Parkinsons disease
1/28
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
29 Terms
What is Parkinson's disease?
Parkinson’s disease a neurodegenerative disorder which is progressive and causes degeneration/death of dopaminergic neurons and dopamine in the substantia nigra in the mid brain
What neuron/ neurotransmitter is affected in Parkinson's disease?
dopamine/ dopaminergic neurons
How do dopamine levels change over time in Parkinson's disease?
Dopamine levels in parkinson disease will reduce over time. This is a progressive disease and usually at the time of diagnosis, many of the dopaminergic neurons have been lost (this is because there is essentially a lag time between disease progression and the onset of symptoms). As the disease progresses, more dopaminergic neurons are lost and as a result symptoms progress
Treatment will increase dopamine levels, but what affect does it have on the dopaminergic neurons?
Treatment is symptomatic, it aims to increase dopamine levels to reduce symptoms but has no effect on the dopaminergic neurons so they continue to degenerate - hence the person will eventually die as a result of the disease - remember neurons in the brain are post-mitotic, meaning they do not undergo mitosis, essentially we are born with all the neurons we will ever have
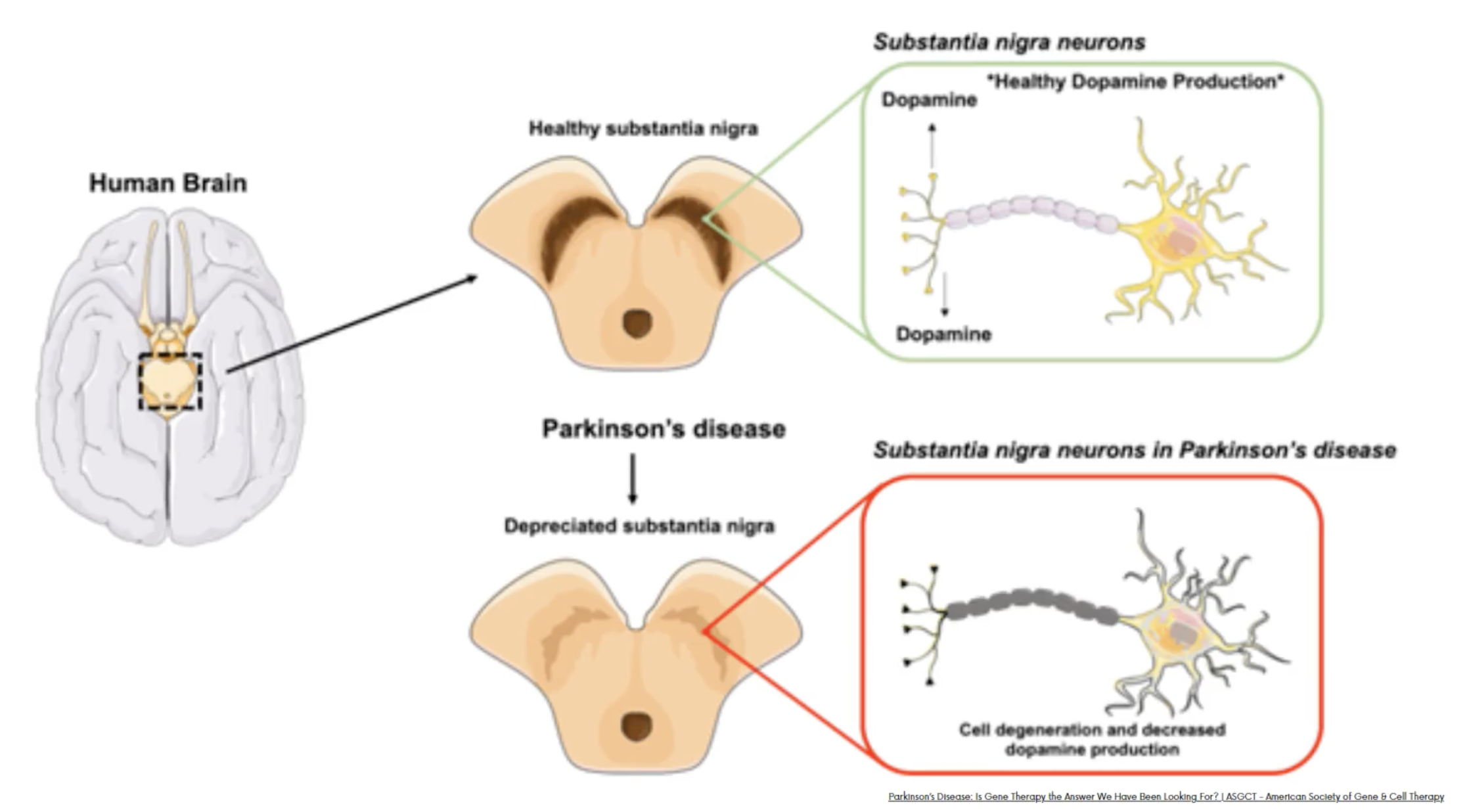
Explain parkinsons disease using this schematic
Parkinson disease is characterised by a loss of dopaminegic neurons and dopamine in the brain in the substantia nigra of the midbrain
What is the role of dopamine?
