MSK Lab Material
1/46
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
47 Terms
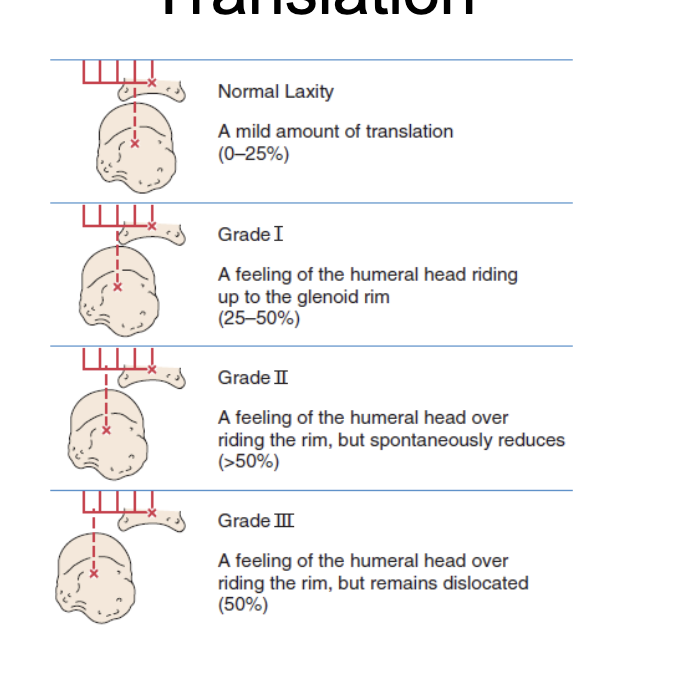
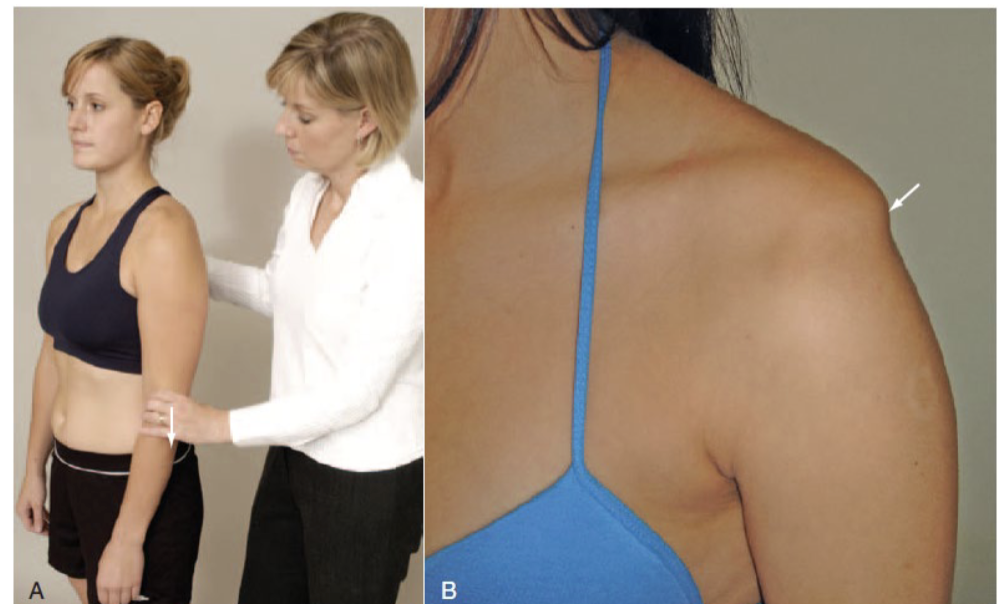
What is the Load and shift test for?
Anterior and Posterior Instability
What is the Relocation test for?
Anterior Instability
What is the aprehension Test for?
Anterior instability
Positive Aprehension Test
A positive test is indicated when the patient looks or feels apprehensive or alarmed and resists further motion.
What is the Jerk Test for?
Posterior Instability
Positive Jerk Test
-A positive test for recurrent posterior instability is the sudden jerk or clunk as the humeral head slides off (subluxes) the back of the glenoid (Fig. 5.76).
-When the arm is returned to the original 90° of abduction, a second jerk may be felt as the head reduces.
-the positive signs also indicate a positive test for a posteroinferior labral tear.
What is the sulcus sign for?
