PathoPharm: ADME & Motions
1/112
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
113 Terms
What are the 3 types of Pharmacotherapeutics?
Drugs/Medications
Biologics
Natural Health Products
What is the difference between a Drug/Medication and a Biologic?
Drugs are a chemical agent that is synthetically produced while biologics are straight from living organisms. So Biologic medications are produced from living organisms
What are examples of biologic medications?
Components of living organisms: —>
Proteins
cells
antibodies (IgG’s)
blood products
hormones etc.
What are natural health products (NHP)?
they’re sourced/derived from nature/plants. So they’re the natural remedies
What do natural health products include?
vitamins
minerals
dietary supplements (calcium, iron, biotin)
Dried herbs
protein powder
What are therapeutics?
they’re interventions done/carried out by health care professionals to benefit the patient’s well being. This can be done by reducing symptoms or eliminating a disease
Sometimes NHP’s can cause chronic side effects and interfere with other medications if taken long term and obsessively, true or false?
True
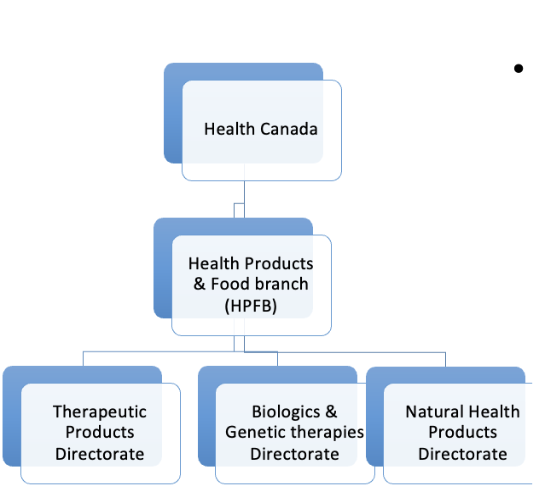
Who is responsible for monitoring and evaluating the safety, efficacy and quality of drugs/pharmacotherapeutics?
Health Canada
What are the branches of Health Canada?
Therapeutics Products directorate
Biologics & Genetic therapies directorate
NHP directorate
What is the most common way biologics are usually given and why?
Biologics are usually given IV and never Orally because if a biologic is given orally it’s usually destroyed in the GI tract before it ever gets distributed
What is the approval process for new drugs (quick summary)
Research
Preclinical Trials/ Lab trials: on animals (not humans) —> medication has to be proven safe and then turned into a form that is safe for humans
Clinical Trails on Humans (3): #1 —> on health small population, #2 —> on bigger population of ppl. with disease, #3 —> up to 3000 people
New Drug Submission: —> Drug receives an NOC (notice of compliance) & DIN (drug identification #)
Drug is continuously monitored after
What are the 3 types of drug (category of therapeutic) names?
1 Generic
Brand
Chemical
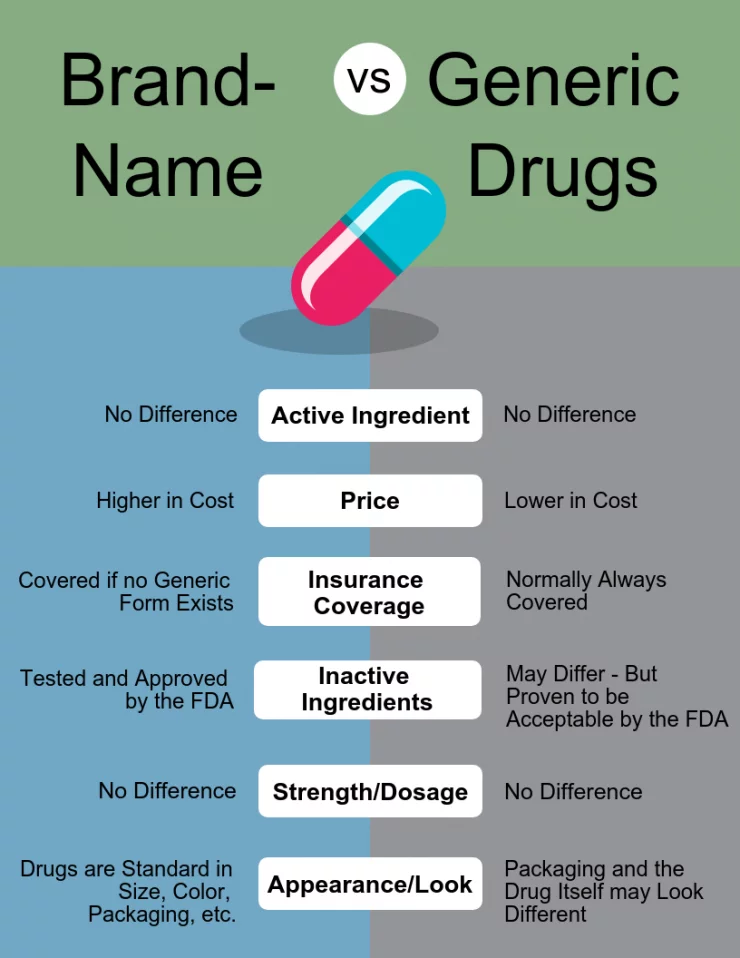
What is the key differences between Brand and Generic names?
