Neuro review
1/15
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
16 Terms
Schiff sherrington
Hyperextension of TLs, paralysis of HLs
Thoracic or cranial lumbar spine
Decerebrate rigidity
Extension of all limbs and opisthotonus, stuporous or comatosed
Rostral brainstem
Decerebellate rigidity
Hyperextension of TLs and opisthotonus, mentation normal
Rostral part of cerebellum
Describing paresis
Tetraparesis - all limbs
Paraparesis - pelvic limbs
Monoparesis - 1 limb
Hemiparesis - both limbs same side
Either ambulatory or non ambulatory
4 aspects of neurological exam
Postural reactions
Spinal reflexes and muscle tone
Spinal pain
Cranial nerve examination
Postural testing
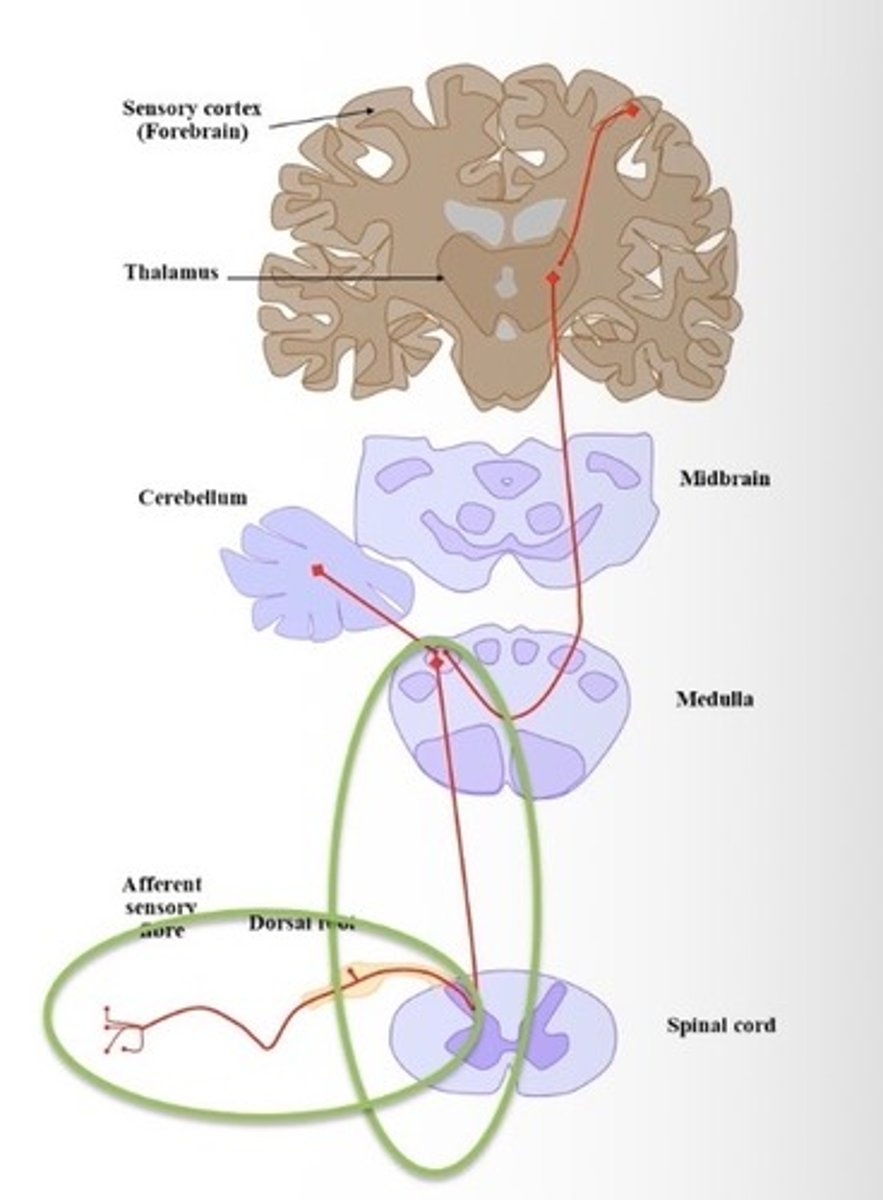
Proprioceptors > contralateral forebrain or ipsilateral cerebellum
Postural tests
Paw position
Hopping
Placing responses
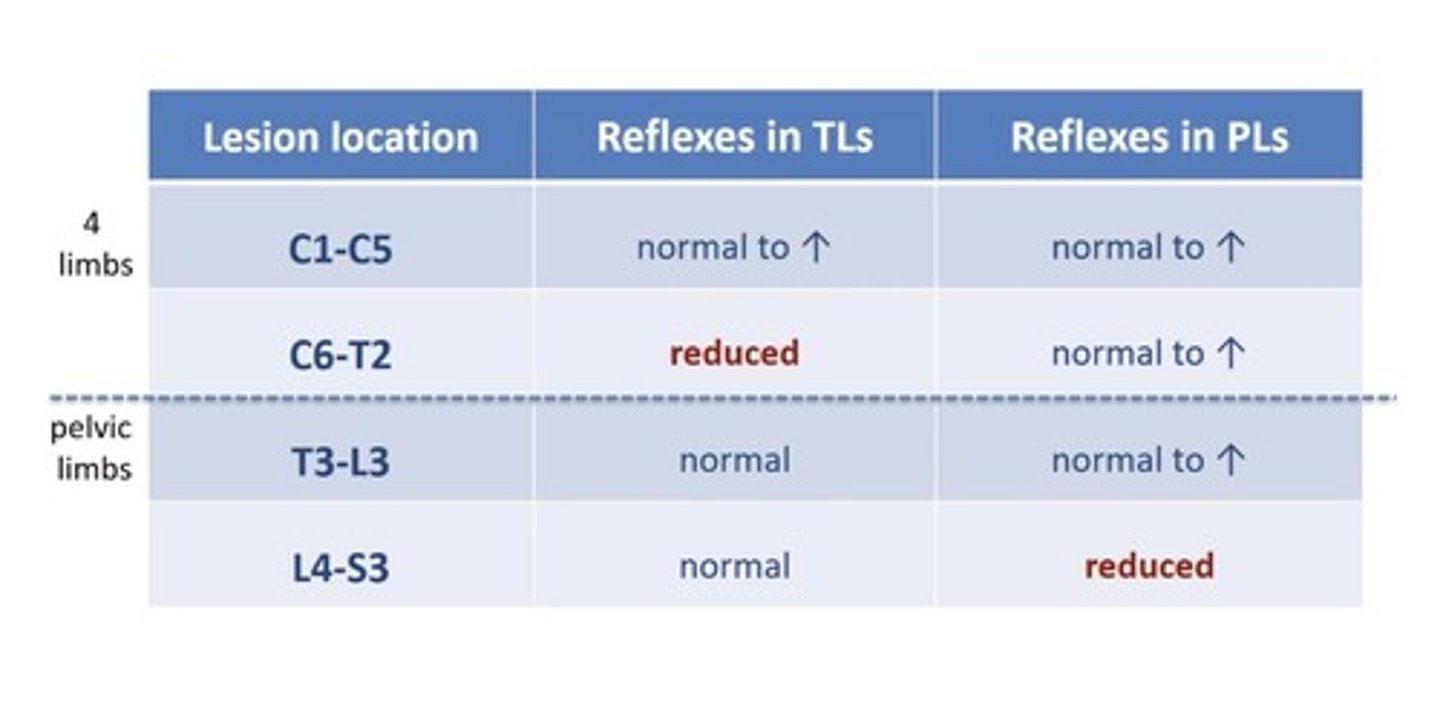
Where is the spinal lesion?
