The Gastrointestinal System: Anatomy, Cephalic Phase, and Acid Secretion in the Gastric Phase
1/77
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
78 Terms
alimentary canal
secretion and motility in this facilitates digestion, also very rich in blood/lymph to absorb nutrients
digestive tube that extends from the mouth to the anus (mouth, esophagus, stomach, SI, LI, accessory organs)
small intestine
digestive organ where most chemical digestion and absorption of food takes place
accessory organs
rich in secretions, which go into GIT
salivary glands, gallbladder (storage), liver, pancreas
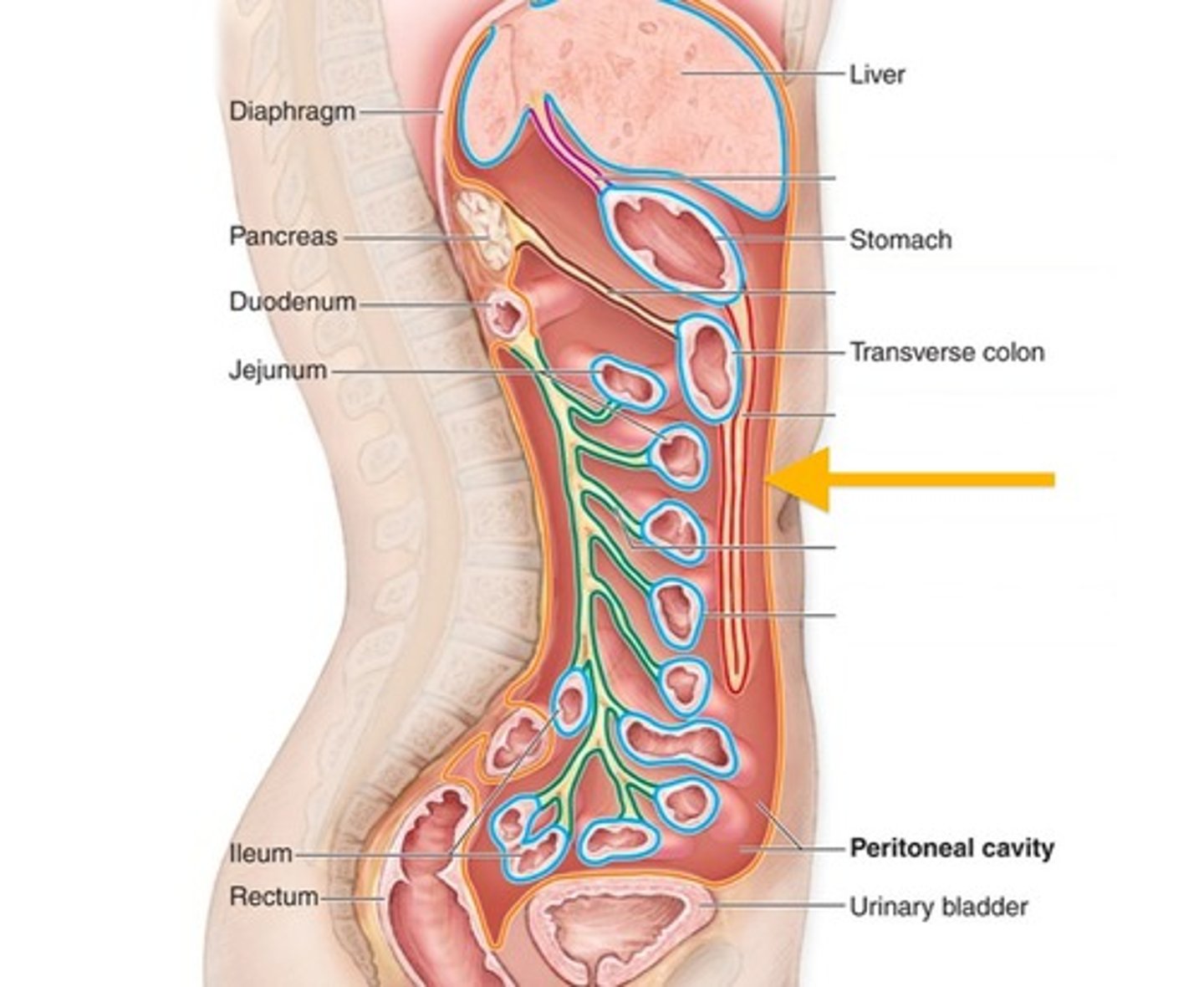
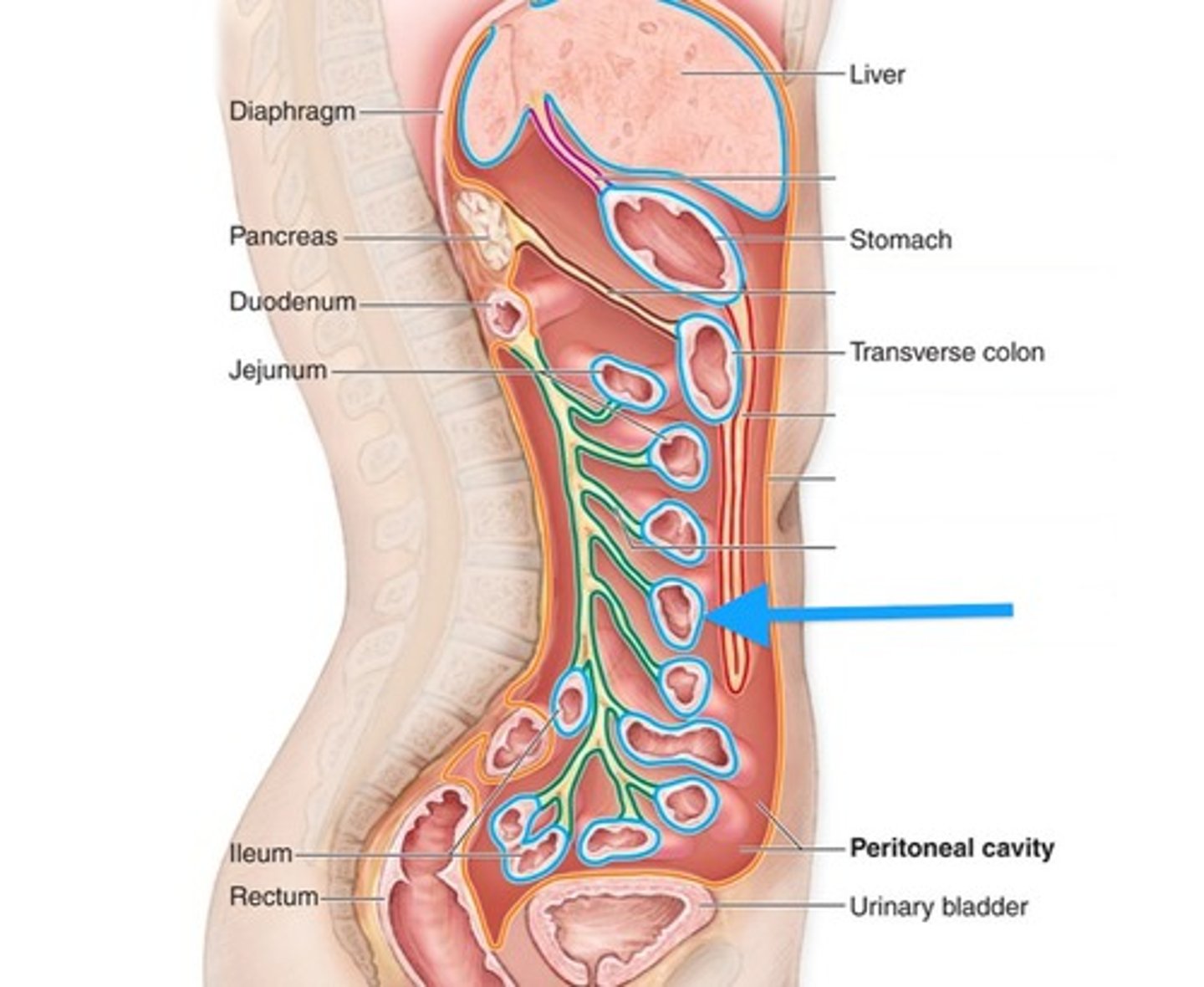
peritoneum
serous membranes within the abdominal cavity; secretes fluid into body cavity so you don't feel pain while it works
supports blood vessels, nerves, and lymphatic vessels
organs don't get tangled because of this connective tissue
parietal peritoneum
outer layer; inside the surface of the body wall
visceral peritoneum
surface of internal organs
peritoneal fluid
produced by serous membrane linings, provides essential lubrication allowing sliding without friction or irritation
intraperitoneal organs
completely housed within the 2 layers of the peritoneum
ex. duodenum (but rest of SI is retroperitoneal)
retroperitoneal organs
located behind the parietal peritoneum against the posterior abdominal wall
ex. pancreas, kidney
mesentery
continuous organ formed by the peritoneum (intraperitoneal) that supports and stabilizes the intestines
conduit for blood vessels, nerves, and lymphatics (provides blood/lymph/innervation)
"new organ," also has a role in diseases like Crohn's (autoimmune disease where small intestine is attacked)
transporting layer/mucosa (mucosal epithelial cells, exchange nutrients) → defense layer/submucosa (immune and blood vessel cells) → muscle layers/muscularis externa (muscle cells/contracting, motility and secretion) → protection layer/serosa (connective tissue)
order the histological layers of the GI tract from inner/lumen-facing to outer and what cell types make each up
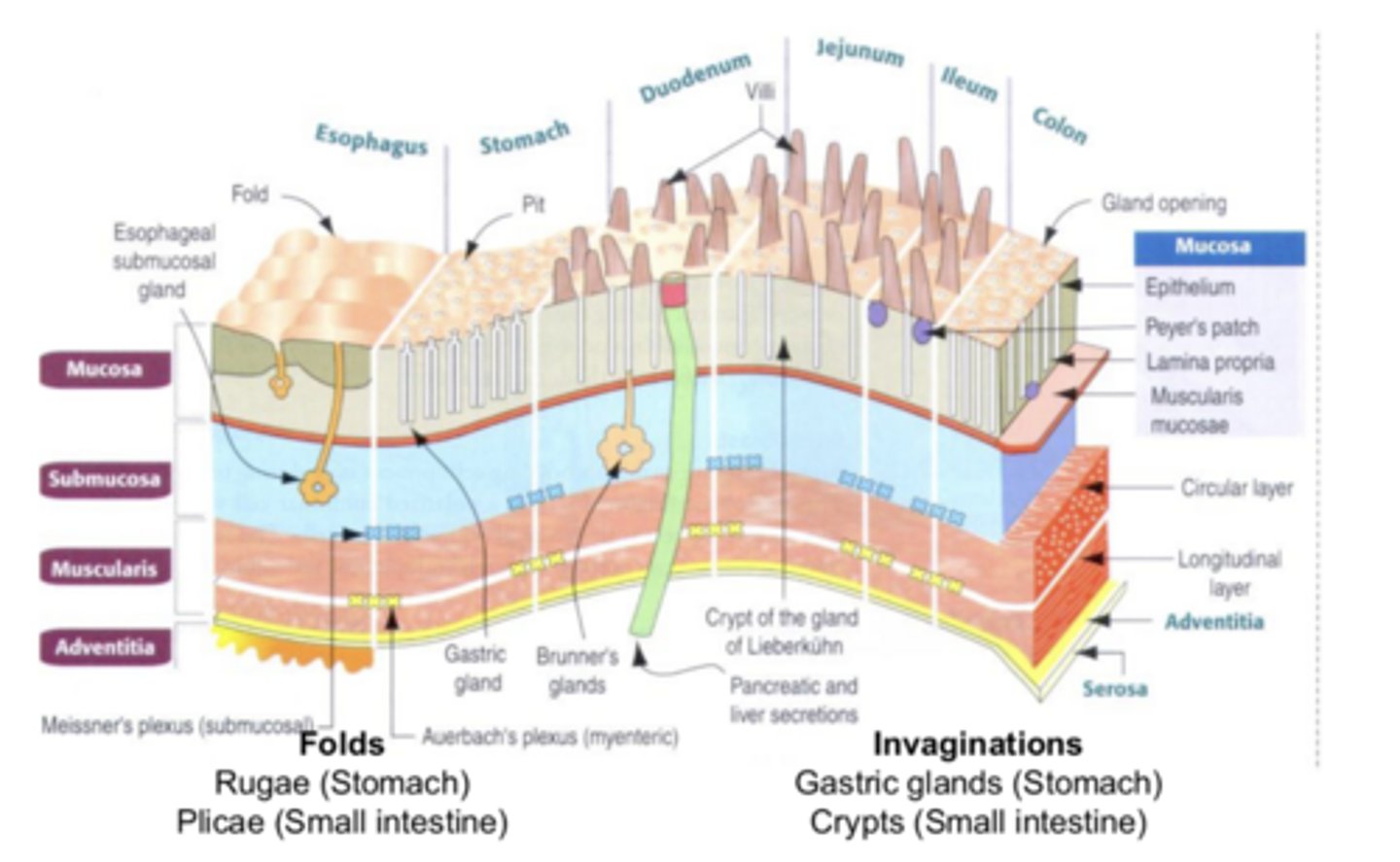
mucosal epithelium, lamina propria, and muscularis mucosae
***mucosa = important role in secretion, digestion, and absorption
what are the 3 layers of the mucosa from innermost to outermost?