Dopamine is involved in motor function, reward (motivation), compulsion, pleasure, attention and learning - hence you can see why reduced dopamine levels lead to impaired motor function and you can see how since the drugs aim to increase dopamine - some of the side effects are increased impulse compulsion disorders
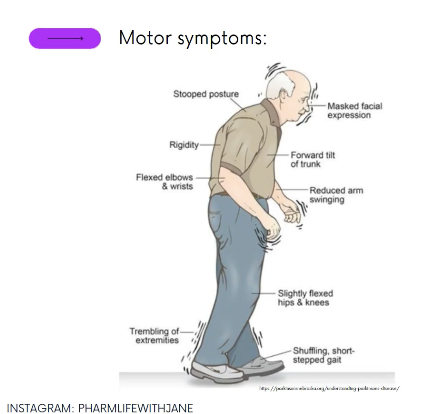
What are the symptoms of Parkinson's disease?
TRAP
Tremor - usually starts on one side
Rigidity - stiffness of limbs
Akinesia - loss or impairment of power or voluntary movement
Postural - stopped
Akinsia - this means A (without) kinsia (movement) - without movement means inability to control voluntary movement
Bradykinesia - this is slow movement (brady meaning slow) kinsia (movement)
What are non-motor symptoms
dementia
depression
swallowing difficulties
weight loss
sleep disturbances
speech and language changes
bladder and bowel dysfunction
What are the treatment aims?
Improve and control the quality of life
Does the individuals symptoms impair their quality of life? - YES & NO pathways
Yes - levodopa with a decarboxylase inhibitor such as carbidopa or benserazide
No - choice of levodopa, or dopamine-receptor agonist, or monoamine oxidase B inhibitor
Do we use combination therapy in PD?
Yes, very likely the patient will take Levodopa/ decarboxylase inhibitor/ COM-T
(Madopar) alongisde MAO-B inhibitor such as selegline or rasagaline or dopamine receptor agonist such such as ronalazine
Levodopa usually taken alongside another drug, what is the class of this ‘other drug’ and what is its role?
Levodopa usually taken alongside peripheral dopa decarboxylase inhibitor (Benserazide or carbidopa) - dopamine cannot cross the blood brain barrier so needs to be in the form of levodopa, by inhibiting dopa decarboxylase we increase the level of levodopa reaching the brain for conversion of dopamine. Prevent peripheral breakdown of levedopa
Example: Co-beneldopa/Madopar

What are the four main modes of action of PD medications?
1) Dopamine replacement - Levodopa - converted into dopamine in the brain
2)Dopamine agonist - Ropinirole and rotigotine
3) Prevent dopamine degradation - COMT inhibitors, MAO-B inhibitors - Selegiline
4)Dopamine release based drugs - Amantadine
How can PD drugs precipitate compulsive disorders?
Dopaminergic drugs increase dopamine levels in the brain. Dopamine is responsible for compulsive behaviours and reward pathways, hence PD drugs can increase the risk for impulse control disorders, people become hypersensitive to reward e.g. can manifest as s*x addiction, binge eating, shopping, gambling addiction, uncontrollable repetitive behaviour which can impair quality of life
Why is it important to tell the DVLA if you are diagnosed with PD?
Parkinson disease can cause suddent onset of sleeping thus its key if individuals drive they inform their car insurance
What is the non-pharmacological management of PD?
Speech and language therapist - if swallowing, saliva or communcation challenge arise
Pysiotherpay help with motor function and balance issues
Occupational therapist - can help the patient with going about their daily activities
dietician - especially is swallowing is impaired
What are the side effects associated with levodopa and why does this occur?
When we use levodopa in the early days, we get good treatment response and the drug stays in the therapeutic window for quite some time. However, as parkinsons progresses, we get loss of dopaminergic neurons and so the therapeutic window shrinks. The duration of action of the drug reduces, and you will see a longer amount of time spent outside the therapeutic window. This means you will see a dyskinetic threshold resulting in involuntary movements
Why does the frequency of treatment need to increase as parkinsons progresses?
