ceutics elimination
1/99
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
100 Terms
elimination vs excretion
elimination: consists of both excretion and metabolism. compound may still be in body, just inactive
excretion: compound is COMPLETELY outside of the body (bile/feces, lungs, kidney/urine)
t/f: phase 2 of metabolism is more dominant, faster, and abundant
false. phase 1
phase 1 vs phase 2 metabolism
phase 1: oxidation, reduction, hydrolysis
phase 2: conjugation; neutralize free radicals
t/f: metabolism can occur in the liver, kidneys, skin, lungs, blood and gut wall
true
excretory organs eliminate polar compounds more efficiently than lipophilic substances except for ___________
lungs (fats can become aerosolized and exhaled)
lipophilic drugs are ____(perfusion/permeability)___ limited, with a ______ half life and a _______ VD
perfusion; long half life; big VD
drugs are eliminated from the body either unchanged (aka _________) or as metabolites
parent compound (means it has not been metabolized)
what is the primary organ for removal of most drugs (especially water soluble)
kidney
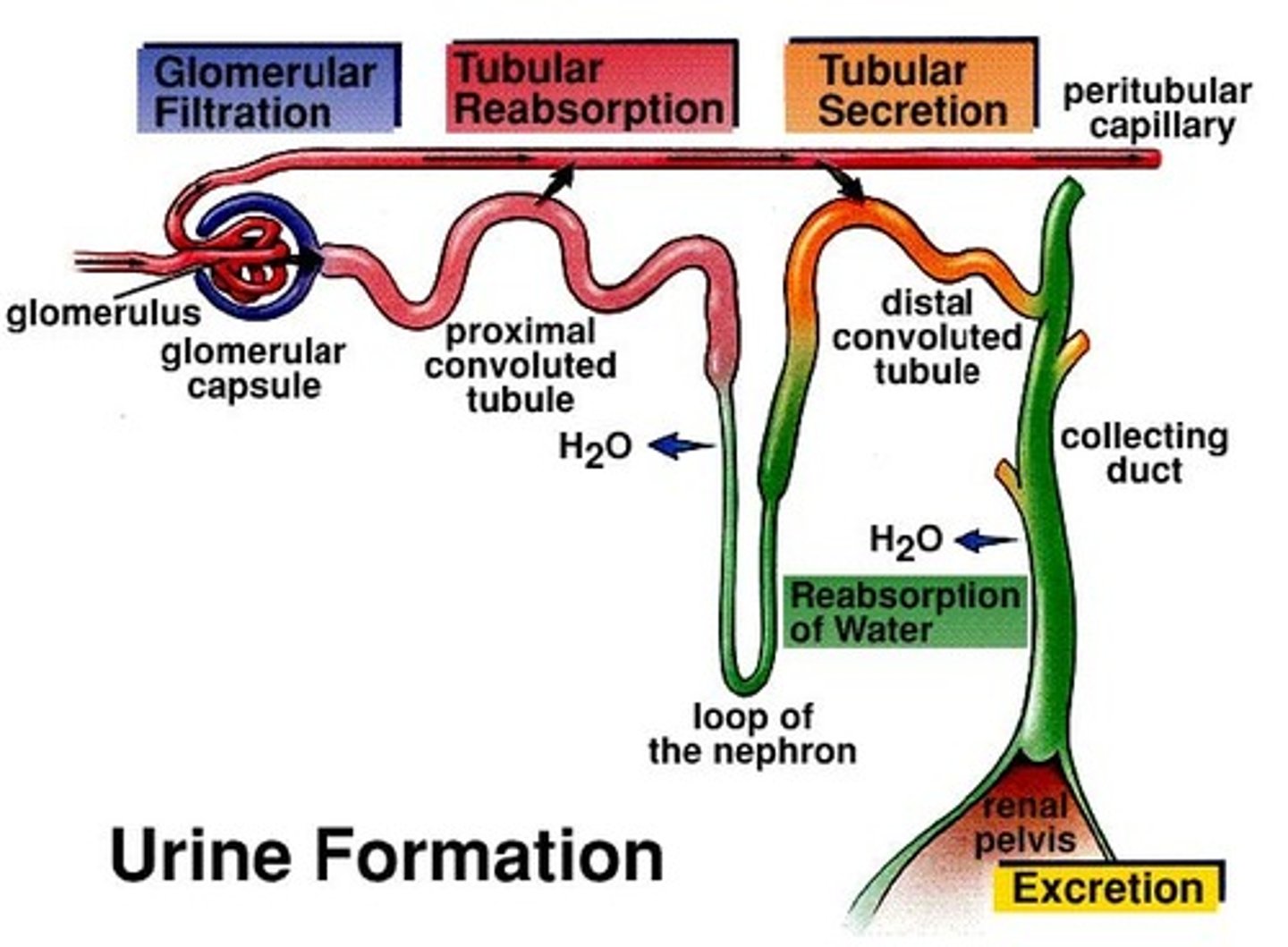
3 principle processes by which the kidney eliminates drugs
1. glomerular filtration
2. tubular secretion
3. tubular reabsorption (returning drug to blood)
most drug filtration occurs where in kidney
renal cortex
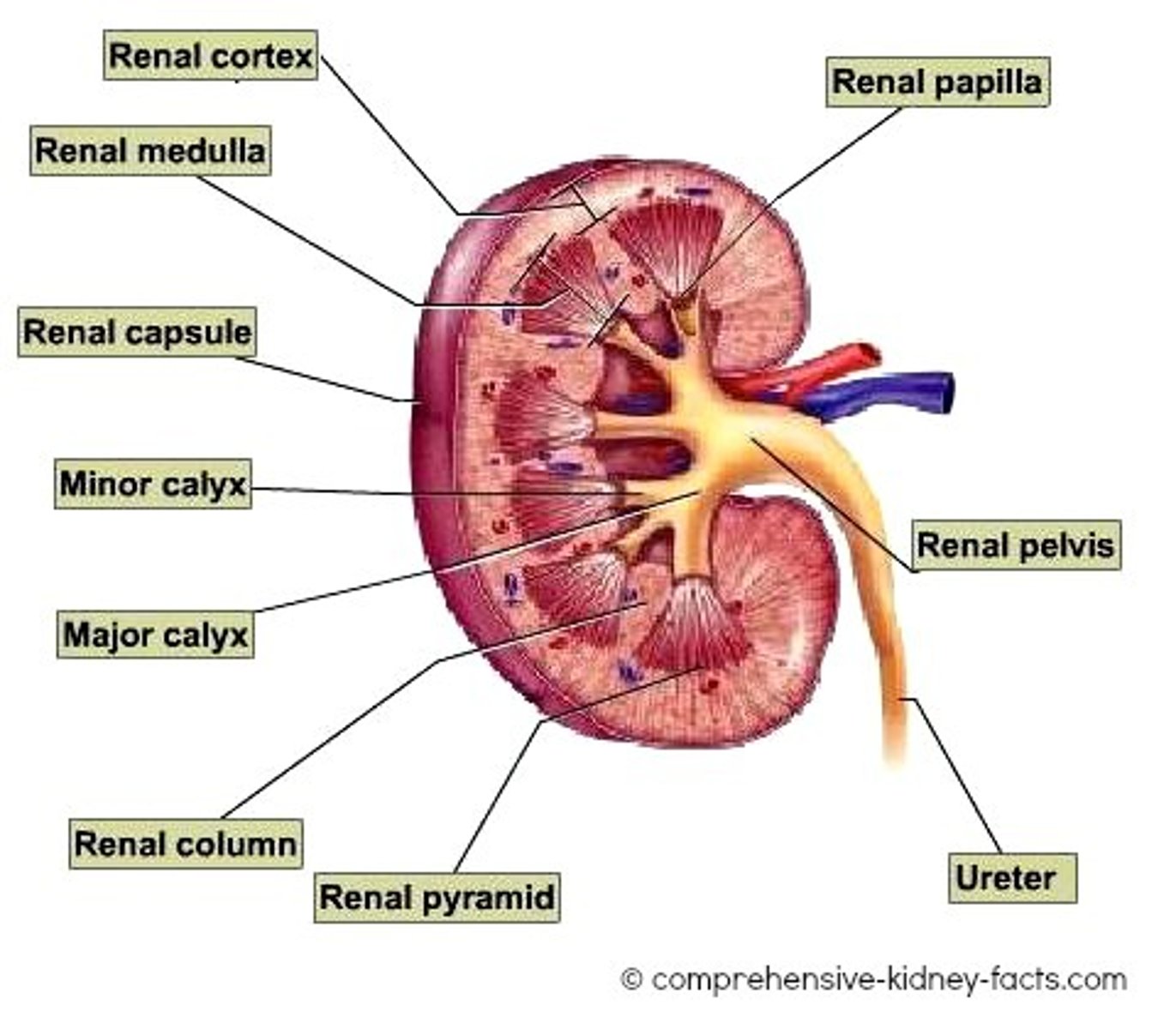
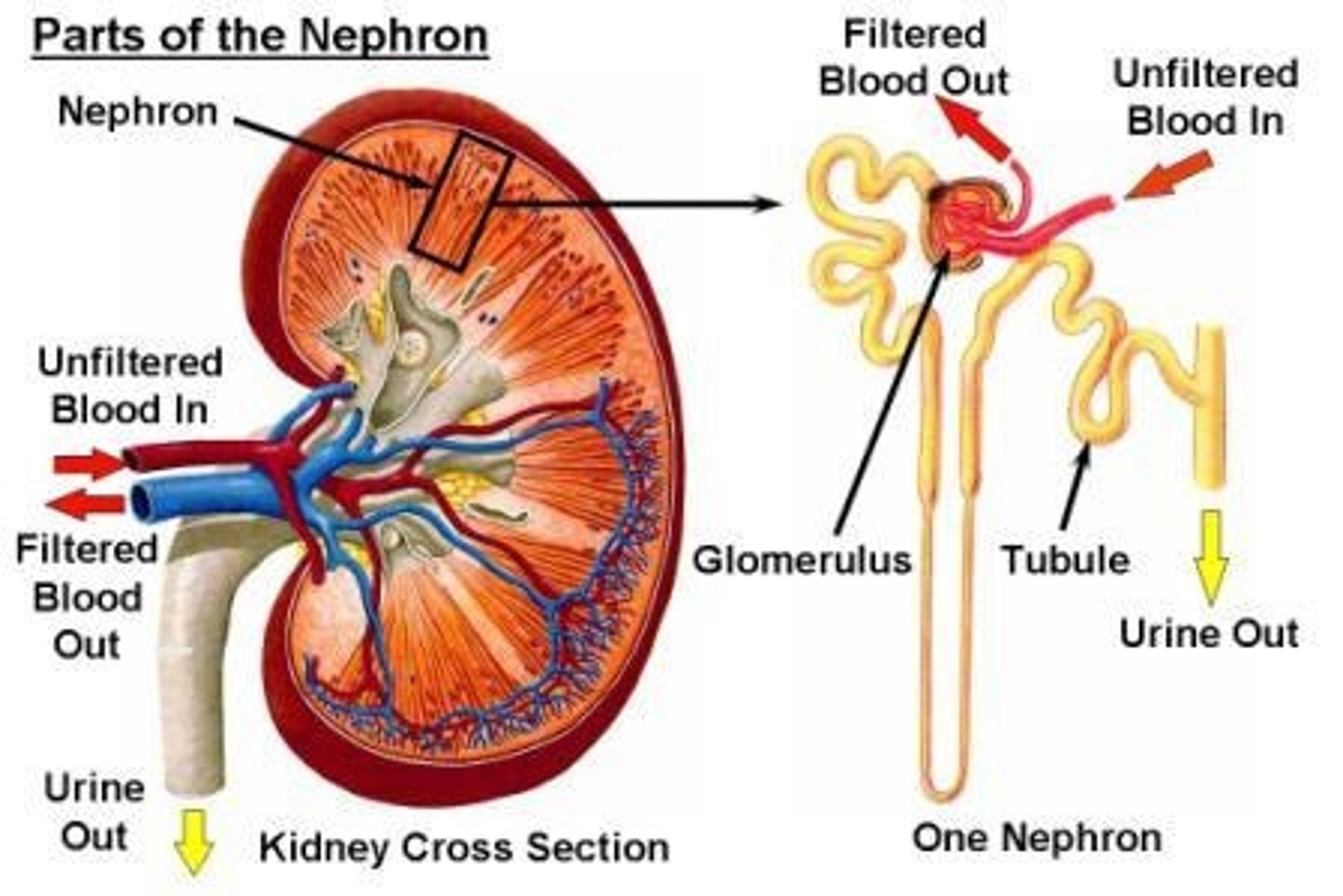
the nephron consists of
