Case 1: T Petty - Central Ventilation Control
1/37
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
38 Terms
Triage Information
TPR + pulse oximetry
Triage: T
Temp
Normal: 37ºC (36.5-37.5)
Regulated by hypothalamus
Triage: P
Pulse rate and BP
Normal: 60-100 bpm
Higher: Tachycardia
Lower: Bradycardia
BP varies
When measuring:
No caffeine and nicotine
Empty bladder
Sitting, uncrossed legs
Triage: R
Respiratory rate
Normal Adult: 12-20 breaths per min
Child: 30-60 breaths per min
Decrease with age
High: Tachypnea
Lower: Bradypnea
Breathing depth
Increased Depth: Hyperpnea
Hyperventilation: Increase breathing rate and depth
Triage: Pulse Oximetry
Normal: 95-100%
Smoking status for clarification
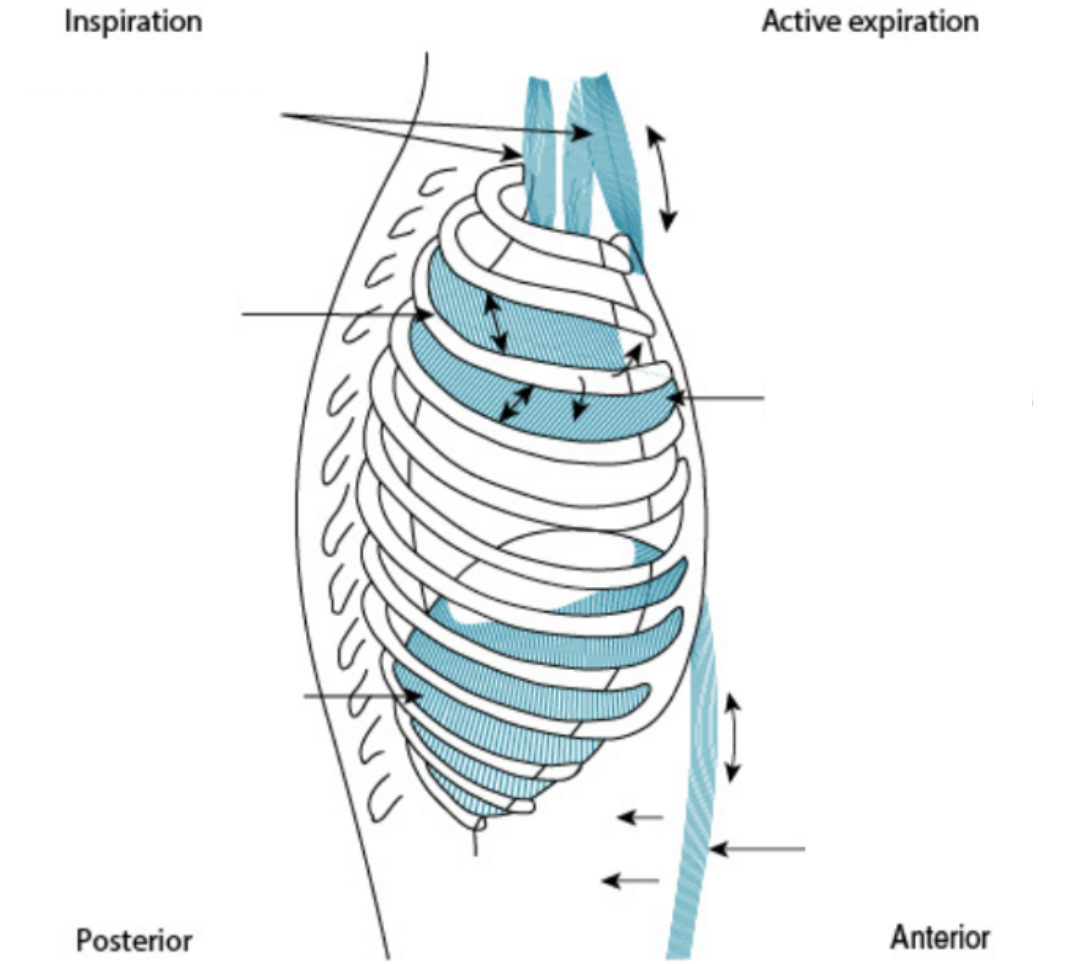
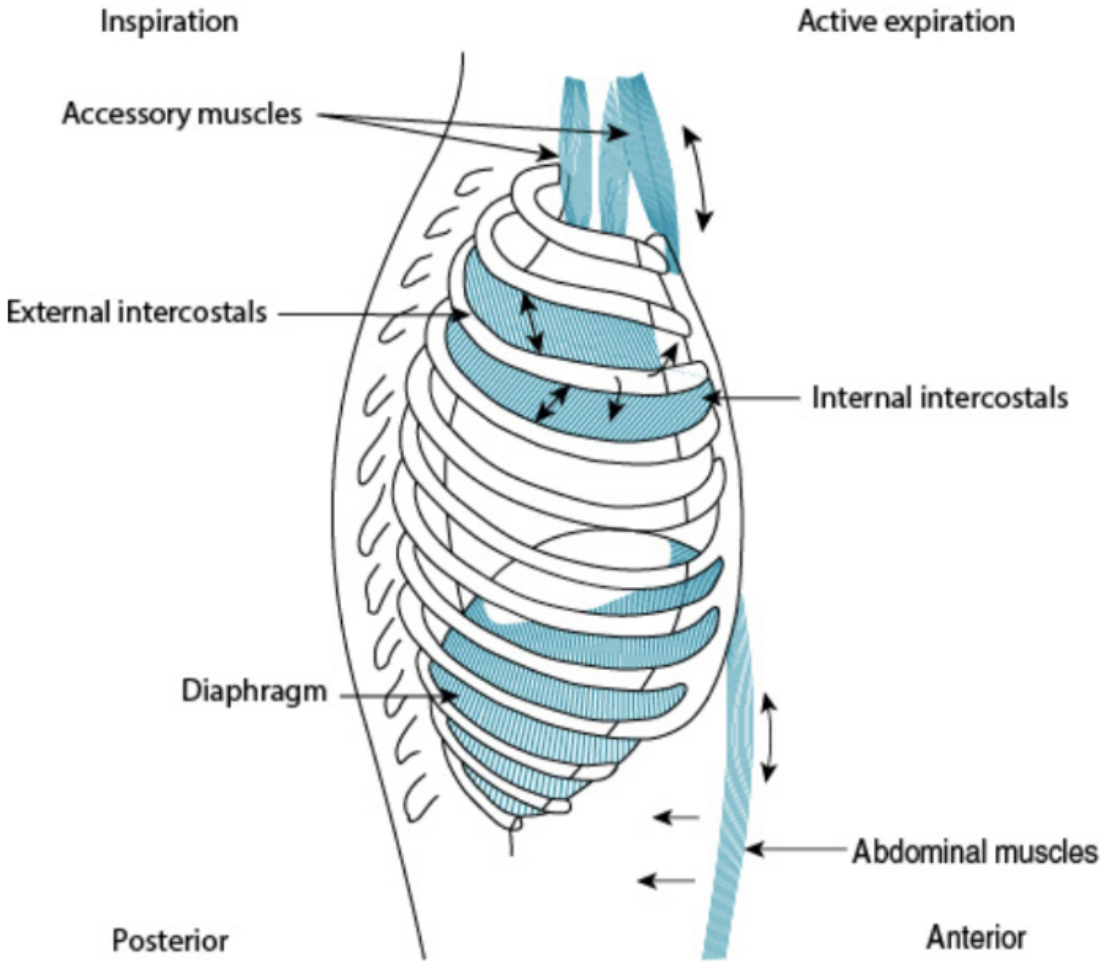
Ventilation Muscles
Diaphragm
Intercostal Muscles
Abdominal Muscles
Diaphragm
Inspiratory muscle
Dome-shaped
Connected to sternum, 6 lower ribs, vertebral column, pericardium
Innervated by phrenic nerves from spinal cord (C3-5)
Intercostal Muscles
External
Internal
External Intercostal Muscles
Inspiratory muscles
Outer muscles under ribs
Anterior and inferior fibres
Internal Intercostal Muscles
Expiratory muscles
Inner muscles under external intercostals
Anterior and superior fibres
Accessory Muscles
Scalene
Abdominals
Accessory Muscles: Scalene
Inspiratory
Accessory Muscles: Abdominal Muscles
Expiratory muscles
3 layers
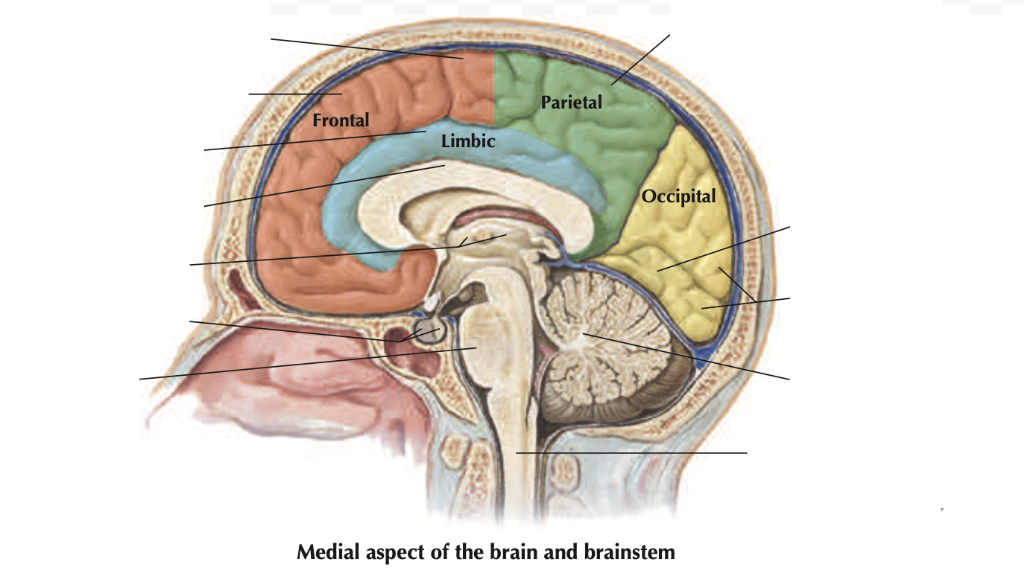