Brand drugs are usually first to the market and protected by a patent for 20 years. Its created by a drug company
It’s more expensive
Many trade names after patent expires
Generic drug names are without proprietary affiliation so they’re cheaper
They’re the assigned name internationally, especially with the main ingredient
1 generic name per drug
Way cheaper
How is the chemical name for drugs given?
Through the chemical composition of the drug name
it’s assigned by the IUPAC (international union of pure and applied chemistry)
How are drugs sorted into classes?
Based on their characteristics;
drugs that have the same method of action or have the same effect on a symptom are sorted into the same class
What is the generic name for advil vs. the brand names
Generic name: ibuprofen
Brand names:
advil
motrin
nurofen
easofen

What are the different drug schedules and what is the difference between them?
The drug schedule depends on what practitioner is giving the drugs/where a rx is required
Schedule I: available only by rx from a pharmacist, NP or doctor
all rx drugs
Schedule II: available from a pharmacist by rx (in an area with no public access; no open shelves) —> you need pharmacist consultation —> pharmacist has to go to the back and get it
Schedule III: Available via pharmacy or pharmacy area where they’re available. If pharmacy is closed, you can’t get it.
You can grab it from the shelves inside the pharmacy area.
Unscheduled: can be sold in any store without medical supervision —> tylenol and advil
What types of drugs are in schedule I and why
Controlled drugs and drugs with the potential for abuse such as narcotics are in schedule I
Ex:
Ecstacy
Cocaine
Morphine
Fentanyl
What schedule does Cannabis fall into?
Schedule I if it’s prescribed by a doctor
Schedule III if it’s recreation party use because you still need professional supervision to get it (over 18+)
What is the difference between therapeutic and pharmacological drugs?
Therapeutic drugs treat a specific problem or disorder or symptom(why drug is being used)
Pharmacological drugs are what the drugs do at the cellular level (receptors and molecules)
Ex:
Therapeutic class: symptoms relieving
antihypertensive
antipyretic
anti-inflammatory
Pharmacological (MOA):
calcium channel blockers
serotonin reuptake inhibitors
What is the difference between pharmacokinetics and pharmcodynamics?
Pharmacokinetics: movement of drug throughout the body
ADME
Pharmacodynamics: what the drug does to the body at a cellular level (receptors and such)
Effects at receptor level —> does BP increase, stop clotting, sedative?
What is the nursing process and at what stage do we give patient education about the drugs and process?
A: assessment —> health hx
D: diagnosis
P: planning
I: Intervention —> pharmacotherapeutics and patient education
E: evaluation (assessment of drug action and drug effects + side effects)
**Patient education is implemented during intervention before the drug is given
What factors do we depend on to decide what formulation/route to give?
The clinical setting
the medical situation
How dire they need the medications (immediate vs. over time)
Duration
Metabolism
Consciousness
Drug properties
Drug Kinetics: how the drug is meant to move throughout the body and what environment it was designed for (ex: steroids for swollen knee joint should be localized and not circulate through entire body)
What is hydromorphone (dilaudid)?
It’s an opioid that is really strong
What is an enteric-coated drug and why can’t it be crushed?
An enteric-coated pill is a pill with a coating that is meant to withstand the acidic environment of the stomach and make it to the small intestine and be absorbed there. If you crush it, it becomes useless and dissolves in the stomach
What are the characteristics of PO medications?
It means taken orally and is always systemic
it goes through the hepatic portal vein and goes through first pass metabolism
can be liquid, pills or powder
We can give medications through a tube like NJ tube if the formulation is correct
The drugs won’t process and be distributed if there’s no peristalsis
There’s no way an orally administered drug can be local, true or false?
true
How does sublingual administration work?
It’s a dissolvable pill given under the tongue
—> the tongue has a high vascularity due to capillaries
The contents of the drug dissolves into the capillaries and into systemic circulation
takes 30 secs to 2 mins
Ex: Angina patients —> nitroglycerine sublingual tablets dilate arteries
Sublingual Administration Kinetics:
Contents of the drug is absorbed into the capillaries and straight into the bloodstream
bypassing the GI system and 1st pass metabolism of liver
why are sublingual tablets not recommended for long-term use or every few hours?
Because SL tablets can irritate the submucosal lining of the tongue
What is an another administration similar to SL (sublingual)?
Buccal medications —> has to dissolve quicker and easier because mucosa in the cheeks and muscles of cheeks are thicker
What is the kinetics of intranasal/insufflation?
Into nasal cavity where contents can either be local or absorbed into the olfactory bulb to systemic circulation and CNS
How does intranasal/insufflation drugs cross the BBB and access CNS?
By being lipophilic
The contents of the drug (if lipophilic) cross the olfactory region through the olfactory bulb and can access the CNS by travelling along the olfactory nerve (CN I)
Intranasal drugs if lipophilic do cross the BBB, true or false?
True
What is an example of a local intranasal spray?
Rhinocort spray
for post-nasal dread
allergy symptoms
localized effect on nasal mucosa
Whats an example of a systemic nasal spray?
Cocaine or the flu vaccine
Absorbed into the capillaries quickly
How is inhalation different than insuffulation/intranasal
inhalation is into the lungs; can be systemic through lung’s capillaries or stay local
Insufflation/intranasal is into the nose
How does kinetics of inhalation drugs work?
