Gen Surg: Trauma / Acute Care
1/42
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
43 Terms
Consult Surgery
A 67 y/o male presents with severe abdominal pain, rigid abdomen, rebound tenderness, fever, and free air under the diaphragm. You administer broad-spectrum antibiotics and start monitoring the patient’s vitals. What is the next step?
CT
A 35 y/o female presents with RLQ pain, nausea, vomiting, and fever. What is the best next diagnostic test?
US
A 6 y/o male presents with RLQ pain, nausea, vomiting, and fever. What is the best next diagnostic test?
CTA
A 78 y/o female with a PMHx of atrial fibrillation presents with severe abdominal pain. She describes the pain as “a constant 10/10” and “feels like a million knives are stabbing me at all times”. On exam, the abdomen is only mildly tender to palpation. What is the next step in diagnosis?
Consult Vascular Surgery
Patient presents with a BP of 84/60 and complains of abdominal pain. On physical exam, a pulsatile mass is noted in their abdomen. What is the next best step?
Mesenteric ischemia, AAA
What are two vascular causes of an acute abdomen?
SBO, volvulus
What are two obstructive causes of an acute abdomen?
Appendicitis, cholecystitis, pancreatitis
What are three inflammatory causes of an acute abdomen?
Surgery
In a patient with involuntary guarding, rigidity, rebound tenderness, or hemodynamic instability, what should be considered?
Hypoxia
What should be considered first as the cause of altered consciousness in trauma?
Hemorrhagic Shock
What is the most common cause of altered consciousness in trauma?
Compound Fractures
Fracture communicates with outside environment, either through direct exposure of the bone or a laceration overlying the fracture
Osteomyelitis
What is the biggest risk associated with a compound fracture?
IV antibiotics
What is the first step in treatment for a compound fracture?
Hypovolemic Shock
Loss of blood or fluid volume due to hemorrhage or fluid loss, which increases the HR/SVR and decreases cardiac output
-Sx: pale, cool, mottled skin. Slow capillary refill, decreased skin turgor, dry mucous membranes, tachycardia, decreased BP and CO
-Dx: decreased Hgb/Hct and PCWP
-Tx: insert two large bore IVs and give crystalloids, monitor urine output
Cardiogenic Shock
Primary myocardial abnormality prevents the heart from maintaining cardiac output
-Sx: severe respiratory distress, cool clammy skin, vasoconstriction, hypotension, decreased cardiac output
-Dx: decreased BP and CO, increased PCWP
-Tx: oxygen, isotonic fluids, and dobutamine/epinephrine
Obstructive Shock
Extrinsic or intrinsic obstruction of the heart or great vessels
-Sx: severe respiratory distress, cool clammy skin
-Dx: CXR, EKG, increased PCWP
-Tx: oxygen, isotonic fluids, inotropic support
Septic Shock
Severe host immune response, which is characterized as sepsis with persistent signs of organ damage, hypotension, and lactate > 4
-Sx: warm flushed extremities, brisk capillary refill, bounding pulses, wide pulse pressure that eventually leads to the development of cool clammy skin
-Dx: SIRS criteria (2 of 4 required)
-Tx: broad-spectrum IV antibiotics + isotonic crystalloids
Anaphylactic Shock
IgE mediated systemic hypersensitivity reaction with histamine release, causing vasodilation and increased capillary permeability
-Sx: pruritis, hives, angioedema, throat fullness, hoarseness, wheezing
-Dx: decreased CO, PCWP, SVR
-Tx: epinephrine, airway management
Neurogenic Shock
Sympathetic blockade leads to unopposed vagal tone on vessels and vasodilation
-Sx: hypotension without tachycardia, bradycardia
-Dx: decreased CO, PCWP, SVR
-Tx: fluids, pressors
Endocrine Shock
Adrenal insufficiency leads to decreased corticosteroid and mineralocorticoid activity
-Sx: low serum glucose, hypotension refractory to fluids and pressors
-Dx: decreased CO, PCWP, SVR
-Tx: hydrocortisone 100mg IV
Massive Transfusion
What is indicated in severe trauma and exsanguinating hemorrhage?
-PRBCs, plasma, platelets
O negative
What is the universal donor?