C1-T2 all legs affected
T3-S3 pelvic limbs affected
C6-T2 - spinal reflexes in thoracic limbs
L4-S3 spinal reflexes in pelvic limbs
Types of spinal reflexes
Withdrawals
TL:
- Extensor carpi radialis
- Biceps
- Triceps
HLs:
- withdrawals
- patellar
- cranial tibial
- gastrocnemius
- perineal
Misinterpretation of spinal reflexes
pain causes reduced reflexes
Very subtle lesion may not affect reflex pathway
Patellar reflex reduced in olf age
Spinal shock
CN testing
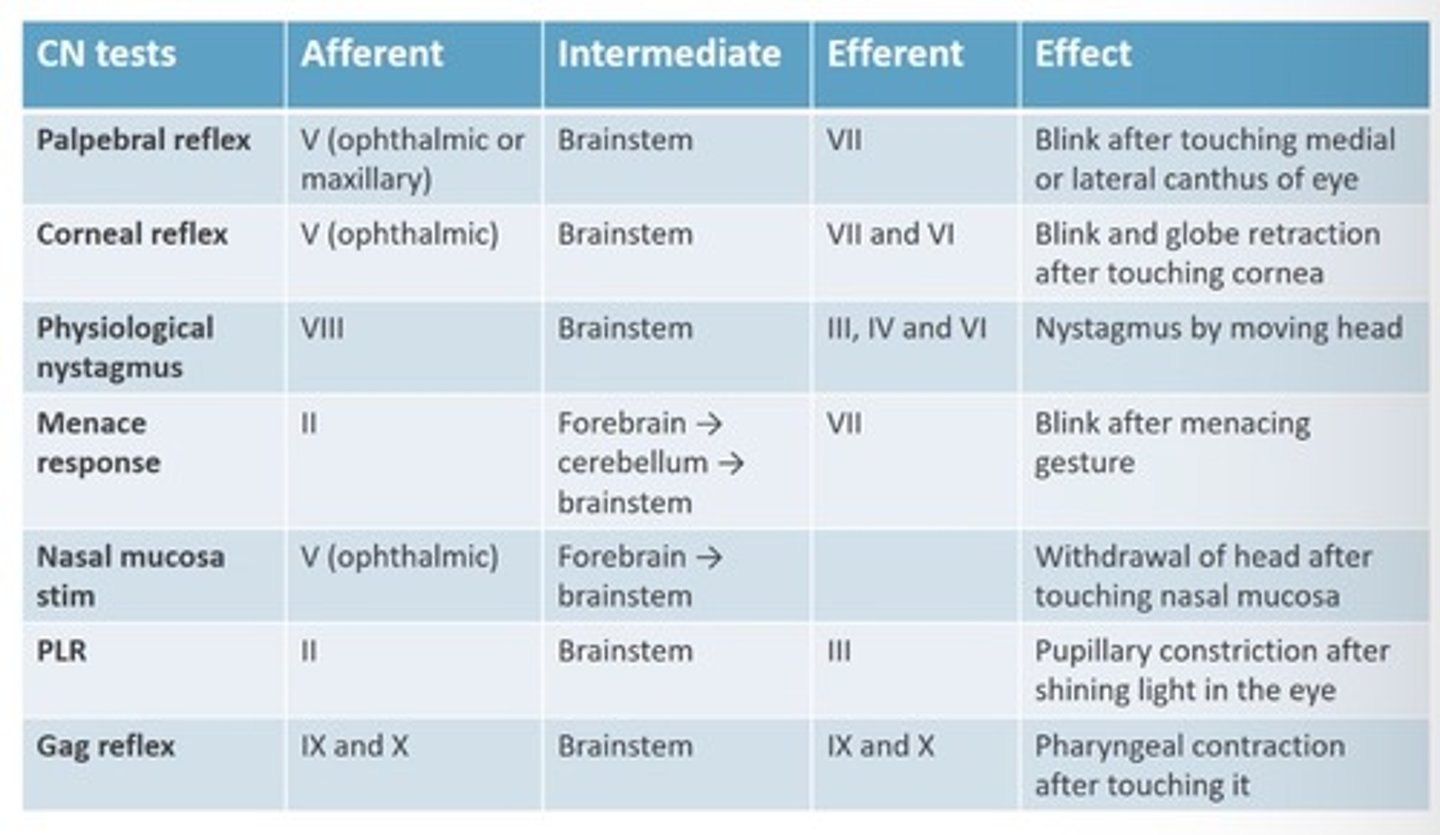
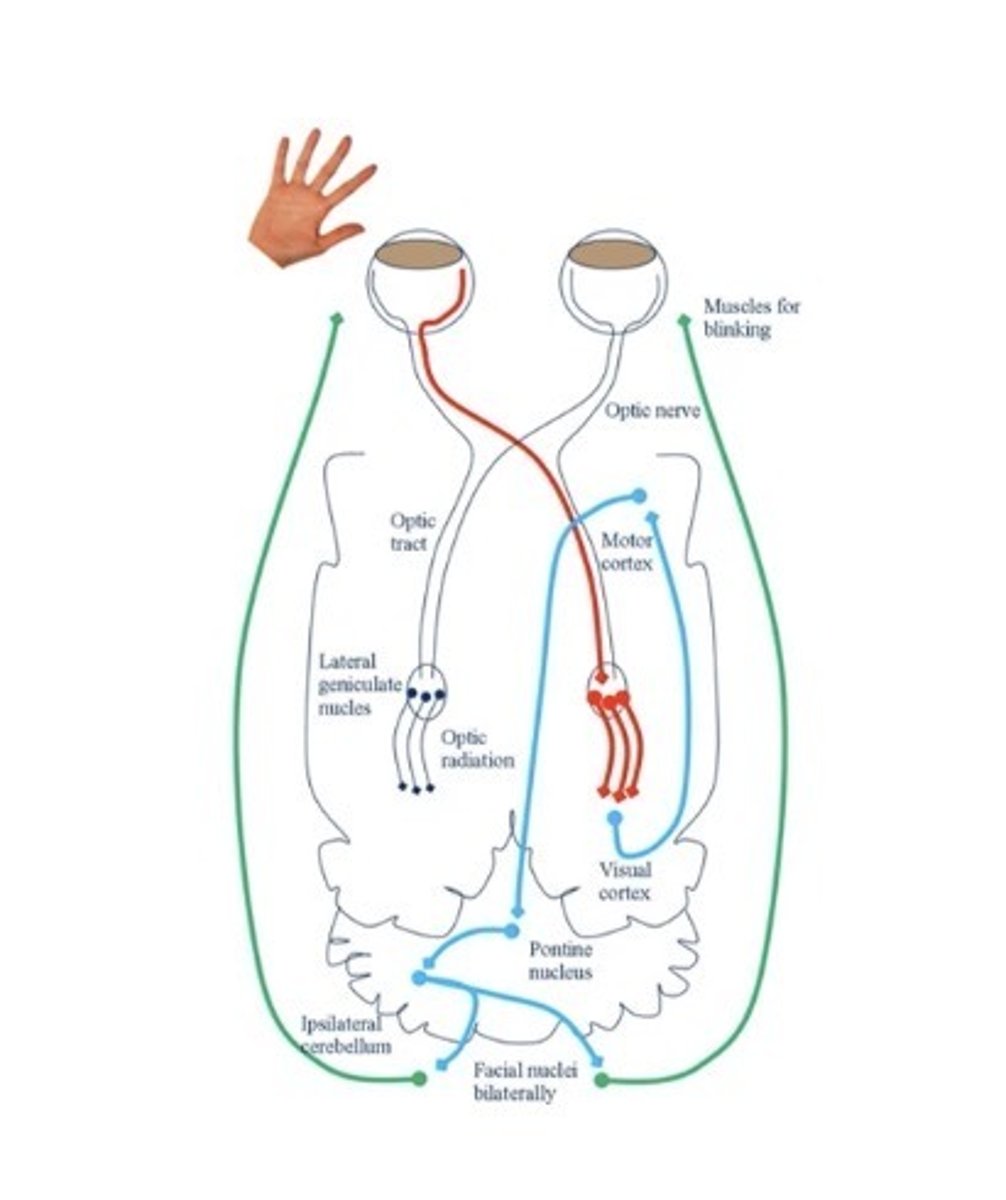
Menace resposne
input - II
Forebrain, cerebellum, brainstem
Output - VII
