Psychological Interventions Lecture 6
1/13
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
14 Terms
Definition of Schema Therapy
Schematherapy is a form of psychotherapy that helps you understand the origins of behavioral patterns and change them.
The influence of childhood experiences on your behavioral patterns and daily life is explored.
You learn to change yourself in such a way that you feel better and can take better care of yourself and stand up for yourself.
You learn to feel what your needs are, and you learn to stand up for them in a healthier way.
This changes not only your behavior, but also your thoughts and feelings.
Development of Schema Therapy
1990s: Jeffrey Young & colleagues
Complex problems
CBT+
Integrative psychotherapy combining: Attachment theory, cognitive, behavioral, Gestallttherapy, Transactional Analyses, psychodynamic psychotherapy and psychodrama
Core Concepts
Schemas: Ingrained patterns from early experiences that in fluence behaviours and emotions
Schema Modes: Different emotional states that reflect schema-based responses (temporarily expressions of activated schemas and coping)
Emotion Regulation: ST helps manage emotional responses to reduce maladaptive coping
Coping styles: Adaptive or maladaptive ways individuals handle schema-based distress
Goals of Schema Therapy
Addressing Negative Patterns: One of the main goals of ST is to identify and change maladaptive schemas that develop from early life experiences. These schemas lead to negative thought patterns and behaviors that contribute to emotional distress.
Promoting Healthier Thinking: ST encourages clients to replace dysfunctional beliefs with healthier cognitive patterns. This cognitive restructuring helps clients develop a more adaptive worldview and improves their self-perception.
Enhancing Emotional Regulation: ST aims to improve clients’ ability to manage their emotions, including addiction triggers, effectively. By recognizing and processing emotions related to their schemas, individuals express feelings more healthily.
Fulfilling Emotional Needs: A significant goal of ST is to help clients identify and meet their unmet emotional needs. This includes understanding how early experiences shaped their current emotional landscape and finding ways to address those needs in their adult lives.
Improving Relationships: ST seeks to foster healthier interpersonal relationships by addressing the underlying issues rooted in maladaptive schemas. Clients learn to communicate more effectively and form more stable, fulfilling connections with others.
For whom is Schema Therapy?
People with a personality disorder diagnosis (DSM-5)
Longer existing, recurrent symptoms/clinical syndromes that were (unsuccessfully) treated before
Requirements:
Some insight into the emergence of negative behavioral patterns / problems
Sufficient insight into one's own emotions, ability to mentalize and tolerate emotional distress
Clinical syndrome is treated first or does not interfere
Long-term commitment (1 to 3 years) which does not suit individuals seeking quick results.
Schema therapy in practice
18 schemas over 5 schema domains related to unmet needs
Disconnection/Rejection
Impaired autonomy and/or Performance
Impaired Limits (e.g. cross other people’s boundaries, maybe because of impaired self-control)
Other-Directedness
Overvigilance/Inhibition (e.g. do not show any form of emotion)
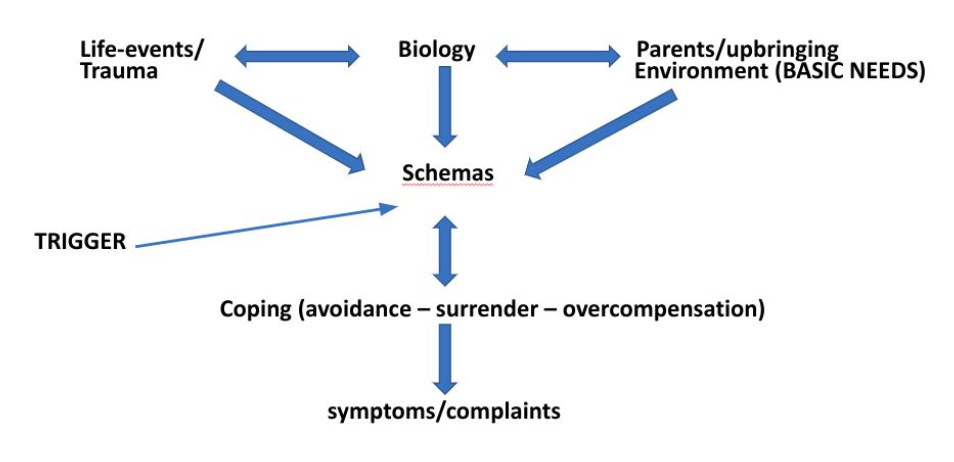
Bio-psycho-social model: Development of schemas and symptoms/complaints
Life-events/trauma, biology and parents/upbringing environment (basic needs) interact and form schemas
Outside trigger evokes coping reaction based on schemas (avoidance, surrender, overcompensation)