Affects the pulmonary capillary network acting quickly and having rapid effects
The lungs are highly vascular so local effect can happen inside the lungs itself
Or systemic effect can happen through the vascular capillaries of the lungs and through to the whole body
What is an example of local inhalation drugs vs. systemic?
local: asthma drugs/inhaler (Albuterol or Salbutamol/Atrovent)
systemic: general anesthesia
systemic drugs work by crossing the BBB because they’re lipophilic and reaching the brain causing the brain to sleep
How do endotracheal (ET) drugs work?
Usually used in ER/ICU emergency situations and it’s administered straight into the lungs.
The ET tube is inserted through the oral cavity or nose and goes into the trachea so we have access to the lungs
How does first pass-metabolism work?
The drug is first going through the GI tract aka. small intestine, into the hepatic portal vein, through the liver (where it’s metabolized for the 1st time) and then goes into circulation via. the heart
First-pass metabolism = drug is partly destroyed in the liver before reaching the bloodstream, lowering its bioavailability.
When is endotracheal (ET) tubes commonly used?
For emergency situations when pushing in NE (epinephrine) to the lungs
usually during anaphylactic shock
How are asthma medications given, aka what device is used for intranasal?
Nebulizer
How many daltons does a molecule have to be to pass through the epidermis into the dermis and reach circulation through capillary network?
Molecule size is measured in “daltons”
Daltons = molecular weight
Has to be less than 500 daltons to be absorbed into the dermis
**Anything above 500 daltons stays on the epidermis staying local
Why are a lot of lotions local and not systemic?
Because their molecules are larger than 500 daltons and stays on epidermis.
Ex: Retinoid creams —> used for preventing wrinkles and supports collagen and recycles the skin
How do transdermal patches function?
They use the dermal capillary system for systemic effect and transdermal patches are majorly meant for systemic response
The molecules are prepped to trickled down the epidermis into dermis and reach capillary absorption
What are transdermal patches commonly used for?
long-lasting, slow and steady release
***Steady release and absorption is the intent and goal of transdermal medications
Nitroglycerine patch, nicotine patch, morphine patch and hormone treatment
When are rectal medications usually administered/that route is used?
for babies and when someone is unconscious
depends on whether we want systemic or local
If someone is constipated, we might give rectal drug
Is rectal drugs systemic or local?
50-75% bypasses the first pass metabolism of liver and goes straight to systemic circulation
What do we have to remember about implanted ports?
Injecting medications into it, we have to know how to properly handle and care for the implanted port so it doesnt get infected
What are the 3 common IM injection spots?
deltoid
vastus lateralis + rectus femoris (thigh)
ventral gluteal
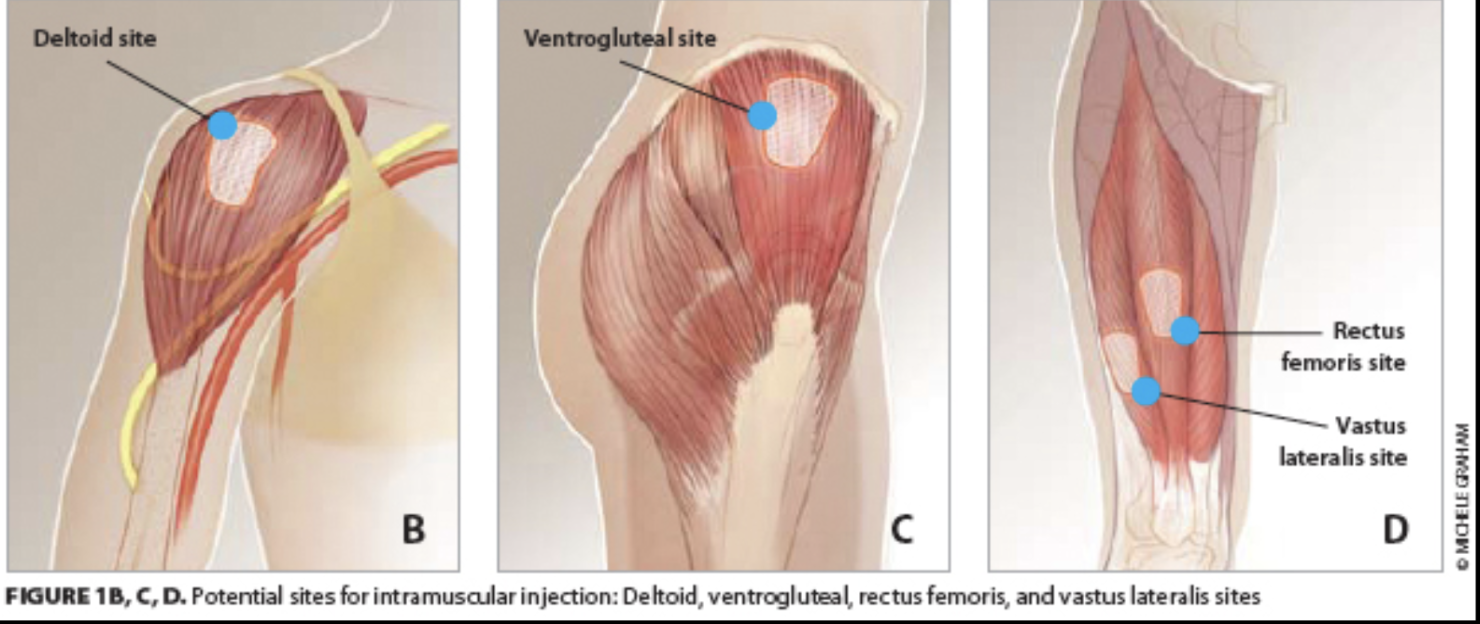
what spot do we never IM inject and why?
dorso-gluteal due to the sciatic nerve cause there’s been too many injuries to that nerve
Where is SC (subcutaneous) injections injected into?