Learnt response - learnt response, present from ~12wks
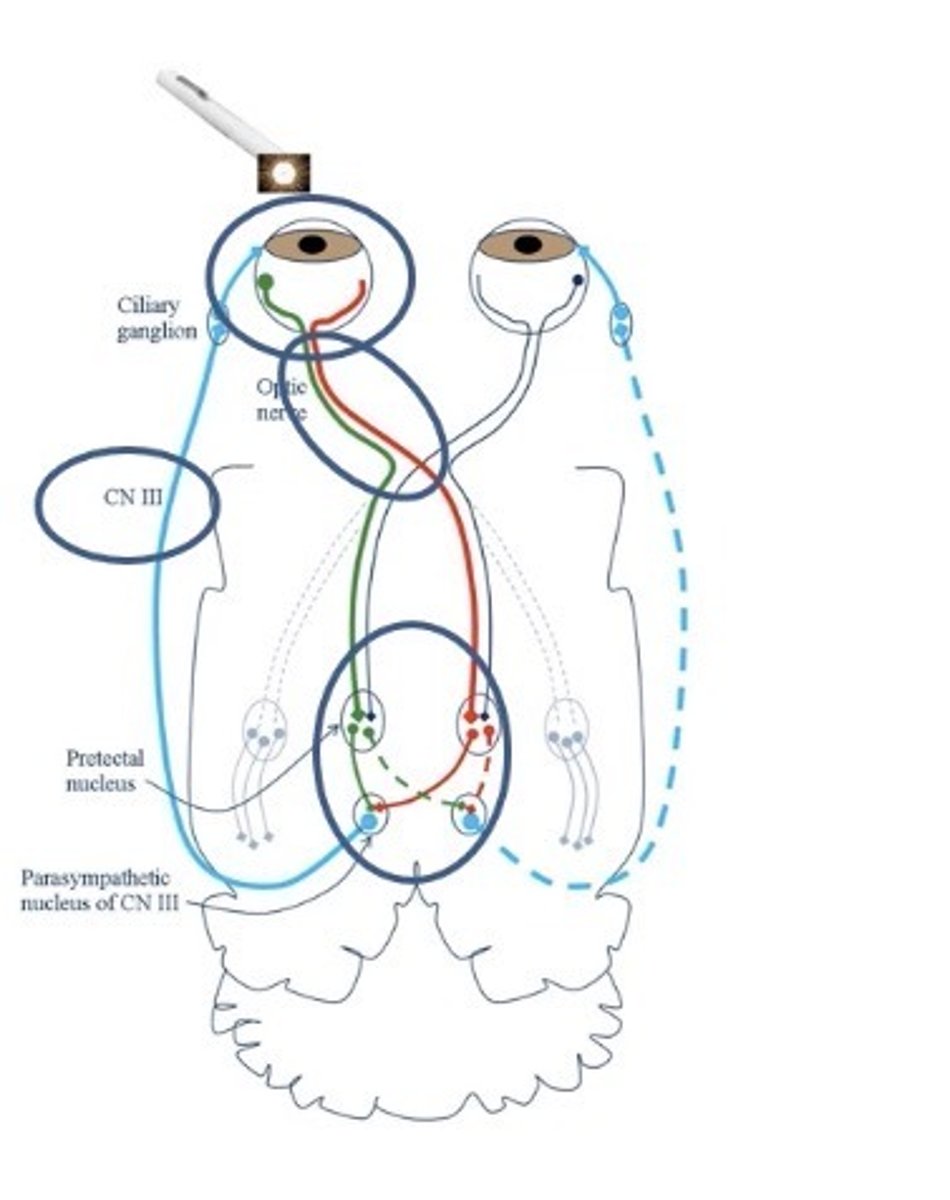
Pupillary light reflex
input - II
Output - III
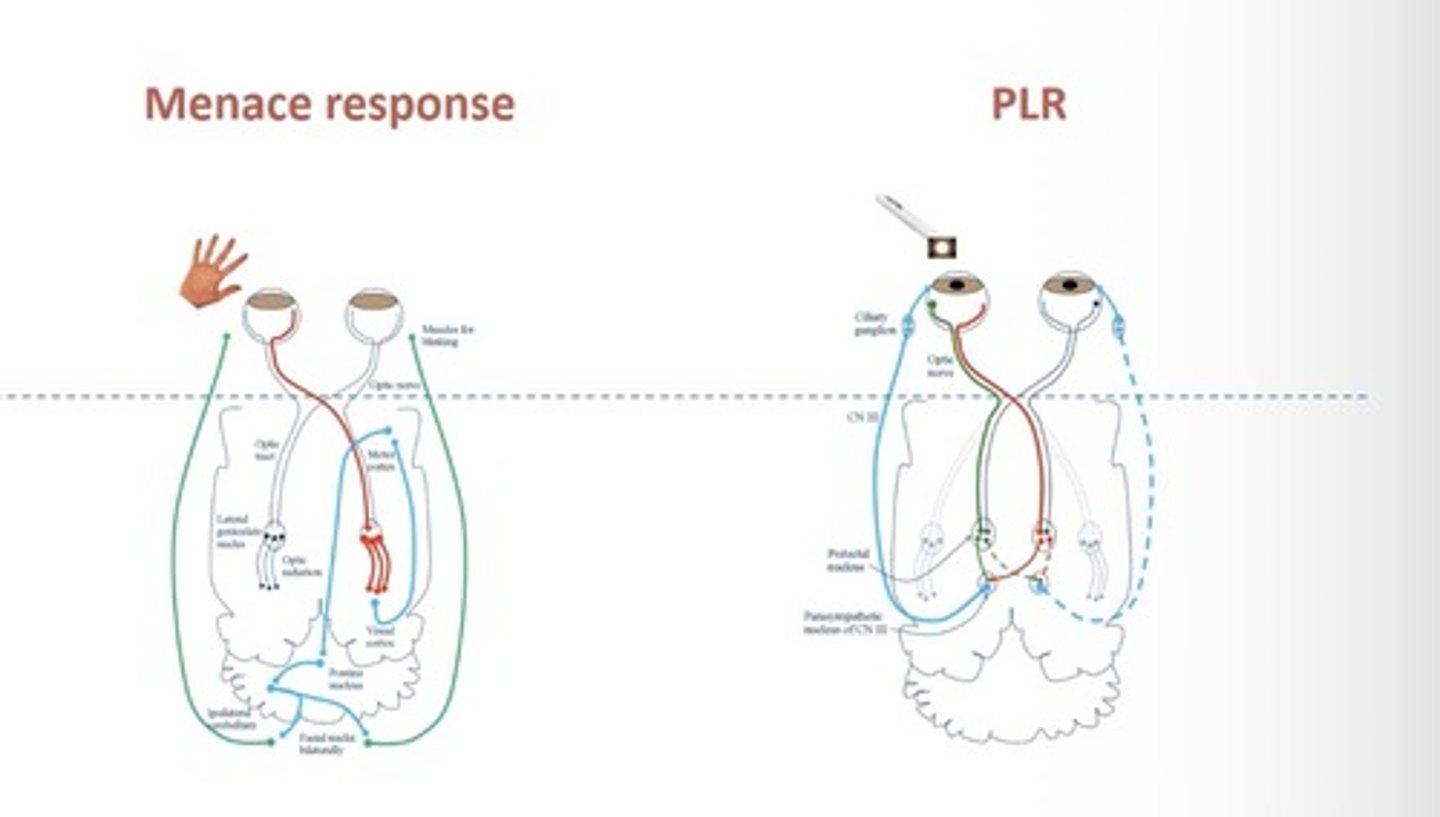
Where do the menace and PLR pathways overlap?
