Transplant 101 Module 1 Part 2B - Surgical Techniques
1/35
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
36 Terms
Deceased organ donation
Primary source of organs for transplantation
multi organ procurement often involving multiple teams from differnet programs working at a remote location
Neurologically deceased donor
Donation after brain death
DCD
Donation after cardiac death
Principles of organ procurement
identify and preserve import structures to allow reconstruction in the recipient
perfuse the organ through its vasculature with a preservation solution
Cool the organ
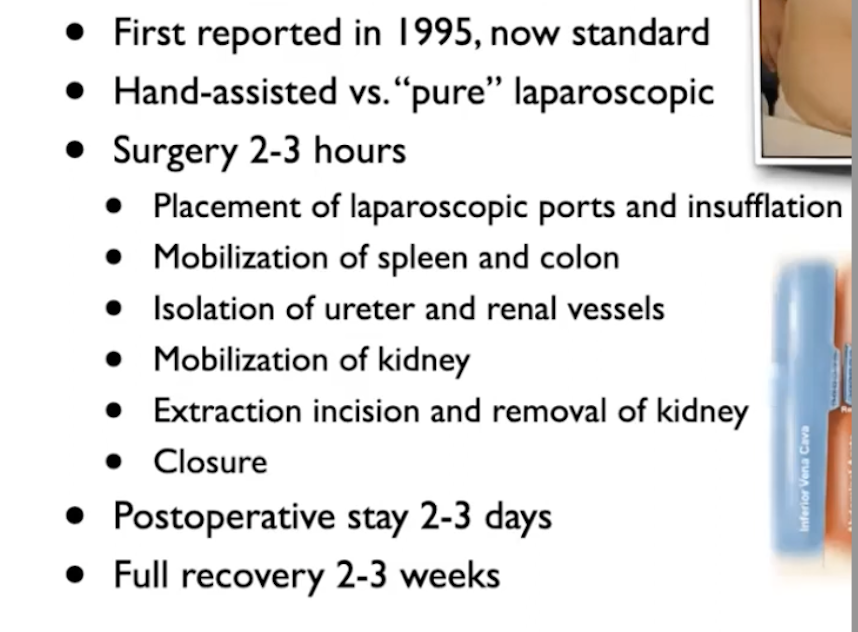
Laparoscopic donor nephrectomy
Incisions used for this kind of nephretomy become barely visible even 3 weeks post nephrectomy
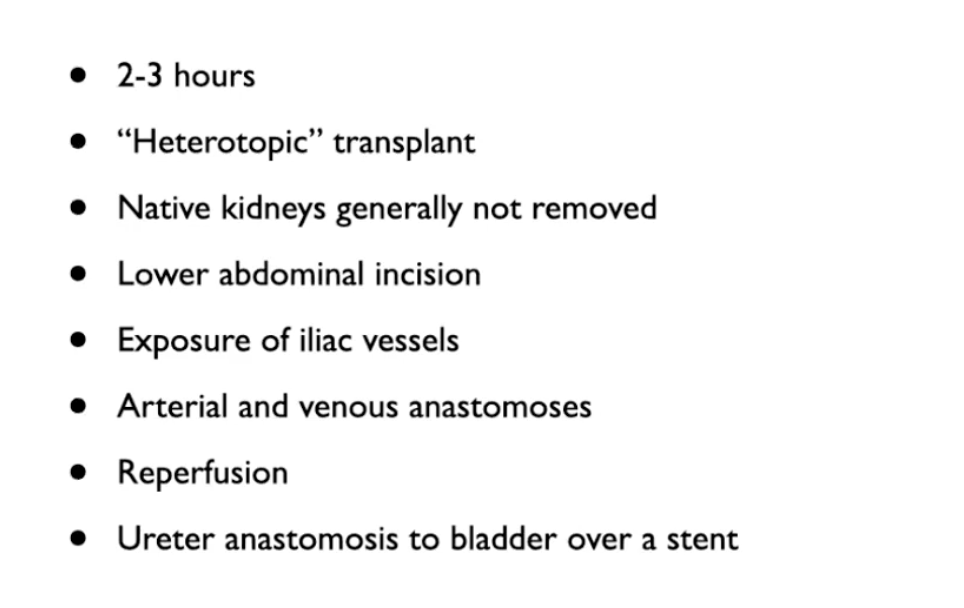
Kidney Transplant
Heterotopic - transplanted kidney is not placed in the same location as native kidney
Transplanted kidney placed in new space in lower abdomen
Right or left illiac fossa is exposed - illiac artery and vein usually externan ones - exposed and skeletonized
once vessels ready venous anastomoses is performed- connect venal vein to external illiac vein
renal artery connected to external illiac artery
repurfuse - release clamps on blood vesssel
Use a stent to connect ureter of transplanted kidney to bladder
External illiac artery