mucosal epithelium
most variable feature in GI; enterocytes, endocrine, exocrine, GI stem cells
endocrine = hormones sent to cells/blood around it (local/distant signals)
exocrine = secretion of enzymes and other things to cell surface
enterocytes = cells that transport nutrients
GI stem cells = reproduce (**this is why certain therapies that affect highly reproductive cells hurts the GIT)
where/what do the 4 components of the mucosal epithelium perform?
lamina propria
connective tissue that contains nerve fibers, vessels, and lymph nodes
contains wandering immune cells (ex. Peyer's path)
muscularis mucosae
thin layer of smooth muscle that shapes the intestinal folds and moves the villi
villi
finger-like projections that provide surface area for nutrient exchange; found in small intestine
submucosa
loose connective tissue containing larger blood and lymph vessels; transports absorbed nutrients and is a defensive layer
submucosal plexus (Meissner's plexus)
nerve supply to muscularis mucosae
muscularis externa
responsible for the contractions we observe in the GIT; two layers of smooth muscle (inner/circular and outer/longitudinal) with the myenteric plexus bw them
inner layer of muscularis externa
circular muscle; when it contracts it decreases the lumen size
pinch when contracting
outer layer of muscularis externa
longitudinal muscle that stretches GIT; in peristalsis (in combination with the pinching), it contracts to make the tract shorter and make less area for the food to have to move along
shortens when contracting
myenteric plexus (Auerbach's plexus)
sits bw the two muscle layers of the muscularis externa and controls their coordinated movement by setting a basic electrical rhythm for contraction frequency
has pacemaker cells that fire slower than heart and are influenced by chemicals like hormones/neuro input
esophagus: has multiple layers of stratified squamous epithelium because it deals with a lot of stress (pushing unprocessed food, vomit)
stomach: because of stomach acid, it has deep pits for secretion and protection
small intestine: villi to increase SA
describe the unique histological features of the esophagus, stomach, and SI
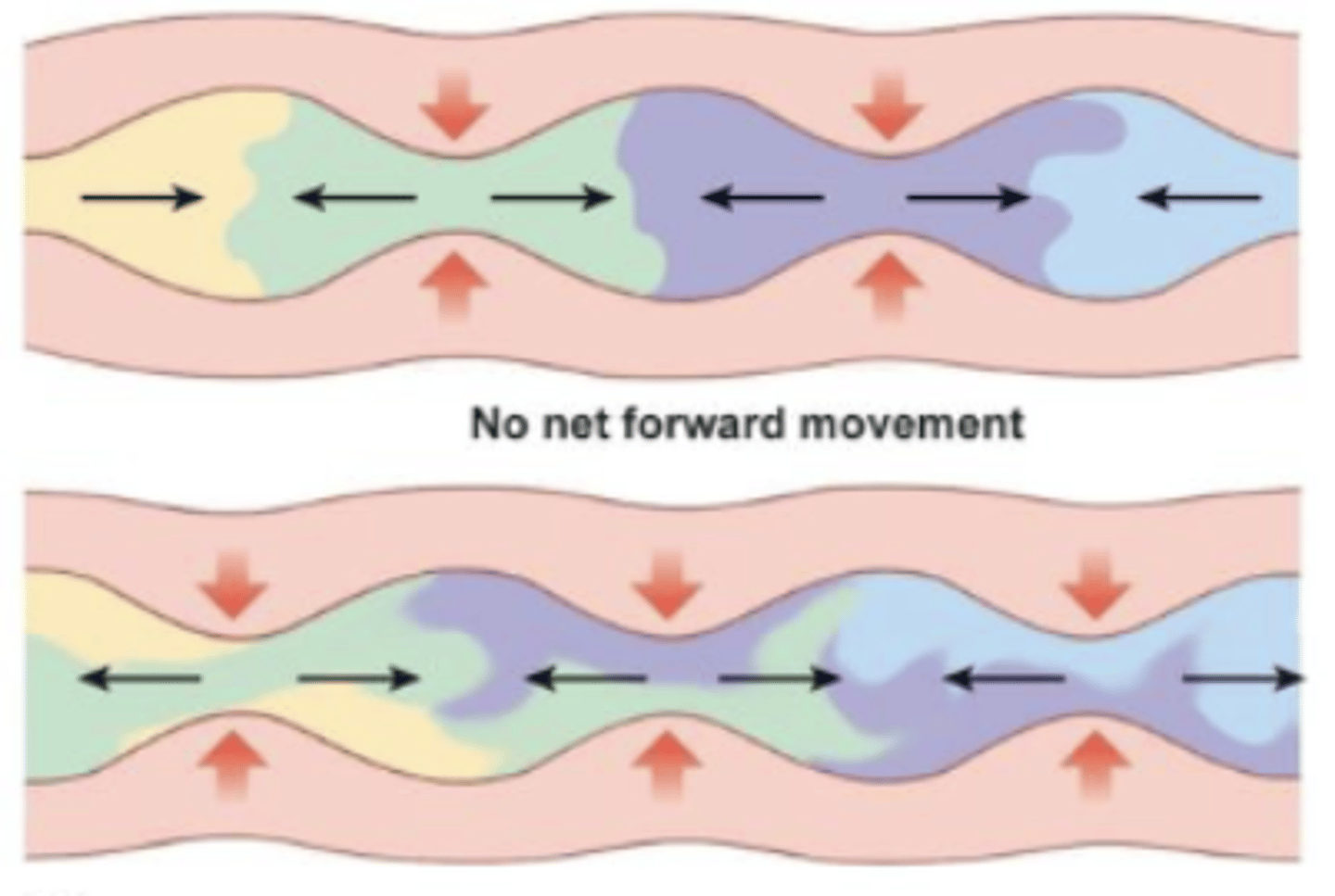
peristalsis and segmentation
what are the two types of (spontaneous) GI smooth muscle contraction?
peristalsis
moves food along; site you want to leave contracts, distance needs to move shortens, site you want to go to relaxes
occurs in esophagus and stomach, NOT SI bc it needs plenty of time for reabsorption into epithelial cells
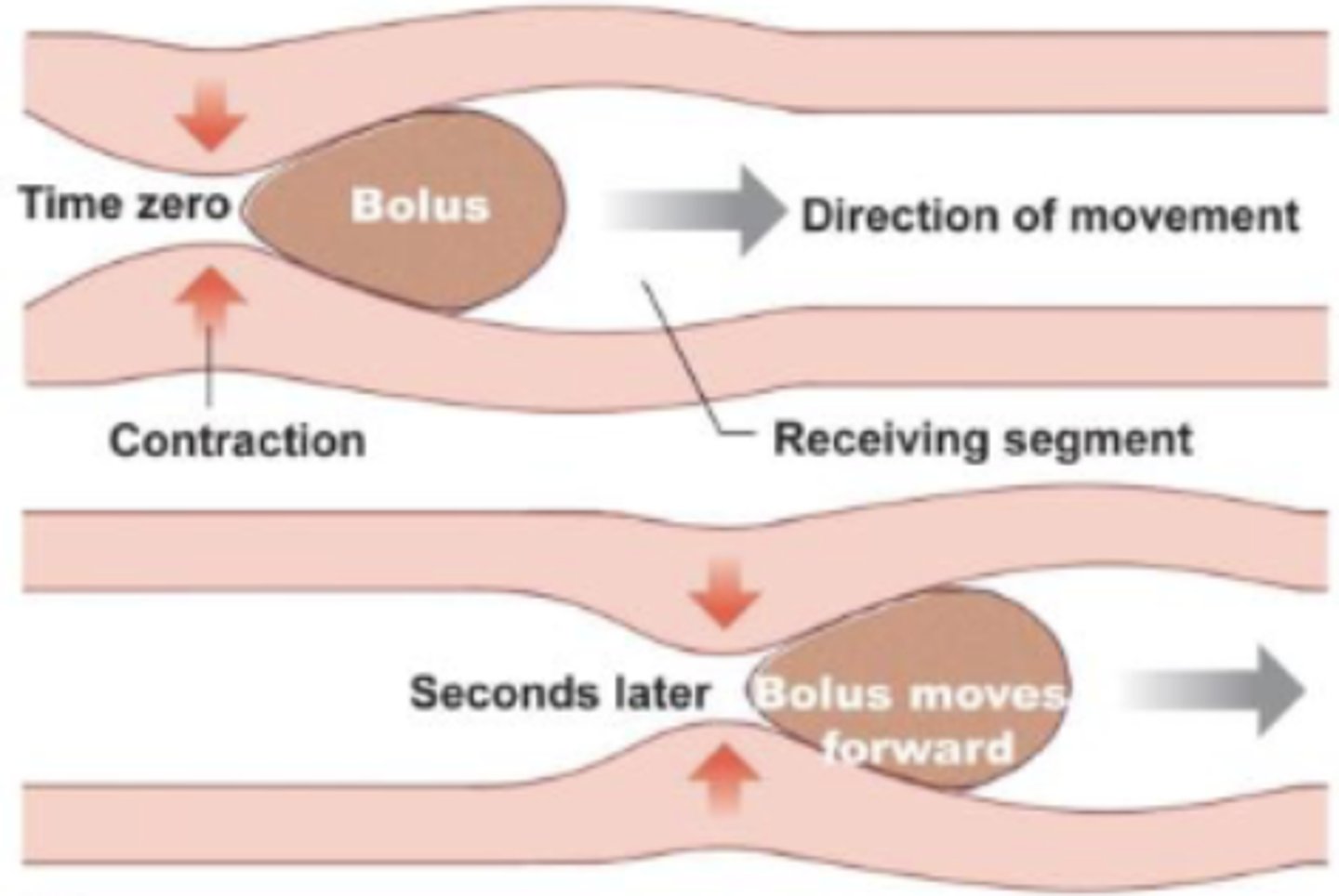
segmentation
mix food and break it down; adjacent areas of GIT alternate relaxing and contracting
mixing with enzymes occurs in small intestine
interstitial cells of Cajal
pacemaker cells (modified SM cells) that produce basic electrical rhythm (BER) to set the contraction frequency of GI smooth muscle; located bw the two muscle layers
sets slow waves (3-20 sec), but diff pace in diff regions of GIT bc of isolated membrane potential (ex. slow in stomach, varied in SI)
can be influenced by chemical input
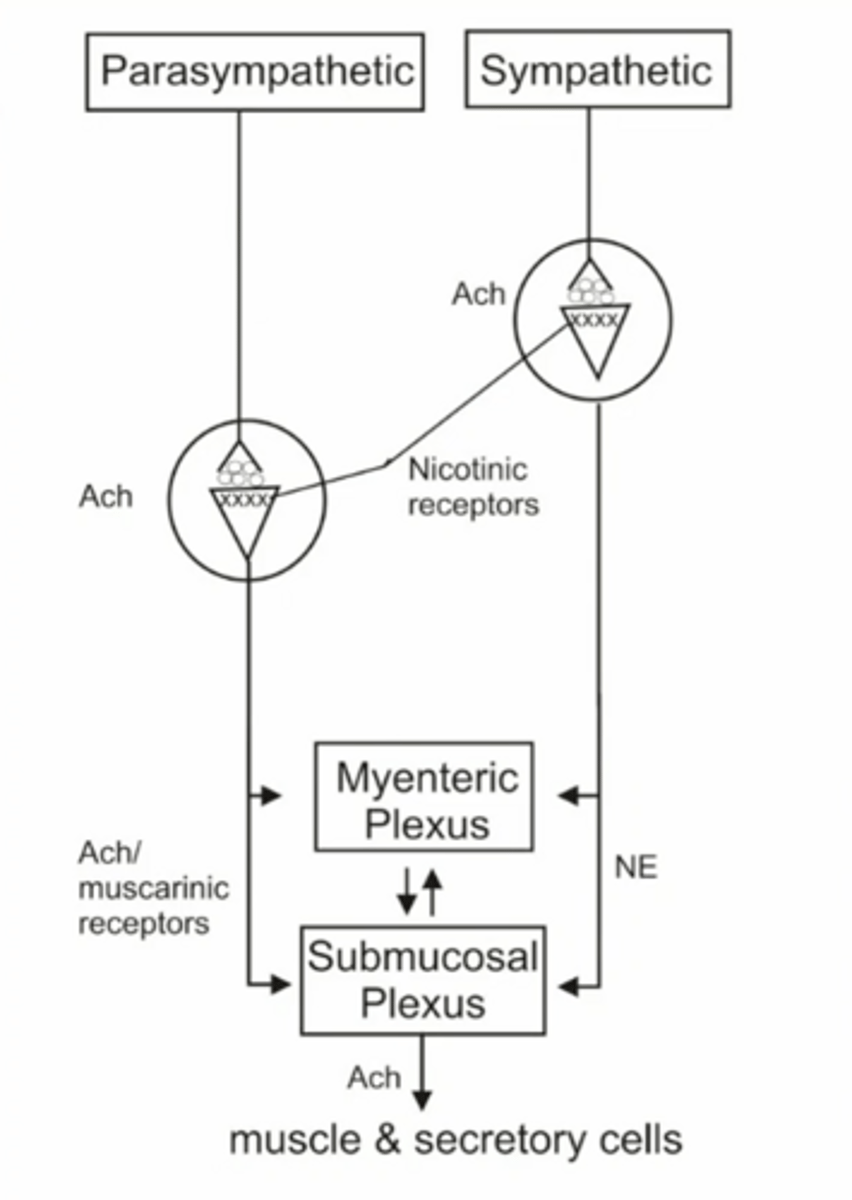
enteric nervous system
nervous system of the GIT (can act independently) that controls secretion and motility and is linked to/shares many features with the CNS
has an integration center (intrinsic neurons), glial cells (support), and responses to many NTs and GI peptides to affect motility and secretion
parasympathetic and sympathetic innervation
***parasympathetic nerve activity controls motility and secretion (rest and digest), which accomplishes other functions of GIT
what kind of innervation does the GIT receive?