Inferior/ Multidirectional Stability
What is the Hawkins Kennedy Test for?
Impingement Test
Positive Hawkins Keneddy Test
Pain indicates a positive test for supraspinatus paratenonitis/tendinosis or secondary impingement.
How to perform Hawkins Keneddy Test
→ The patient stands while the examiner forward flexes the arm to 90°
→ then forcibly rotates the shoulder medially
What is Coracoid Impingement Sign
An Impingement test
is the same as the Hawkins-Kennedy test but involves:
→ horizontally adducting the arm across the body 10° to 20°
What is Yokum Test For?
Impingement Test
is a modification of Coracoid Impingement test in which the patient’s hand is placed on his or her opposite shoulder and the examiner elevates the elbow.Pain indicates a positive test
What is Neer Test for?
Impingement Test
Positive Neer test
a positive test result: The patient’s face shows pain
The test indicates an overuse injury to the supraspinatus and sometimes to the biceps tendon.
How to Perform Neer Test?
The patient’s arm is passively and forcibly fully elevated in the scapular plane with the arm medially rotated by the examiner.
What is the Internal (Medial) Rotation Resistance Strength Test (IRRST) (Zaslav Test) for?
This test is a follow-up to a Neer test.
→ The patient stands with the arm abducted to 90° and laterally rotated 80° to 85°.
→ The examiner then applies an isometric resistance into lateral rotation
→ followed by isometric resistance into medial rotation (Fig. 5.94).
Positive Zaslav Test?
The test is positive in a patient w/ positive impingement test:
- if the patient has good strength in ER but not IR;
- it indicates an internal impingement.
This test may be used to differentiate between:
if IR stronger than ER it is outlet (subacromial space)
If ER are stronger it is non outlet (Occurs inside the glenohumeral joint)
What is Posterior Internal Impingement Test for?
Internal (Non-Outlet) Impingement — Short Version
Most common in overhead athletes (especially throwers).
Occurs when the arm is abducted, extended, and externally rotated (late cocking position).
The undersurface of the rotator cuff gets pinched between the greater tuberosity and the posterosuperior glenoid/labrum.
Often associated with anterior instability or pseudolaxity.
Can lead to a posterior labral ("kissing") lesion.
Patients typically report posterior shoulder pain during the late cocking and early acceleration phases of throwing.
Positive Posterior Internal Impingement Test
The test is considered positive if it elicits localized pain in the posterior shoulder.
EMPTY CAN/ Lateral Jobe test: Describe test and what would be a positive sign
(supraspinatus test)
→ The patient is in standing with the arm abducted to 90° on the scapular plane and thumbs facing down
→ examiner then applies an inferior (i.e., downward) force to the arm at the elbow.
Interpretation:
A positive test is indicated by pain, weakness, or inability to hold position. It indicates rotator cuff pathology
Describe Lift-Off Sign (Gerber’s Test) and what a Positive test means
→ The patient stands and places the dorsum of the hand on his or her back pocket or against the midlumbar spine. The patient then lifts the hand away from the back.
Interpretation:
-An inability to lift dorsum of the hand indicates a lesion of the subscapularis muscle. Abnormal motion in the scapula during the test may indicate scapular instability
→ If the patient is able to take the hand away from the back the examiner applies a load pushing the hand toward the back to test strength of the subscapularis + to test how the scapula acts under dynamic loading
Interpretation:
With a torn subscapularis tendon, passive (and active) ER increase
Describe Abdominal Compression Test (Belly-Press or Napoleon Test) and what a Positive test means
This test checks the subscapularis muscle, especially if the patient cannot ER the shoulder enough to take it behind the back.
→The patient is in a standing position. The examiner places a hand on the abdomen below the xiphoid process The patient places the hand of the shoulder being tested on the examiner’s hand and pushes the hand as hard as they can into the stomach IRl shoulder rotation). While pushing the hand into the abdomen, the patient attempts to bring the elbow forward to the scapular plane, causing greater medial shoulder rotation.
Interpretation:
the test is positive for a tear of the subscapularis muscle:
- If the patient is unable to maintain the pressure on the examiner’s hand while moving the elbow forward, or posteriorly flexes the wrist or extends the shoulder
Describe Drop-Arm (Codman’s) Test and what a positive test means
→ The examiner abducts the patient’s shoulder to 90°
→ then asks the patient to slowly lower the arm to the side in the same arc of movement
Interpretation:
A positive test is if the patient is unable to return the arm to the side slowly or has severe pain when attempting
A positive result indicates a tear in the rotator cuff complex.
