KNES 355 Final Exam Review Part 2
1/51
Earn XP
Description and Tags
biological maturation, skeletal system + growth injuries
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
52 Terms
What are the most common techniques for assessing maturity? When are they used?
somatic maturity (age at peak height velocity, maturity offset)
growth studies + clinically
skeletal maturity (hand-wrist radiograph)
pediatric clinical research
sexual maturity (genitalia, breast + pubic hair development)
pediatric non-clinical research
endocrine maturity (blood draw for circulating estrogen or testosterone)
clinical research + treatment programs
dental maturity (# of erupted teeth, level of tooth calcification)
What is maturity offset?
years from peak height velocity
What is the average age at peak height velocity (APHV) for girls and boys?
girls: 11.5
boys: 13.5
Distinguish between early, average, and late maturers for girls and boys?
girls:
early → 1 year before average APHV
<10.5 years
average → 1 year before or 1 year after average APHV
10.5 - 12.5 years
late → 1 year after average APHV
>12.5 years
boys:
early → 1 year before average APHV
<13.5 years
average → 1 year before or 1 year after average APHV
13.5 - 14.5 years
late → 1 year after average APHV
>14.5 years
How is percent of attained adult height used to determine maturity?
pre-pubertal = <88%
pubertal = 88-95%
post-pubertal = >95%
What are the advantages of using APHV or % attained adult stature for assessing maturity?
APHV: estimates are valid when used close to APHV (~after age 10)
% attained adult stature: can be estimated throughout childhood/adolescence
Why is a radiograph of the hand + wrist used to assess skeletal age?
sequence of events is predictable
universal
rate of development varies
many bones from which to make assessment
region not sensitive to radiation (low risk)
can be used for one-time assessment + longitudinally
How many bones are in the hand/wrist at maturity?
30
How is skeletal age used to determine maturity status?
skeletal age - chronological age
± 1 year = average maturer
< 1 year = late maturer
> 1 year = early maturer
What are the advantages of sexual maturity assessment?
non-technical
relatively inexpensive + reliable
can be self-assessed, at any time
______________ sex characteristics are used in male maturity assessment. This includes what?
______________ sex characteristics are used in female maturity assessment. This includes what?
primary, penis/testes development
secondary, breast size + shape, pubic hair distribution (males + females)
What is the alternative secondary sex approach for girls for assessing maturity? What are the strengths + limitations?
menarcheal age
strengths:
most girls experience it
memorable occurrence, accurately recalled
usually predictable in order of events
limitations:
only useful in girls
used as a reference only after it occurs
How does timing of maturity impact performance in sports?
early-maturing youth have temporary advantage in sports that demand strength, speed + power
late-maturing youth eventually catch-up if they persist in or are retained by sport
may be more technically skilled
What is bio-banding?
players are grouped by % of adult height (grouped by similar maturity) vs. chronological age
What are the pros and cons of bio-banding for both early and late maturers?
pros:
late: leadership + game-play, increased confidence, lower perceived injury risk, less physically challenging, impact game play, demonstrate wider range of physical + technical skills
early: skill development, lower perceived injury risk, adopt more team-oriented playing style, more physically + technically challenging
cons:
late: social/psychological factors with “playing down”
early: not real life, parent buy-in and
What are windows of opportunity in maturity + performance?
skill development during childhood prior to PHV
strength gains after PHV
What are the components of bone?
inorganic components:
~65% of bone weight, mostly inorganic calcium + phosphate
remainder:
25% organic matrix, collagen
10% water
What is cortical bone? What percentage of our bones are cortical bone?
‘compact’ bone
external part of long bones
dense, calcified tissue
~80% of bones
structural support, protective functions
What is trabecular bone? What percentage of our bones are trabecular bone?