Adipose tissue (fat) of the hypodermis
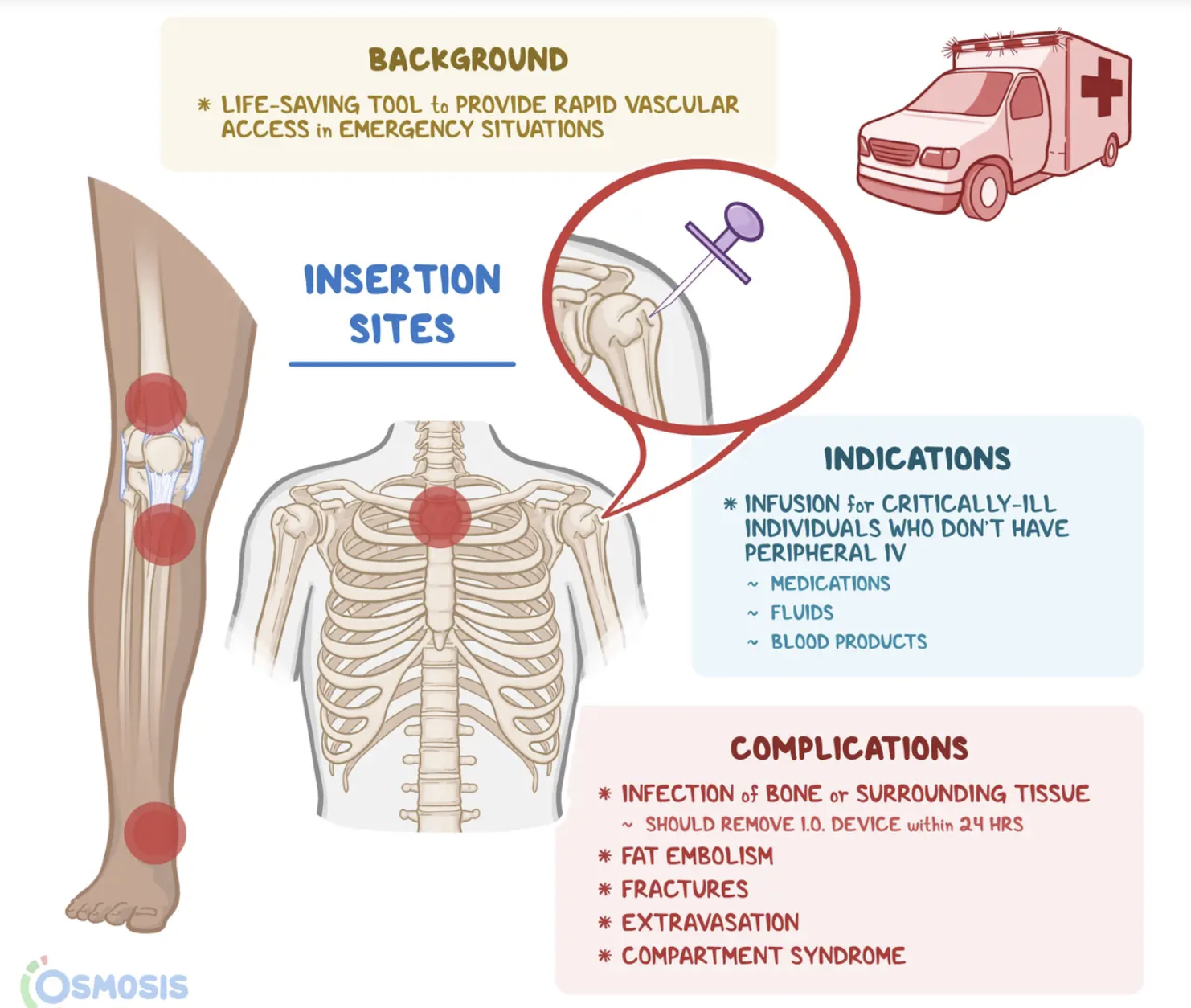
What are the 3 sites of intraosseous injections?
proximal end of tibia (under knee)
medial distal end of tibia
Distal femur (above knee)
What are the 10 rights of drug administration?
right drug
right dose
right route
right time (delivery and frequency)
right patient
Documentation
History & assessment
informed consent
interactions evaluation
educations & information
What is pharmacokinetics? (PK)
the motion of a drug throughout the body
—> it’s movingg
ADME
What is pharmacodynamics? (PD)
the receptor binding and affinity of the drug
(is the receptor saturated, is there a competing drug?)
either increases or suppresses existing processes
What is an antagonist drug and what does it do? (PD)
Only blocks the receptor; elicits no reaction on it’s own. Just stops whatever
what does ADME stand for?