Artery that undergoes anastamoses to the renal artery in kidney transplant
External illiac vein
Vein that undergoes anastamoses to the renal vein in kidney transplant
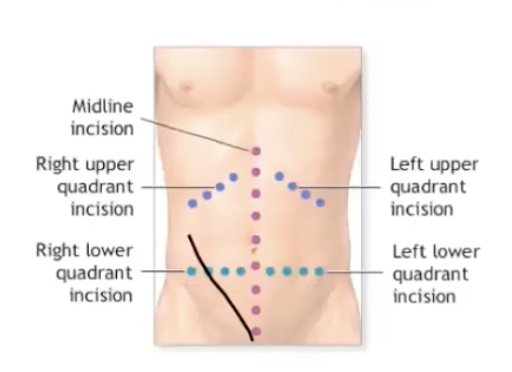
Typical incision for kidney transplant
Oblique incision in lower right quadrant
Heterotopic procedure
transplanted kidney is not placed in the same location as native kidney
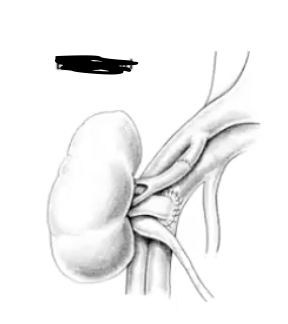
End to side anastamosis
most common anastamosis technique
connects illiac vessels to renal vessels
End to end anastamosis
less common anastamosis technique
connects illiac vessels to renal vessels
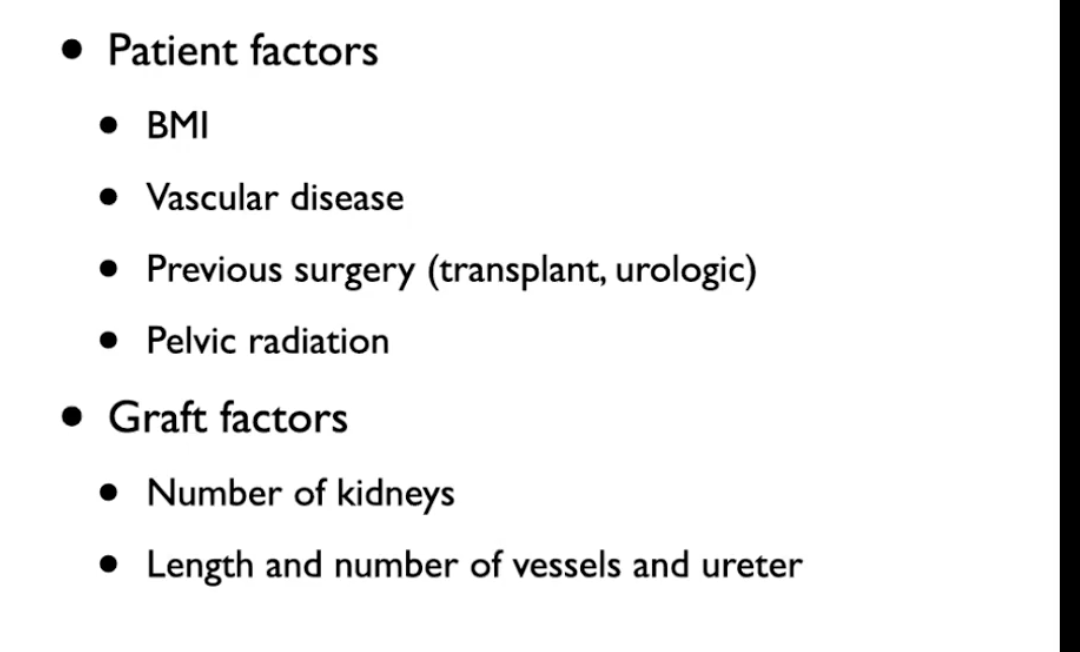
Factors that impact the intraoperative course
Vascular disease - ex. advanced atherosclerosis
Number of kidneys to implant
sometimes double kidney tranpslant is performed - lengthen procedure
More vessels and ureters - makes implantation more challenging
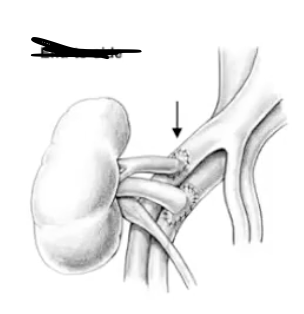
Anatomical variations in kidney transplant
Multiple vessels
ex. donor kidney has two arteries instead of one
two arteries are connected together in a backtable procedure before they are anastamized as one artery to the recipient
Multiple kidneys
double kidney transplant
implant both kidneys on both side or one on left side and one on the right
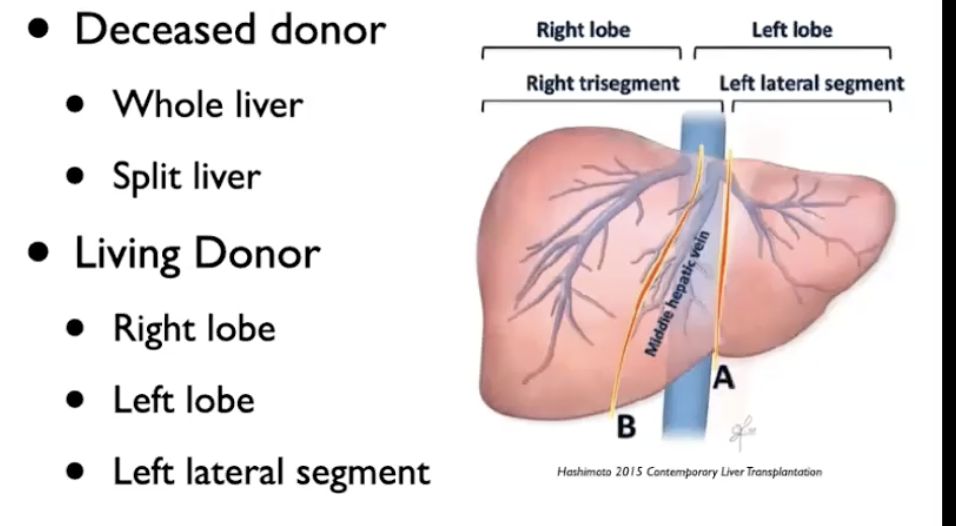