glomerulus and renal tubules (proximal and distal)
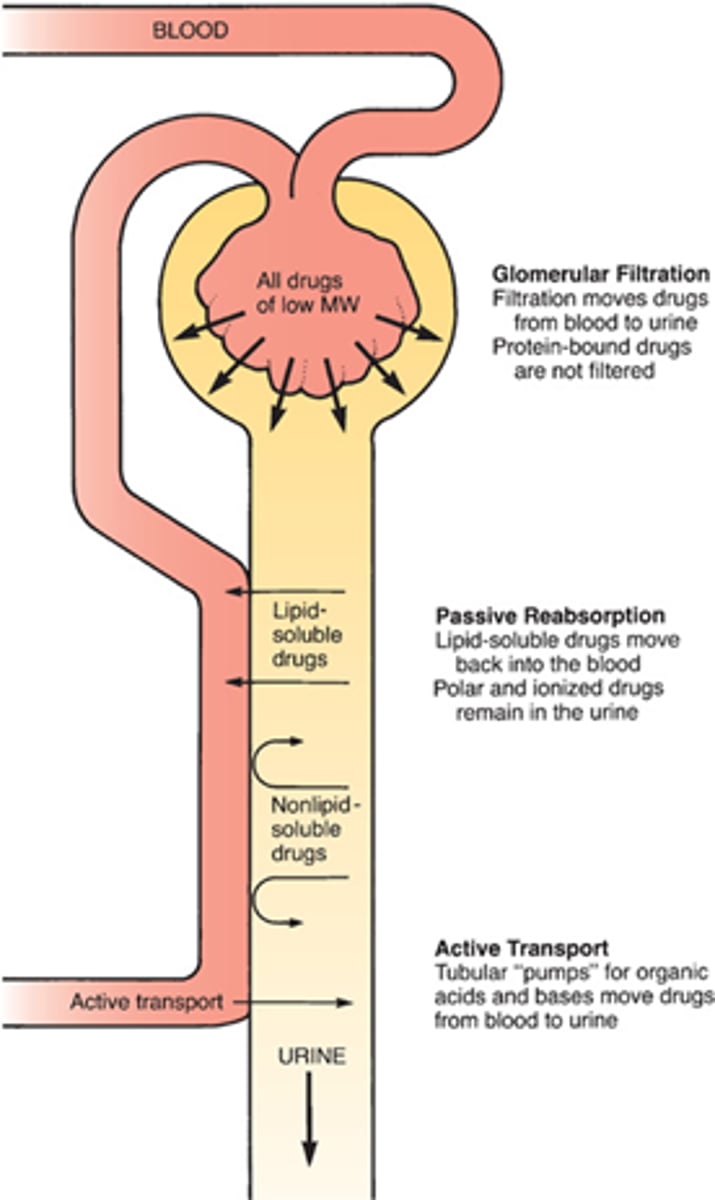
which drugs dont undergo glomerular filtration? what happens to them?
protein bound drugs. undergo carrier transport
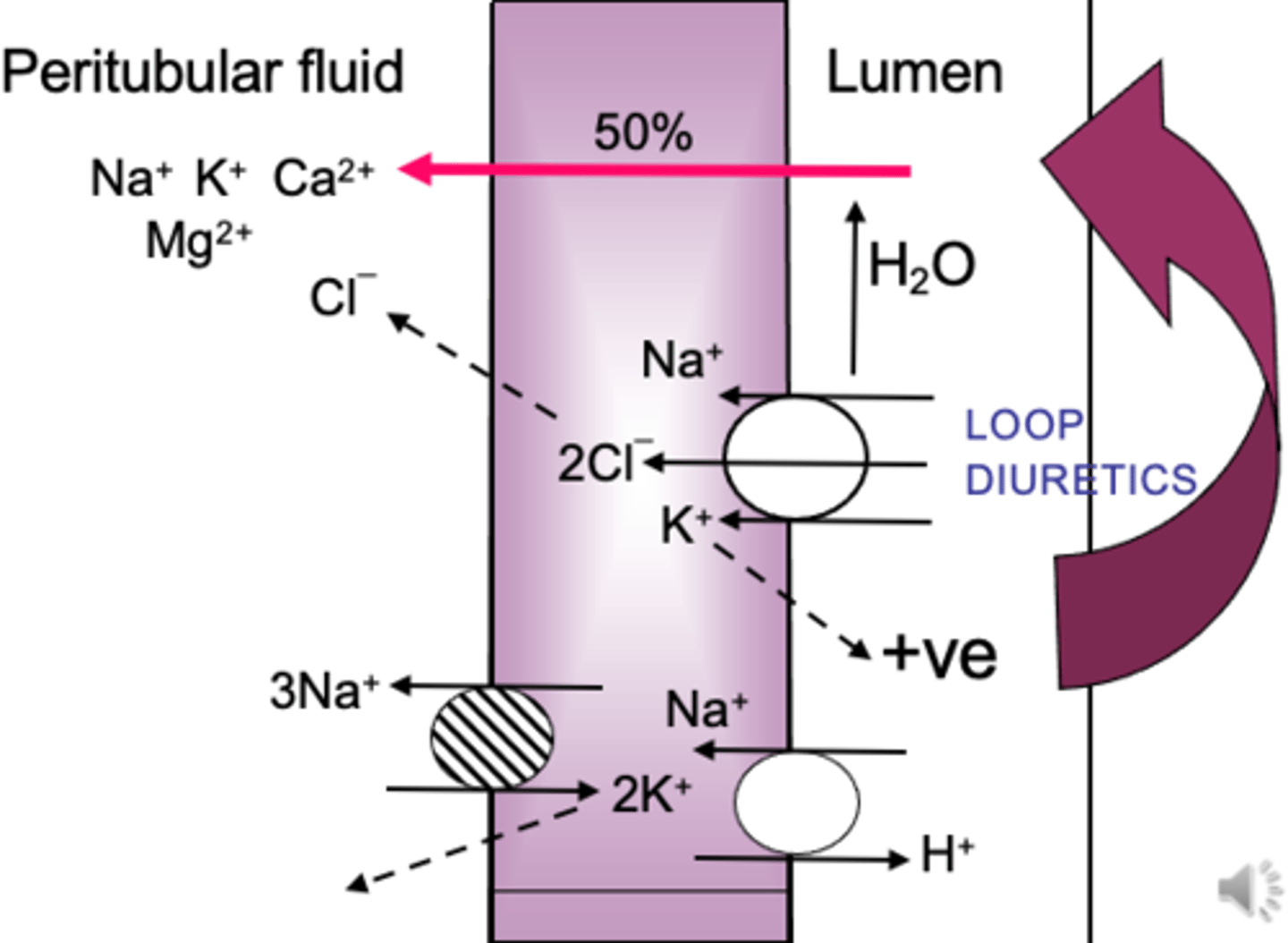
peritubular fluid
the interstitial fluid surrounding the renal tubule. 1st to make it into urine. aka ultrafiltrate
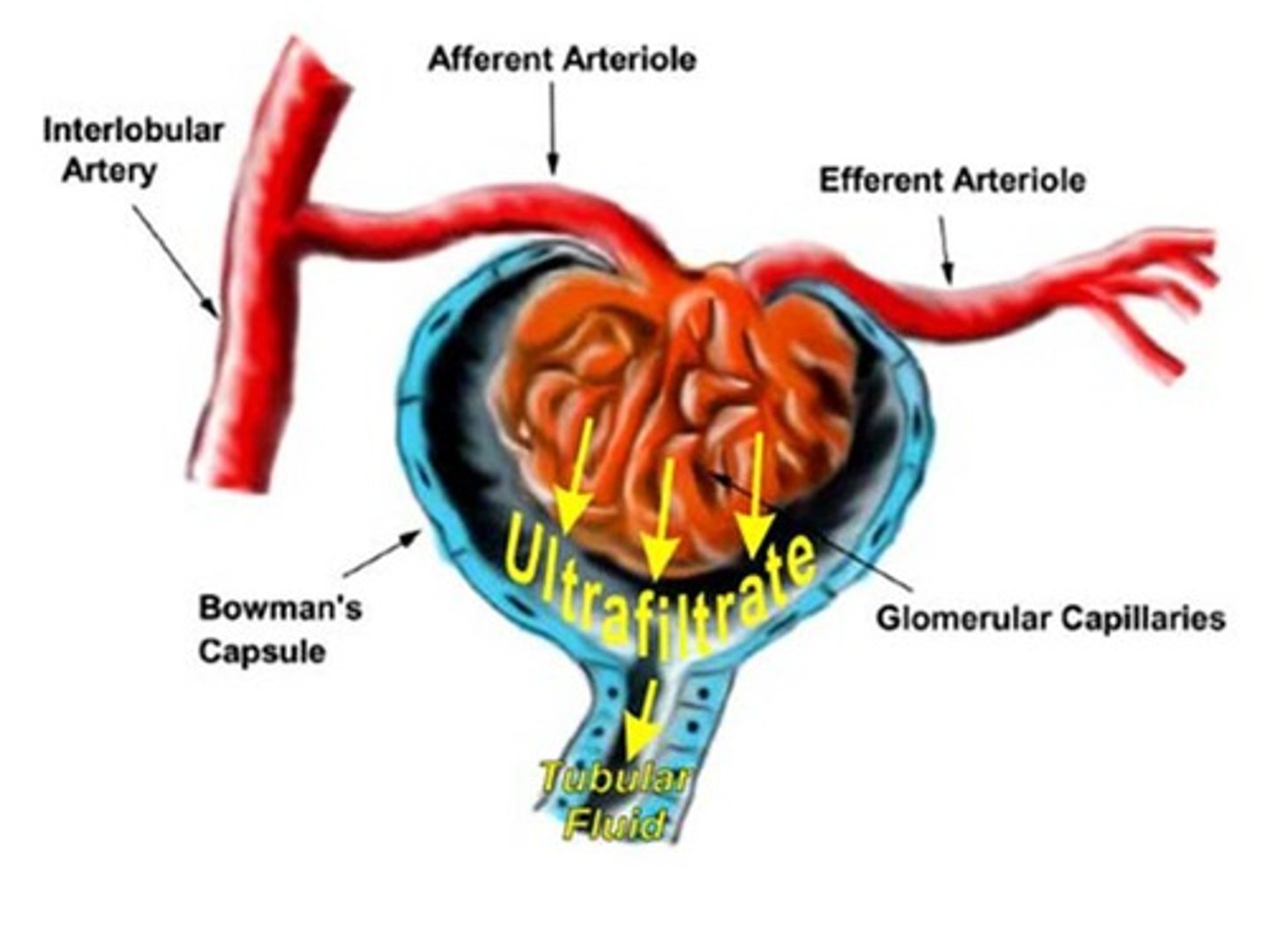
summarize the processes in the kidney & blood flow
1. blood w drug comes in through afferent arteriole
2. glomerular filtration (pressure bc afferent wider)
----> tubular reabsorption/secretion= urine formation
3. blood exits through efferent arteriole
4. blood enters venous side
which factors influence what the glomerulus filters out
1. large molecular size (too big= cant pass)
2. charge (static cling)
3. shape (bulky)
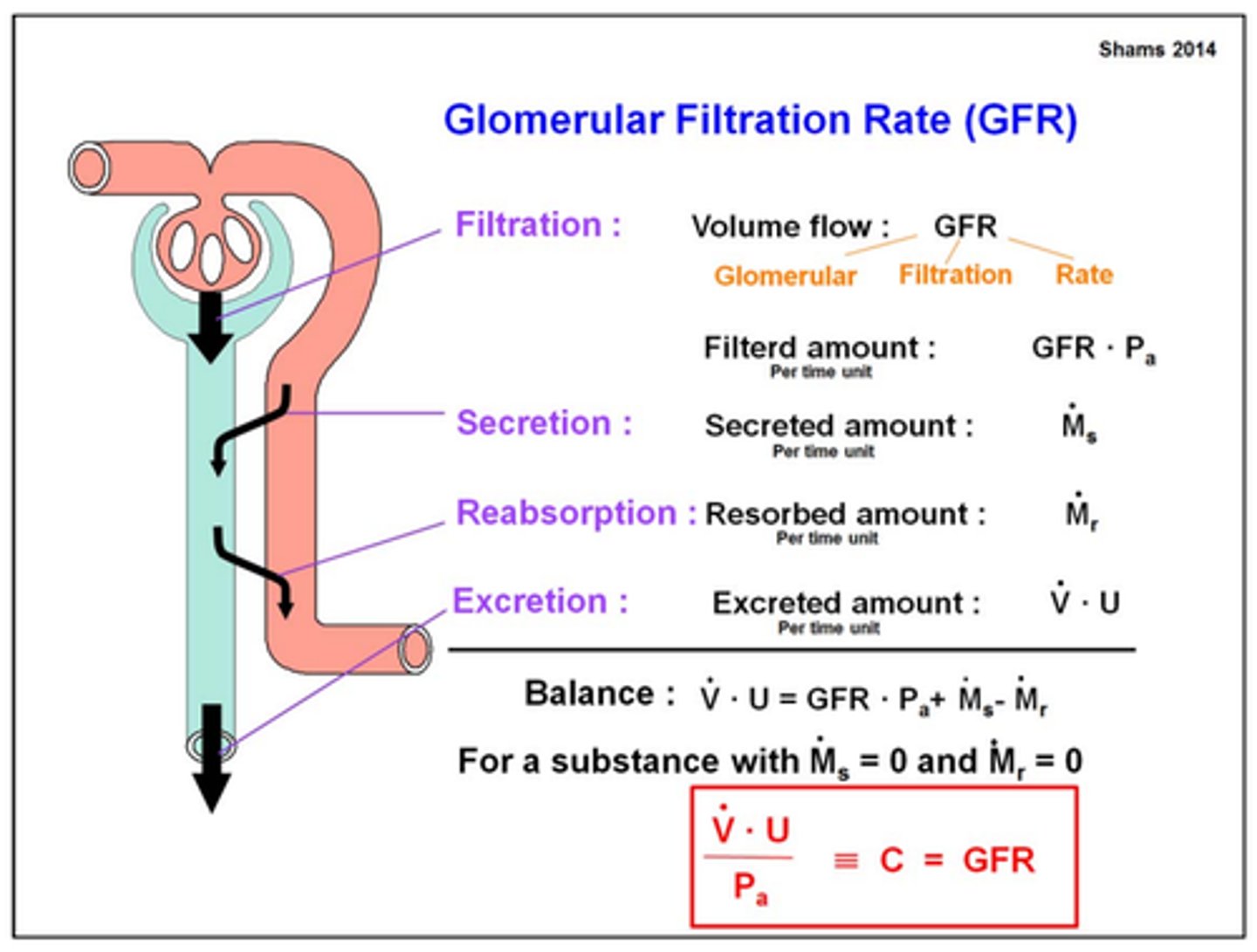
GFR
glomerular filtration rate
about 130ml/min
[190L per day]
why is GFR not always drastically impacted if one of our kidneys is removed
other kidney undergoes hypertrophy/hyperplasia and picks up the slack
ultrafiltrate
aka peritubular fluid-> fluid around tubules that is the first to potentially make it into urine
fluid that enters the glomerular capsule
how does low CO affect GFR and xenobiotic clearance
renal artery is getting less blood-> lower GFR and less clearance
relate charged compounds to glomerular filtration
-charged things get filtered out slower bc of static cling(+/-) or repulsion (-/-) [glomerulus is negatively charged]
