PANCE Blueprint GI and Nutrition - All system flashcard sets combined (Smarty PANCE)
1/573
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
574 Terms
What is cholecystitis?
Inflammation of the gallbladder usually associated with gallstones
What is cholangitis?
Cholangitis is an acute inflammation of the bile duct characterized by pain in the upper-right quadrant of the abdomen, fever, and jaundice. In most cases, cholangitis is caused by a bacterial infection
The formation of gallstones that afflicts mostly the western world
Cholelithiasis (gallstones)
A patient with painless jaundice, weight loss, and a palpable RUQ mass has what suspected diagnosis?
Gallbladder or Pancreatic cancer
What is the next test of choice in a patient with RUQ pain and an inconclusive US for cholecystitis?
Nuclear scan (HIDA or PIPIDA)
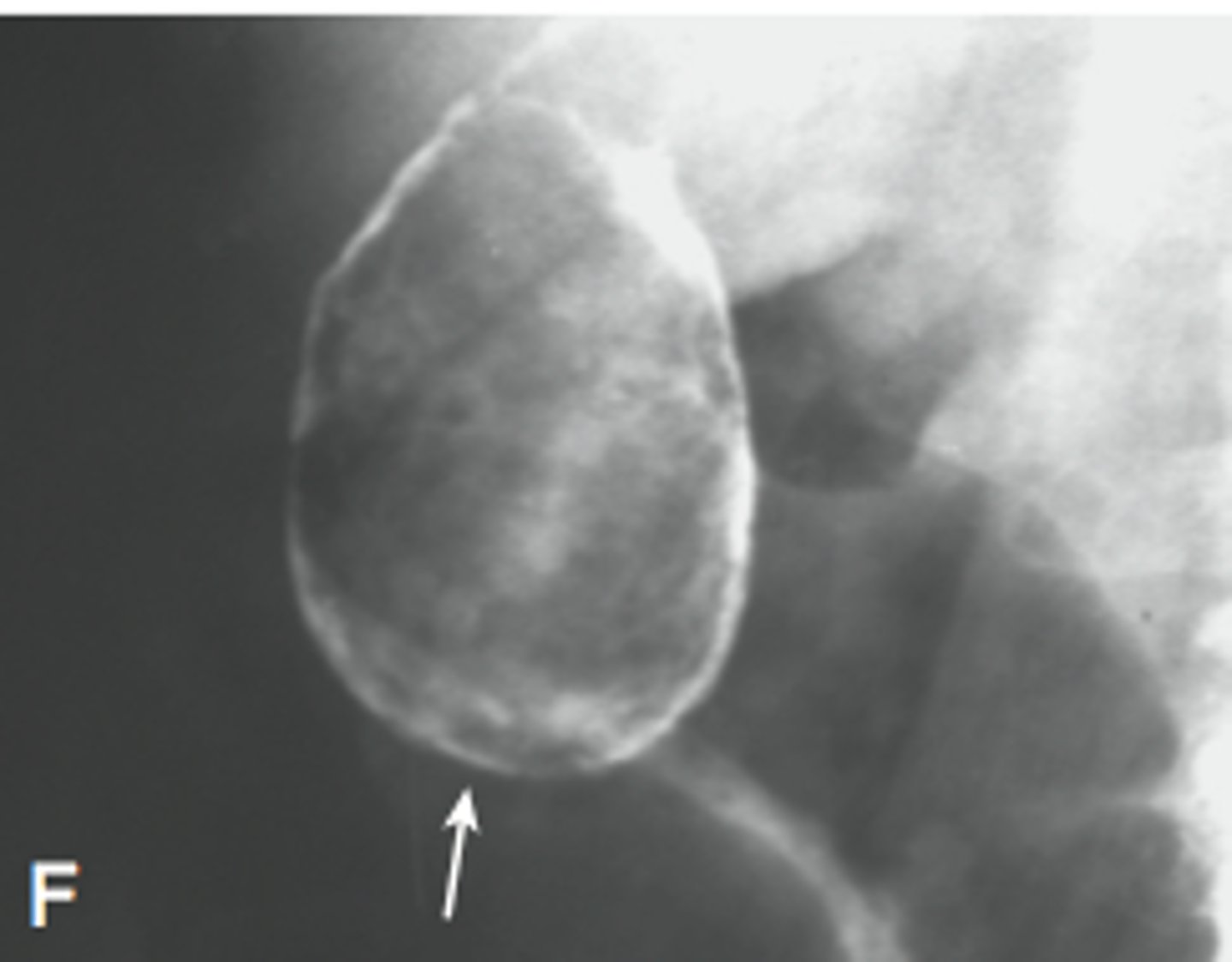
A patient presents to your office with weight loss and a palpable mass in the right upper quadrant. What X-ray finding supports gallbladder cancer?