Liver Transplant - Types of Grafts
Deceased donor
maybe whole liver
split liver transplant may occur - not often
left lateral segment of liver usually used for pediatric recipient
right lobe graft used for an adult recipient
Living donor
most common at uHn - right lobe adult to adule can be used
left lateral segment can be procured for a pediatric liver transplant recipient
rarely - left lobe transplant peformed
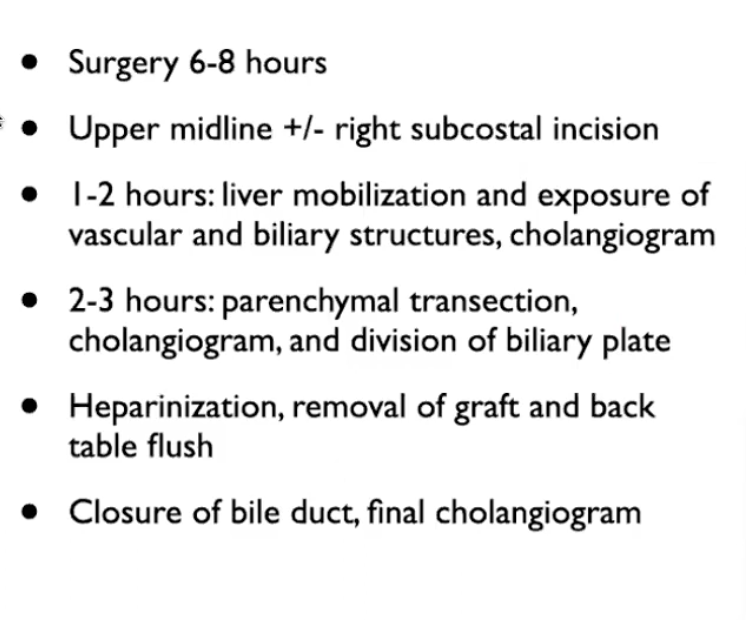
Living donor hepatectomy
done through upper midline incision maybe sometimes with a right subcostal incision added in
First two hours verify liver anatomy - vasucular and billary structure
Cholangiogram - verify biliary anatomy of the donor
2 to 3 hours - parenchymal transection
Bile duct is carefully divided to ensure that it is not taken away from donor
Donor is anticoagulated with heparin - major blood vessels to be removed and split up are divided
Graft is removed and flush of graft with pefusion liquid is done
final cholangiogram done to verify that the bile duct anatomy is intact in the portion remaining in the donor
- hepatectomy
Total hepatectomy must occur in recipient
major consideration - significant bleeding can occur
involves cross clamp the portal vein and the inferior vena cava above and below the liver
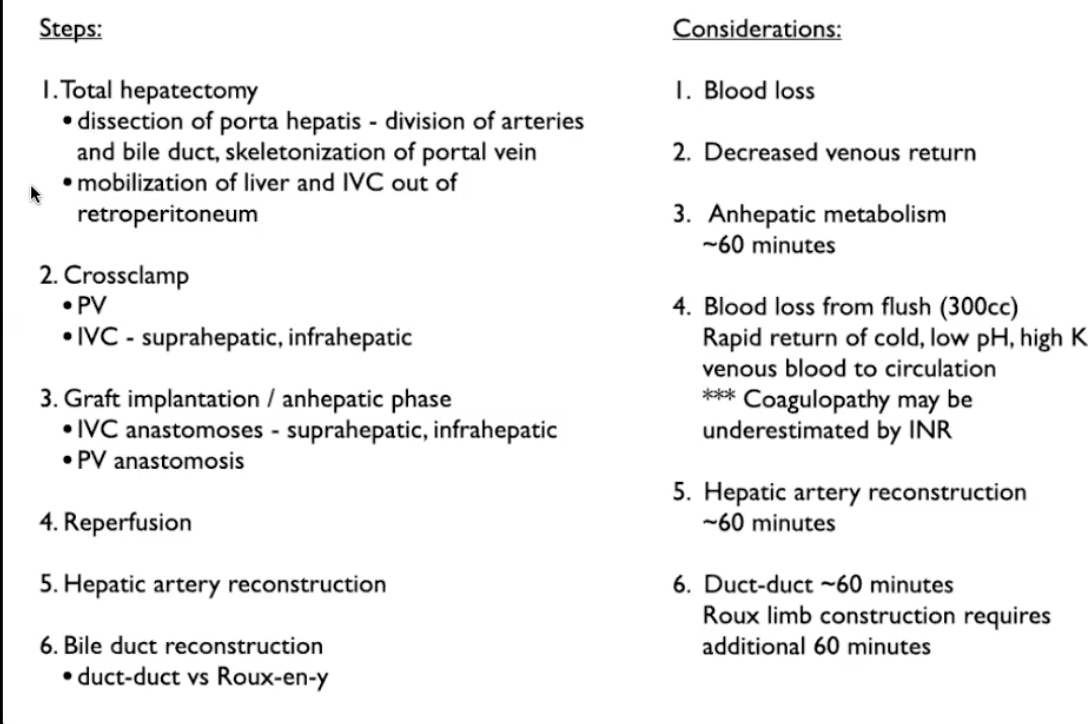