- neutral compounds filtered out quickly
how will glomerular inflammation affect glomerular filtration
decreased GFR: if there is swelling, makes it more difficult to cross glomerulus= longer half life
(BUT hyperfiltration== we are losing plasma proteins== shorter half life of bound drugs)
will a pt with lupus and glomerular nephritis have a lower or higher half life for drugs
slower GFR= longer half life of drugs undergoing filtration
hypersecretion of plasma proteins= shorter half life
factors influencing GFR
1. inflammation (loss of static cling, increased permeability, OR swelling/lower)
2. drug-plasma protein binding (too big= wont pass)
3. percentage of total body water (less water= less blood cleared)
4. CO, volume, rate
how does the concept of passive diffusion affect urine formation
movement of drugs is favored from tubular lumen to blood
-tubular fluid is concentrated with drug molecules, passive diffusion forces it back into blood
[this is prevented by urine pH/ion trapping]
where does passive back-diffusion of drugs back into blood occur
distal tubules and collecting ducts (where urine is acidified)
how does an acidic urine affect reabsorption and elimination of weak acids and weak bases
- acidic urine increases reabsorption/decreases elimination of weak acids (salicylates)
-and decreases reabsorption/increases elimination of weak bases [since they get ion trapped]
t/f: we must make urine more acidic if we want to eliminate weak acids
