and haemorrhagic
describe an ischaemic stroke - how does it occur
- sudden blockage of blood flow to brain and an area is deprived of blood
- most common form of stroke
- occlusion of artery occurs via a thrombus (blood clot) or embolus (plaque or thrombus breaks off and blocks artery downstream)
what is a transient ischaemic attack (TIA)
thrombus/embolus blocks vessel temporarily, then is moved away due to building pressure of blood. Causes temporary symptoms as neurons stopped electrical activity but didn't die.
general pattern of infarction in ischaemic stroke
- occurs in one half of brain because an artery only supplies one side.
- territory depends on size and location of occlusion because each artery supplies different areas.
what happends when ischaemic stroke affects branches of basilar arteries
supplies brain stem => cranial nerve defects
describe a haemorrhagic stroke
ruptured vessel leaks blood into brain.
MOI of haemorrhagic stroke
- hypertension (weakens walls)
- rupture of an aneurysm
- vascular malformation
- complication of anticoagulation medication
incidence, mortality, MOI of spontaneous intracerebral haemorrhage
- 10-15% of strokes
- high morbidity and mortality
- main MOI is hypertension
common places for intracerebral haemorrhages
most common = basal ganglia and thalamus
middle = lobes
least common = pons (highest mortality)
3 consequences of intracerebral haemorrhage
1. haematoma expansion
2. cell death due to pressure or chemical toxicity
3. peri-haematomal oedema which increases intracranial pressure and herniation
incidence, mortality rate, and MOI of subarachnoid haemorrhage
- 5% of strokes
- incredibly high mortality
- MOI = rupture of intracranial aneurysm in 85% of cases
timeline of subarachnoid haemorrhage (3 stages)
1. early brain injury - ischaemia and toxic effects of blood in subarachnoid space
2. delayed cerebral ischemia in 1/3 of patients
3. systemic response - increases SNS activity, angiotensin system activation, inflammatory cytokines activated
symptoms of subarachnoid haemorrhage
- sudden onset of most severe headache ever, peaks within 1 minute
- neck pain/stiffness combined with headache
- CT +/- lumbar punture to diagnose
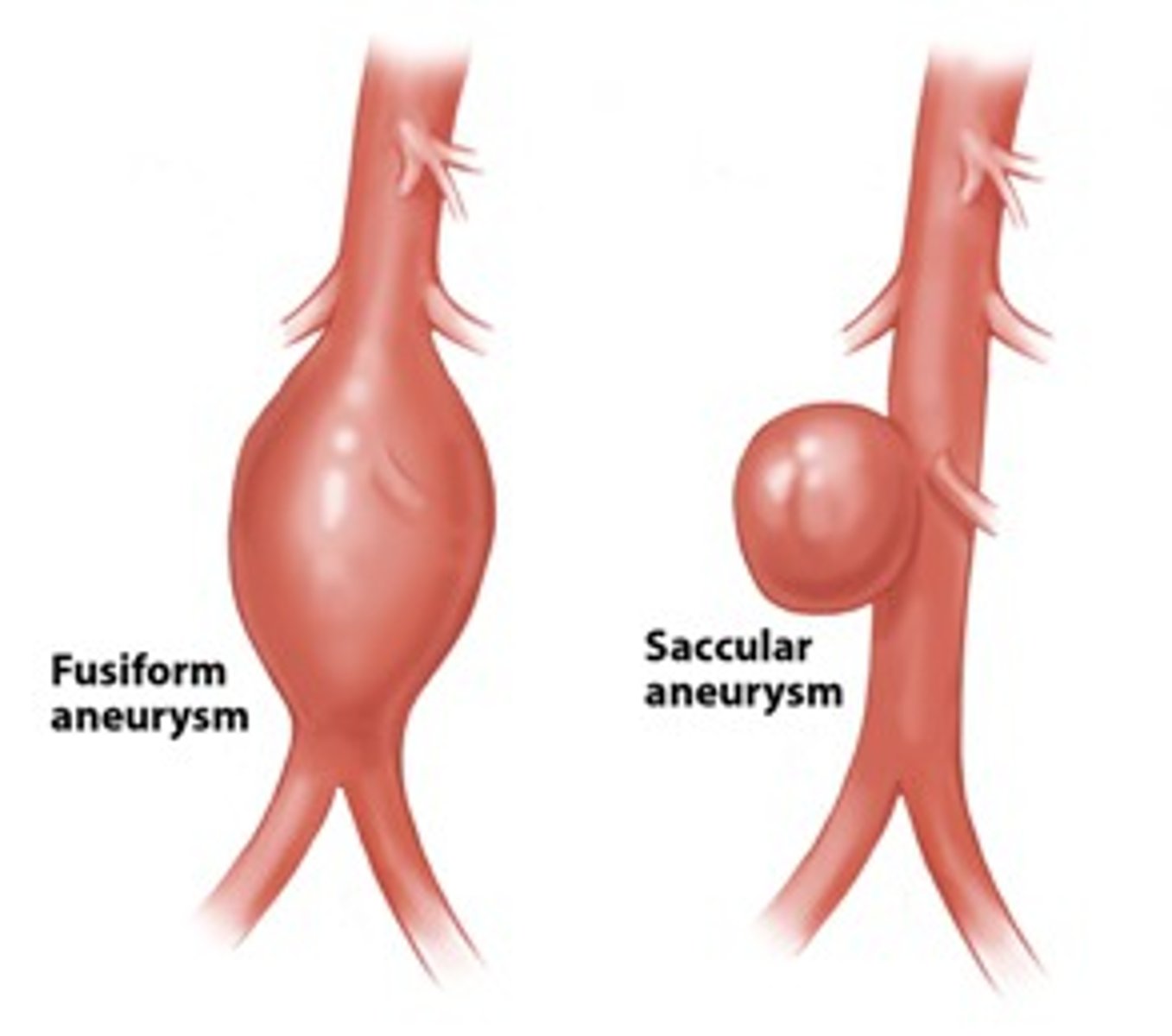
what is a saccular/berry aneurysm
