renal physiology III - renal clearance
1/11
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
12 Terms
renal clearance
• Renal clearance is the removal of a given substance from the plasma by the kidney, excreted into the urine per minute
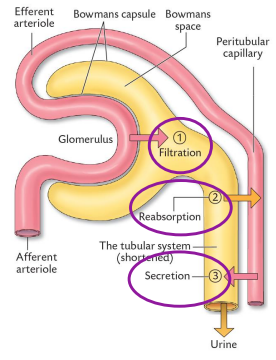
It is a function of:
• Filtration (GFR).
• Tubular Reabsorption.
• Tubular Secretion.
• The collective work of the three processes lead to urine formation and determines the amount of a specific substance in the urine.
• Clearance values provide numerical expressions of how efficient the kidneys excrete various substances.
• The Renal Clearance Rate (C) of a substance (s) is defined as the volume of plasma containing (s) being completely cleared of (s) and excreted in the urine per minute.
renal clearance rate calculation
Collect urine for known period of time.
• Measure concentration of the substance (s) in the urine and calculate its excretion in the urine per minute.
• The clearance of the substance (Cs) i.e. the volume (mL) of plasma that would have to be cleared completely of the substance to result in the measured urinary excretion can then be calculated.
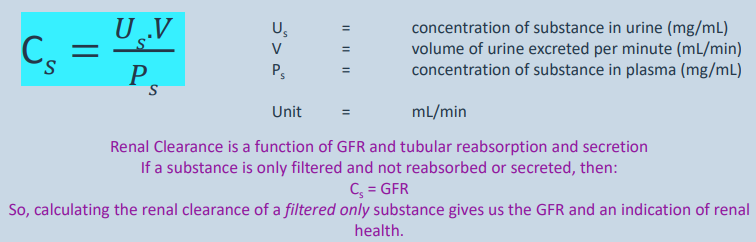
renal clearance (cleaning rate) = GFR (flow speed) +tubular reabsorption and secretion
if substance only filtered and not reabsorbed/secreted=Cs(renal clearance) = GFR
calculating renal clearnace of filtered only substance gives us GFR and indication of renal health
renal clearance as a measure of GFR
The clearance of a substance which meets the following criteria will give a measure of GFR:
• It is freely filtered at the glomerulus.
• It is not reabsorbed from the filtrate.
• It is not secreted into the filtrate.
• It is not metabolised by the tubular cells.
• It does not interfere with kidney function - not toxic.
• Easily measured.
In other words, such a substance enters the tubular filtrate via filtration only and then flows through the tubules and exits in the urine. There should not be any reabsorption or secretion.
what substance could we use to calculate GFR?
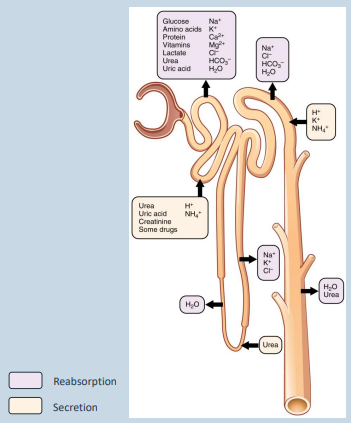
basically this slide explains why everyday substances like glucose, vitamins and urea cant be used by docs to calculate GFR, because the substance needs to have been an OG - passing through the filter in renal corpuscle, travelling down the tube completely untouched, and exits in your urine - not reabsorbed or secreted in any way. Both urea and the substances mentioned below fail the test because first ones are reabsorbed back into blood/metabolized, and urea is reabsorbed into blood
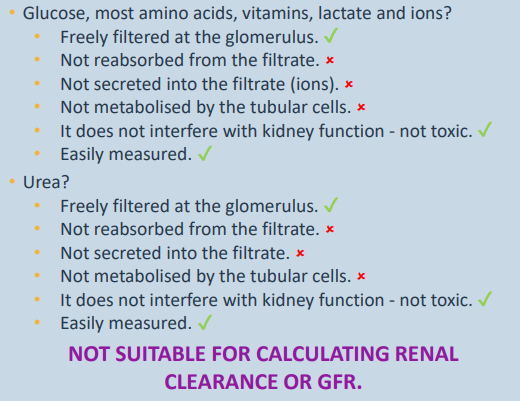
Glucose, most amino acids, vitamins, lactate and ions?
