EMT Exam 1 Diagram | Quizlet
1/99
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
100 Terms
Why is the year 1966 is important to EMS.
National Highway Safety Act charged the U.S. Department of Transportation (DOT) with developing EMS standards.
"White paper"
the document that lays the foundation for modern EMS
Emergency Medical Responder (EMR)
1st Responder; immediate care for life threatening injuries; controlling the scene
Emergency Medical Technician (EMT)
Basic; basic medical care, trauma interventions, and transport
Advance Emergency Medical Technician (AEMT)
Basic Life Support and Advance Life Support; i.e. advance airways, blood sugar, and intervenous medications
Paramedic
this healthcare provider possess the skill set of an EMT and AEMT in addition to other advance life support
Who is responsible for EMS at a federal level?
the Department of Transportation
Who is responsible for an EMS system as a whole?
National Highway Traffic Safety Administration
Who is responsible for the care of a patient?
Medical Director
Scene Size Up
(1) Is the scene safe?
(2) PPE/BSI
(3) MOI/NOI
(4) # of Patients
(5) Call for Additional Resources?
MOI
Mechanism of Injury [trauma]
NOI
Nature of Illness [medical]
BSI
Body Substance Isolation
Secondary Assessment
(1) Physical Exam: DCAP/P-BTLS
(2) Past Medical History(PMH): SAMPLE
(3) History of Present Illness (HPI): OPQRST
(4) Vital Signs
Vital Signs
~Level of Consciousness (LOC)
~Pulse (Carotid and Radial)
~Respirations & Lung Sounds
~Blood Pressure
~Skin (Temperature, Color, Condition)
-Pupils
-Capillary Refill (pt. under 6 y/o)
Primary Assessment
(1) General Impression
(2) C-Spine consideration
(3) Mental Status
(4) A.B.C.
(5) Identify Patient Priority
Reassessment process is
when you repeat BOTH the Primary and Secondary Assesment, including Vital Signs and Patient Priority
How often are Reassessments conducted for LOW Priority patients?
Every 15 minutes
How often are Reassessments conducted for HIGH Priority patients?
Every 5 minutes
When is a Detailed Assessment performed?
...when the patient is in transit to the hospital
Detailed Assessment
(1) Assess Mental Status
(2) Emphasis on C.C. and prior exam
(3) Reassess Vital Signs
(4) Perform Rapid Trauma DCAP/P-BTLS
DCAP/P-BTLS
Deformities
Contusions
Abrasions
Punctures
____
Penetrations
Burns
Tenderness
Lacreations
Swelling
AVPU
regarding patient's responsiveness:
Alert
Verbal response
Painful response
Unresponsive