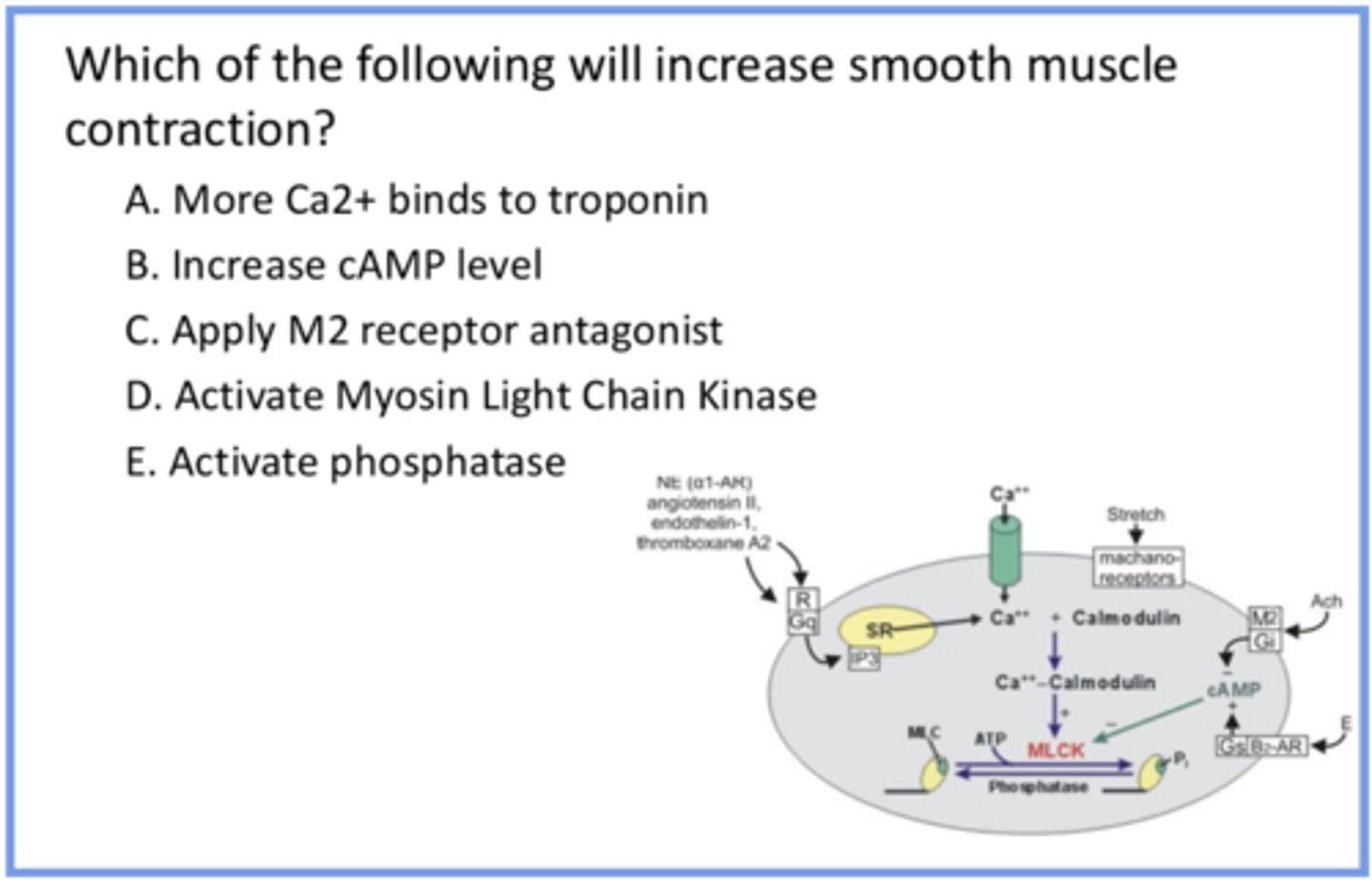
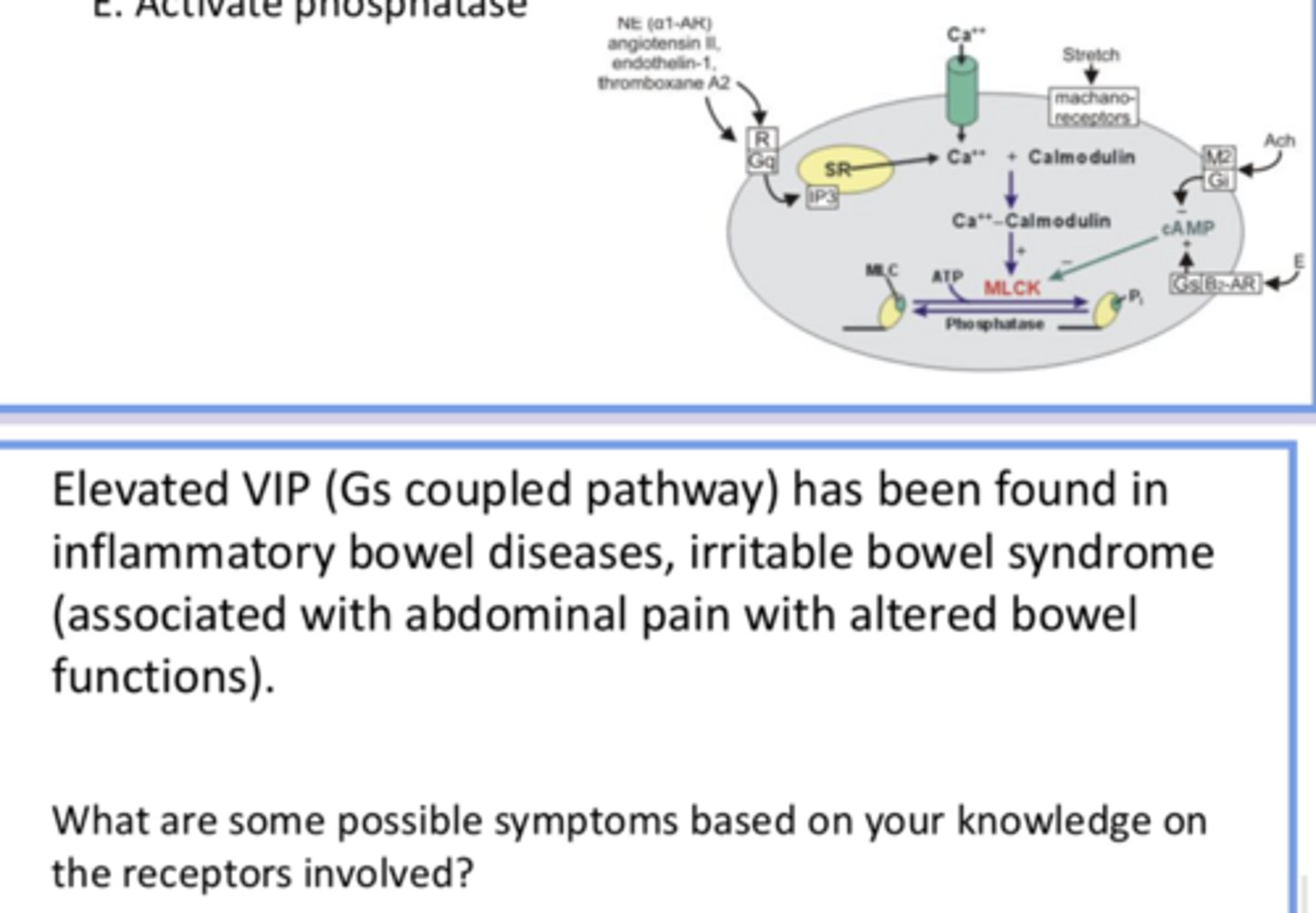
Not A because smooth muscle has MLCK instead of troponin
Not B bc cAMP inhibits MLCK (causing relaxation)
Not C bc it results in more activity of cAMP (bc M2 normally inhibits cAMP, so inhibiting it would lead to less inhibition of cAMP and thus MLCK) which has the same outcome (parasympathetic activation via ACh = more smooth muscle contraction to facilitate digestion)
D bc activating MLCK leads to contracting
Not E bc phosphatase does the opposite of MLCK
knowing that chemical signals regulate smooth muscle, answer the question and provide reasoning for all answer options
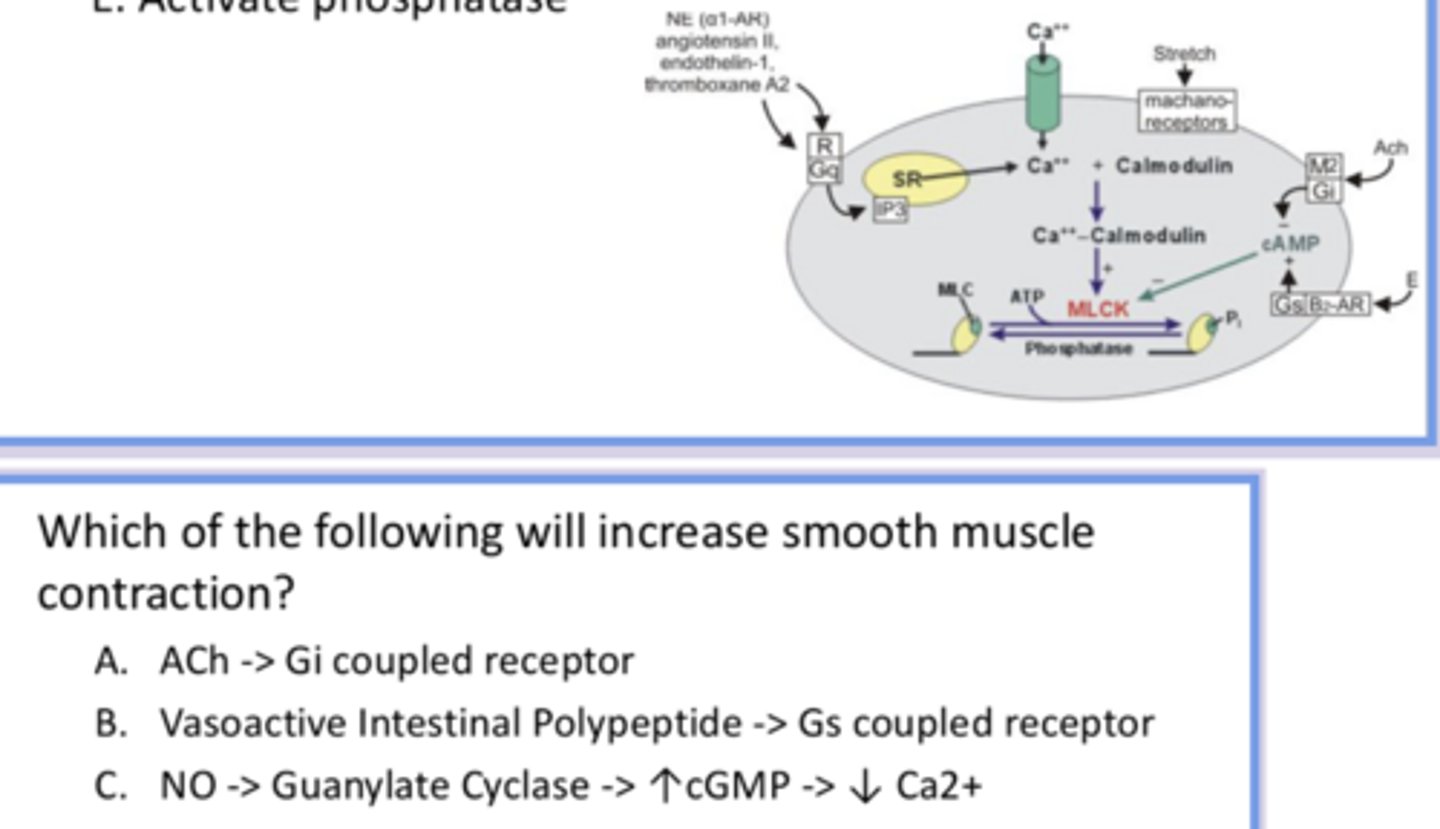
A bc ACh activates contraction, and Gi inhibits cAMP (which decreases inhibition on MLCK and increases contraction)
Not B bc Gs activates cAMP
Not C bc this pathway leads to less Ca available for contraction
answer the question and provide reasoning for all answer options
elevated Gs coupled pathway = more relaxation of smooth muscle → less movement of food through GIT and sphincters open too much, leading to overly frequent bowel movements/pain from food buildup and bloating
Gs coupled pathway leads to less motility and increased secretion