Gag reflex
Input IX and X brainstem
Output IX and X
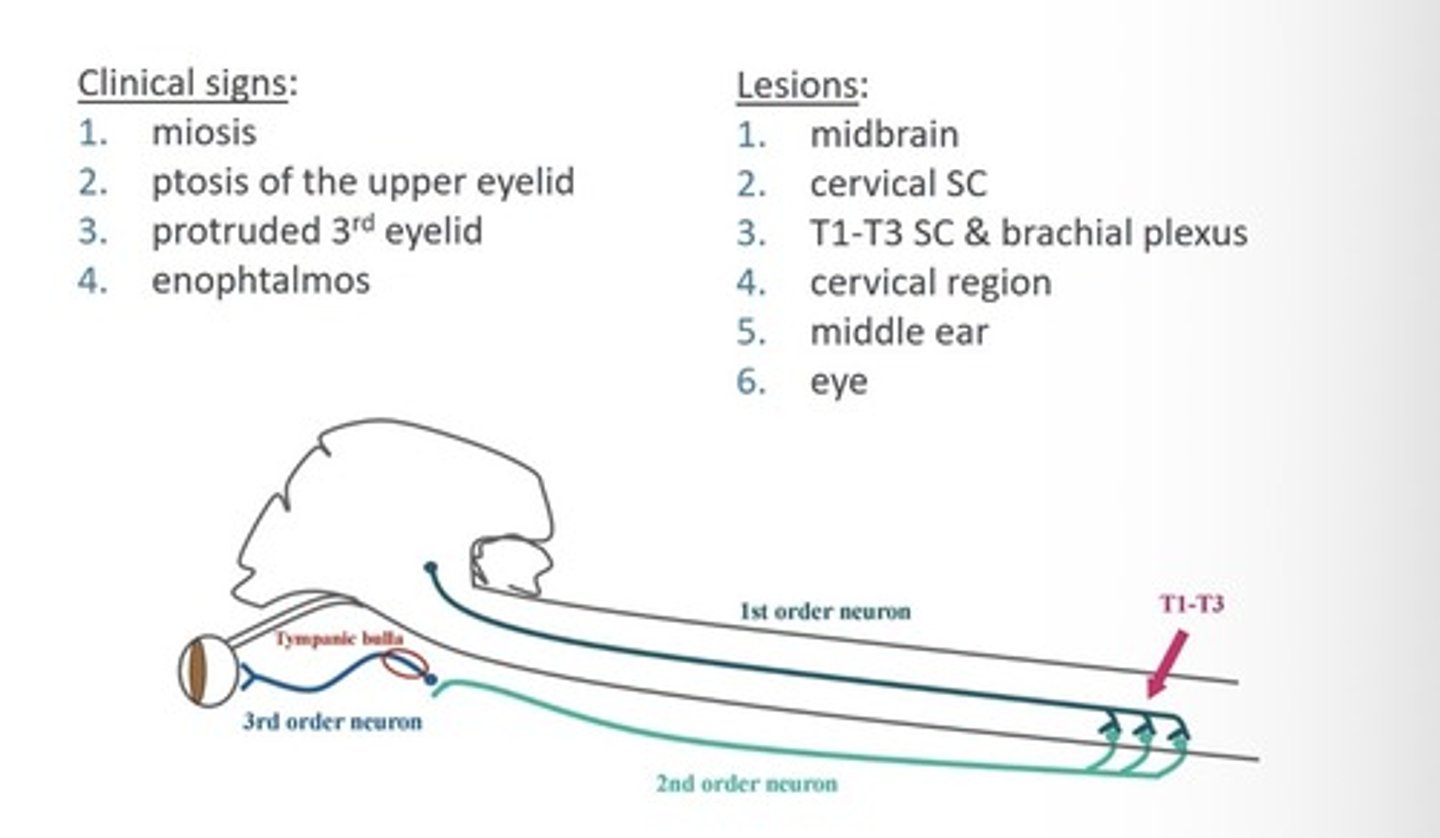
Horners