What are some Compression SLAP tests
-Obrien
-Compression rotation
-clunk’
-Anterior slide
-Kim test I (biceps load test)
What are some Traction injury SLAP tests
-Speeds
-Dynamic Speed’s
-O’brien
What are some overhead injury SLAP tests?
-Pronated load (Biceps load) test
-Resisted supination ER
-Kim Test II (Biceps load)
-Pain provocation
- Labral Crank test
What are some Labrum SLAP tests?
-Obrien
-Compression rotation
-clunk test
-Anterior slide
--Kim test I (biceps load test) (pt. is passive)
-Pronated load (Biceps load) test/ Kim test II (Biceps load test) (pt. resists you)
-Resisted supination ER
- -Pain provocation
- Labral Crank test
What are some bicepts tests?
Speed’s Test
Biceps Stretch Test
Describe O’Brien Test and what a positive test would be
This test is designed to detect SLAP (type II) or superior labral lesions.
→ The patient is standing position with arm forward flexed to 90° + the elbow fully extended.
→ The arm is then horizontally adducted 10° to 15° (starting position) + IR(so the thumb faces downward).
→ examiner stands behind patient and applies a downward eccentric force to the arm
→ The arm is returned to the starting position and the palm is supinated so that the shoulder is rotated laterally; then the downward eccentric load is repeated.
interpretation:
the test is considered positive for labral abnormalities
-If pain on the joint line or deep painful clicking is produced inside the shoulder in IR
AND
- eliminated or decreased when tested supinated
Describe Compression Rotation Test and what a positive test would mean
→ The patient is supine with the examiner standing beside the test shoulder.
→ examiner passively abducts the shoulder to between 20° and 90°, the patient’s elbow at 90°.
→The examiner applies an axial compression force through the long axis of the humerus
(pushing up through the elbow)
→ while passively rotating the humerus back and forth (small and large circles) to try to trap the labrum within the joint (Fig. 5.110).
interpretation:
If pain, clicking, or a catching sensation is elicited, the test is considered positive for a torn labrum.
Describe Clunk Test and what a positive test would mean
→ The patient lies supine. Examiner places one hand on the posterior aspect of the shoulder over the humeral head.
→ The examiner’s other hand holds the humerus above the elbow.
→ examiner fully ABducts the arm over the patient’s head.
→ examiner then pushes anteriorly with the hand over the humeral head (a fist may be used to apply more anterior pressure)
→ while the other hand rotates the humerus into lateral rotation
Interpretation:
A clunk or grinding sound indicates both a positive test and a tear of the labrum.
--The test may also cause apprehension if anterior instability is present
Kim Test (Bicep Load Test) - a positive test would mean
Interpretation:
A sudden onset of posterior shoulder pain and click indicates a positive test for a posteroinferior labral lesion.
Describe Anterior Slide Testand what a positive test would mean
→ The patient is sitting with the hands on the waist, thumbs posterior.
→ The examiner stands behind the patient and stabilizes the scapula + clavicle with one hand.
→ With the other hand, the examiner applies an anterosuperior force at the elbow
Interpretation:
If the labrum is torn (SLAP lesion):
- the humeral head slides over the labrum with a pop or crack with pain on the joint line, and the patient complains of anterosuperior pain.
Biceps Load Test (Kim Test II) / Pronated load (Biceps load) test
This test is designed to check the integrity of the superior labrum.
→The patient is in the supine / seated position with the shoulder ABducted to 120° + laterally rotated, -elbow flexed to 90°, the forearm supinated (as it is for the apprehension or crank test.)
→ The examiner performs an apprehension test on the patient by taking the arm into full ER.
→ If apprehension appears, the examiner stops ER and holds the position.
→ The patient is then asked to flex the elbow against the examiner’s resistance.
Interpretation:
If the apprehension remains the same or the shoulder becomes more painful, the test is positive for a SLAP lesion in the presence of recurrent dislocations (Fig. 5.107).
If apprehension decreases or the patient feels more comfortable, the test is negative for a SLAP lesion.
recommended to do the test with the forearm pronated (pronated biceps load test ).If the pain is located deep in the superior glenohumeral joint, the test is considered positive.*
Resisted Supination External Rotation Test (RSERT).