Classical deceased donor full liver transplant- Anhepatic phase
when the new liver is added in
anastamosis of inferior vena cava above and below the liver as well as the portal vein anastamosis
major consideration in anhepatic phase
decreased venous return to heart - vasuclar challenges
anhepatic - absence of liver function - patients metabolism can be deranged - managed by anesthesia
Classical deceased donor full liver transplant- reperfusion
Remove portal vein clamp and flush 300 ccs of first pass blood and venting it through inferior vena cava to wash out as much as the high potassium cold preservation solutoin in the liver graft
inferior vena cava clamps released to restore circulation
major considreations for surgery and anesthesia
hemodynamic instability from blood loss due to flushing of the liver
as well as effects on circultion of low pH high potassium blood from the liver graft into systemic circulation
Classical deceased donor full liver transplant- hepatic artery reconstruction
After the reperfusion state
reconstruct important artery
takes about 30 - 60 minutes
usually direct anastamosis from recipients native hepatic artery and donor hepatic artery can be done
hepatic artery provides critical source of blood flow to billary tree in new liver
Classical deceased donor full liver transplant- bile duct reconstruction
Last step of the process
In these cases - direct connection between native bile duct and donor duct can happen
Roux en hepaticojejunostomy may occur if compliations
after done abdomen is closed
Roux en hepaticojejunostomy
Occurs when native bile duct of recipient is unhealthy or of poor size - special procedure to connect to donor duct that takes another hour in the OR
Piggyback implantation
Situation where the retorhepatic inferior vena cava is preserved in recipient rather than removed
requires additional disection to mobilize liver off inferior vena cava
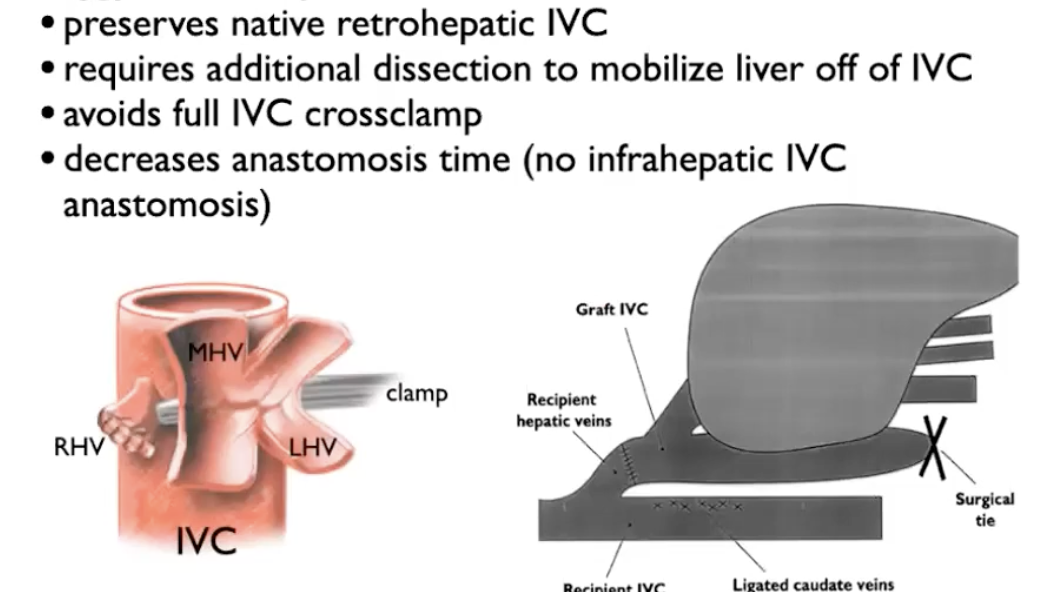
Partial liver transplantation
Used most commonly at UHN for living liver transplant when donor graft from right lobe implanted into recipeint
Can also be used in deceased donor split liver tranpslantation
preserves inferior vena cava of recipient
branches of hepatic veins are anastamosed to inferior vena cava directly
this graft is move sensitive to cvp in recipient because it is smaller part of the liver so more predisposed to venous congestion
sometimes amount of blood flow of liver into portal veins needs to be adjusted to reduce congestion - fixed through splenic artery ligations, splenctomy or portal cava shunt
More common in split liver deceased donotion, less common in living donor - signficant bleeding from cut surface of liver parenchyma after reperfusion