false. must be more basic so that they get ion trapped. otherwise they will diffuse back into blood
what would you administer in a weak acid overdose to promote urinary excretion
bicarbonate
(give base to promote ion trapping and stop diffusion back into blood)
what would you administer in a weak base overdose to promote urinary excretion
NH4Cl
(give acid to promote ion trapping and stop diffusion back into blood)
2 types of active tubular secretion
1. organic anion secretion
2. organic cation secretion
-> actively move drugs from the blood and into luminal fluid
protein bound drugs most often undergo _____________ to end up in urine
a. glomerular filtration
b. active tubular secretion
c. tubular reabsorption
b. active tubular secretion
t/f: competition kinetics is often exhibited in active tubular secretion and most often results in an increased rate of excretion for each substance
false. decreased rate of excretion
which 3 factors may affect active tubular secretion of a drug and their rate of excretion
1. competition(lowers rate)
2. saturation (lowers rate)
3. affinity (higher affinity= shorter half life)
-> both w other drugs and endogenous compounds
in active tubular secretion, the drug with the highest affinity will have the _______ half life
shortest (eliminated first)
active tubular secretion
active transport systems that move mostly protein bound drugs (take off of the protein) from the blood and into the urine
in active tubular secretion, a carrier protein that is saturated will have a ________ rate of elimination
a. faster
b. shorter
c. constant
c. constant
how are charged anions and cations often eliminated
they are usually bound to plasma proteins and eliminated via active tubular secretion
when would a protein bound drug potentially undergo glomerular filtration
if equilibrium btwn protein bound and unbound shifts, then the FREE drug may potentially undergo glomerular filtration (but usually active tubular secretion)
compounds normally eliminated by tubular secretion will be excreted ____(slower or faster)____ in the very young and old
slower bc either not fully developed in neonate or damaged/scarred/polypharmacy in elderly. elderly also have lower CO
some substances filtered into the luminal fluid at the glomerulus are reabsorbed via active transport found in ____________
proximal tubules
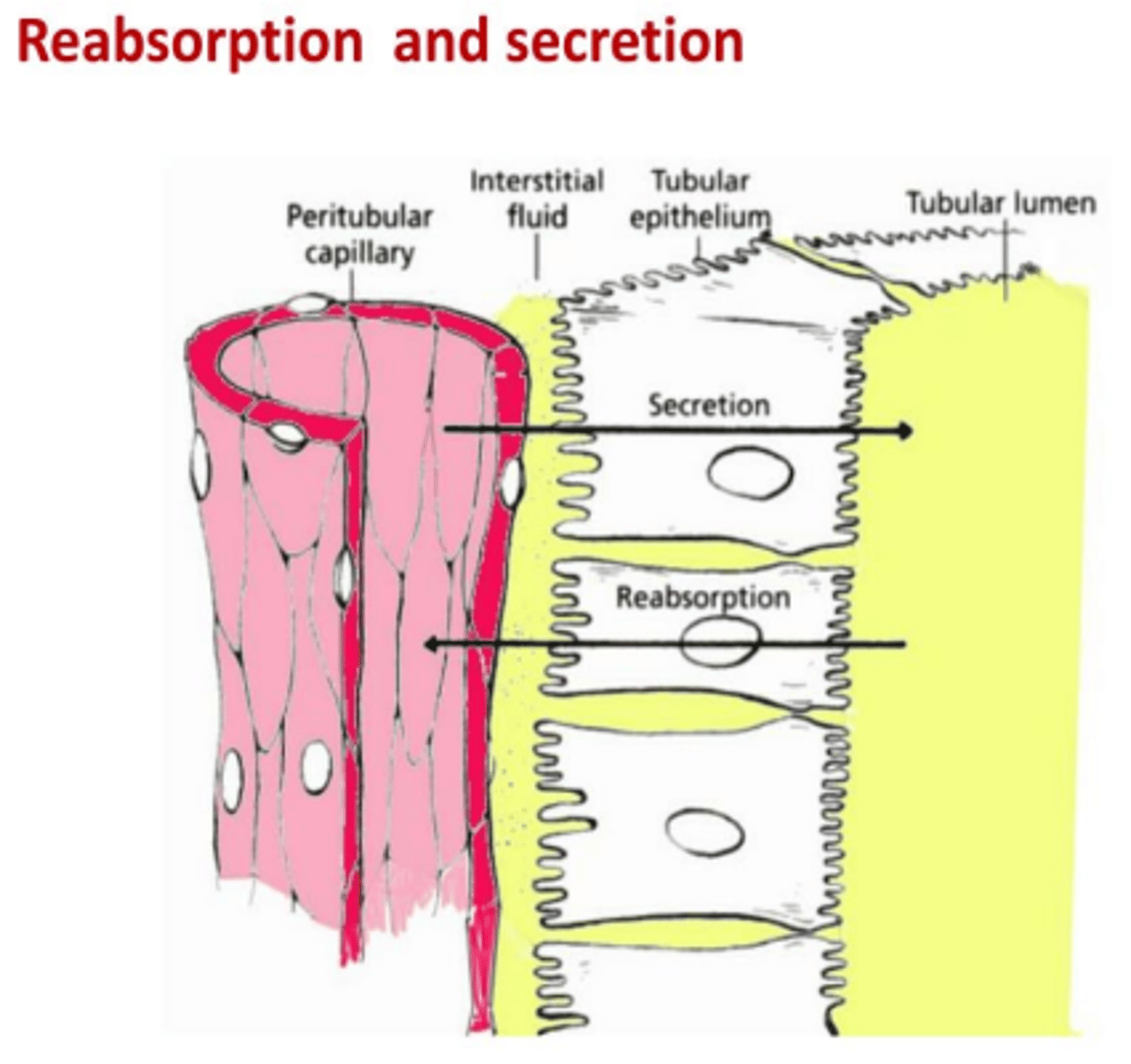
by which mechanism do endogenous substances (glucose, amino acids) stay in the body rather than undergoing excretion? why?
active tubular reabsorption (transporters)
[NOT VIA DIFFUSION BACK bc of ion trapping]
drug X undergoes a lot of reabsorption (back into blood). what will the effect be on the half life? curve?
increased half life
shifts elimination upwards (less neg slope) with no effect on absorption
t/f: both drugs that undergo glomerular filtration or active tubular secretion may undergo active tubular reabsorption
true