when arteries branch, blood hitting fork point causes it to balloon out and distend with blood. Common in circle of Willis. Causes gradual degeneration of internal elastic lamina and tunica media which eventually ruptures. Can grow to 6-7mm
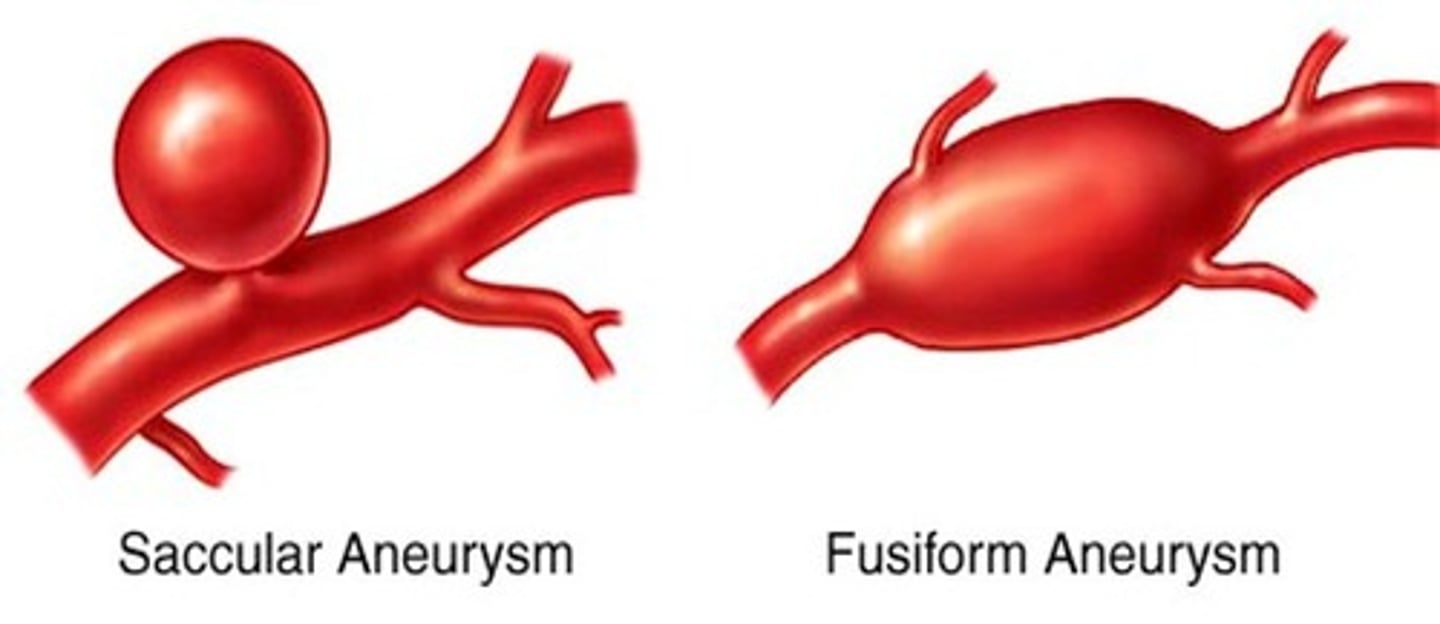
what is a fusiform aneurysm
all sides of blood vessel balloon out uniformly
what is an arteriovenous malformation
- generally congenital
- tangled mass of thin dilated blood vessels creating abnormal channels between arteries and veins that rupture
- blood bypasses the typical capillary network which means poor nutrient and gas exchange and less regulation of BP
incidence and mortality of ischaemic stroke vs intracranial haemorrhage vs subarachnoid haemorrhage
incidence: ischaemic > ICH > SAH
mortality: SAH > ICH > Ischaemic
stroke risk factors modifiable and non-modifiable
non-modifiable = older age (weakened vessels), female, family history, previous incidence
modifiable = smoking, alcohol, high BP
what are the FAST signs of stroke
F - facial drooping (generally one side)
A - arm can't be raised
S - slurred speech
T - time is critical
how can BBB breakdown cause secondary injuries
can allow infiltration of immune cells (different to brain's immune cells) that secrete IL-6 and TNF-∂ which activate Caspase which triggers apoptosis of neurons
what is necrosis and apoptosis, how do they differ
- have different MOI - necrosis generally primary injury while apoptosis is secondary injury in response to dysfunctional cells
- necrosis = cell swells and bursts, releasing cellular contents WITHOUT membrane to bind them up
- apoptosis = cell breaks up and shrinks rather than ruptures, apoptotic bodies are membrane bound and eaten by phagocytes
6 axonal impairments of diffuse axonal injury
rapid tensile stretch of axons causes:
1. myelin degeneration
2. impaired axonal transport
3. axonal swelling and accumulation of protein
4. damaged axonal cytoskeleton
5. influx of Ca2+ and Na+
6. secondary axotomy (axotomy of non-severed axons due to secondary injuries)
which all lead to cell death
consequence of excitotoxicity
influx of excitatory NTs like glutamate causes influx of Ca2+ and Na+ which eventually causes apoptosis
what is neuroinflammation