What mnemonic do you use to assess mental status during the Primary Assesment?
AVPU
Upper Airway
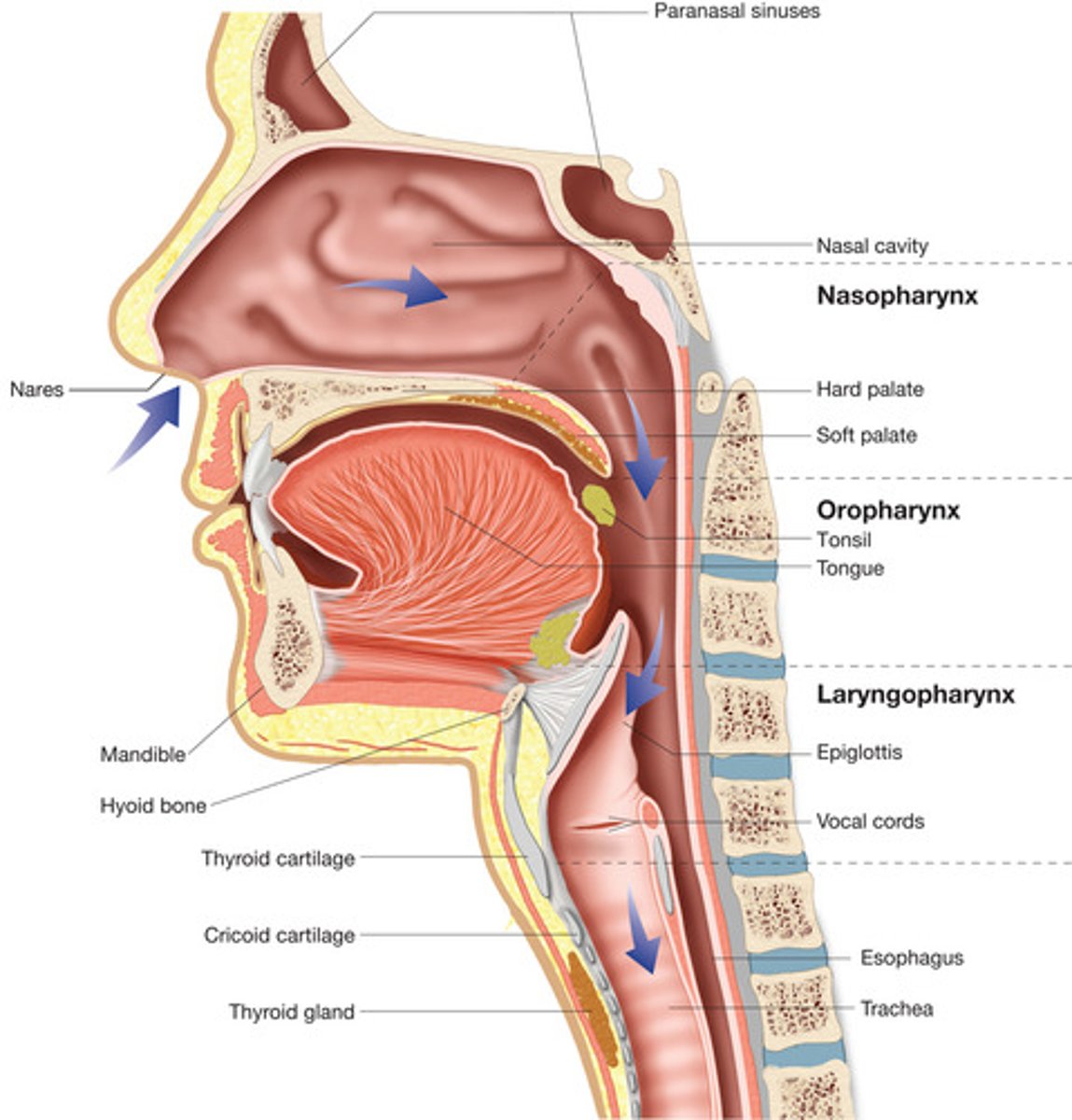
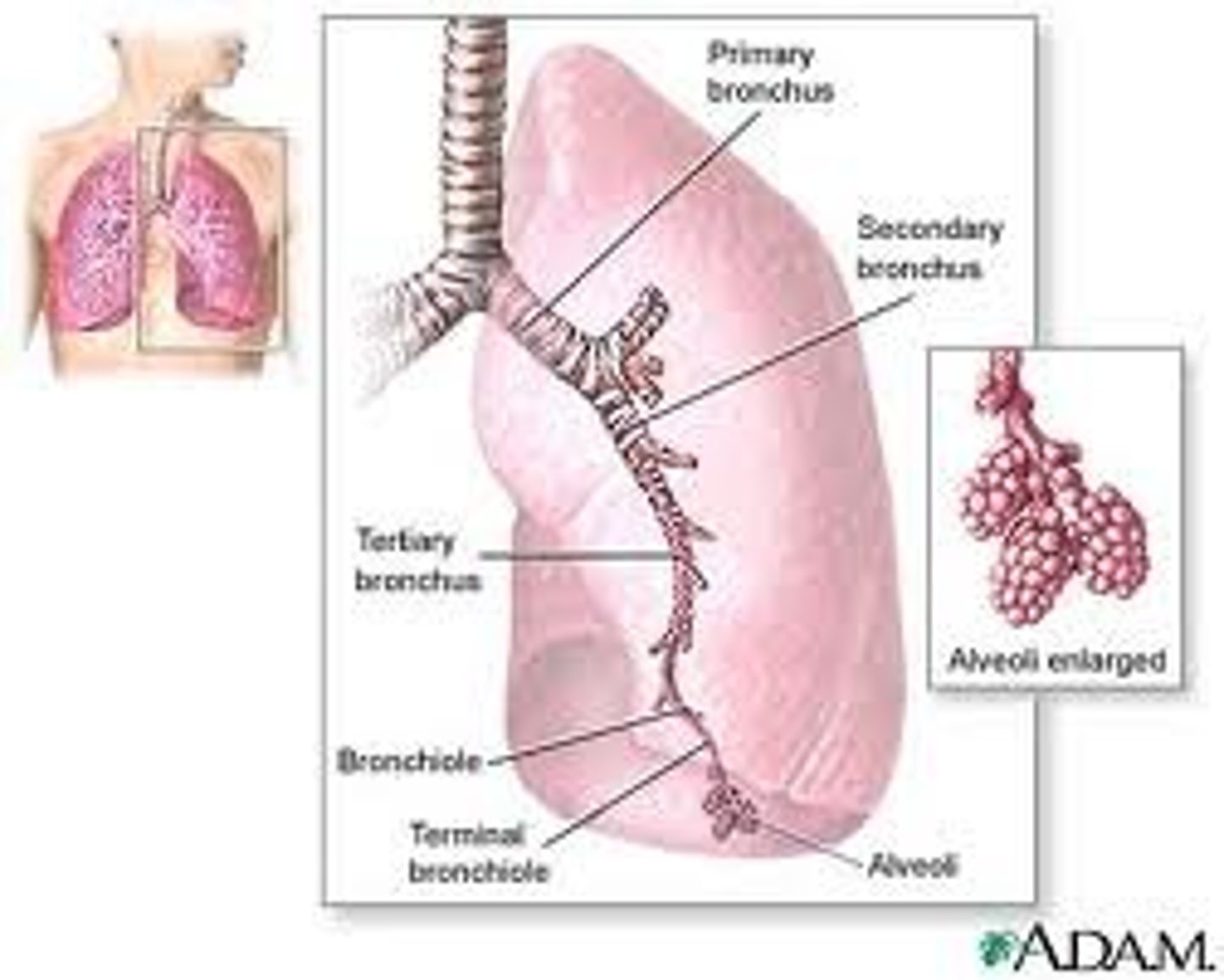
Lower Airway
Rules of Suctioning
(1) Wear PPE
(2) Suction for no more than 10 seconds
(3) Suction on the way (OUT)
*If a patient is vomiting purfuselly, keep suctioning
What could happen if you suction a patient's airway for too long?
...the patient may become hypoxic
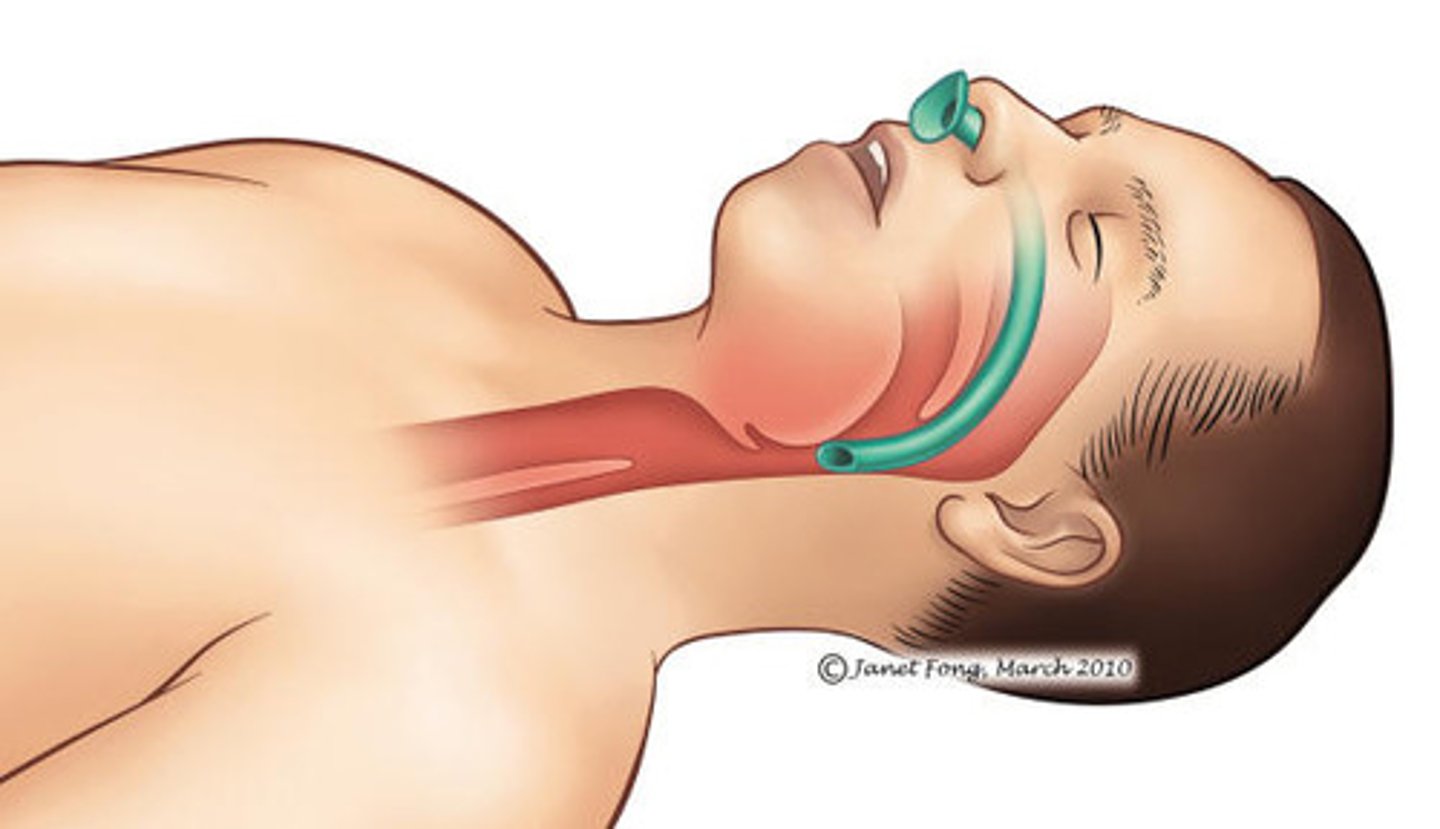
How do you OPEN an Airway?
~ Head tilt, Chin lift
~ Jaw Thrust
~ Airway Adjuncts
~Suctioning
How do you ASSESS an Airway?
Look, Listen, and Feel
Characteristics of a Poor Airway
~Abdominal breathing
~Diminished breath sounds
~Trouble speaking
~Retraction and Nasal Flaring (in Children)
Rapid Trauma Exam
When the patients is Unresponsive, has an Altered Mental Status OR a Severe M.O.I.
(1) C- Spine
(2) DCAP/P-BTLS: head to tow
(3) Immobilize the patient
(4) SAMPLE
(5) Vital Signs
Pulse Deficit
the conditionin which the central pulse is greater than the distal/periphial post
Pulsus Paradoxus
absent pulse during Inspiration
Anisocoria
the condition in which 1 pupil is always larger/smaller than the other
Pulse
characterized by Rhythm, Quality, & Rate