Anatomy: CNS Breathing Control
Brainstem
Delicate location
Pressure/obstruction stops breathing
Brainstem
Midbrain
Medulla oblongata
Pons
Brainstem: Medulla Oblongata
Contain:
Dorsal Respiratory Group (DRG)
Sensory termination of:
Vagus Nerve (Lungs): Central Chemoreceptors
Glossopharyngeal Nerves (Carotid, Aortic): Peripheral Chemoreceptors
Ventral Respiratory Group (VRG)
Pre-Botzinger complex
Brainstem: Pons
Contain:
Pontine respiratory group
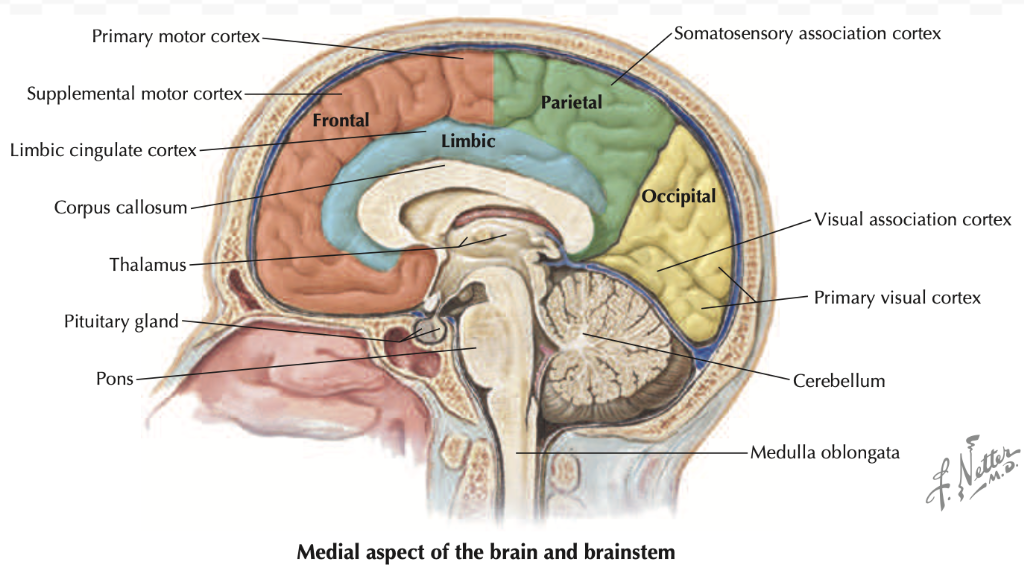
Physiology: Central Respiration Control
Respiratory Centre: Neurons in medulla oblongata and pons
DRG: Inspiration
VRG: Inspiration + Expiration
Pontine Respiratory Group: Breathing rate/depth
Respiratory Centre: DRG
Integrate signals from chemoreceptors + baroreceptors
Respiration:
Transmit ramping signal to muscles for 2 secs = Contraction = Inspiration
Signal stops for 3 secs = Muscles relax = Expiration
Cycle repeats
Heavy Respiration: Increase ramp signal speed = Rapid lung filing
Frequent Respiration: Decrease ramp signal limit = Shorter inspiration length
Respiratory Centre: VRG
For forced inspiration and expiration
Inspiration: Increase respiratory drive
Expiration: Stimulate accessory muscle contraction
Pre-Botzinger Complex: Pacemaker neurons controlling respiration rate/pattern
Respiratory Centre: Pontine Respiratory Group
Control “off” point of inspiratory ramp
Strong Signal: Decrease inspiration time (30-40 breaths per min)