Porcelain gallbladder
A patient with cholangitis develops confusion and hypertension. What do you suspect?
Acute obstructive suppurative cholangitis
A patient presents with fever, jaundice, and right upper quadrant pain. What do you suspect?
Cholangitis
During an exam, palpation of the right upper quadrant during inspiration causes the patient to stop breathing in due to pain. What is the initial test of choice?
RUQ Ultrasound
What antibiotic is a major cause of biliary sludge?
Ceftriaxone
RUQ tenderness + jaundice + fever
Charcot's triad (describing the presentation of cholangitis)
Charcot's triad + altered mental status + hypotension
Reynold's pentad
Jaundice and pruritus. Associated with IBD, cholangiocarcinoma, pancreatic cancer, colorectal cancer
Primary sclerosing cholangitis
Accounts for > 85% of gallstones in the Western world
Cholesterol stones
Slate colored skin may represent which underlying GI disorder?
Primary Biliary Cirrhosis
Diffuse, multifocal strictures and focal dilation of bile ducts with a "beaded look" are found on a patient with ulcerative colitis. What is your suspected diagnosis?
Primary Sclerosing cholangitis
What are +Anti-Mitochondrial antibodies associated with?
Primary Biliary Cirrhosis
What is the Dx? Fatigue Pruritus hepatomegaly associated with high ALK PHOS cholesterol and bilirubin.
Primary Biliary Cirrhosis
What does a porcelain gallbladder or a radiopaque gallbladder on imaging suggest?
Gallbladder cancer
RUQ palpation maneuver reveals pain and cessation of inspiration. What is this called? What does it indicate?
Murphy's sign = cholecystitis
Primary biliary cirrhosis often has a high elevation of alkaline phosphatase and bilirubin levels. What is the gold standard for diagnosis?
Gold standard - antimitochondrial antibodies found with liver biopsy
A 45 year old female presents with painful defecation, pruritus of the anus and occasional blood. What is your diagnosis?
Internal hemorrhoids
Significant rectal pain, and pruritus but no bleeding. Affects the lower 1/3 of anus (below dentate line)
External hemorrhoids
A 55-year-old patient with rectal bleeding and tenesmus (a feeling of incomplete emptying after a bowel movement). What must you consider?
Anorectal cancer
Whenever rectal bleeding occurs, even in patients with obvious hemorrhoids or known diverticular disease, coexisting cancer must be ruled out
Tearing rectal pain and bleeding which occurs with or shortly after defecation, bright red blood on toilet paper
Anal fissure
What type of hemorrhoids are usually painless?
Internal hemorrhoids
Treatment for fecal impaction?
Digital rectal /manual disimpaction - Diet with fiber stool softeners/laxatives for prevention
What is the recommended treatment for a perianal cyst?
Surgical drainage
Rectal mass rectal bleeding and tenesmus?
Rectal cancer (solitary tenesmus may occur with anal inflammation)
The definition of constipation is less than how many bowel movements per week?
less than 3 bowel movements per week
LLQ pain, tenderness, abdominal distention, fever and leukocytosis in older patients
Diverticulitis
Describe diverticulitis
Infection or perforation of a diverticulum
What is diverticulosis?
Condition in which diverticula can be found within the colon, especially the sigmoid; diverticula are actually false diverticula in that only mucosa and submucosa herniate through the bowel musculature; true diverticula involve all layers of the bowel wall and are rare in the colon
Describe the pathophysiology of diverticulosis?
Weakness in the bowel wall develops at points where nutrient blood vessels enter between antimesenteric and mesenteric taeniae; increased intraluminal pressures then cause herniation through these areas
What is the pathophysiology of diverticulitis?
Obstruction of diverticulum by a fecalith leading to inflammation and microperforation
What are the signs/ symptoms diverticulitis?
LLQ pain (cramping or steady), change in bowel habits (diarrhea), fever, chills, ano- rexia, LLQ mass, nausea/vomiting, dysuria
What are the associated lab findings of diverticulitis?
Increased WBCs
What are the associated radiographic findings of diverticulitis?