***Secretory and muscle cells' response to VIP/Gs pathway is diff!
→ reduced motility = abdominal bloating, distension can cause pain
→ increased GI secretion (Cl-) = watery diarrhea
answer the question and provide reasoning for all answer options
cephalic phase
only long loop reflex in GI system; involves integration in the brain (while other processes are locally controlled)
involves the function/secretion of saliva and the swallowing reflex
saliva
softens and lubricates food, involved in chemical digestion and taste, offers protection
protection = lysozymes (innate immune response), immunoglobulins (IgA, adaptive immune response), fluoride (teeth strength), HCO3
salivary amylase and some lipase are in this → digest carbohydrates
we have 3 pairs of salivary glands and secrete 1-1.5 G of saliva every day
autonomic NS impacts salivation, especially parasympathetic
how many saliva glands do we have, and what impacts their secretion?
parotid glands
salivary glands that produce a watery solution
sublingual glands
salivary glands that produce secretion rich in mucus
submandibular glands
salivary glands that produce mixed secretions
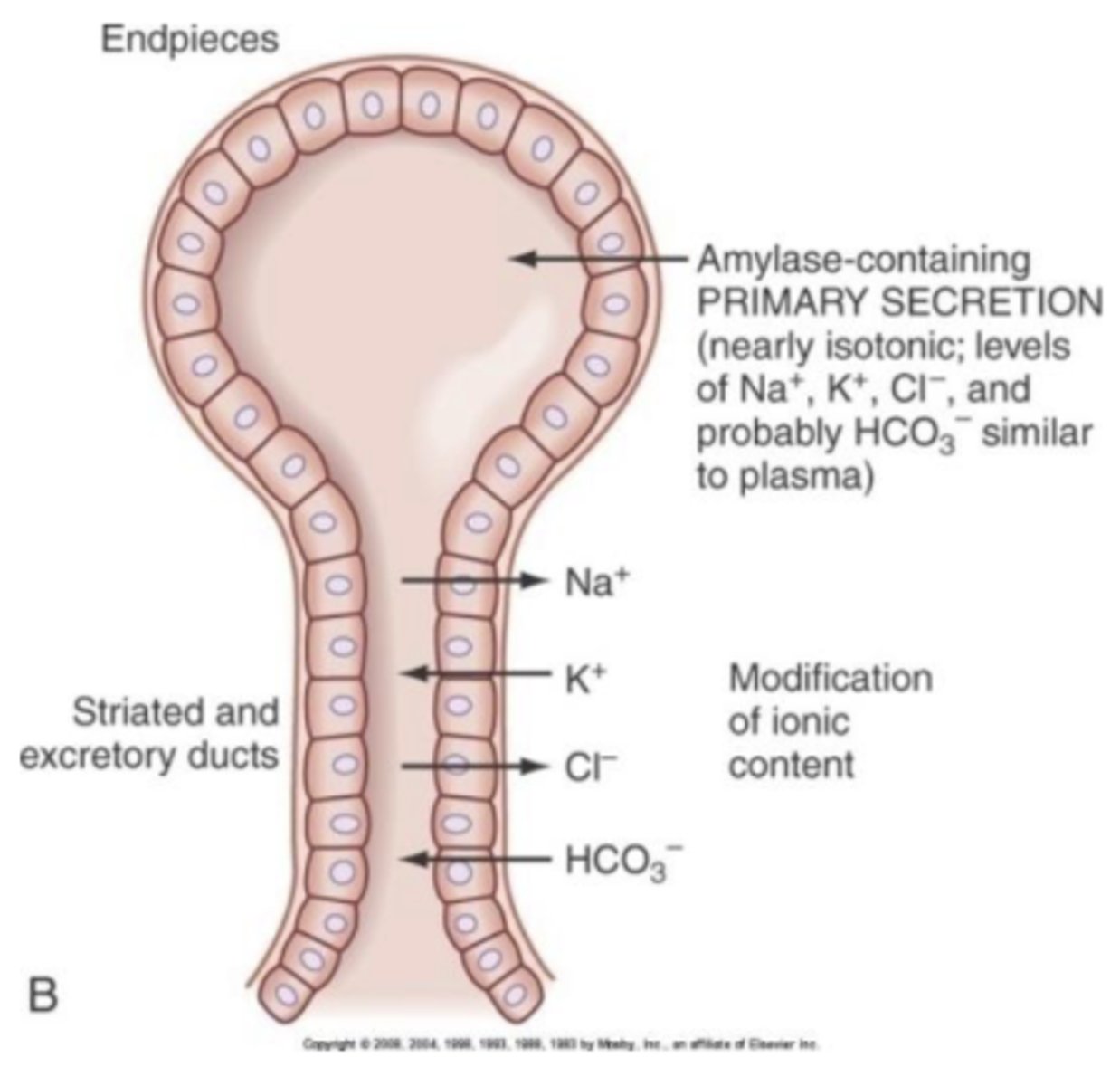
acinar cells and ductal cells
what are the two epithelial transport steps/cell types involved in salivary secretion?