Recipient portal vein thrombosis
May require signficant variation in surgical technique
Commmon solution is to place interposition vein graft from the recipients superior mesenteric artery to the portal vein on the graft
superior mesenteric interposition graft is often done earlier before native hepatectomy
ensures good inflow through portal vein graft established for placing the new liver in place and attemping reperfusion
Recipient hepatic artery stenosis and thrombosis
Problems in arterial flow in recipients native hepatic artery due to stenosis or thromobosis
most common solution - use a graft of illiac artery from deceased donor to construct an interposition graft from the recipients aorta to donor hepatic artery
done before anhepatic phase and implating of new liver - arterial flow prepped for new liver
partial infrarenal aortic clamp is required for graft - hemodynamic effect on recipient
Liver transplantation from DCD donors
At UHN we infuse tPA (thrombolytic agent) to break up the microvascular thrombosis into hepatic artery before graft reperfusion
yields a higher risk of post reperfusion bleeding and a prolonged period to return to hemostasis before return to operation
Patient factors impacting liver transplant intraoperative course
Degree of liver dysfunction in recipeint can impact risk of bleeding
degree of portal hypertension impacts the space for liver, ascites
Collateral vessels and portal hypertension - impact ability to tolerate cross clamp
Portopulmonary hyptertention and hepatopumonary syndrome - impact pulmonary outcomes and need for monitoring by anesthetia in surgery
Previous surgerys such as liver transplant or resection can cause adhesions making surgery challengin
Hepatic artery or vein thromnbosis extend surgery due to need for conduit grafts to establish good blood flow to graph
Diagnoses such as cancer impact it
Cell saver device cannot be used for patients with hepatocellular cancer
comorbidities such as cardiac, lung and renal disese influence degree of blood lost
Liver graft factors that impact intraoperative course
Size of donor liver and type of flush solution for liver procurement - impact the amount of cold, low pH and high Potassium fluid released into recipient systemc
donor age, steatosis (degree of fattiness of liver), size of donor liver and ischemic time and whether liver is got from (dcd ndd or ld)
impacts pH and level of coagulopathy
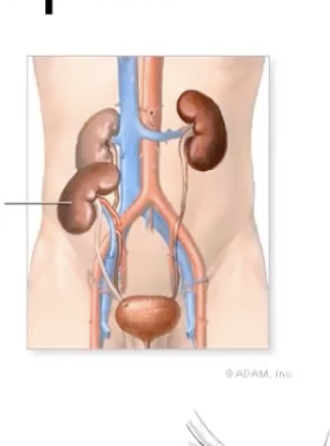
Function of Kidneys
Each kidney has an artery and a vein associated with it
Kidney anatomy
Each kidney has a cortex and a medulla
made up of a million nephron
Nephron = funtional unit of the kidney