Weak Signal: Increase inspiration time (3-5 breaths per min)
Contains:
Apneustic Centre: Inspiration depth
Pneumotaxic Centre: Inspiration duration
Physiology: Chemical Respiration Control
CO2, H+, O2
Detected by chemoreceptors
Central: Brain + brainstem
Peripheral: Carotid arteries + aortic arch
Chemical Respiration Control: Blood CO2 and H+
Direct control
Increase CO2 (Hypercapnia)
Cross BBB = Increase H+ = Decrease pH
Stimulate central chemoreceptors in chemosensitive areas (ventrolateral medulla + retrotrapezoid nucleus) to contract respiratory muscles
Increase respiratory rate + depth
Decrease CO2
Decrease H+ = Increase pH
Decrease respiratory rate + depth
Chemical Respiration Control: Blood O2
Indirect control
Decrease O2 (Hypoxia)
MUST be dissolved in blood, unbound to hemoglobin
Stimulate peripheral chemoreceptors to signal respiratory centre to contract muscles
Increase respiration
Physiology: Mechanical Respiration Control
Stretch receptors
Ventilation Pathophysiology: Hyperventilation
Increased breathing rate + depth
Insufficient gas exchange
Decrease blood CO2
Increase pH
Consistent O2
Ventilation Pathophysiology: Hypoxemia
Decreased blood O2
Stimulate peripheral chemoreceptors to increase respiration rate + depth
Opioids
Analgesic compounds working on opioid receptors
CNS depressant
Includes:
Morphine
Codeine
Endogenous opioid peptides
Endorphins
Enkephalins
Dynorphins
Opioid Receptors