infiltration of immune cells passing through broken BBB which secrete their immune factors which cause inflammation and damage to CNS
what are consequences of reactive oxygen species (free radicals) in brain e.g. H2O2, O2-, OH
1. activates Caspase within cells which is a major trigger for apoptosis
2. cause DNA damage to cells - can cause fragmentation, micro deletions, damage telomeres etc
5 categories of treatment for acquired brain injuries
1. prevention
2. prediction
3. manage secondary injury
4. repair consequences of injury
5. treat ongoing symptoms
describe 2 prevention measures of acquired brain injuries
1. avoid the trauma which is generally a MVA - don't drink and drive
2. exercise and diet to lower smoking, hypertension, cholesterol, BP
describe a prediction strategy for acquired brain injury
develop biomarkers/diagnostic tools to predict outcome/personalise treatment e.g. concussion protocols for sports trainers
3 types of drugs to manage secondary brain injuries
1. anti-oxidants - oppose action of reactive oxygen species
2. calcium channel blocker - reduce excitotoxicity
3. competitive inhibitor - binding to excitatory amino acid receptors instead of excitatory NTs like glutamate
what are the 4 ways to repair consequences of an acquired brain injury
1. stem cell therapy (pluripotent -> neuron)
2. regrow damaged axonal connections
3. encourage brain plasticity
4. surgical intervention of haematoma
describe stem cell therapy for treatment of acquired brain injury
- pluripotent stem cell planted in brain to replace dysfunctioning neurons
- can use embryonic cells, adult donor cells, other tissue stem cells
- risk of cancer
how can you encourage brain plasticity
- cognitive exercises
- exercise, diet, and sleep are great for neuroplasticity
- aim is to recruit healthy neurons to take over job of lost neurons
- exercise can prompt endogenous stem cells to build neural cells
4 ways to treat ongoing symptoms of acquired brain injuries
1. rehabilitation and retraining for motor deficits
2. pharmaceutical or therapy for cognitive deficits
3. rearrange life + plan routines so they can cope with lost planning skills, attention, memory etc
4. callosotomy - stop seizures spreading across hemisphere but changes lateralisation of function