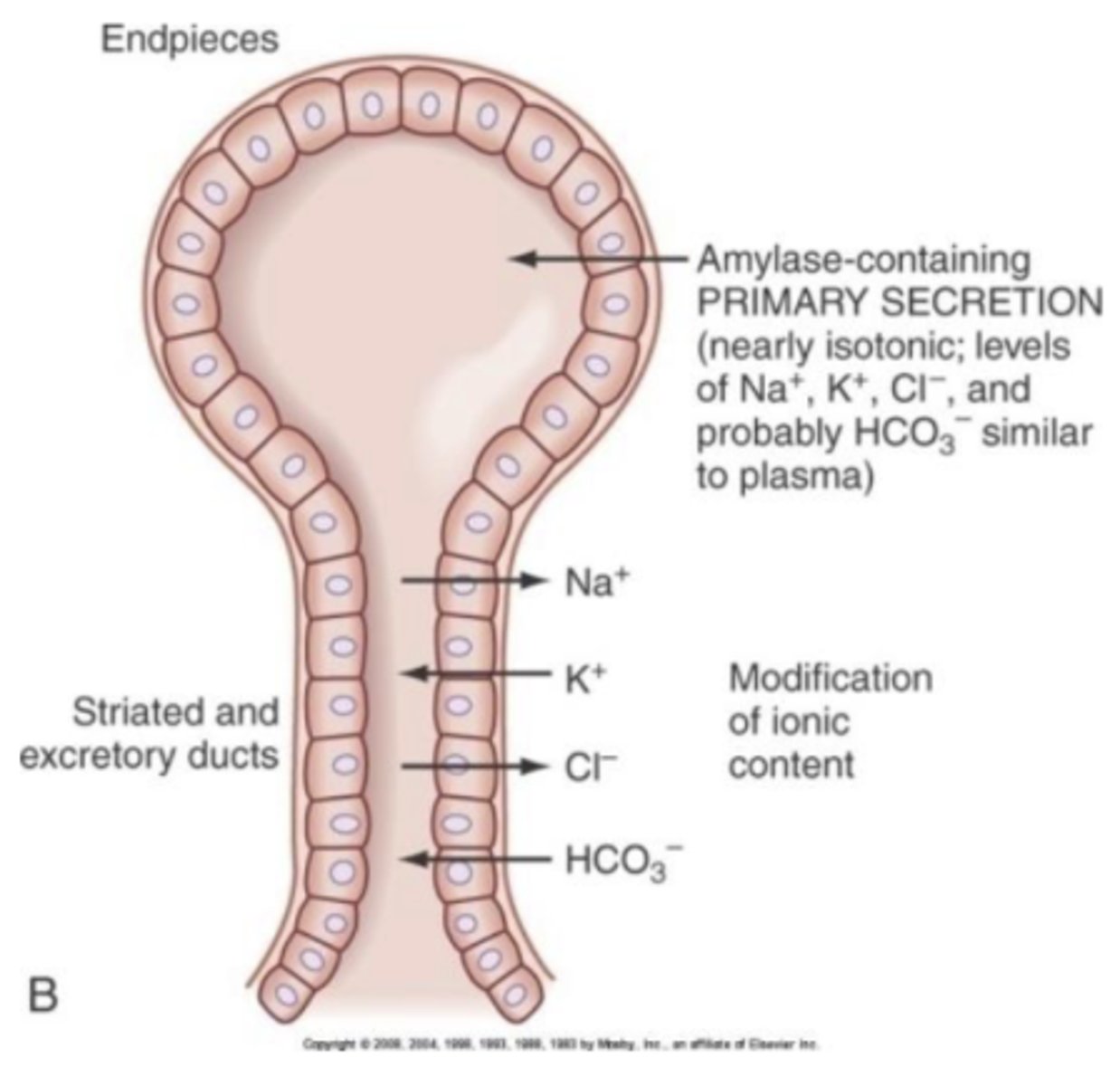
acinar cells
secrete fluid that resembles extracellular fluid → high in Na and Cl, low in K and HCO3
found in the endpiece (bulbar part of the salivary gland)
K is found mostly intracellularly instead
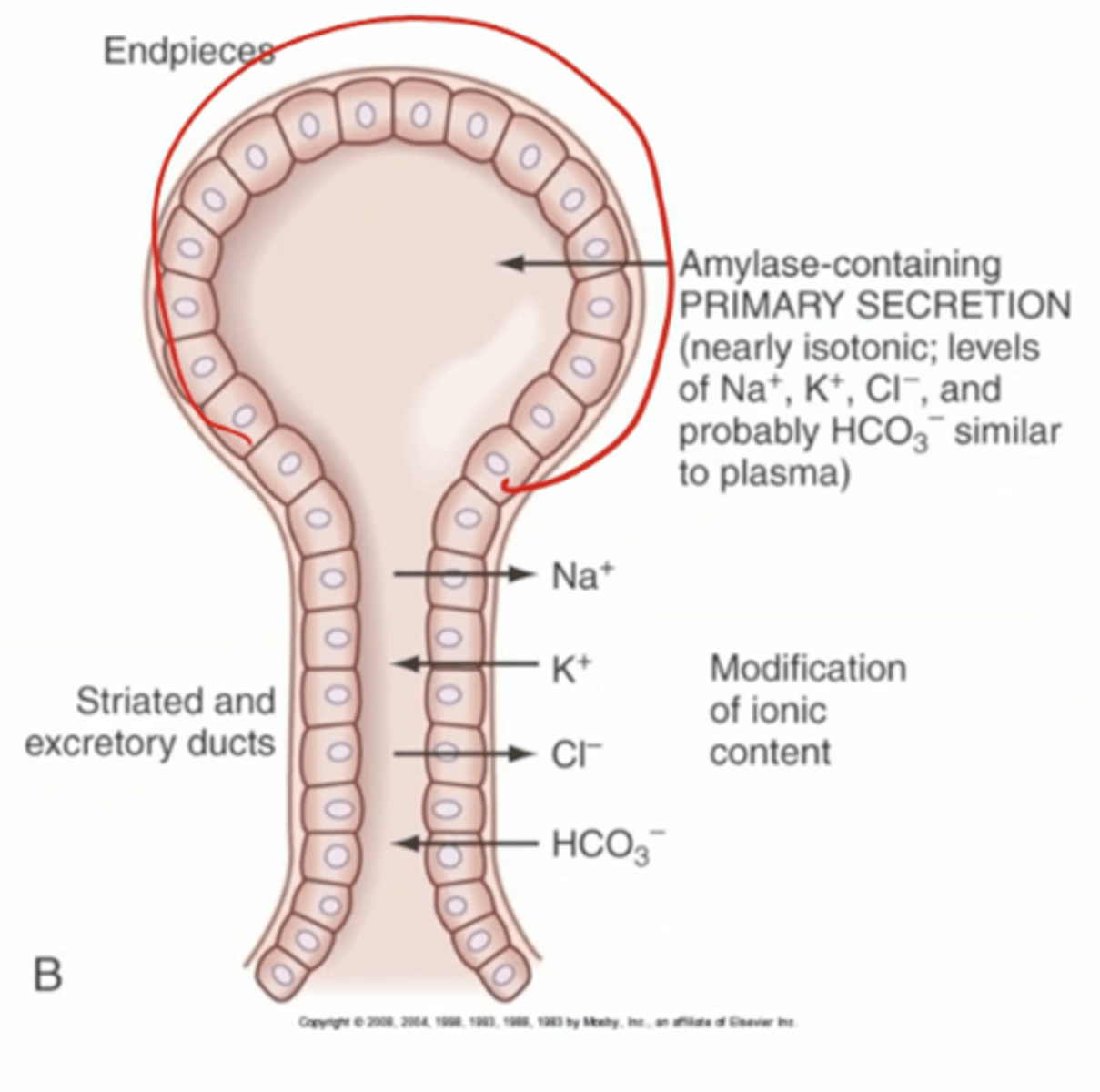
ductal cells
absorb (remove from saliva) Na+ and Cl-, secrete K+ and HCO3- into saliva, net removal of solute, impermeable to water
where ductal modification (alteration of saliva ionic composition) occurs in the excretory ducts (shaft part of the salivary gland)
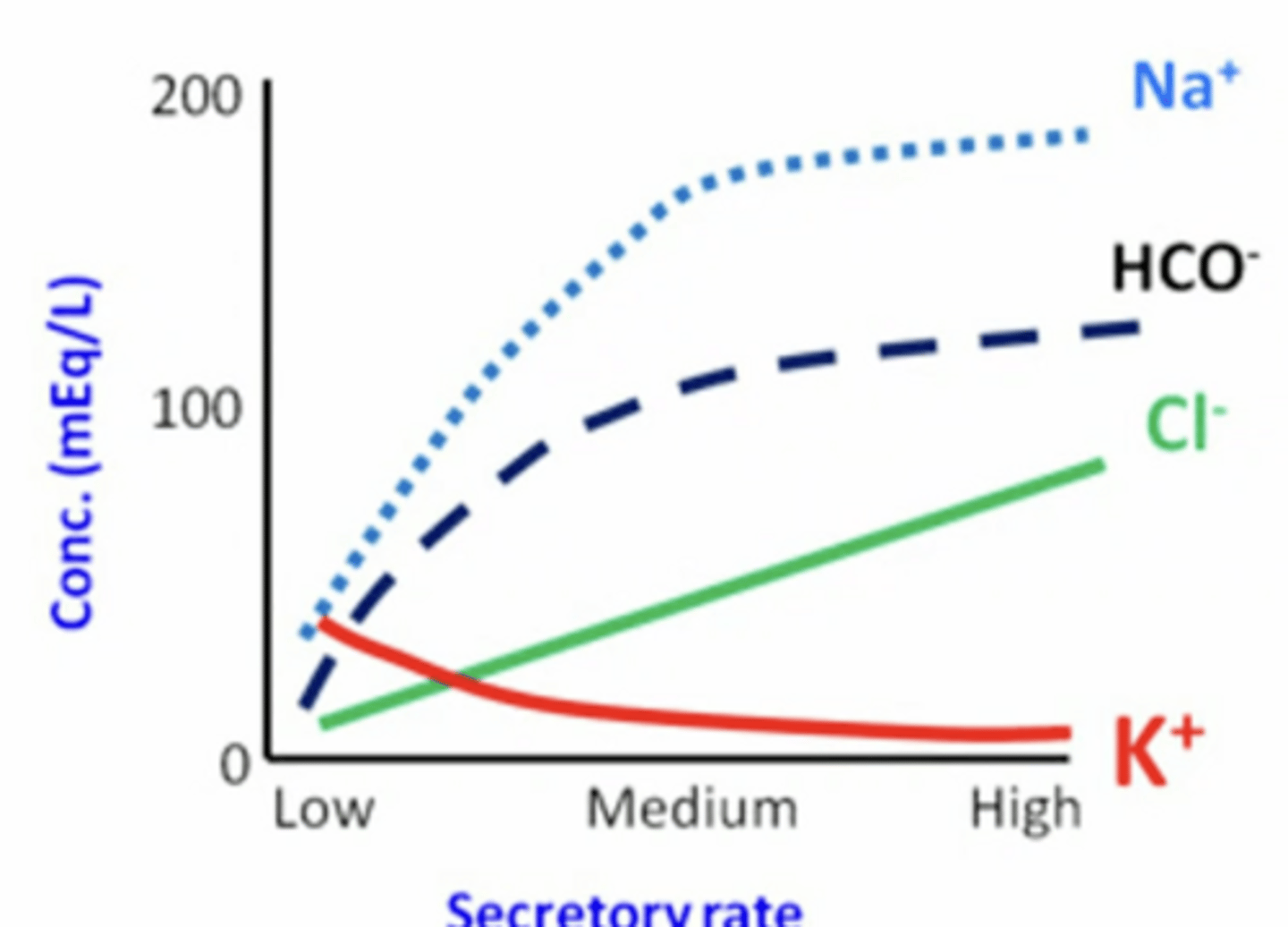
during stimulation (salivation) ductal modification reduces bc there’s not enough time for ion movement away from where it is typically found to move in/out of saliva (from/to blood)
Na and Cl concentration increase (Na > Cl) (not time for Cl or Na to be removed from the saliva)
K concentration decreases (not time for K to be excreted into the saliva)
[HCO3-] remains high bc of secretagogues (Cl < HCO3 < Na)
compared to a low rate of saliva secretion, when you are chewing what happens to the concentration of Na, Cl, K, and HCO3?
secretagogues
mechanism that stimulates secretion
unique chemical signal that also stimulates HCO3 increase in response to increased salivation; when cells are activated to salivate they also release HCO3, which is why HCO3 increases during chewing
gland is made of epithelial cells
top bulb part (endpiece) = made of acinar cells; where secretion occurs
bottom shaft part (duct) = ductal cells; where modification occurs
blood vessels run above bulb part, and dilate when salivating to allow fluid exchange
describe the parts of the salivary gland
swallowing reflex
tongue pushes bolus against soft palate and back of mouth, triggering this → upper esophageal sphincter relaxes when epiglottis closes to keep swallowed material out of the airways → food moves down into esophagus, propelled by peristaltic waves and aided by gravity
epiglottis
separates trachea off from GIT to prevent food from getting lodged in it; gets closed when food is pushed against it
trachea
has soft bit of tissue so when food is pushed through the esophagus against it it doesn't create resistance
primary peristalsis → secondary peristalsis occurs if food doesn't move all the way through (repetition only when necessary)
coordinated with lower esophageal sphincter to allow food into stomach
doesn't rely on gravity (though it helps)
what kind of muscle contraction occurs in the esophagus?