This test is to check for SLAP lesions and is thought to re-create the peel-back mechanism of the superior labrum.
→While in supine, the patient’s arm is placed with the shoulder abducted to 90°, elbow flexed to 65°- 70° the forearm is neutral / slight pronation.
→ The patient is then asked to maximally supinate the hand while the examiner resists.
→While the patient continues to supinate against the examiner’s resistance, the examiner rotates the shoulder laterally to end range
interpretation:
-The test is positive if the patient has anterior or deep shoulder pain, there is clicking or catching in the shoulder, or the symptoms are reproduced.
-The test is considered negative if there is posterior shoulder pain, no pain, or apprehension
Pain Provocation (Mimori) Test
→ the patient is seated and the arm abducted to between 90° - 100°,
→ the examiner laterally rotates the arm by holding the wrist (Fig.
→ The forearm is taken into maximum supination and then maximum pronation.
Interpretation:
the test is considered positive for a superior (SLAP) tear:
If pain is provoked only in the pronated position
or
if the pain is more severe in the pronated position
As with other superior labral tests, the biceps must be tested (Speed test) to rule out biceps pathology causing the pain.
Labral Crank Test
The patient is in the supine lying or sitting position.
→ The examiner elevates the arm to 160° in the scapular plane.
→ the examiner applies an axial load to the humerus with one hand
→ while the other hand rotates the humerus medially and laterally.
interpretation:
A positive test is indicated by pain on rotation, especially lateral rotation, with or without a click or reproduction of the patient’s symptoms
Speed’s Test (Biceps or Straight-Arm Test)
-The examiner resists shoulder forward flexion by the patient
- while the patient’s forearm is first supinated, then pronated, and the elbow is completely extended.
→ The test can also be performed by forward flexing the patient’s arm to 90°
→ then asking the patient to resist an eccentric movement into extension first with the arm supinated, then pronated (Fig. 5.165).
Interpretation:
-A positive test elicits increased tenderness in the bicipital groove especially with the arm supinated and is indicative of bicipital paratenonitis or tendinosis.
-It has been reported that this test may cause pain; therefore it is positive if a SLAP (type II) lesion is present.
-If profound weakness is found on resisted supination, a severe second- or third-degree (rupture) strain of the distal biceps should be suspected
Biceps stretch test (Tightness test)
-The patient lies supine with the shoulder in extension over the edge of the examining table with the elbow flexed and the forearm supinated.
-The examiner then extends the elbow, which would normally have a bone-to-bone end feel if the biceps flexibility is normal.
- If the biceps is tight, full elbow extension does not occur, and the end feel is a muscular tissue stretch
Paxinos Sign
→The patient is seated with the test arm relaxed at the side.
→ The examiner stands beside the test arm and places one hand over the shoulder so that the thumb is under the posterolateral aspect of the acromion and the index and long fingers of the same hand (the fingers of the opposite hand may also be used instead) over the middle part of the clavicle on the same side (Fig. 5.135).
→The examiner then applies pressure to the acromion with the thumb anterosuperiorly
→ while applying an inferior directed counterforce to the clavicle with the fingers.
The test is considered positive if pain in the area of acromioclavicular joint is increased.
Acromioclavicular Shear Test.
→ With the patient in the sitting position
→ examiner cups hands over the deltoid muscle with one hand on the clavicle and one hand on the spine of the scapula.
→The examiner then squeezes the heels of the hands together
Abnormal movement and pain at the acromioclavicular joint indicate a positive test as well as acromioclavicular joint pathology.
Acromioclavicular Crossover, Cross-Body, or Horizontal Adduction Test (BCE)
→ The patient stands and reaches the hand across to the opposite shoulder. (The examiner may also passively perform the test)
→ With the patient in a sitting position, the examiner passively forward flexes the arm to 90° and then horizontally adducts the arm as far as possible
If the patient feels localized pain over the acromioclavicular joint, the test is positive.
Localized pain in the sternoclavicular joint indicates that joint is at fault.
What do you check for during Cervical Screening?
Neck
Flexion
L/R sidebending
L/R Rotation
Extension
STJ instability is often an underlying cause of
Subacromical mpingement
STJ Stability Tests
Resting Postion
Bilateral Flexion to 90 deg
Scolding Position
Active elevation - Flexion
Active Elevation - Abduction
Grades of GFJ translation