‘spongy’ or ‘cancellous’ bone
metaphyses of long bones, vertebrae, iliac crest
inner network of thin, calcified trabeculae
active metabolic role
~20%
What are the 3 types of bone cells? What does each one do?
osteocytes → mature bone cells
osteoblasts → bone forming cells
osteoclasts → bone resorbing cells
What is Wolff’s Law?
bone will optimize structure, so as to withstand functional loading, and to ensure the metabolic efficiency of locomotion
What is bone growth?
the accrual of bone mass through bone formation during childhood and adolescence
changes in shape + length
under endocrine control
ceases following puberty, with epiphyseal closure
What is endochondral bone formation?
formation of hyaline cartilage which will later be replaced by bone, responsible for growth in length of long bones
primary ossification center in the hyaline cartilage, bone collar forms around the sides of the cartilage
cavity (medullary canal) forms within primary ossification center
secondary ossification center at the epiphysis
epiphyseal growth plate eventually fuses
What is appositional growth?
direct production of bone without cartilage transition, responsible for growth in girth of long bones
In long bone growth, the epiphysis expands circumferentially due to the __________________________, further elongating the bone. Growth in bone length = ______________ and ______________ expansion.
secondary ossification center, metaphyseal, epiphyseal
What are the 4 zones of the epiphysis/epiphyseal plate? What occurs in each zone?
zone 1: resting zone
cells are relatively inactive
zone 2: proliferating zone
chondrocytes (cartilage cells) rapidly divide + produce collagen
zone 3: hypertrophic zone
cells increase in size + organize into columns
zone 4: terminal zone
chondrocytes stop producing collagen + die
calcification occurs
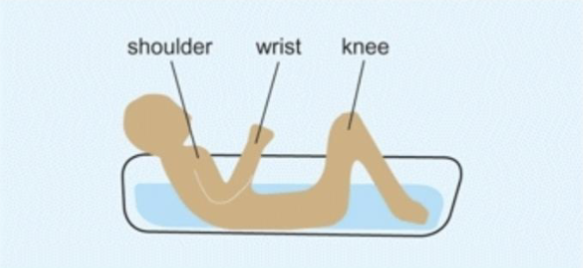
At any point in time, the growth plates within a single long bone are growing at different rates. What is the way to remember which ends of which bones grow faster?
the ‘bathtub’ rule
growth plates above the water line are the fastest growing
What is bone modeling?
osteoblast + osteoclast activity at different places at the same or different times
formation/resorption uncoupled, not sequential as in remodeling
new bone formed by osteoblasts on outer surface (periosteal surface)
bone resorbed by osteoclasts on inner (endocortical surface)
How does bone modeling affect the bone? When does it usually occur?
alters shape + mass
increases bone strength
primarily in the growing years
regional response to local mechanical factors
As the ends of bone grow longitudinally, _____________ and _____________ modelling occur to preserve bone shape.
formation, resorption
To preserve cortical thickness during growth, formation modeling occurs on the ________________ surface and resorption modeling occurs on the ________________ surface.
periosteal (outer), endocortical (inner)
What is bone remodeling?
osteoblast + osteoclast activity on the same site, at the same time, but in specific sequence
coupled action (resorption followed by formation)
replaces old bone + adds new bone
temporary lag between removal + formation (fragility)
Bone remodeling is the predominant bone process modifying mass in _________ but occurs concurrently with bone modelling during ____________. It repairs _______________ on bone.
adults, growth, everyday stress
Peak bone mineral content occurs after ___________. Age at peak bone mineral content velocity is _______ in boys vs. girls. Magnitude of PBMCV is ______________ in boys.