Agonists of:
μ-opioid receptor
Major analgesic receptor
Morphine > codeine
δ and κ opioid receptor-like subtype 1 receptors
Opioid Treatment
Naloxone
Opioid receptor antagonist
Half-Life: 30-80 mins
Opioid Pharmacokinetics: A
Well absorbed subcutaneously, intramuscularly, orally
Oral: First-pass effect = Higher dose (variable outcome)
Less in codeine and oxycodone
Other Methods: Oral mucosa (lozenges), transdermal patches
Opioid Pharmacokinetics: D
To high perfusion tissues
Skeletal Muscle: Main reservoir
Adipose tissue
Opioid Pharmacokinetics: M
Into polar metabolites
Adverse effects for renal failure patients
Prolonged doses = Excess CNS excitation
Opioid Pharmacokinetics: E
By kidneys in urine
Renal impairment = Sedation + respiratory depression risk
Opioid Pharmacodynamics (MOA)
Bind opioid receptors (G protein-coupled receptors) in brain and spinal cord
Mostly μ receptors in spinal cord dorsal horn
Decrease NT release to cause
Sedation
Respiratory depression (difficult to overcome)
Mioisis
Analgesia
Euphoria
Cough suppression
Tolerance and dependence from repeated use
Opioids: Effect on Respiratory Drive
Dose-dependent effects
Opioids bind μ receptors in brainstem respiratory centre
Inhibit excitatory signals
Decreased response to increased CO2 levels
No increase in respiratory drive (rate + tidal volume) when CO2 increases
Decreased respiratory drive = Respiratory depression
Dangerous/fatal for patient