On x-ray: ileus, partially obstructed colon, air-fluid levels, free air if perforated On abdominal/pelvic CT scan: swollen, edematous bowel wall; particularly helpful in diagnosing an abscess
What are the associated barium enema findings of diverticulitis?
Barium enema should be avoided in acute cases
Is colonoscopy safe in an acute setting of diverticulitis?
No, there is increased risk of perforation
What are the possible complications of diverticulitis?
Abscess, diffuse peritonitis, fistula, obstruction, perforation, stricture
What is the most common fistula with diverticulitis?
Colovesical fistula (to bladder)
What is the best test for diverticulitis?
CT scan
What is the initial therapy of diverticulitis?
IV fluids, NPO, broad-spectrum antibiotics with anaerobic coverage, NG suction (as needed for emesis/ileus)
When is surgery warranted for diverticulitis?
Obstruction, fistula, free perforation, abscess not amenable to percutaneous drainage, sepsis, deterioration with initial conservative treatment
What is the lifelong risk of recurrence after: First episode of diverticulitis?
33%
What are the indications for elective resection in diverticulitis?
Case by case decisions, but usually after two episodes of diverticulitis; should be considered after the first episode in a young, diabetic, or immunosuppressed patient or to rule out cancer
What surgery is usually performed ELECTIVELY for recurrent bouts of diverticulitis?
One-stage operation: resection of involved segment and primary anastomosis (with preoperative bowel prep)
What type of surgery is usually performed for an acute case of diverticulitis with a complication (e.g., perforation, obstruction)?
Hartmann's procedure: resection of the involved segment with an end colostomy and stapled rectal stump (will need subsequent re-anastomosis of colon usually after 2-3 postoperative months)
What is the treatment of diverticular abscess?
Percutaneous drainage; if abscess is not amenable to percutaneous drainage, then surgical approach for drainage is necessary
How common is massive lower GI bleeding with diverticulitis?
Very rare! Massive lower GI bleeding is seen with diverticulosis, not diverticulitis
What are the most common causes of massive lower GI bleeding in adults?
Diverticulosis (especially right sided), vascular ectasia
What must you rule out in any patient with diverticulitis/ diverticulosis?
Colon cancer
What is an anal fissure?
Tear or fissure in the anal epithelium
What is the most common site of anal fissure?
Posterior midline (comparatively low blood flow)
What is the cause of anal fissure?
Hard stool passage (constipation), hyperactive sphincter, disease process (e.g., Crohn's disease)
What are the signs/symptoms of anal fissure?
Pain in the anus, painful (can be excruciating) bowel movement, rectal bleeding, blood on toilet tissue after bowel movement, sentinel tag, tear in the anal skin, extremely painful rectal exam, sentinel pile, hypertrophic papilla
What is a sentinel pile?
Thickened mucosa/skin at the distal end of an anal fissure that is often confused with a small hemorrhoid
What is the anal fissure triad for a chronic fissure?
1. Fissure
2. Sentinel pile
3. Hypertrophied anal papilla
What is the conservative treatment?
Sitz baths, stool softeners, high fiber diet, excellent anal hygiene, topical nifedipine, Botox®
What disease processes must be considered with a chronic anal fissure?
Crohn's disease, anal cancer, sexually transmitted disease, ulcerative colitis, AIDS
What are the indications for surgery?
Chronic fissure refractory to conservative treatment
What is one surgical option?
Lateral internal sphincterotomy (LIS)—cut the internal sphincter to release it from spasm
What is the "rule of 90%" for anal fissures?
90% occur posteriorly 90% heal with medical treatment alone 90% of patients who undergo an LIS heal successfully
What are hemorrhoids?
Engorgement of the venous plexuses of the rectum, anus, or both; with protrusion of the mucosa, anal margin, or both
Why do we have "healthy" hemorrhoidal tissue?
It is thought to be involved with fluid/air continence
What are the signs/symptoms?
Anal mass/prolapse, bleeding, itching, pain
Which type, internal or external, is painful?
External, below the dentate line
If a patient has excruciating anal pain and history of hemorrhoids, what is the likely diagnosis?
Thrombosed external hemorrhoid (treat by excision)
What are the causes of hemorrhoids?
Constipation/straining, portal hypertension, pregnancy
What is an internal hemorrhoid?
Hemorrhoid above the (proximal) dentate line
What is an external hemorrhoid?