how does the volume of distribution of a drug affect renal excretion
large Vd= drug is in tissue= lower rate of elimination
small Vd= mostly in vasc compartment = higher rate of elimination
drug A has a Vd of 2L. drug B has a Vd of 200L. which one will have a higher rate of elimination
drug A bc small Vd= confined to vasc compartment= blood will pass through kidney and drug will be eliminated
how does the degree of protein binding affect renal excretion?
more protein bound= _____ elimination rate
more protein bound drug will have longer elimination rate
how does a faster GFR affect clearnace
higher clearance
extent of back diffusion of the un-ionized form is usually minimal because? which drugs may potentially undergo diffusion back into blood?
-most drugs are weak bases and acidic urine ion traps them
- an acidic drug may undergo diffusion since the urine is acidic as well
if genetic variations resulted in poor functioning transport proteins, how will this affect active tubular secretion and half life
less active tubular secretions means more of the drug stays in the blood= longer half life
renal active tubular reabsorption will be the opposite of which process in absorption of drugs?
p-glycoprotein
in absorption, pgp prevents absorption
when do we have to worry about metabolite elimination
if the drug is a prodrug. increased metabolite elimination will decrease half life
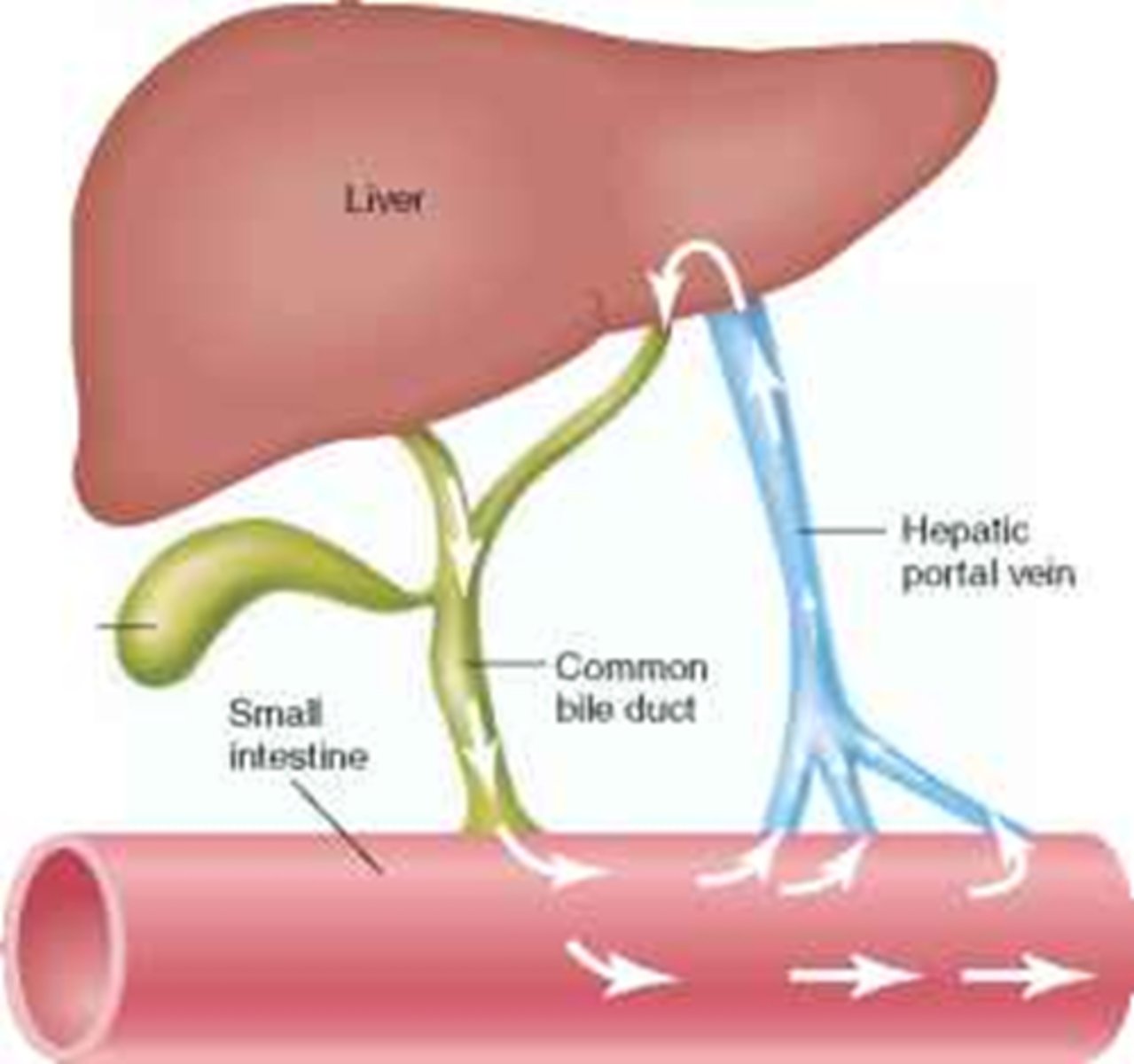
where is bile made? where does it go?