gastroesophageal junction
lower esophageal sphincter has a resting pressure of about 30 mmHg → higher pressure than stomach to make sure food doesn't backflow
pressure reduces (loosens sphincter) due to alcohol, caffeine, cig smoke, chocolate
gastroesophageal reflux disease (GERD)
pathology where lower esophageal sphincter pressure decreases because it is looser
can be caused by excessive vomiting
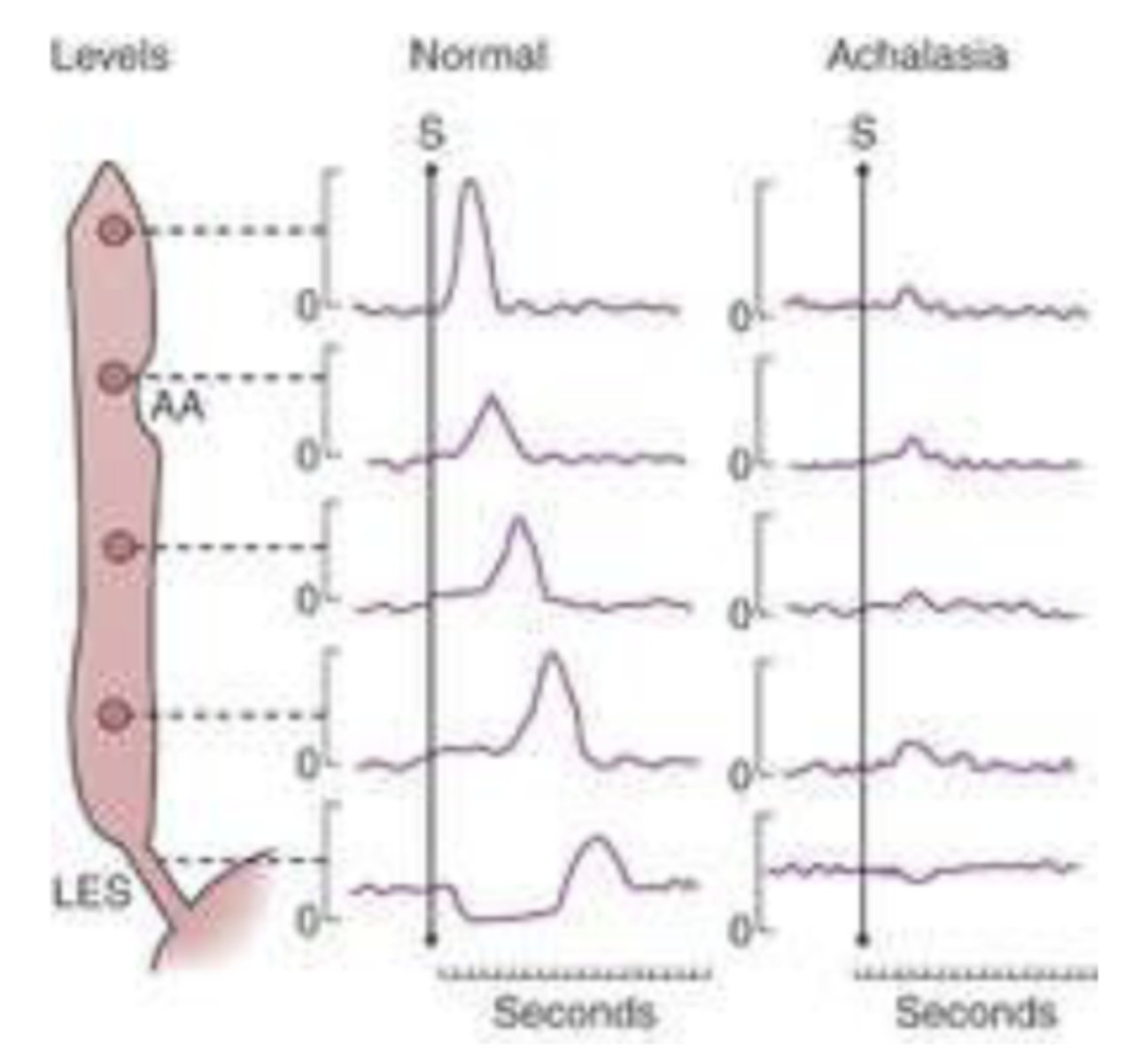
achalasia
pathological condition involving increased pressure of the esophageal stricture/sphincter → you won't be able to fluctuate from baseline pressure as much which makes the passageway more restrictive and thus prevents food from going down
nerve cells (myenteric plexus) innervating esophageal muscle degeneration
symptoms include solid dysphagia (weak peristalsis), fullness in chest while eating, chest pain, and weight loss
baseline pressure is higher (making peaks look smaller)
synchronized "peaks", but normally they fall in more of a cascade bc if it all contracts at once you can't contract down the pathway
smaller peaks and poor contraction causing little movement of food
last peak is inverted because you relax, not contract, to allow food to move into stomach (but inversion is smaller in achalasia)
what would a graph tracking the change in pressure during the process of swallowing food down the esophagus look like in achalasia (in comparison to baseline)?
gastric phase
series of short reflexes initiated when food enters the stomach; involves secretion and motility in the stomach (which occur in distinctly in its anterior and posterior regions)
anterior/proximal stomach
reservoir (relaxes to store food and liquids); includes the cardia, fundus, and body
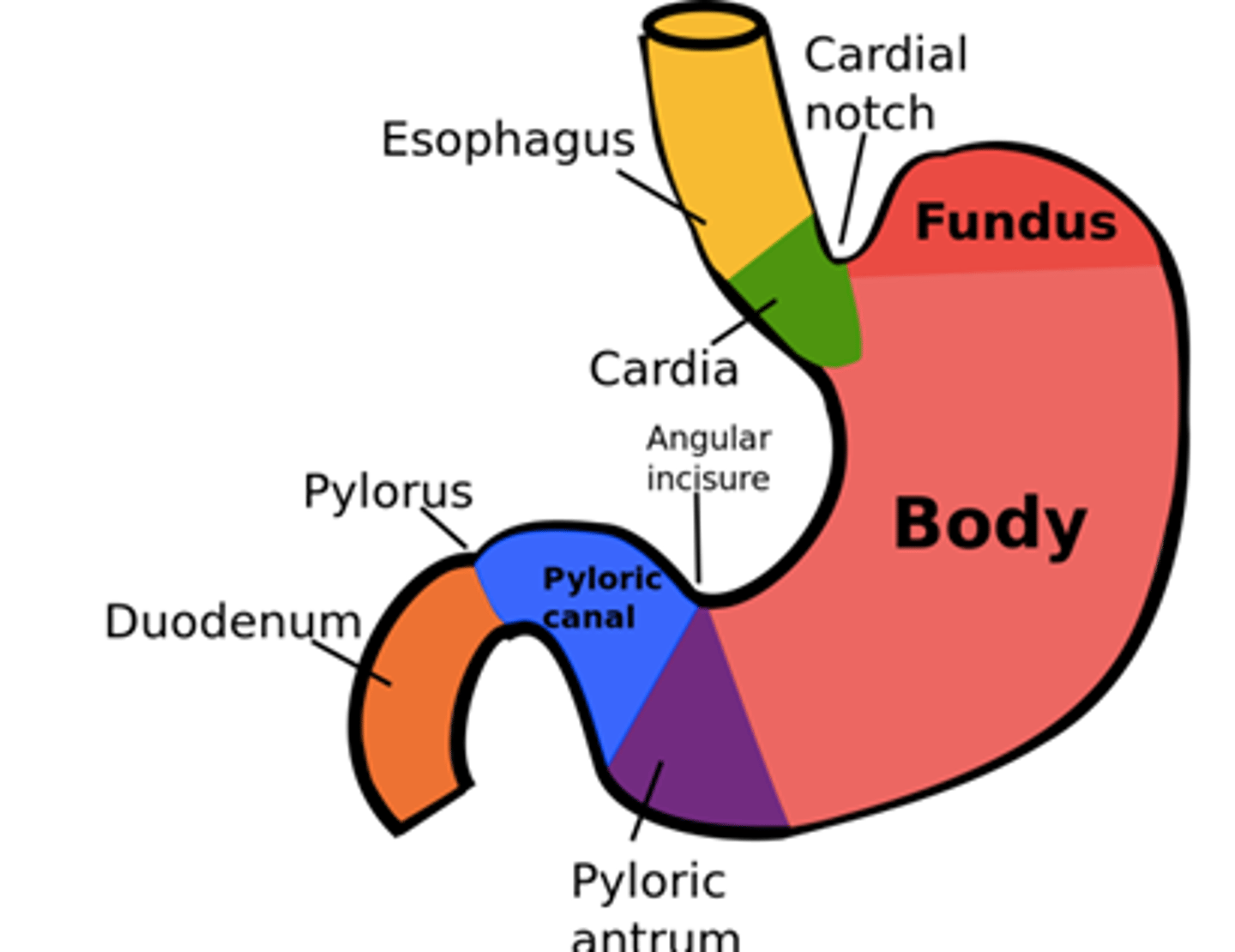
posterior/distal stomach
pump/grinder where food is churned; where peristalsis occurs (which functions to mix in the stomach)
includes the antrum (pyloric region) and pyloric sphincter
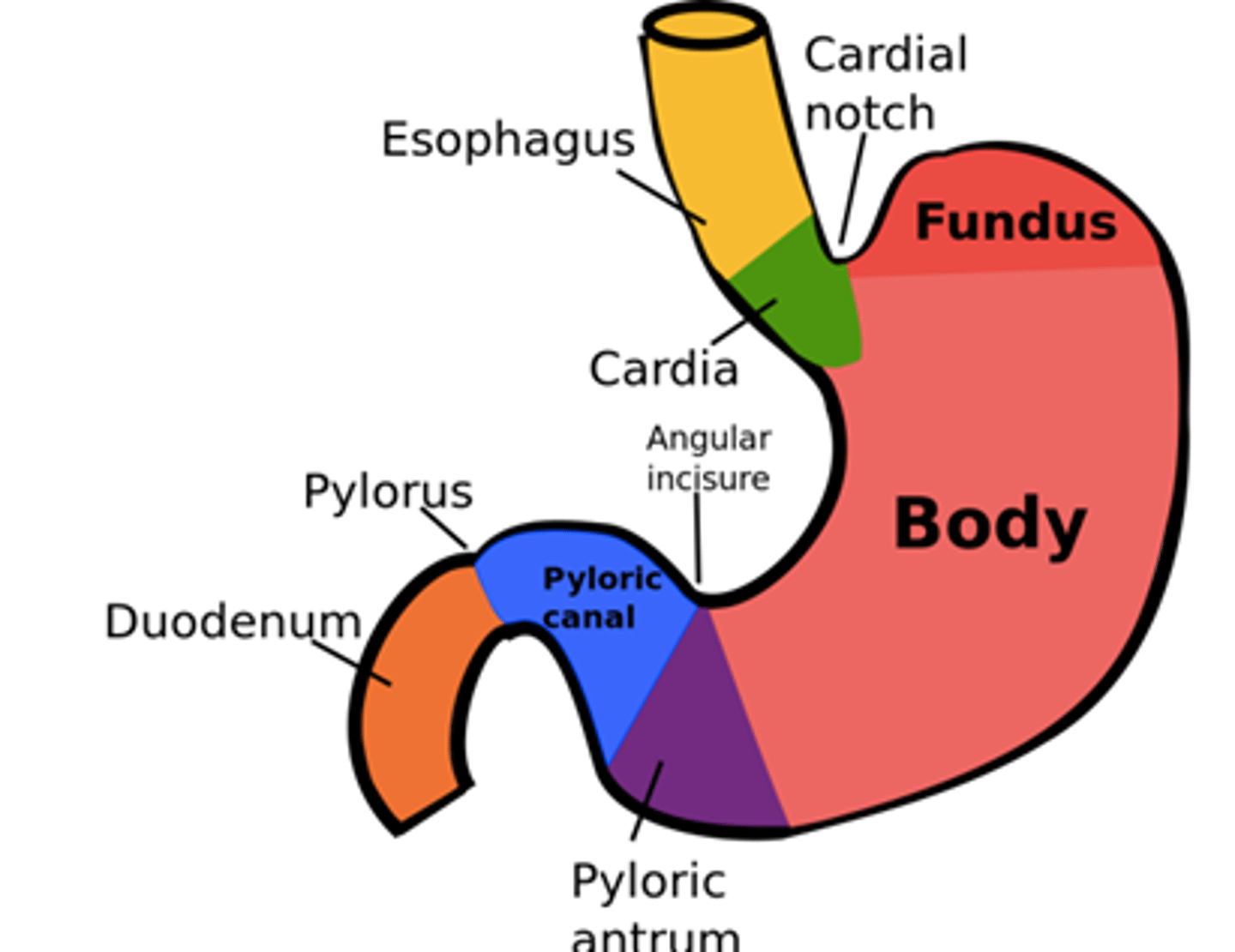
rugae
unique structure of the stomach, which are folds that allow the stomach to expand when you eat a lot
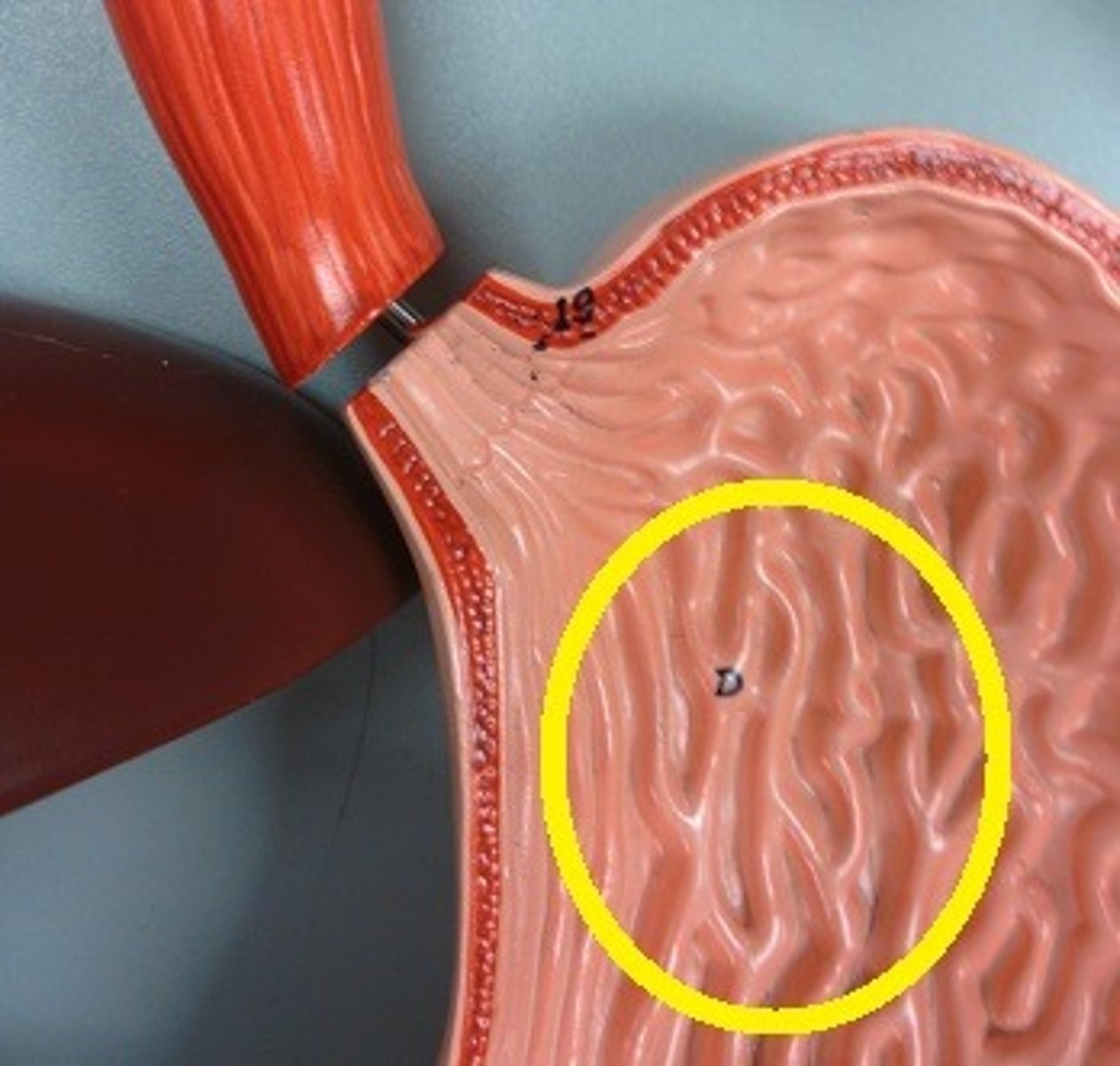
oblique layer
unique structure of the stomach, which is a third smooth muscle layer to give the stomach more strength and integrity (other 2 are inner circular layer and longitudinal layer)
lots of motility and mixing occurs in the stomach
LES (esophagus) and cardia of stomach
have mucus and HCO3 (provide protection)
motility = prevention of reflux, entry of food, and regulation of belching
fundus and body of stomach
have mucus and HCO3 (provide protection), but also pepsinogens, lipase, intrinsic factor, and H+