The frequency of treatment increases as parkinson’s progresses, this is because, as the disease progresses, we lose dopaminergic neurons, which means there are fewer dopaminergic neurons for L-DOPA to be packed in, which means the drug is used up more quickly. Therefore, in advanced parkinsons, we give the drug more frequently as the duration of action is reduced. Allows for the patient to maintain the therapeutic window for as long as possible
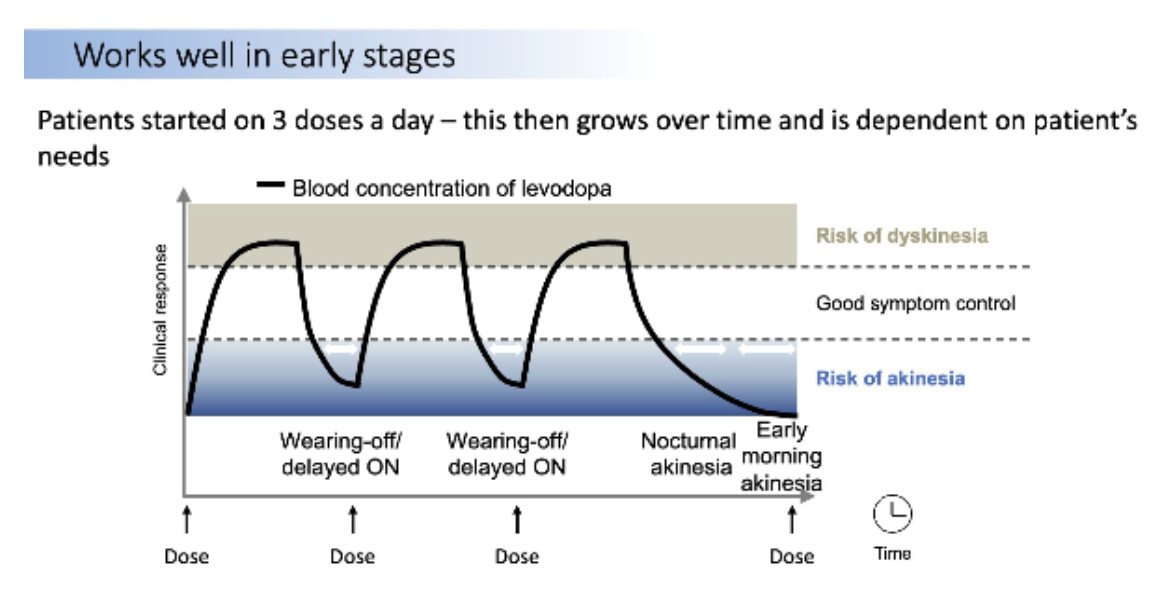
When PD worsens how does the therapeutic window change? and how does this affect symptoms displayed?
As Parkinson's disease worsens, the therapeutic window reduces as we loose dopaminergic neurons. As a result, we see dyskinesia which is a involuntary movements caused by excessive dopamine levels in the brain followed by akaensia which is inability to move - stiffened movements and no control over voluntary movements.
If a PD patient has dementia - how would we manage this pharmacologically?
Dementia - use acetylcholinesterase inhibitors such as rivastigmine or donepezil or galantamine
If a PD patient has psychosis - how would we manage this pharmacologically?
2nd generation antipsychotics as they block dopamine and serotonin receptors - because they block both are less potent dopamine blockers - quetipine or clozapine
If a PD patient has N&V - how would we manage this pharmacologically?
Nausea and vomiting - AVOID METOCLOPRAMIDE
Domperidone is preferred
Why can’t we use metoclopramide in PD?
Metoclopramide is a dopmaine antagonist which enters the BBB, hence will lower dopamine levels which is contraindicated in PD. Dromperidone is preferred does not act in this way

Describe the purpose for each drug here?
Levodopa - active - converted in dopamine
Carbidopa - prevents perhipheral breakdown of levopodopa - dopa decarboxylase inhibitor
Entacapone - COMT inhibitor - increases levodopa mechanism of action, slows breakdown of levodopa in the periphery so levodopa can reach the brain
Name an example of a MAO-B inhibitor?
Rasagaline or selegiline
True or false: the use of alzheimers disease medication in PD is unlicensed?
True, but if needed should be used - start with acetylcholinesterase inhibitors and then move to memantine (glutamate inhibitor)
How to manage patient with drooling of saliva in PD?
Ensure speech and language therapist intervention, If these fail offer:
Glycopyrronium bromide, botulinum toxin A (Ach blocker does not cross BBB)
What medication can be given for postural hypotension/orthostatic hypotension in PD?
Midodrine hydrochloride (1st line) (alpha-1-adrenoreceptor agonist used for vasoconstriction to increase BP) or fludrocortisone acetate (mineralocorticoid - causing sodium and water retention by kidneys to increase BP)
how would we treat symptoms of sleepines and sudden onset of sleep in PD?
Offer modafinil and review every 12 months - modafinil causes wakefulness