Hypoxia
low blood oxygen levels which leads to inadequate breathing
characterized by shallow breath, diminished/unusual sounds, cyanosis, a Blood oxygen saturation less than 95%
Airway Management
"Make it, Check it, Keep it"
When CO2 levels are HIGH and O2 levels are LOW
Patient will exhibit S.O.B., increased Respiration Rate and depth, & increase in Heart Rat
Tripod Position

What is the Intervention for Inadequate breathing?
Positive Pressure Ventilation
Hyperventilation leads to vasoconstriction -OR- vasodilation?
Vasoconstriction
BVM
Bag-Valve Mask
(i.e. Ambu Bag)
When artificially ventilating a patient with a stoma...
..Leave the Patient's head in a neutral position and clear mucus plugs
In which siutaitons do you ALWAYS provide supplemental Oxygenn?
~Cardiac Arrest
~Respiratory Arrest
~Repiratory Distress
~Other respiratory conditons
~Myocardial Infarction
~Stroke
~Shock
~Head injury
Non-Urgent Move
Patient is stable
Urgent Move
performed with precautions for spinal injury; rapid spinal immoblizaiton
Emergency Move
the scene is hazardous, move patient immediately:
Use dragging methods. (i.e. emergency clothes drag, blanket drag, arm drag, arm-to-arm drag)
How far is a severe fall?