motility = being a reservoir and tonic force during emptying
antrum and pylorus of stomach
have mucus and HCO3 (provide protection)
motility = mixing, grinding, sieving, and regulation of emptying
acid, gastrin, paracrine, and enzyme
what are the 4 types of gastric secretion?
acid secretion
parietal cells in the gastric glands secrete acid
H2O and CO2 converted to HCO3 and H+ by carbonic anhydrase
proton pump bc it is ATP dependent, not dependent on environment around cell → this drives homeostasis and determines the environment/rate of everything else
more H+ pumped = you need to increase CO2 and water (bc of equilibrium equation: H2O + CO2 <--> HCO3 + H)
***HCl concentration never increases intracellularly though because it can damage the cell/membrane --> the protons and Cl are pumped out of the cell into the lumen where HCl is formed
what is the rate limiting part of acid secretion (how much HCl can be made)?
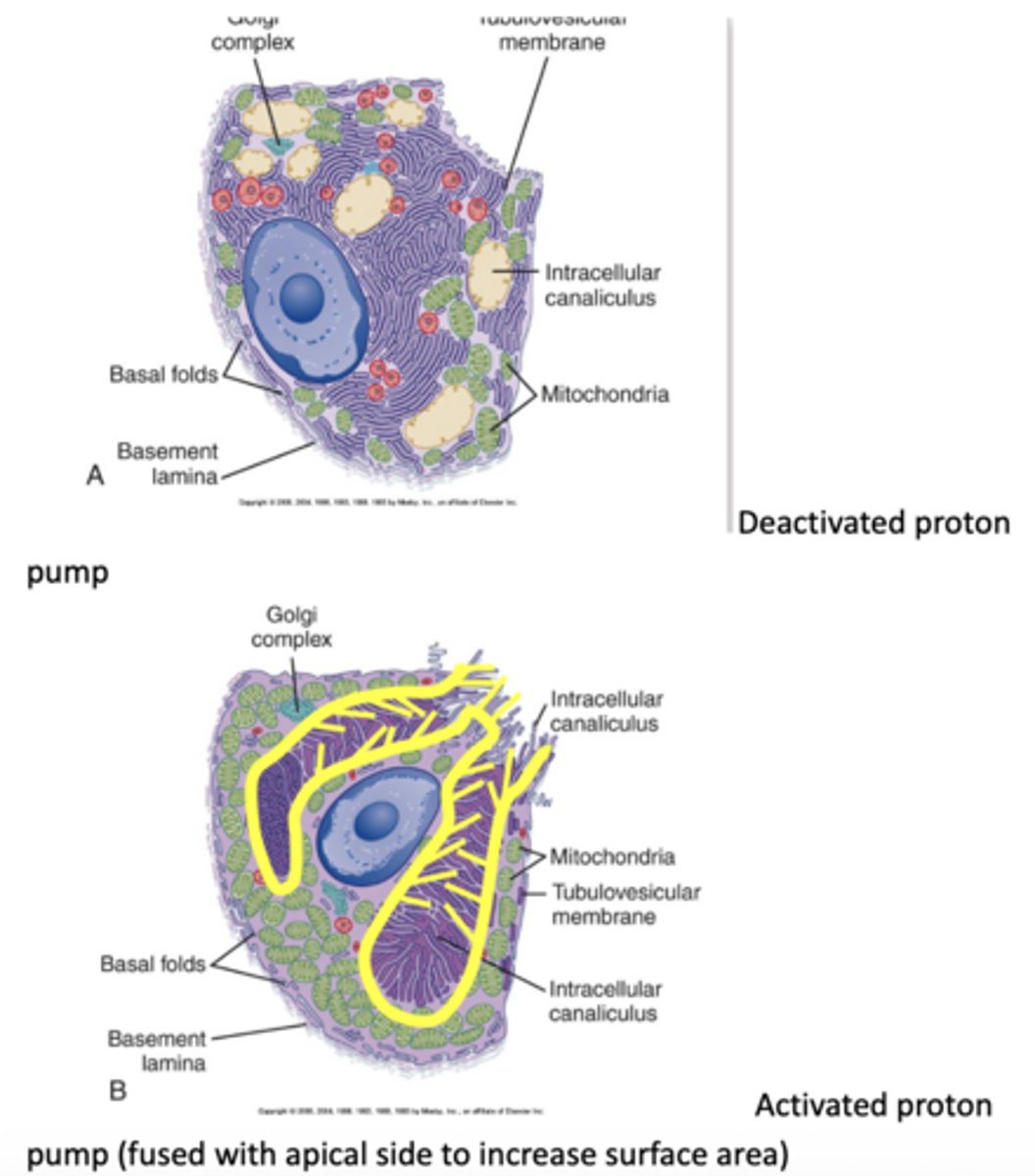
during eating the tubovesicular membrane and intracellular canaliculus merge ("fuse"), which pushes the tubovesicular membrane and its proton pumps up to apical surface (which has few proton pumps) and exposes it to the lumen
before you fuse, the proton pumps on the tubovesicular membrane have no access to the lumen so they are "inactive" → when you fuse with the intracellular canaliculus (which acts as a reservoir for the tubovesciular membrane to fuse with the apical side) you provide surface area to the lumen where exchange can occur, thus activating the proton pumps
describe how the proton pump is "activated" in the stomach parietal cells to facilitate acid secretion
gastrin
hormone secreted in the stomach that stimulates acid secretion
cAMP
second messenger system, meaning it activates protein kinase A → activates cell membranes
in GIT secretory cells increasing this means you have more fusion of the membranes and more acid production (more secretion), but in smooth muscle cells this inhibits contraction
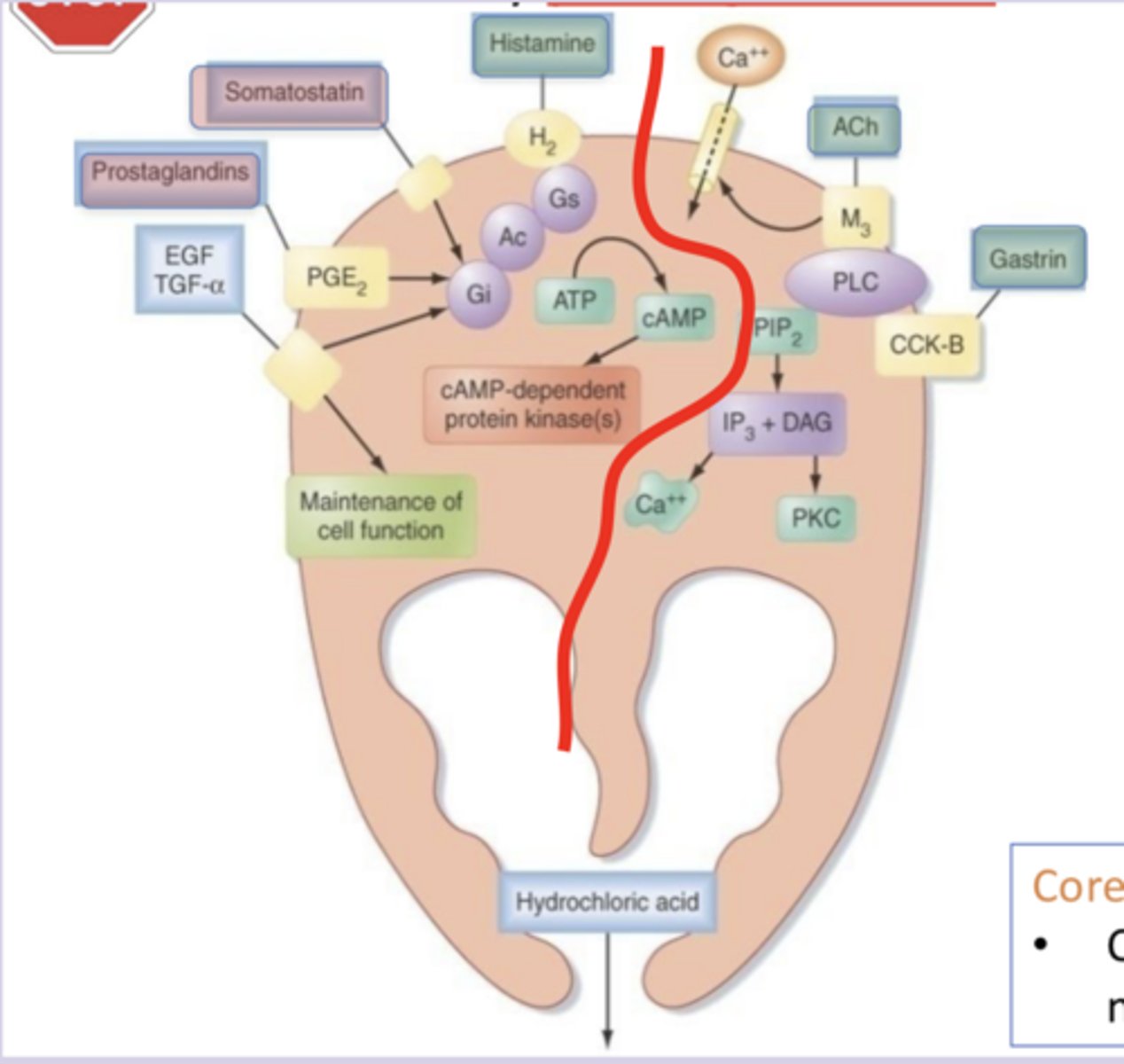
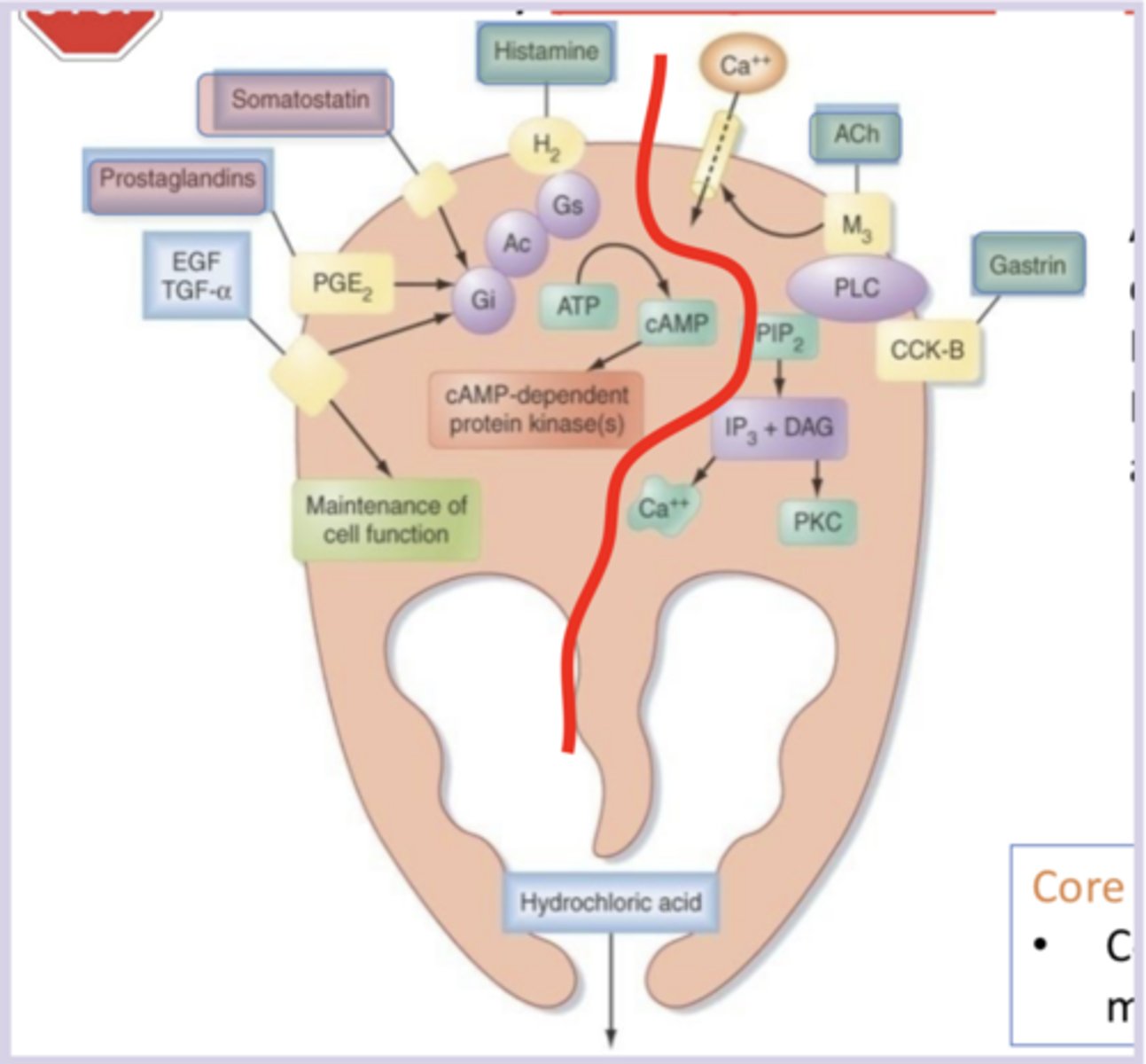
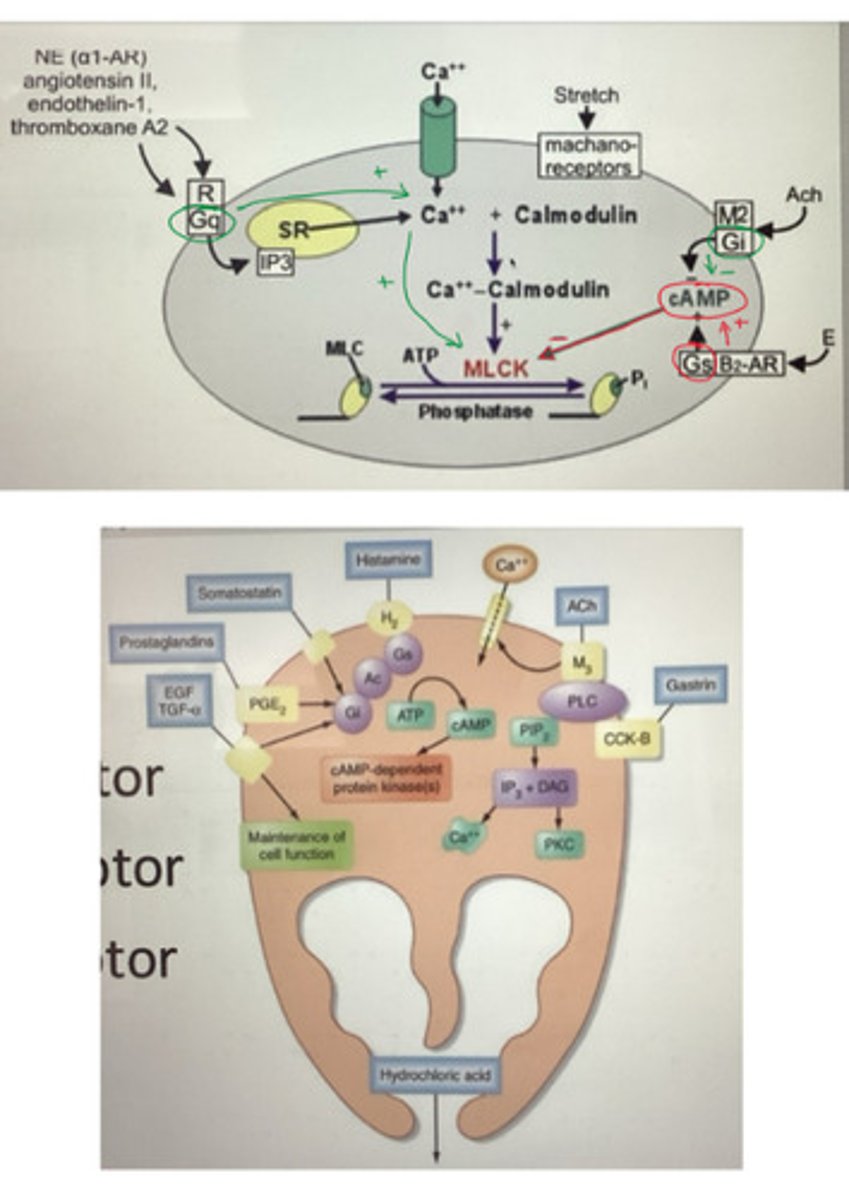
increase: histamine (Gs), ACh (Gq), gastrin (Gq)
decrease: somatostatin and prostaglandins (both Gi)
group these chemical stimulants into categories based on if they increase or decrease secretion of gastric acid by parietal cells, and label them as Gs/Gq/Gi coupled: histamine, somatostatin, ACh, gastrin, prostaglandins
parietal cells
specialized epithelial cells in the stomach lining (fundus and body) that secrete HCl