made in liver (hepatocytes), transported via common bile duct and stored in gallbladder; released into jejunum
[ if theres no gallbladder, then theres just a more constant flow of bile]
![<p>made in liver (hepatocytes), transported via common bile duct and stored in gallbladder; released into jejunum</p><p>[ if theres no gallbladder, then theres just a more constant flow of bile]</p>](https://knowt-user-attachments.s3.amazonaws.com/e93f5683-18b3-4e83-bb61-044aa59b0529.png)
t/f: biliary excretion is a major route of elimination, with most drugs being excreted via the bile
false. only a small amount of drugs reach bile by diffusion
but biliary excretion DOES have a major role in drug removal for some anions, cations, and cardiac glycosides
once drugs are inside the bile, why dont they diffuse/recycle back into blood?
1. too highly charged to back-diffuse across epithelium
(remember most of these drugs are cations/anions/cardiac glycosides)
2. most of these are conjugated
3. gallbladder has specialized epithelium
where can drugs in the bile be secreted next? what happens to them?
bile-> small intestine-> feces-> excretion (for unabsorbed xen
bile-> small intestine-> enterohepatic recycling
are xenobiotics that undergo biliary excretion absorbed
yes. they are absorbed and reach hepatocytes, then enter bile
what is enterohepatic recycling? when does it stop?/
drug in small intestine is absorbed, enters liver, then bile, then transported back to SI where it is reabsorbed back into blood (cycles)
cycle will stop when drug is metabolized (ex: more water soluble) or excreted by kidney or both
enterohepatic recycling is important in conserving which endogenous substances
vitamin D3 and B12
folic acid
estrogens
enterohepatic recycling ____________ the half life of drugs
increases
describe the pathway a drug that undergoes enterohepatic recycling travels
1. enters liver where it is conjugated and put into bile-> gallbladder
2. gallbladders shoots bile into small intestine
3. in small intestine, drug is cleaved by glucuronidases and reabsorbed into blood
----> may go to target, renal excretion, or enterohepatic recycling
4. drugs that are not cleaved undergo fecal excretion
what are drugs that undergo hepatic recycling cleaved by in the SI once they have been conjugated in liver
bacterial beta-glucuronidases
describe that characteristics of a drug that is fecally excreted
- unabsorbed orally ingested drugs
- metabolites excreted into bile and NOT reabsorbed
breast milk is more ________ than plasma, thus ______ compounds tend to accumulate
(basic or acidic?)
breast milk is acidic
basic compounds accumulate
(ex: morphine, codeine)
which kinds of drugs accumulate in breast milk
- basic
- lipid soluble
- non electrolytes
- abx (tetracyclines bc high calcium)
which of the following will accumulate in breast milk (select all that apply)
a. acidic drug
b. basic drug
c. strong electrolyte
d. non electrolyte
e. tetracycline
f. penicillin
b. basic drug (milk is acidic)
d. non electrolyte
e. tetracycline (bc calcium)
which drugs are eliminated by the lungs
substances in gas phase (ex: nitrous oxide, Co2)
which route of drug excretion allows us to see the drug 3-4 months later
hair, nails
t/f: ocular fluid is a long term ultrafiltrate of plasma
true
first order kinetics
rate is directly PROPORTIONAL to substrate concentration (not just a constant rate like zero order)
elimination rate constant (K)=
K= mass of drug x elim rate
calculate the elimination rate constant (K) if
rate of elimination= 1mg/h
mass= 50mg
rate = mass x K
1mg/hr = (50mg) x K
K = 1/50 h^/1
remember unit conversions!!! this is in hours. check if he wants diff units
if the rate constant is 0.02h^-, how would you convert it into days?
24 hours in a day so
0.02 x 24hrs= 0.48 day^-1
t/f: the rate at which a drug disappears from the body is a fxn of both its rate of metabolism and its rate of excretion
true
define half life
time it takes to reduce the drug concentration by 1/2 in a particular body component (ex: plasma)
-> allows us to compare rate of elimination for several drugs
t/f: half-life is dependant on initial concentration
false. half life is independent on initial concentration. it is an intrinsic property
in a concentration-time graph, how do you know what the half life is?
it is the slope. that is why it does not depend on initial concentration bc regardless of initial dose, the slope will be the same
t/f: the half life is the same for a drug regardless if it was administered at 1x, 10x, or 100x
true (slope is the same, which is indicative of half life)
t/f: 500mg of drug A will remain in the bloodstream longer than 50mg of the drug
false. half life is an intrinsic property so it will take the same amount of TIME to decrease by half [but you may have more drug MOLECULES in the body]
t/f: there is a direct relationship btwn K and half life
false. inverse
K= 0.693/ half life
relationship btwn K and half life
K= 0.693/ half life
if t=6.93hrs, calculate K
K= 0.693/t
t= 0.10 h^-1
what is the extraction ratio a measure of? what would 1 mean? 0.5?