Adult: 20ft
Child: 10ft OR twice their heigh
Non-Rebreather Mask
80-100% Oxygen
12 - 15 liters/minute
Nasal Cannula
24-44% Oxygen
4 - 6 liters/minute
Partial Rebreather/Simple Mask
40-60% Oxygen
9 - 10 liters/minute
Tracheotomy Mask
Placed over stoma
8 - 10 liters/minute
Up and Over Injury Pattern
i.e. head-on collision; starred windshield; C-Spine
Down and Under Injury Pattern
i.e. head-on collision; C-Spine; leg and hip injuries
Rear-End Collision
whip lash; C-Spine
Which type of motor vehicle collision is most likely to cause Ejection from the vehicle?
Rollover Collision
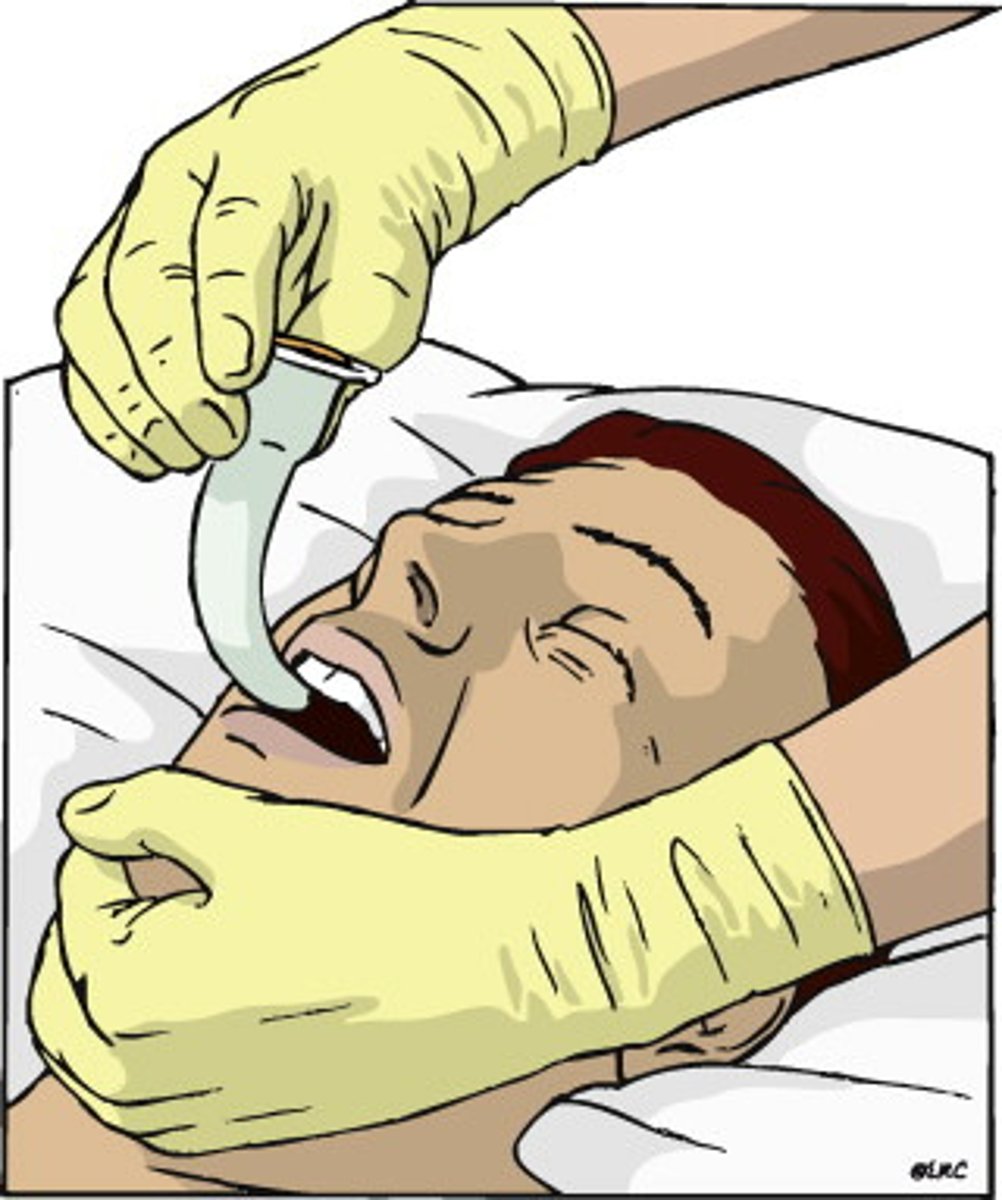
OPA
Used for:
~Unresponsive patients
~Patients with no gag reflex
NPA
Used for:
Patients with a gag reflex
Patients who will not tolerate the feeling of an OPA
SAMPLE
Sample
Allergies
Medications
Prior Medical History
Last Oral Intake
Events leading up to the incident
OPQRST
Onset
Palliation/Provocation
Quality
Radiation
Severity
Time
Trending
determined by Reassessment; indicates to the hospital/receiving providers if the patient is deteriorating or improving
CISD
Critical Incident Stress Debriefing
CISM
Critical Incident Stress Management system
Quality Assurance
= quality evaluation
Quality Improvement
= quality interventions
Oxygen Cylinders Rules
~Cylinders are always green
~ Keep containers filled to at least 200psi
~ Always store the cylinder laid down on its side
~No Smoking
Dead Airspace
150mL of air that rests in the lungs, but does not reach (the alveoli) for gas exchange
Chief Complaint (C.C.)
the reason why EMS was called; typically in the patient's own words
What mnemonic do you use to obtain a Past Medical History (PMH)
SAMPLE
What mnemonic do you use to obtain the History of Present Illness (HPI)?
OPQRST
Rules to Remember for Lifting and Moving
~Use your legs
~Keep the load close to your body
~Don't twist your torso
~Know your limits
~Feet shoulder width apart
Respiratory Distress
Adequate breathing with:
~unsual sounds
~normal or slighlty elevated breathing rate