Hemorrhoid below the dentate line
What are the three "hemorrhoid quadrants"?
1. Left lateral 2. Right posterior 3. Right anterior
Define the following terms for internal hemorrhoids:
First-degree
Second-degree
Third-degree
Fourth-degree
First-degree hemorrhoid: Hemorrhoid that does not prolapse
Second-degree hemorrhoid: Prolapses with defecation, but returns on its own
Third-degree hemorrhoid: Prolapses with defecation or any type of Valsalva maneuver and requires active manual reduction (eat fiber!)
Fourth-degree hemorrhoid: Prolapsed hemorrhoid that cannot be reduced
What is the treatment of hemorrhoids?
High-fiber diet, anal hygiene, topical steroids, sitz baths Rubber band ligation (in most cases anesthetic is not necessary for internal hemorrhoids) Surgical resection for large refractory hemorrhoids, infrared coagulation, harmonic scalpel
What is a "closed" vs. an "open" hemorrhoidectomy?
Closed (Ferguson) "closes" the mucosa with sutures after hemorrhoid tissue removal Open (Milligan-Morgan) leaves mucosa "open"
What are the dreaded complications of hemorrhoidectomy?
Exsanguination (bleeding may pool proximally in lumen of colon without any signs of external bleeding) Pelvic infection (may be extensive and potentially fatal) Incontinence (injury to sphincter complex) Anal stricture
What condition is a contraindication for hemorrhoidectomy?
Crohn's disease
Classically, what must be ruled out with lower GI bleeding believed to be caused by hemorrhoids?
Colon cancer (colonoscopy)
Crohn disease is an inflammatory bowel disease that can affect what portion of the gastrointestinal tract?
Any portion of the gastrointestinal tract, though often spares the rectum.
Crohn disease is more commonly associated with mucosal or transmural transmural inflammation?
Crohn disease is an inflammatory bowel disease that is more commonly associated with transmural inflammation and skip lesions.
Name two monoclonal antibodies that can be used to treat Crohn disease
Adalimumab and infliximab are two monoclonal antibodies that can be used to treat Crohn disease by binding to tumor necrosis factor-alpha.
Crohn disease causes what type of appearance in the mucosa?
cobblestone appearance in the mucosa
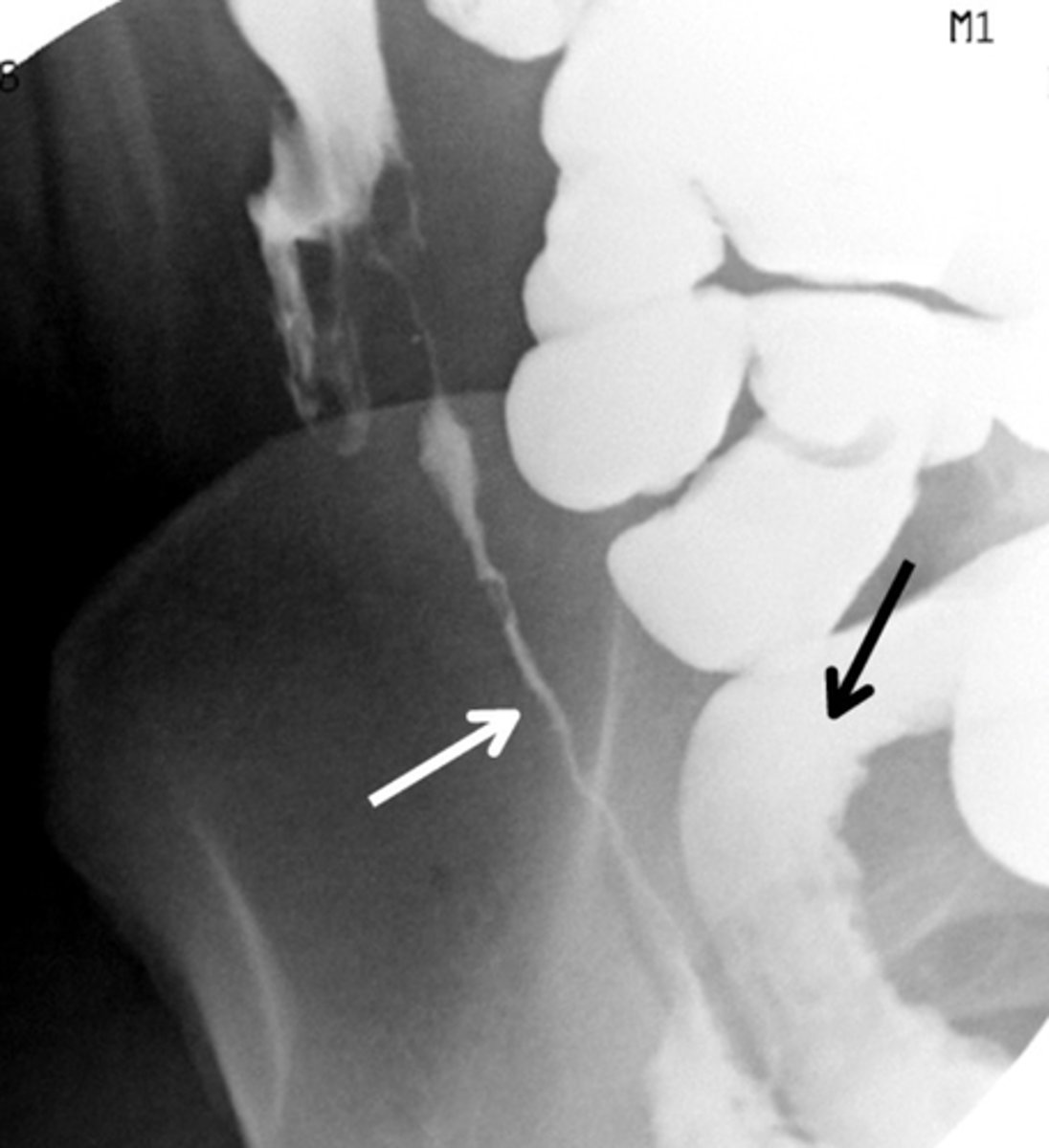
What is classically seen on abdominal X-ray in a patient with Crohn disease
Crohn disease is associated with the string sign or narrowing of the bowel lumen on X-ray
Crohn disease most commonly affects... ?
The ileum and colon
Ulcerative colitis is an inflammatory bowel disease that involves what layers of the GI tract?