APHV, later, greater
Peak bone mass + strength occurs when?
early 20’s
Boys have greater bone ______ and greater _____________ area, which places bone mass further from the neutral axis, leading to increased bone strength.
area, medullary canal
Adolescence is characterized by __________________ and __________________ in relation to bone. Aging is characterized by ______________, reduced __________________ and _________________.
rapid bone growth, increases in strength, thinning of cortex, bone density, strength
What is stress?
force applied per unit area
What is strain?
deformation of a material → amount bone deforms when stress is applied
What are the 3 rules for bone adaptation?
bone responds to dynamic rather than static loading
adaptation increases with increases in strain magnitude + strain frequency
short bouts of loading are more osteogenic (bone promoting) than longer duration bouts
ceiling effect for bone tissue stimulation (bone desensitizes after longer durations)
bone becomes used to routine strains; structural change is driven by abnormal strains
bone responds to unusual strain distribution
in short:
dynamic loading
short, frequent bouts with recovery periods
abnormal, non-routine strains
Larger bone gains are seen when training is started _____________ puberty or in __________ puberty.
before, early
What is unique about children’s bones compared to adults?
more porous + flexible which allows for greater bending before breaking vs. adults → unique fracture patterns
What is the most common fracture pattern in kids?
buckle fracture (bone compression)
What is a greenstick fracture?
cortex fails on the tension side (analogy to green wood that only breaks on the outside)
in adults, this mechanism would usually result in complete fracture
Which zone of the growth plate is the weakest?
hypertrophic zone
List + describe the 5 Salter-Harris fractures.
type I (slipped/separated)
separation of epiphysis from metaphysis
type II (above the growth plate)
through growth plate + metaphysis
type III (lower than the growth plate)
through growth plate + epiphysis
type IV (through the growth plate)
through all 3 elements
type V (rammed growth plate)
crush injury of growth plate
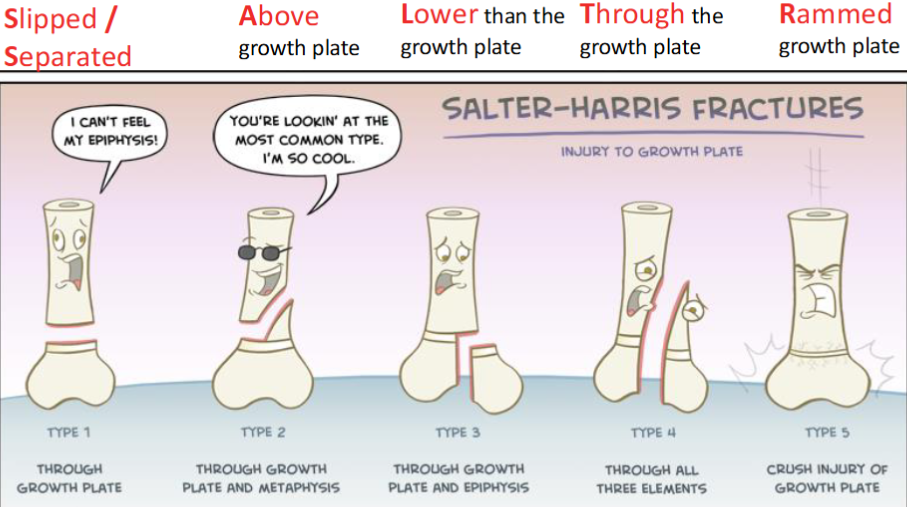
Which Salter-Harris fracture is the most common?
type II
Which Salter-Harris fracture is rare, difficult to see on an X-ray, has a poor prognosis and is almost always diagnosed retrospectively when growth arrest occurs?
type V (rammed)
What is Sever’s disease?
affects growth plate at back of heel, attachment point for Achilles tendon
repetitive stress from running, jumping, etc. causes pain + inflammation
What is Osgood-Schlatter disease?
swelling + irritation of the growth plate at the proximal tibia, pain + swelling below patella, patellar tendon pulls on growth plate causing injury + pain (caused by activities involving lots of running + jumping)
How does the injury pattern for children match the pattern of growth?
growth distal to proximal
Osgood-Schlatter usually more common in older age groups
Sever’s disease usually more common in younger age groups
Late maturers have higher incidence of overuse injuries in the year before PHV and during PHV compared to their early or average maturing peers. Why?
exposed to greater training load + higher intensity games due to their greater chronological age