HSCT
1/30
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
31 Terms
Graft =
hematopoietic stem cells
Graft sources → 3
bone marrow
*peripheral blood stem cell (most common)
umbilical cord blood
IMMUNOLOGY OF GRAFT SOURCES
__________ → own stem cells are used
__________ → identical twin’s stem cells are used
__________ → donor stem cells used, matched based on HLA antigens
autologous
syngeneic
allogeneic
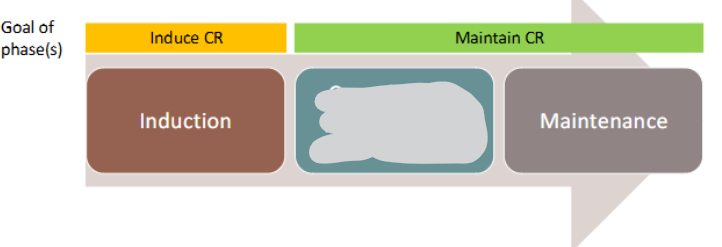
Goals of conditioning regimen
Autologous HSCT
Allogeneic HSCT
eradicate disease
eradicate disease + immunosupp
AUTO HSCT
Supp care →
Complications → Relatively well tolerated (4)
Long term complication →
GFs + transfusion supp, antimicrobial prophylaxis
NV, infxn, fatigue, diarrhea
secondary malignancies
ALLO HSCT
Supp care →
Complications →
same as auto + immunosupp
same as auto + more infxn, graft vs host disease, hepatic SOS (sinusoidal obstructive syndrome)
ACUTE LEUKEMIAS
type 1 →
type 2 →
Major goals of therapy (for both) → (*CR complete remission)
ALL more common in children, CNS prophylaxis routine
AML more common in adults, CNS prophylaxis NOT routine
achieve rapid CR → maintain CR → minimize tox
ALL LYMPHOCYTIC Treatment Phases
consolidation (chemo and/or allo HSCT)
interim maint
delayed intensification
interim maint II
CNS prophylaxis w intrathecal chemo
Adult AML Treatment Phases
consolidation (chemo and/or allogeneic HSCT)
ACUTE LEUKEMIA PEARLS
Intrathecal chemo →
High dose cytarabine (_______ mg/m²) → __________ to prevent corneal toxicity & hemorrhagic conjunctivitis
DO NOT USE preservative-containing solutions/drugs
>1000 → use steroid eye drops
CHRONIC MYELOID LEUKEMIA (CML)
Mainstay of therapy →
BCR-ABL tyrosine kinase inhib
CHRONIC MYELOID LEUKEMIA (CML)
Generic → *Toxicity
ALL CAN CAUSE ___________
Gleevec →
Sprycel →
Tasigna →
Iclusig →
myelosupp
imatinib → fluid retention/edema
dasatinib → pleural/pericardial effusions
nilotinib → +QTc BW
ponatinib → arterial thrombosis, hepatotox, VTE, HF
CHRONIC LYMPHOCYTIC LEUKEMIA
Clinical presentation:
*1st line tx if NO deletion 17p →
→
→
leukocytosis
acalabrutinib (Calquence) ± obinutuzumab (Gazyva)
venetoclax (Venclexta) + obinutuzumab (Gazyva)
zanubrutinib (Brukinsa)
CML/CLL DRUG PEARLS
CML → _______ generic & less expensive. but generally ____ preferred than other BCR/ABL inhibitors
Patients take BCR/ABL inhibitors long term, pharmacists are key in monitoring for toxicities, DDIs, complianceCLL → may see _____________ after initiation of venetoclax, ibrutinib, and acalabrutinib
CLL → ___________, dose is ramped up initially to mitigate risk to TLS (tumor lysis syndrome)
imatinib, less
transient lymphocytosis
venetoclax
HODGKIN LYMPHOMA
NON-HODGKIN LYMPHOMA
classical HL, 4 subtypes, nodular lymphocyte-predominant HL
B cell & T cell lymphomas
CLASSICAL HODGKIN LYMPHOMA (HL)
_______ is the prototype chemotherapy regimen, NOT USED FOR NHL
ABVD
NON-HODGKIN LYMPHOMA CLINICAL PRESENTATION