Freely filtered at the glomerulus.
Not reabsorbed from the filtrate.
Not secreted into the filtrate (ions).
Not metabolised by the tubular cells.
It does not interfere with kidney function - not toxic.
Easily measured.
Urea?
Freely filtered at the glomerulus.
Not reabsorbed from the filtrate.
Not secreted into the filtrate.
Not metabolised by the tubular cells.
It does not interfere with kidney function - not toxic.
Easily measured.
NOT SUITABLE FOR CALCULATING RENAL CLEARANCE OR GFR.
Glucose, Amino Acids, Vitamins, Lactate, & Ions
The Good: They easily pass through the filter, are safe, and are easy to measure.
The Flaw: Your kidney actively reabsorbs them back into the blood, secretes extra ions into the fluid, or metabolizes them inside the cell walls.
Urea
The Good: It passes through the filter easily, is non-toxic, and is easy to measure.
The Flaw: Your kidney reabsorbs a massive amount of urea back into the blood (to help run that Loop of Henle salt gradient we talked about earlier) and also secretes some.
what substance could we use to calculate GFR?
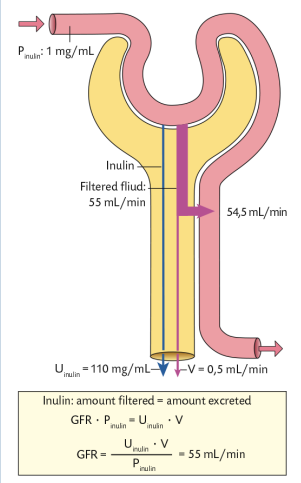
Inulin (not insulin!).
• A polymer of fructose with molecular weight 5.2kDa.
• Not produced in the body.
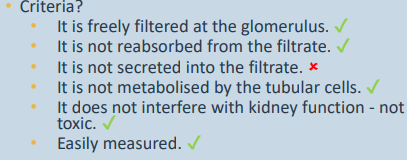
Criteria?
• It is freely filtered at the glomerulus.
• It is not reabsorbed from the filtrate.
• It is not secreted into the filtrate.
• It is not metabolised by the tubular cells.
• It does not interfere with kidney function - not toxic.
• Easily measured.
•Inulin: amount filtered = amount excreted.
• However… must be administered intravenously (as continuous rate infusion).
• Useful research tool but not very useful clinically
essentially renal clearance is just how fast the liquid gets completely cleared of (from blood) and excreted in the urine per minute. so the efficiency of the kidney. The best candidates for this are inulin and creatinine, the body’s substances cant be used to measure.
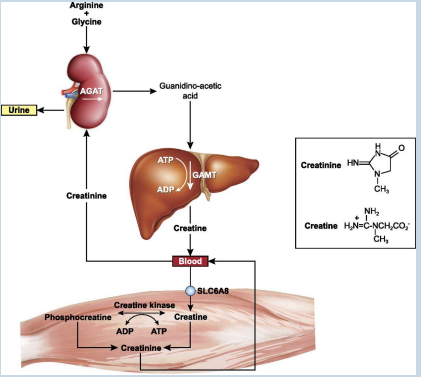
Is there a substance that is more useful clinically? creatinine
• Degradation product of creatine phosphate in muscles.
• Production and degradation usually very stable
• Species variability in secretion – 5-10% in primates, negligible in cats and dogs.
• Small error in clearance formula…
it meets the criteria to measure renal clearance, unlike inulin which is an artificial method for research purposes
creatinine error cancellation
• Slight secretion means that creatinine enters the filtrate not only by filtration but also by secretion.
• Therefore, the term “U” (conc of substance in urine) in the clearance formula is erroneously high
However…
• the method used for estimation of plasma creatinine concentration also detects another compound.
• Therefore, the term “P” (conc in blood plasma) in the formula is also erroneously high.
• The two errors cancel each other out so creatinine clearance is commonly used to measure GFR.

plasma concentrations of substances to indicate GFR
• Can also measure substances normally excreted by the kidneys in plasma (or serum).
• Urea (blood urea nitrogen, BUN).
• Creatinine.
• SDMA (symmetric dimethylarginine).