~normal or pale skin
~Anxiety
Respiratory Failure
INadequate breathing with:
~unusual sounds
~too fast or too slow breaths
~Cyanosis
~Alerted Mental Status
Respiratory Arrest.
INadequate breathing with:
~NO breath sounds
~Cyanosis
~Unconsciousness
Emergency Response Guide
when determining whether or not the scene is safe; look for info about hazardous chemicals in this guide
Example of Supplemental Oxygen
Non Rebreather Mask, Nasal Cannula
Example of Artificial Ventilation
Pocket Face Mask, Bag Valve Mask (i.e. Ambu Bag)
How to calculate approximately normal BP for infants and children
Systolic= [80+ (2)(AGE)], Diastolic = [ (2/3) x (Systolic #)]
Shock
AKA Hypoperfusion: a life-threatening condition that occurs when the body is not getting enough blood flow.
Compensated Shock
When low blood flow (perfusion) is first detected by the body.A number of systems are activated in order to maintain/restore perfusion. The heart beats faster, the blood vessels become smaller in diameter, and the kidney works to retain fluid in the circulatory system to maximize blood flow to the most important organ systems of the body. The patient in this stage of shock has very few symptoms, and aggressive treatment may slow or stop progression to stage II shock
Decompensated Shock
When the methods of compensation begin to fail. The systems are unable to maintain perfusion any longer. Oxygen deprivation in the brain causes the patient to become confused and disoriented.
Irreversible Shock
The length of time that poor perfusion has existed begins to take a permanent toll on the body's organs and tissues. The heart's functioning continues to spiral downward, and the kidneys usually shut down completely. Cells in organs and tissues throughout the body are injured and dying. The endpoint is patient death.
Hospital Notification Script
(1) Address destination
(2) Identify self
(3) Relay: Age, Sex, C.C., Vitals, Status/Priorty, and ETA
Medical Command Script
(1) Address destination
(2) Identify self
(3) Why did I call?