~40% present with B symptoms → 3
Fatigue, malaise, pruritus, peripheral _________
unexplained weight loss >10% of BW, unexplained fever, night sweats
lymphadenopathy
NON-HODGKINS 1ST LINE TX DEPENDS ON LYMPHOMA SUBTYPE
DLBCL →
Follicular lymphoma →
Burkitt lymphoma →
H pylori associated lymphoma →
RCHOP or polatuzumab + RCHP ± radiation
watch-and-wait, bendamustine + rituximab, RCHOP
hyperCVAD, dose-adj EPOCH
if early, tx by eradicating H pylori
R-CHOP REGIMEN
→
→
→
→
→
Cycle every _____
Rituximab
Cyclophosphamide
Doxorubicin
Vincristine
Prednisone
21d
RITUXIMAB
_________ chimeric IgG1 mAb
Most common side effects → ________, fever, lymphopenia, chills, infxn, asthenia
^ required premedication:
Formulations
WARNINGS & PRECAUTIONS → 4
antiCD20
infusion rxns
antihistamine + APAP ± steroid
IV, SQ
infusion rxns (1st dose!), HBV rxns, sev mucocutaneous rxns, PML (progressive multifocal leukoencephalopathy)
RITUXIMAB & HBV REACTIVATION
Screen all patients receiving rituximab or other anti-CD20 mAb → core antibody + surface antigen
IF EITHER TEST IS POSITIVE, prophylaxis → ______ preferred
Monitor ________ and ______ during tx
Continue prophylaxis for at least _____ after completion of therapy
anti-HBc IgG + HbsAG
entecavir
HBV DNA, LFTs
12m
ANTHRACYCLINE CARDIOTOXICITY
Acute
Subacute
Chronic/delayed
w/in 1w
w/in weeks
~1yr post tx, IRREVERSIBLE
Multiple proposed mechanisms of anthracycline cardiotoxicity (CHRONIC/DELAYED)
cardiomyocytes _______
_____ formation
**_________ accumulation
dysregulation of cardiomyocytes ________
apoptosis
ROS
mitochondrial iron
autophagy
ANTHRACYCLINE CARDIOTOXICITY risk is related to the _________ dose
cumulative
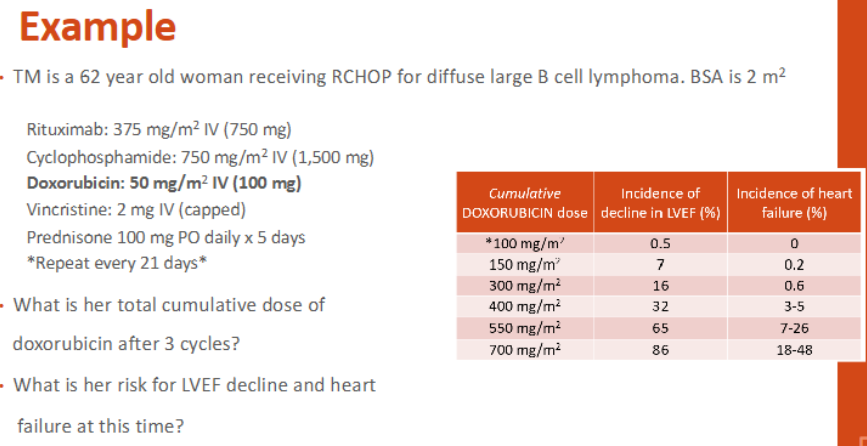
What is her total cumulative dose of doxorubicin after 3 cycles?
What is her risk for LVEF decline and HF at this time?
150 (look at the mg/m²)
7%, 0.2%
ANTHRACYCLINE monitoring recommendation →
baseline LVEF by echocardiogram or MUGA
ANTHRACYCLINE CARDIOPROTECTION
Limit lifetime ________
_____________
Cardioprotectant → ONLY FOR DOXORUBICIN
Use ________ formulation if appropriate (Doxil)
cumulative dose
prolong inf rate
dexrazoxane (Zinecard)
liposomal
DEXRAZOCANE (ZINECARD)
MOA
Use after _____ mg/m² of doxorubicin has been given
Dose ratio dexrazoxane:doxorubicin
Infuse immediately _______ doxorubicin infusion
iron chelator, topo II inhib
300
10:1
BEFORE
LATE EFFECTS OF CHEMOTHERAPY (Survivorship)
Effects on __________
_____________
Other: ________, avascular necrosis, pulmonary fibrosis, hearing loss, endocrine dysfx, cataracts
fertility
secondary malignancies
cardiotox
SUMMARY:
chronic myeloid leukemia
chronic lymphocytic leukemia
hodgkin lymphoma
non-hodgkin lymphoma (DLBCL)
BCR-ABL tyrosine kinases inhib (-tinibs)
acalabrutinib ± obinutuzumab, venetoclax + obinutuzumab, zanubrutinib
ABVD
RCHOP, polatuzumab + RCHP ± radiation
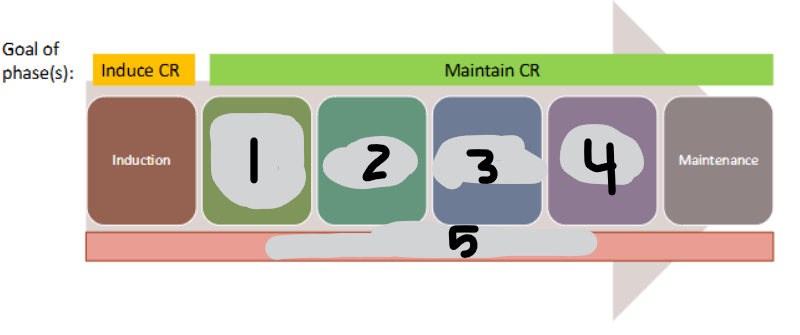
HSCT REGIMEN → 5
mobilization
collection
conditioning
transplant
engraftment