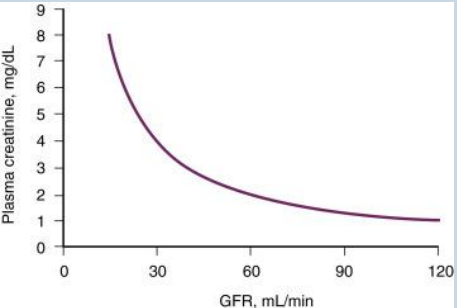
Relationship between GFR and plasma (or serum) concentration
basically when kidney filtration speed goes down, the waste sitting in your blood goes up
so high levels of urea/creatinine is bad because GFR is not high enough to filter it out
plasma concentrations of substances to indicate GFR cont
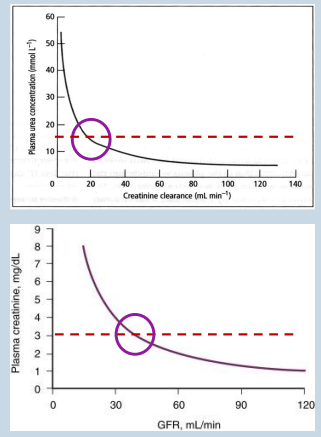
Urea:
• Reabsorbed in PCT and CD.
• Secreted in descending loop of Henle for hyperosmotic gradient.
• Variable concentration depending on diet and hydration.
• Requires significant kidney damage before noticeable effect in plasma concentration.
Creatinine:
• Not reabsorbed.
• Only small amount secreted into renal tubules.
• Stable production/degradation ratio.
• Raised when up to 75% reduction in GFR
the circles are the warning points - lose a massive amount of kidney function before standard blood test notices a change - red dashed lines show upper limit of whats considered normal
danger zone is right side - shows kidney damage/failure
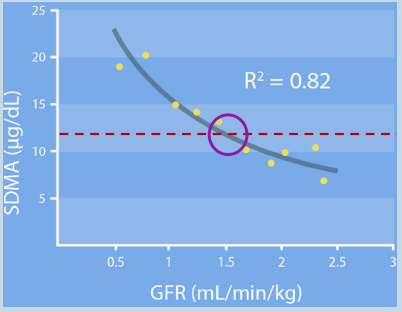
plasma concentrations of substances to indicate GFR cont - SDMA
• Symmetric dimethylarginine.
• A methylated amino acid produced alongside asymmetric dimethylarginine (ADMA) as a
biproduct of intranuclear methylation of regulatory proteins and subsequent proteolysis.
• SDMA is biologically inactive and excreted by the kidneys.
• (ADMA is metabolised).
• Detectably raised when 25-40% reduction in GFR
SDMA is just cell waste, that’s it.
It’s only exit is through the kidney filtered.
It’s a great marker because urea and creatinien couldnt catch kidney damage until 75% of kidney is already destroyed, it’s more sensitive at detecting kidney damage- only at 25%
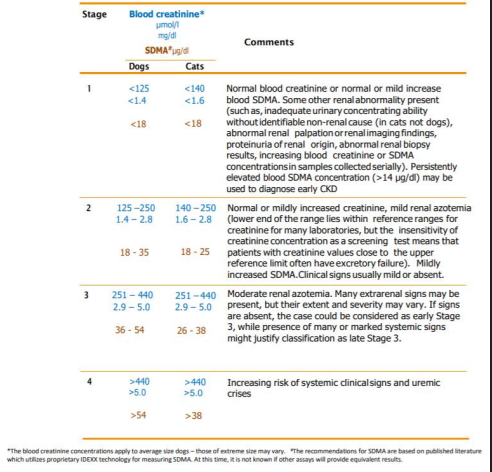
Combination of serum creatinine and SDMA used to help stage chronic renal failure.
Used in conjunction with clinical signs.
other tests
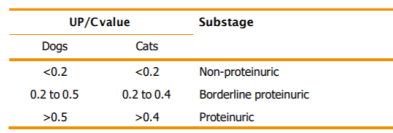
Urine protein:creatinine (UPC).
• Detect protein loss in urine e.g. if glomerular disease is causing destruction of the filtration barrier.
Need to first rule out:
• Urinary tract infection.
• Inflammation.
• Haematuria (blood in urine).
Not always high in renal disease.
proteinuric means too much protein left the blood plasma (hence now leaked in urine) because the glomerulus is broken