Dementia (Kaminski)
1/46
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
47 Terms
What are the signature lesions in Alzheimer’s?
Which neurons and NTs are affected?
Amyloid plaques and neurofibrillary tangles
Reduction in number of cholinergic neurons and loss of nicotinic receptors
Basically ACh
How is AD diagnosed
Diagnosis of exclusion
Only way to confirm diagnosis is with autopsy or biopsy
Should evaluate blood cell counts, electrolytes, liver function tests, thyroid, and B12 to rule out other causes
Imaging (MRI, CT) recommended by guidelines
What are the stages of dementia
What is the MMSE score of each
Mild Cognitive impairment
Mild dementia (26-21)
Moderate dementia (20-10)
Severe dementia (9-0)
Patient characteristics of Mild Cognitive Impairment (MCI)
Precedes dementia
Cognitive complaints that do not impact patient functioning
Patient characteristics of Mild dementia
Difficulty remembering recent events
Ability to manage finances, prepare food, and carry out other household activities declines
May get lost when driving
Begins to withdraw from difficult tasks and give up hobbies
Patient characteristics of Moderate dementia
Requires assistance with activities of daily living (ADLs)
Frequently disoriented to time (date, year, season)
Severe impairment to recall of recent events
Begins to lose long term memory (life events, names of family members)
Functioning may fluctuate
Unable to drive safely
May become suspicious or tearful; agitation, paranoia, delusions common
Patient characteristics of Severe dementia
Loses ability to speak, walk and feed self
Incontinent of urine and feces
Requires around the clock care
What are the treatment goals for a patient diagnosed with AD
Primary Goals
Symptomatically treat cognitive difficulties
Preserve patient function for as long as possible
Secondary Goals
Managing psychiatric and behavioral sequelae
Do current treatments prolong life?
Current treatments do NOT prolong life, cure AD, or halt or reverse pathophysiology
What type of treatment should be done first
Nonpharm treatment
What are some general principles for interacting with someone with AD
Consider vision, hearing, or other sensory impairment
Find optimal level of patient autonomy and adjust expectations over time
Avoid confrontation – remain calm, firm, and supportive; validate feelings
Maintain a consistent, structured environment with appropriate level of stimulation
Provide frequent reminders and orientation cues
Reduce choices, keep requests simple, avoid complex tasks
Redirect to an enjoyable activity
“Meet the patient where they are at”
How should we address symptoms of AD like sleep disturbances and incontinence
Use behavioral interventions rather than meds whenever possible for symptom management
Sleep hygiene for sleep disturbances
Redirection for wandering
Identifying triggers for agitation and aggression
Bladder training/habit training for incontinence
Who needs to be educated aside from the patient
Caregiver
Which meds are associated with cognitive impairment
Benzodiazepines and sedative hypnotics
Anticholinergics
Antipsychotics
Which meds can cause delirium or acute cognitive changes
H2 receptor antagonists
Corticosteroids
Merperidine
What would we want to do with the meds that cause delirium and cognitive impairment
Deprescribe where possible/clinically appropriate
How do you treat MCI due to AD
Anti-amyloid mAb
How do you treat mild-moderate AD
Cholinesterase inhibitor (or anti-amyloid mAb)
How do you treat moderate-severe AD
Memantine
Memantine + cholinesterase inhibitor
or Donepezil or Rivastigmine patch alone
List the Cholinesterase inhibitors
Donepezil (Aricept)
Rivastigmine (Exelon)
Galantamine (Razadyne, Razadyne ER)
Benzgalantamine (Zunveyl) (new)
What is the MOA of Cholinesterase inhibitors
Inhibit hydrolysis of ACh by AChE → enhance cholinergic activity
What are the Adverse Effects with Cholinesterase Inhibitors
Dizziness, syncope
Bradycardia*, atrial arrhythmias, SI and AV block, MI
N/V/D, anorexia, weight loss
Peptic ulcer disease, GI bleed
Insomnia, vivid dreams, nightmares
*C/I if HR <50 BPM
What is monitored with Cholinesterase Inhibitors
Reports of dizziness or falls
Pulse at baseline, monthly during dose titration and every 6 months
Periodic BP and postural BP changes
Weight and GI complaints
Signs/Symptoms of GI bleed
Complaints of sleep disturbances, daytime drowsiness
Which Cholinesterase Inhibitors are available as a patch?
How frequently is each patch applied?
Donepezil (Adlarity) applied once weekly
Rivastigmine (Exelon Patch) applied daily
Which needs dose adjustments for renal or hepatic impairment
Rivastigmine
Which can cause serious skin reactions, like SJS
Galantamine
Goal dose is reached by titration over several weeks.
What would cause titration to restart and what would happen then?