(4) Relay: Age, Sex, C.C., Vitals, Status/Priorty, and ETA
(5) Assessment
(6) Response to treatment
(7) Vitals
(8) ETA
Crepitation
bone fragments rubbing together; identified during palpation
Acute Stress
fight or flight
Delayed Stress
i.e. PTSD
Cumulative Stress
Burnout
Stages of Stress
(1) ALARM---fight or flight
(2) RESISTANCE---coping
(3) EXHAUSTION
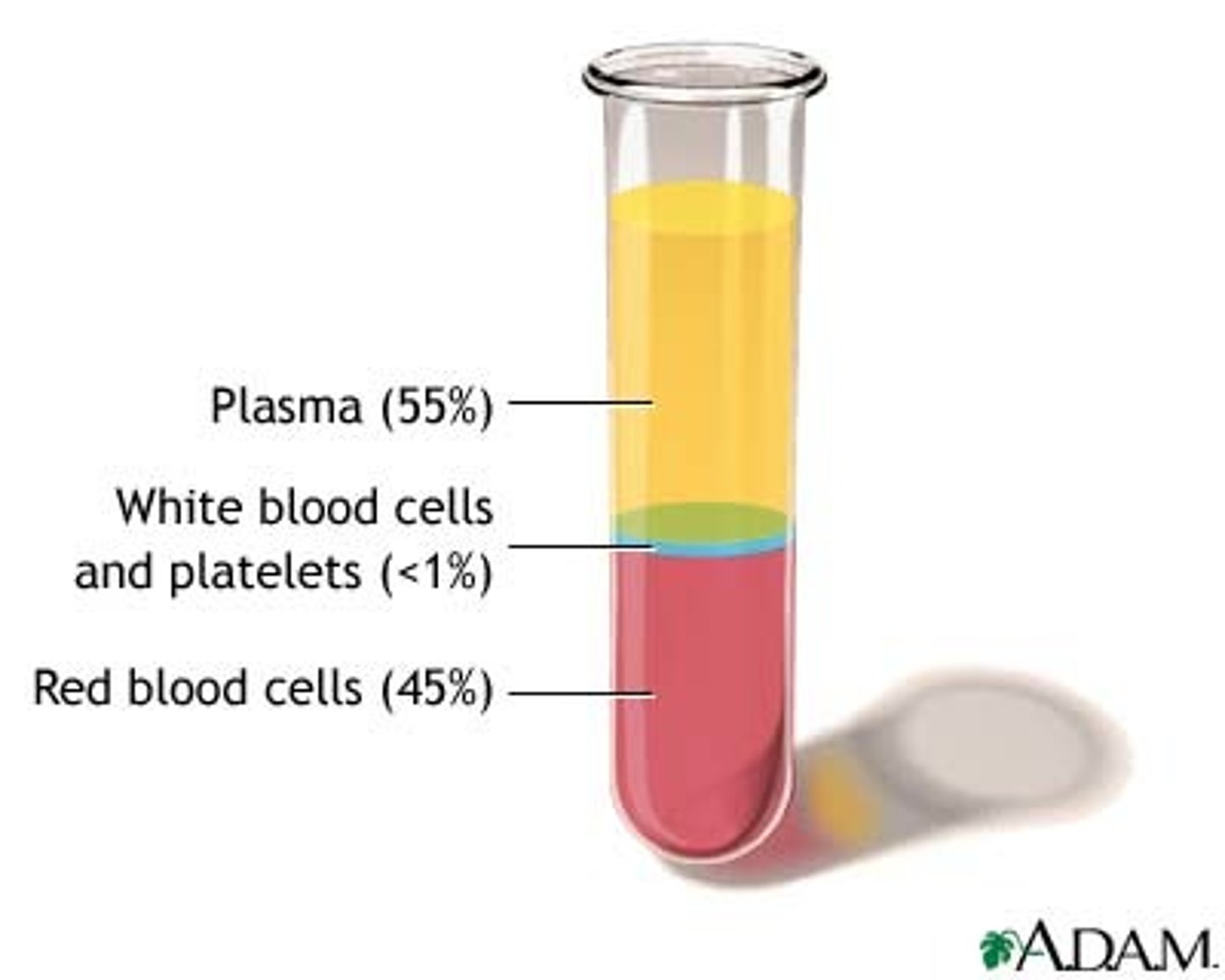
Components of Blood
Portable Radio
radio carried by an EMT
Mobile Radio
radio fixed to an ambulance
Base Radio
radio located at the hospital
What is the #1 Rule?