Kidney has high blood flow
- Goes through glomerulus through the nephron, waste products eventually enter the ureter to be excreted as waste from the bladder
Chronic Kidney Disease
Fluid retention in the lungs - causes pulmonary edema - build up of fluid in the lungs that compromises the function of gas exchange - can be fatal
Uremia - consequences of build up waste products
fatigue
vomitng
seizures
pericarditis - inflammation of lining of the heart - can be
neuropathy - issue of nerves being not feeling
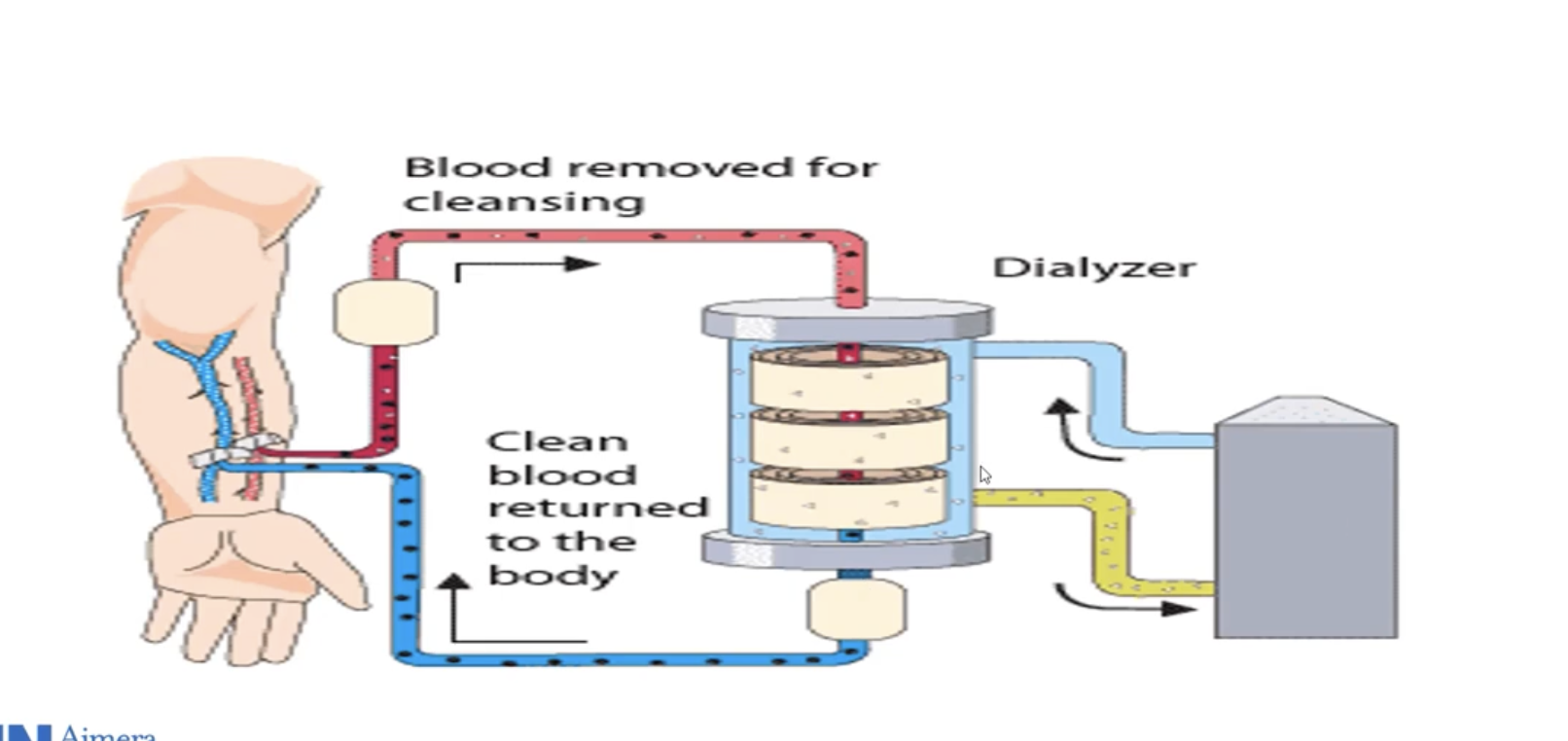
Hemodialysis
Need acess to artery and vein (aka fistula)
Blood flows into hemodialyzer and is cleaned of waste products and goes back into patients
Helps maintain fluid and electrolytes
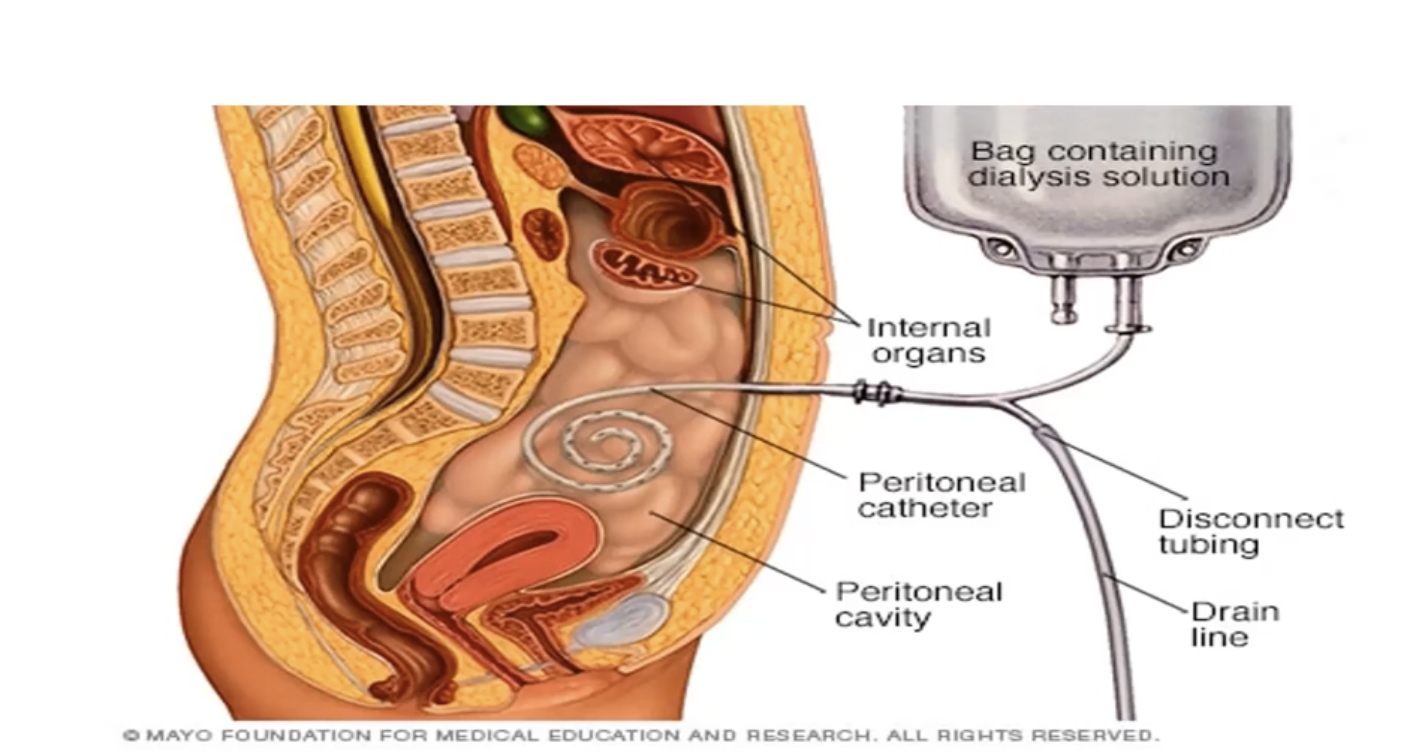
Peritoneal dialysis
Catheter inserted in the peritoneal cavity
Dialysate is pumped in through the catheter and helps to remove the waste products in the body
pumped in and out of the peritoneum many times to achieve full filtration
Why is renal transplantation the superior intervention to dialysis in ESRD?
Provides constant removal of wastes and homeostasis
higher quality of life
Survival is better on tranpslant
cheaper cost to healthcare system
50 k every year for dialysis vs 50 k investment in tranpslant and then 10 to 15 k in the following years