A: absorption —> how it gets in
D: Distribution —> to tissues
M: metabolism —> broken down by liver
E: excretion —> by the kidneys
What molecular characteristics makes a drug more likely to be absorbed vs. excreted
Absorbed —> non-ionized, lipophilic, small
Excretion —> ionized, small, hydrophilic (travels with water)
What is passive vs. active transport and give examples
Passive —> diffusion (particles), osmosis (water), facilitated diffusion (passive channels like aquaporins)
Active transport —> uses ATP to get particles from low to high
goes against the transportation gradient
What are the characteristics of ADME?
A: drug into circulation (bioavailability) —> route
D distributing drug to target tissues from circulation —> dependant on blood flow, tissue size, plasma protein mound
M: metabolized by liver —> activates prodrugs
E: excretion aka. 1st order vs. Zero order kinetics
What top 4 organs does the most amount of blood flow to?
Liver: 25% (1/4)
Brain: 18%
Kidneys and muscles: 20%
What is biotransformation?
Biotransformation = the enzymatic conversion of drugs into metabolites, usually to detoxify and prepare them for excretion.
What is the formula for cardiac output?
Stroke volume (ml) x heart rate (min) = ml/min
How much blood is pumped out (cardiac output) per minute?
5-6L per mins
What is the big group of enzymes that break down/metabolize drugs in the liver?
CYP450 enzymes
What is therapeutic range?
Its the range in which we want to keep the plasma drug concentration so the patient feels the therapeutic effects at all times.
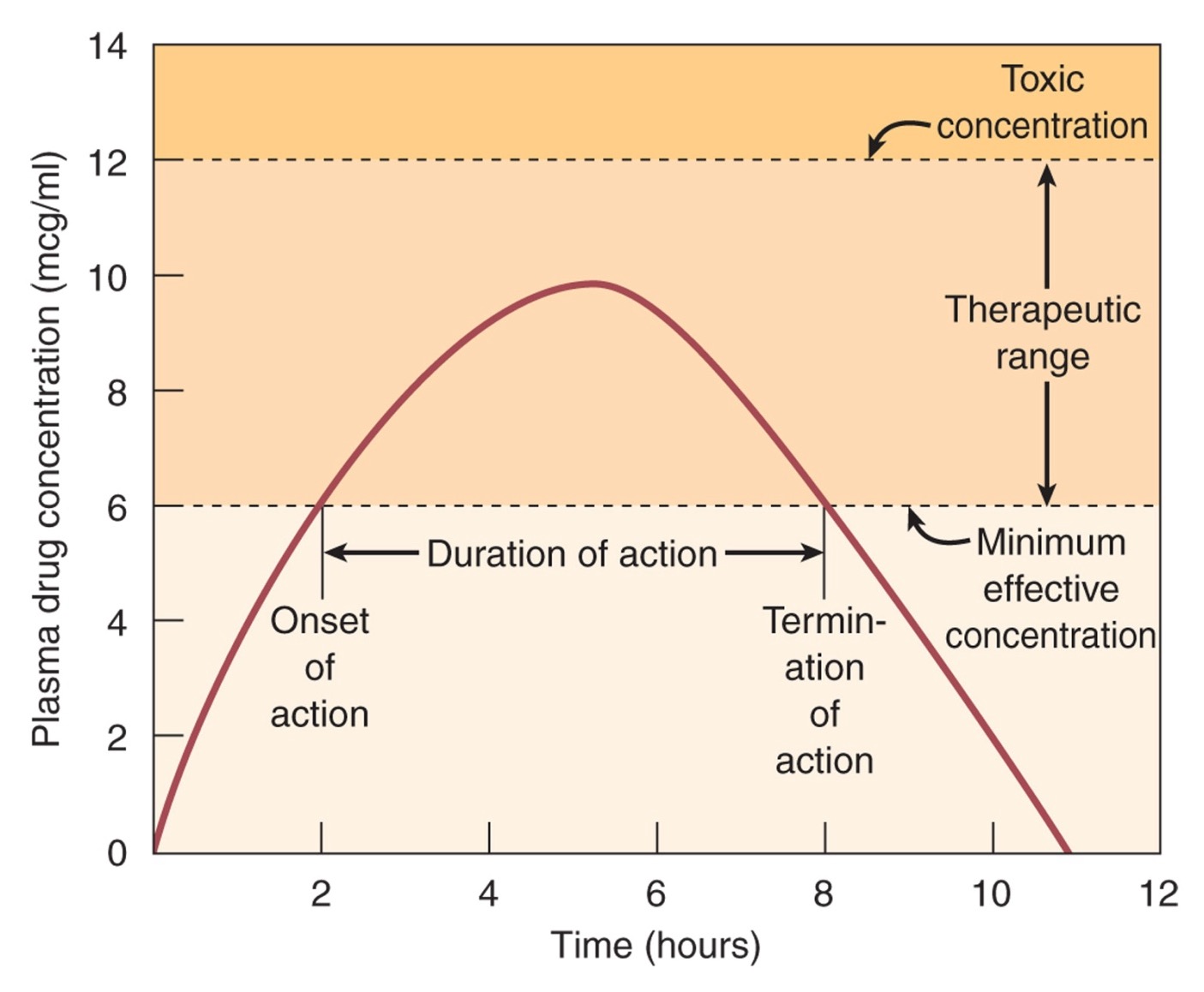
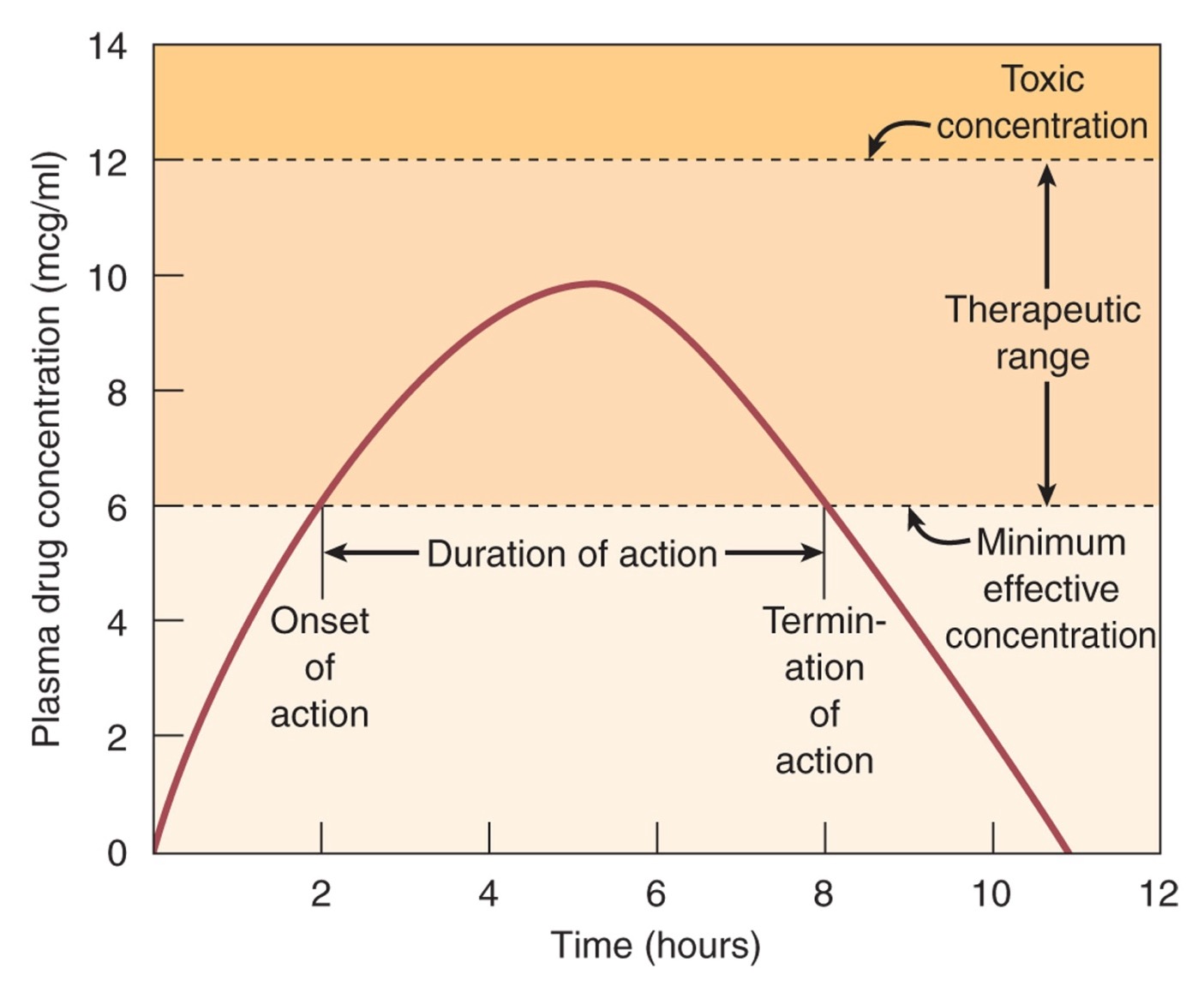
How do we determine the duration of action of the drug from the graph?
Termination of action - onset of action
so from the time it reach therapeutic range to the time it started to fall off therapeutic range
What is onset of action?