Ulcerative colitis is an inflammatory bowel disease that involves only mucosal and submucosal inflammation
Ulcerative colitis is limited to what sections of the GI tract?
Ulcerative colitis is limited to the colon, including the rectum
Ulcerative colitis is associated with what symptoms?
Left lower quadrant pain and bloody diarrhea
Describe x-ray finding in ulcerative colitis
Pseudopolyps, loss of haustra, and a resultant "lead pipe" appearance on imaging

Name the oral extraintestinal manifestation of Crohn disease and ulcerative colitis
Aphthous stomatitis is an oral extraintestinal manifestation of Crohn disease and ulcerative colitis.
What is the definitive surgical treatment of ulcerative colitis?
Colectomy is the definitive surgical treatment of ulcerative colitis.
What is the first line treatment of ulcerative colitis?
The first line treatment of ulcerative colitis is 5-aminosalicylic preparations such as mesalamine.
Name a complication of ulcerative colitis that may be a presenting symptom
A complication of ulcerative colitis that may be a presenting symptom is toxic megacolon, which is severe dilation of the colon.
Name a complication of ulcerative colitis that is usually not a concern until after ten years of disease
Adenocarcinoma of the colon can be a complication of ulcerative colitis that is usually not a concern until after ten years of disease.
What characterizes irritable bowel syndrome
Irritable bowel syndrome is a gastrointestinal disorder characterized by recurrent abdominal pain, bloating, and regular changes in bowel habits typically between constipation or diarrhea
Who is most commonly affects by IBS?
Irritable bowel syndrome most commonly affects middle-aged women
Name two medications indicated for the treatment of irritable bowel syndrome?
Hyoscyamine and dicyclomine are antimuscarinic antispasmodics indicated for irritable bowel syndrome
What dietary modification may relieve symptoms of irritable bowel syndrome in patients with constipation as the primary symptom?
Increased dietary fiber may relieve symptoms of irritable bowel syndrome in patients with constipation as the primary symptom, as symptoms normally improve with defecation
Colicky abdominal pain, nausea, bilious vomiting, obstipation, abdominal distention, hyperactive bowel sounds (early) or hypoactive bowel sounds (late), prior abdominal surgery
Small bowel obstruction
Gradually increasing abdominal pain with longer intervals between episodes of pain, abdominal distention, obstipation, less vomiting (feculent), more common in the elderly
Large bowel obstruction