Gs (histamine in parietal, VIP in SM) increases cAMP activity and leads to more fusion of the membranes/proton pumps and more HCl secretion/decreased activation of MLCK and less SM contraction
Gq (ACh/gastrin in parietal, NE/angiotensin II/endothelin-1/thromboxane A2 in SM) increases Ca levels (no involvement with cAMP and weaker pathway than Gs)
Gi (SST/prostaglandin in parietal, ACh in SM) decreases cAMP activity and leads to less fusion of the membranes/proton pumps and less HCl secretion/increased activation of MLCK and more SM contraction
what do Gs, Gi, and Gq coupled pathways do in parietal cells/smooth muscle cells, and what activates them?
a "horizontal mitten" where the straighter edge = basolateral and the curvy side = lumen facing
within the cell, metabolic waste is used to create gastric acid
describe the orientation of a parietal cell
carbonic anhydrase
enzyme that facilitates the creation of HCO3 + H+ from H2O + CO2 (metabolic waste)
reversible reaction, but without this it would not be able to occur
ATPase: the basolateral side (which faces the blood and ECF) because any secretions/exchange in the apical side is "lost" in the lumen
proton pump: apical/lumen side
HCO3 pump: basolateral side
Cl- channel: apical side
K+ channel: basolateral side
which side of a parietal cell are the 5 main pumps/transporters on (Na/K ATPase, proton pump, HCO3/Cl, Cl-, K+ channel) and if known, why?
H+/K+ ATPase (proton pump)
found on the apical/lumen side of the parietal cell, and pumps H+ ions out into the lumen in exchange for K+
the H+ comes from the carbonic anhydrase reaction
there is a K+ channel on the basolateral side that transports K+ out of the cell
HCO3+/Cl- pump
on the basolateral side of the parietal cell, transports HCO3 out and Cl- in
there is a Cl- channel on the apical side that transports Cl- out of the cell into the lumen
it becomes more basic because more HCO3+ is transported out of the cell
this is because more H+ needs to be made to use in HCl, and HCO3 is a byproduct that acts as a buffer and makes blood more alkaline
after you eat how does your blood pH change and why?
histamine
Gs pathway stimulant that binds to H2 receptors to increase cAMP production; H2 receptor activates guanylate cyclase, which facilitates more ATP converting to cAMP, which increases cAMP-dependent protein kinases that increase fusion of membranes to promote HCl secretion
the increased cAMP increases the fusion of membranes and action of the H+ pump in parietal cells to increase HCl secretion
ACh and Gastrin
Gq pathway stimulants that bind to M3 receptor/CCK-B receptor respectively and lead to more membrane fusion and secretion of gastric acid
increases Ca2+ in the cell