These reactions lead to symptoms and complaints
Schema Modes (emotional states)
Healthy adult (desired outcome)
Dysfunctional coping modes: reaction to triggers
Detached protector
Compliant surrender
Over-compensator
Dysfunctional parent mode: negative things they think about themselves (often based on parents, teachers and peers)
Punitive parent
Demanding parent
Child modes
Happy child
Angry child
Vulnerable child
Impulsive/undisciplined child
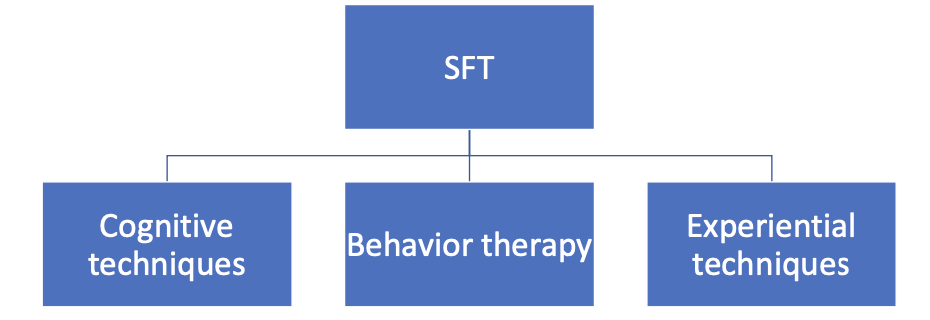
Schema therapy intervention
Cognitive techniques (e.g., holistic theory, socratic dialogue, challenging cognitions)
Behavior therapy (e.g., behavior activation, exposure)
Experiential techniques (Imagery rescripting, chair work, roll play)
Limited reparenting (e.g., empathic confrontation)
Schema therapy: Research
Ongoing studies in the Netherlands:
BOOTS Borderline Optimal Treatment Selection: ST vs DBT (Dialectcal Behavior Therapy) in patients with BPD (C. Wibbelink, A. Arntz en J-H Kamphuis)
Schema therapy for patiënts with ASD (Autism Spectrum Disorder) (Richard Vuijk)
SMI-3: development of a new comprehensive schema mode inventory (M. Rijkeboer & Lobbestael)
SFT for DID (Dissociative Identity Disorder) (R. Huntjens & M. Rijkeboer)
SFT for adolescents with behavioral problems in residential youth institutions (M. van Wijk-Herbrink)
FORCE project (NPI): SFT vs psychodynamic treatments, both individual and group, for people with cluster C personality disorders (M. Daniels & B. van den Heuvel)
The BOOTS study
Which treatment is most effective for BPD?
Schema therapy (ST) or DBT
What we know:
Both DBT and ST can be effective for BPD, but... Often low quality research (Sempertegui et al., 2013; Storebro et al., 2020)
In 1/3 of clients with BPD no reduction in severity of BPD complaints after treatment with ST or DBT (Woodbridge et al., 2021; Meuldijk et al., 2017)
High dropout rates (up to 30% with both treatments) (Giesen-Bloo et al., 2016; Gülu, 2018)
So the question is: “What treatment, by whom, is most effective for this individual with that specific problem, under which set of circumstances?”
ST for Autism Spectrum Disorder (ASD)
Scoping review from Vuijk et al. (2023)* highlights:
Increasing interest in ST for adults with ASD within both clinical practice and research
However, the available research remains limited
Studies on ST in adults with ASD have predominantly utilized case series designs and uncontrolled trials with small sample sizes.
Oshima et al. (2015): three EMSs appeared to be particularly significant in adults with ASD:
Insufficient Self-Control; Emotional Deprivation; Vulnerability to Harm and Illness
Developments
International workgroup (Arntz, Rijkeboer et al., 2021)
From clinical view → more empirical research needed (mediation effects coherence & cross-cultural validation)
General conclusion & proposals for future research:
Add 3 new schemas (Lack of a Coherent Identity, Lack of a Meaningful World, and Unfairness)
Validate the new Schema Mode Inventory (SMI) cross-culturally
Study non-verbal techniques (psychomotor therapy, art therapy and drama therapy)
Conclusion
The main goal of schema focused therapy (SFT) is to help people to recognize schemas and break through their unhealthy patterns of thinking, feeling and behaving
Not all people develop (disfunctional) schemas. Only if basic childhood needs are not met, people suffer from traumatic experiences or life events and are biologically prone to do so.
The therapist - client relationship is an important part of therapy and mechanisms of change.
SFT mostly investigated (and found effective) for personality disorders (particularly BPD). SFT for BPD is most effective when individual and group therapy are combined.