How long after administration a drug starts working
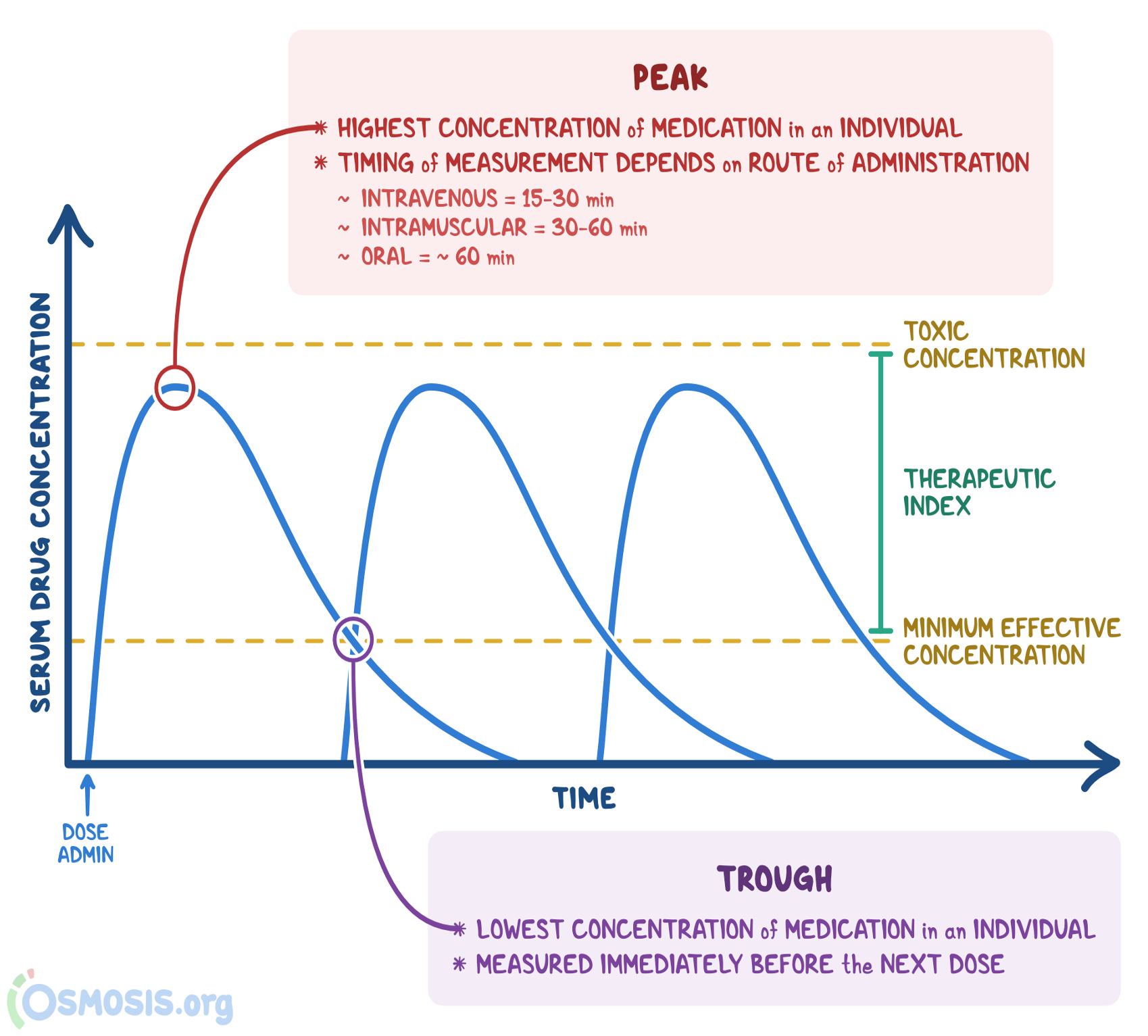
What is peak plasma concentration (C-max)?
The highest level of bioavailability by the drug and the time to it took for peak drug effect to take place
What is the trough on the graph?
The lowest concentration of a medication in an individual, it’s measured immediately before the next dose
Ex: think of it like the trenches (trough) —> the medication and it’s effects are in the trenches so it’s time to give the next one
What does the onset of action depend on?
The route of administration and the dosage
What does distribution of the drug to the tissues depend on?
A person’s cardiac output —> so how well their perfusion is
If their blood flow is really bad, especially to the extremities, then we would have to increase their fluids/volume
How do you calculate cardiac output?
stroke volume (ml) x heart rate (min) = CO ml/min
usually the range for both is 60-100 ml/min
so about 5-6L of blood volume on average
What is TI and what does it signify?
Therapeutic Index
the therapeutic index determines how safe a drug is to administer frequently; so how easy/hard it is to overdose
A small TI (ex: 2) = means the drug is easily overdosed and would not be given frequently; it would also have to be monitored
A large TI (ex: 18) = drug is safe to administer frequently and is hard to overdose
We never go over the recommended safe dosing/maximum amount we can give, true or false?
True
How do we calculate the therapeutic index (TI?)
ED50/TD50
ED50: the dosage that was required to produce a therapeutic effect in 50% of population
TD50: the dosage that gave 50% of the population a toxic response from the drug
This is derived from LD50 lab data
LD = lethal dose in lab trials
What are the narrow TI meds? aka. the drugs that are really easy to overdose
Digoxin (lanoxin)
Warfarin (Coumadin)
Phenytoin (Dilantin)
Tacrolimus (Prograf, Astagraf)
TI of 2 means you only need 2x the recommended dose to elicit a toxic response
A TI of 18 means you need 18x the recommended dose to elicit a toxic response
Yes
What’s the acornym for narrow TI?
DWPT; don’t worry pt.
D: Digoxin (lanoxin)
W: warfarin (coumadin)
P: Phenytoin (Dilantin)
T: Tacrolimus (Prograf, Astagraf)
How does the mechanism of distribution work?
Based on Plasma protein binding
Drugs bounds to plasma proteins won’t enter tissues and simply float around in the circulation
Drugs unbound are effective and go to the tissues
What type of protein does an acidic drug have an affinity for vs. a basic drug
acidic drugs have an affinity for Albumin (a=a)
basic drugs have an affinity for alpha-1-acid-glycoprotein (alpha’s are basic)
Why is PPB binding actually useful?
because it decreases the distribution rates (use to advantage in high PPB drugs)
so now the drugs are competitive for receptors, they’re reversible, and they’re saturable
What organ makes Albumin and alpha glycoprotein and other plasma proteins?