-A measure of how much drug is delivered to a clearing organ vs how much is removed by that organ
-ER of 1.0 means that 100% of the drug delivered to the clearing organ is removed
-ER of 0.5 means that 50% of the drug delivered to the clearing organ is removed
what is the "organ" that is usually used for the extraction ratio
liver
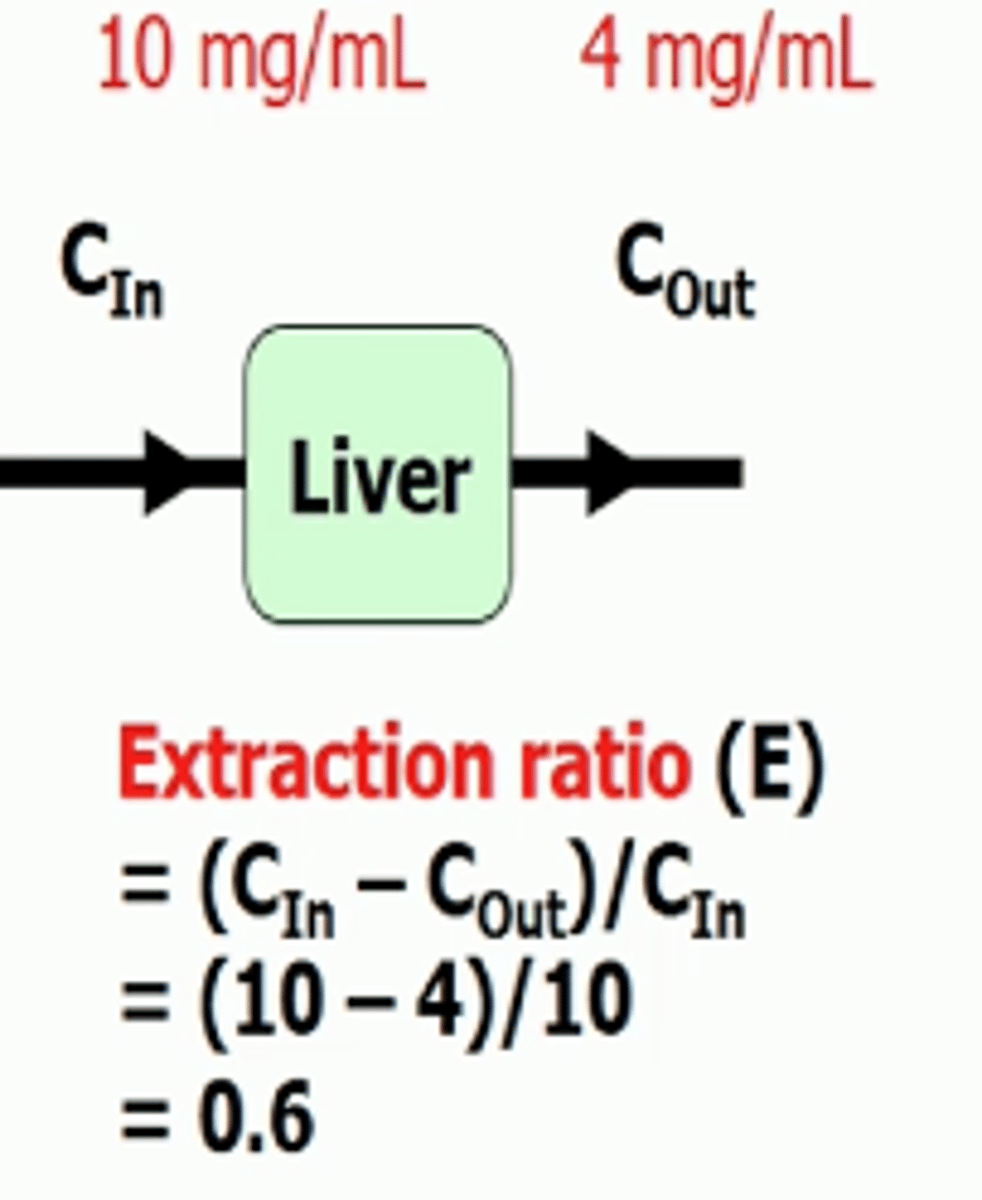
extraction ratio equation
Cin-Cout/Cin
so if 10mg enters liver and only 4mg comes out then
E= (10-4)/10-> 60% of drug was extracted
interpret what an extraction ratio of 80% means
80% of the drug was extracted by the tissue
for the extraction ratio, is Cin absorbed or non-absorbed drug?
absorbed. its the concentration in the blood stream
what is the definition of clearance (CL)
volume of blood cleared per unit time
if the extraction ratio=1.0 and Q=2L/min, what can you tell about clearance?
extraction ratio= 1.0 means that all of the blood is cleared of the drug
Q= blood flow= 2L/min
this means that clearance is 2L/min or 2L of blood are completely cleared of the drug every minute
what does Q mean
blood flow
if the extraction ratio=0.5 and Q=2L/min, what can you tell about clearance?
extraction ratio=0.5 means that only 50% of blood is cleared
Q=2L/min is blood flow
so every minute, 50% of the blood is cleared so that means 1L is completely cleared of drug every minute
clearance = 1L/min
clearance=
flow x extraction
Q x E
-relate elimination rate constant (K), CL, and V
-relate rate, Cl, C
K= CL/V
rate= CL x C
if volume=50L and 5 liters is cleared per hour, what is the elimination constant K
K= CL/V
K= 5/50= 0.1
what is the bioavailability of a 10mg IV bolus dose?
10mg. IV means it going straight to blood, so you get all 10mg
no absorption and no extraction
what is F
bioavailability constant
F= 1-E (amount of drug left over after extraction that is active)
if Cin= 10 and Cout=4
what is the extraction ratio?
bioavailability?
what do they mean?
E= (10-4)/10= 0.6 or 60% of drug loss by first pass metabolism
F= 1-E= 1-0.6= 0.4. 40% of drug is still left in blood and able to exert its action (bioavailability)
Qh= 1.6L/min
E=65%
V=280L
calculate Cl, K (in hours), and Max F
Cl= Q x E
K= Cl/V
F= 1-E
Cl= Q x E= (1.6L/min) x (0.65)= 1.04 L/min
K= (1.04L/min) / (280L) = 291.2 * 60mins = 0.22 h
[dont forget units!!]
F = 1-E = 1- 0.65 = 0.35
[formulas are given, except for extraction ratio?]
blood clearance vs plasma clearance
blood clearance= estimating extraction ratio
plasma clearance= most often investigated
-> depends on binding to plasma proteins and blood cell components
-> if a drug has high affinity for RBCs, after centrifugation you will NOT see it in the plasma vs CT curve bc it will be in the packed cell compartment [compare to drug that binds to plasma proteins]
total clearance=
rate of elimination =
C= renal clearance + hepatic clearance
RoE= rate of renal clearance + rate of hepatic metabolism
(dont forget to take in account both liver and kidney)
t/f: clearance is made up of both liver metabolism and physical excretion in the kidneys
true