Safety!
Inspiration
an active process; negative (-) pressure
Expiration
a passive process; positive (+) pressure
Ventilation
the movement of air in/out of the lungs
Respiration
gas exchange
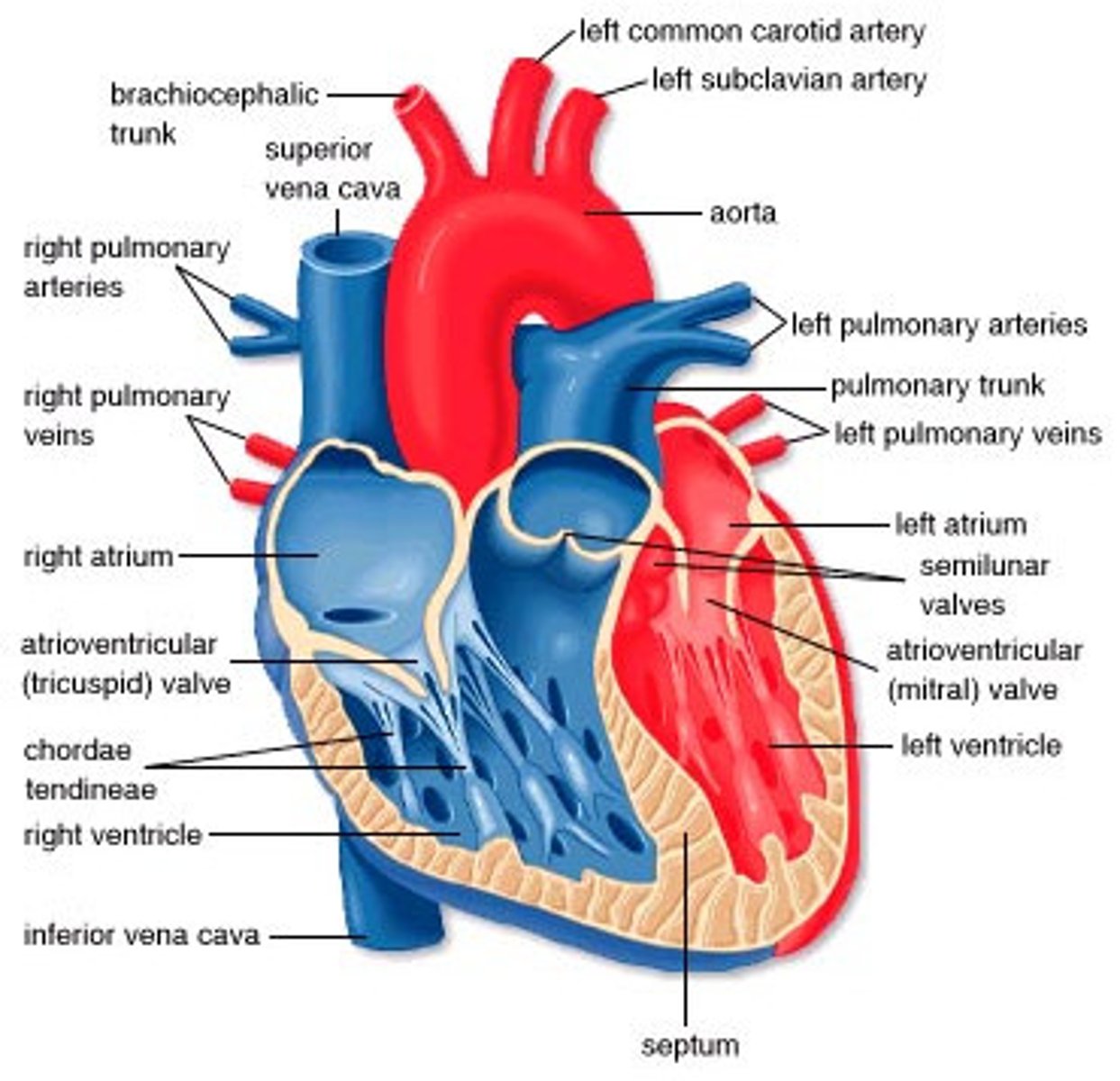
Anatomy of the Heart