The liver —> makes enzymes and clotting factors and plasma proteins
So liver disease impacts the level of drug distribution
What causes overdose in highly PPB drugs?
If there’s another drug with same or stronger affinity for the plasma protein so then too much of the other drug is free and becomes a risk for OD
If a drug such as warfarin is 99% PPB and the PPB decreases by 1%, how much more warfarin is free?
double the amount of warfarin is going to tissues resulting in bleeding out and over reduced blood coagulation
Why/how do side effects occur when there’s too much of a drug?
Because all the receptors are saturated so the drugs are now bouncing around to other receptors and binding to them. Receptors such as one’s that cause nausea
What is biotransformation?
The same thing as metabolism
it’s a process using chemicals and enzymes to prepare the drug/substance for excretion
This happens in the liver
What are prodrugs?
Drugs that require metabolism to be activated (codeine —> morphine)
What is the biotransformation process of tylenol/acetaminophen?
Phase I: Tylenol is biotransformed/metabolized by p450 enzymes which creates the toxic metabolite NAPB (N-acteyl-P-benzo-quinoine)
NAPB is a toxic metabolite to the liver, it destroys it
Phase II: conjugation aka. ionization inactivates the metabolite through glutathione therefore making it ready for excretion
What does the liver do to make drugs easier to excrete?
Ionizes them aka. conjugation
What is given to pt’s who OD on Tylenol to induce metabolism?
NAC; a precursor for glutathione
The acetylcysteine of the NAC is converted into glutathione
What is an example of a drug that undergoes biotransformation but doesn’t change aka. travels unchanged?
Amoxicillin
What type of drug is Lovastatin?
Cholesterol reducing drug
CYP3A4 metabolized
What is the induction and inhibition of enzymes like for drugs? (ask chat gpt about this)
If a substance induces (speed up)the enzymes, the enzymes become more active and metabolize faster →
drug will be quickly metabolized; so not enough is remaining in circulation after biotransformation
If the drugs inhibit the enzymes, they metabolize slower; more of drug in circulation increasing distribution to tissues
What factors affect renal excretion?
The size, ionization (pH of environment) and hydrophilicty
Cardiac output; not enough volume of fluid = less to excrete
Renal Fx: renal fx in older adults and neonates is bad; also worse if they have renal (kidney) disease
Changing the environment of a drug makes it easier to excrete, true or false?
True, if a drug survives in a acidic environment and we make it basic, it’ll become ionized and be easier to excrete
To clear acidic drugs, we need a basic/alkaline environment to make it easier to excrete them
What is clearance?
The rate of elimination of drug in an hour
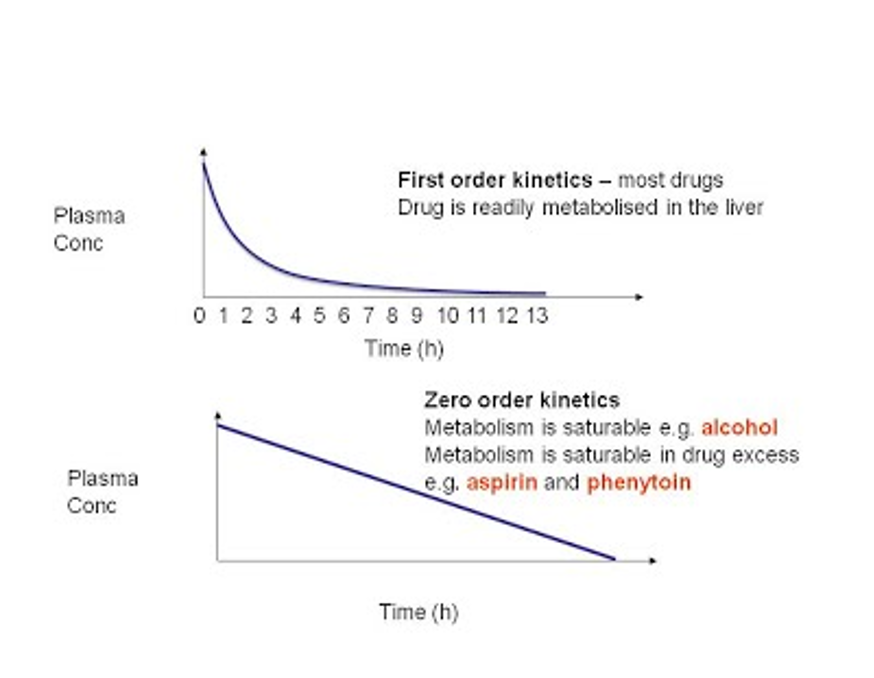
What’s the difference between 1st order and zero order kinetics for clearance (cl)
First order (drug-dose dependant): —> The elimination depends on the drug serum concentration
so it depends on what the drug dosage was aka. the more drug there is, the faster the body will work to clear it
Zero order: Doesn’t matter how much of a drug is in circulation, the body stays clearing/eliminating at the same pace as always
This makes a drug easy to overdose
ASA and Alcohol are zero order
More drug present = body won’t speed up and it gets easily overdose because it stays in the system