Titration for a treatment interruption due to potential for GI upset will have to restart
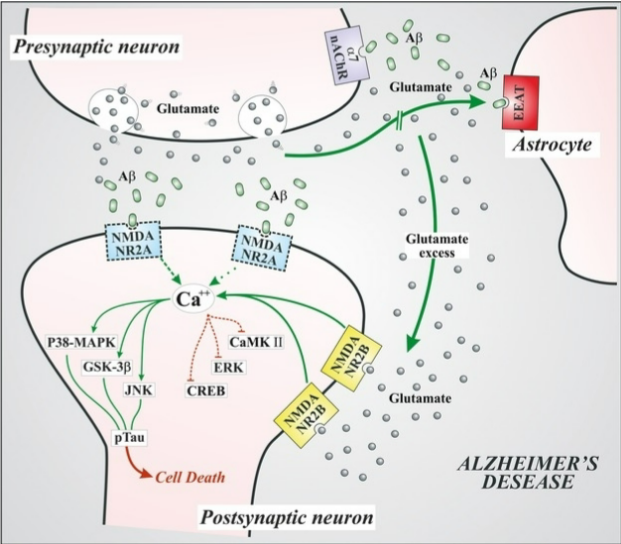
Memantine (Namenda) MOA
NMDA receptor antagonist
Blocking NMDA receptors mitigates excitatory neurotoxicity and potentially provides neuroprotection
Memantine (Namenda) adverse effects
Generally well tolerated
HA, confusion, dizziness, hallucinations
Constipation
Memantine (Namenda) Counseling
Interruptions require re-titration of dose
Taken w/ or w/o food
Capsules can be open and sprinkled on applesauce
Does Memantine require dose adjustments for renal or hepatic impairment
Yes
Not recommended w/ severe renal or hepatic impairment
Memantine goal dose
Titrated up to goal dose over several weeks and interruptions require re-starting the titration
What is the name of the product that combines Memantine and Donepezil
Namzaric
Should any of these agents be stopped abruptly?
No
What are the Monoclonal Antibodies
Aducanumab - withdrawn
Lecanumab (Leqembi)
Donanemab (Kisunla)
Gantenerumab (in trial)
Which stage(s) of disease are these approved for
FDA approved for MCI due to AD or mild AD
Monoclonal Antibodies MOA
Is there any evidence that this mechanism has a significant effect on symptoms?
Anti-amyloid antibodies bind to and remove amyloid in the brain
Currently approved agents show modest slowing of cognitive decline, not reversal
Monoclonal Antibodies adverse effects
Infusion related reactions
Amyloid-related imaging abnormalities (ARIA)
Cerebral edema (ARIA-E)
Microhemorrhage (ARIA-H)
What monitoring is needed because of these AE
Test for ApoE ε4 allele (not used in homozygotes)
Consider patients on anticoagulation
All mAbs require baseline and routine MRIs to monitor for ARIA - specific recs for each
Monitor for HA, confusion, dizziness, visual disturbances, nausea, gait difficulty, seizures
What is the dosage form of mAbs
What else should be known
Lecanemab (IV and SubQ)
Donanemab (IV)
require a provider to administer
Require significant (and expensive!) monitoring
What are some examples of neuropsychiatric symptoms
Psychotic
Hyperactive - inappropriate or disruptive behavior
Affective - depression
Apathy - lack of emotion
Often reason for nursing home placement
How should neuropsych symptoms first be addressed
Nonpharm therapy
Identify and eliminate potential causes – medications, illnesses, environment
Identify triggers – noise, glare, background distractions, personal discomfort (pain, hunger, thirst, skin irritation, temperature, fear)
Redirect patient rather than confront
When are meds warranted for neuropsych symptoms
Are severe enough to cause significant distress to patient or caregivers
Interfere with function/cause disability
Impede delivery of necessary care
Pose a danger to self or others
Have not responded to nonpharmacologic measures
What are general best practices for pharm treatment?
General principles:
Reserve for situations where nonpharmacologic therapies have failed
Used reduced doses
Monitor closely
Titrate doses slowly
Minimize duration of therapy
Attempt tapers/discontinuation – behaviors fluctuate over time
Document carefully
Treatment should be considered temporary
Manage caregiver expectations
Which antidepressants are generally preferred?
Which class should be avoided
SSRIs generally preferred based on AE, risk of interactions, and efficacy
Best evidence for Sertraline and Citalopram
Avoid tricyclic antidepressants
Which antipsych has an FDA-approved indication for management of agitation associated with AD
Brexpiprazole (Rexulti)
What is the BBW for all antipsychs?
What other AEs of antipsychs may be concerning in AD patients
BBW
increased risk of mortality in older adults with dementia related psychosis
Suicidal thoughts and behaviors
Risk of sedation
Extrapyramidal symptoms
Anticholinergic effects
Hypotension