Acute Hemolytic Reaction
Most dangerous transfusion reaction, caused by ABO incompatibility
-Sx: fever, flank pain, hypotension, hemoglobinuria
-Tx: stop transfusion
Febrile Nonhemolytic Reaction
Most common transfusion reaction
-Sx: fever, chills
TRALI
Transfusion-related acute lung injury that occurs within 6 hours of a transfusion
-Sx: acute hypoxia, bilateral infiltrates
TACO
Transfusion-associated circulatory overload, seen mostly in CHF patients
-Sx: pulmonary edema after transfusion
-Tx: diuretics
Fluid resuscitation
A 45 y/o man with a history of alcohol use disorder presents with profuse hematemesis that began just prior to arrival. His vital signs demonstrate a HR of 120 and BP of 98/62. What is the best first step in managing his care?
Balloon tamponade
What should be initiated in all patients with esophageal variceal hemorrhage who fail initial endoscopic management?
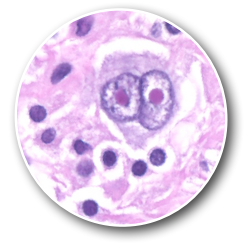
Reed-Sternberg Cells
A 32-year-old man presents to your office with worsening fatigue. He reports feeling tired most of the day and is unable to focus at work. He reports no changes to his regular routine, and he has not started any new diets or medications. He reports receiving 7 to 8 hours of uninterrupted sleep most nights and has one to two cups of black coffee each morning. The only other abnormality he has noticed is an 8-pound unintentional weight loss, which he contributes to increased stress at work. On physical exam, he is a pleasant, healthy-appearing, athletic man in no acute distress. His heart sounds are normal, and his lungs are clear. His thyroid is smooth and symmetrical, but he does have an enlarged left anterior cervical lymph node. Overall, his skin exam is normal, although there are many superficial excoriations. He reports his skin has been feeling itchier than normal over the past few months. A complete blood count reveals WBC 8,200/mcL and thyroid function studies reveal TSH 3.4 mIU/L. An Epstein-Barr virus IgG antibody test is positive. An excisional biopsy of the enlarged lymph node is elected, and the histology is shown above. What are these cells, given the most likely diagnosis?
Abdominal US
A 17-year-old boy is admitted for acute appendicitis after presenting with fever, abdominal pain, and anorexia for the last 3 days. He undergoes a laparoscopic appendectomy, in which the surgeon notes and removes a ruptured appendix. After the surgery is completed without complications, he is admitted postoperatively for IV antibiotics, pain control, and supportive care. He does not have drains or a urinary catheter. On postoperative day 5, he is still unable to tolerate oral intake though he is passing gas. He is requiring pain medication and has a rising fever curve. On physical exam, his belly is mildly distended and tender to palpation and his lungs are clear to auscultation. His surgical wounds are clean, dry, and intact. He reports no dysuria. The rest of his exam is unremarkable. What is the most important next test to order?
Strangulated Indirect Inguinal Hernia
A 24 y/o male presents to the ED for severe abdominal pain that radiates to his scrotum. The pain began 1 hour ago after lifting a 50 lb box at work. He has no significant past medical history and is sexually active. Physical exam reveals a painful, irreducible mass in the right scrotum. There is mild erythema of the skin overlying the mass. US of the scrotum reveals fluid within the sac and dilated bowel loops. What is the most likely diagnosis?
DIC
A 56-year-old man is admitted to the hospital for wound care of an infected right leg. Two sets of blood cultures are positive for Escherichia coli. Intravenous antibiotics are started. The next day, the patient develops tachycardia, hypotension, altered mental status, and shortness of breath. Epistaxis, gingival bleeding, and hematemesis are noted. Further examination reveals the presence of petechiae and purpura as well as diffuse thromboses. His platelet count on admission 24 hours ago was 145,000/mcL but is now 79,000/mcL. What is the most likely diagnosis?
Wernicke Encephalopathy
A 56 y/o woman with a history of chronic alcohol use disorder presents via EMS with altered mentation. Vital signs are WNL. On exam, she is noted to have nystagmus leading to conjugate gaze palsy with extraocular movement. Laboratory studies are unremarkable. Brain MRI demonstrates signal abnormality within the mamillary bodies. What is the most likely diagnosis?
Cecal volvulus
A 40 y/o woman presents to the ED with acute abdominal pain and cramping that began about 2 hours ago and has gotten progressively worse. She had episodes like this in the past that resolved after a few minutes and none have ever lasted this long. She has not had a bowel movement in 48 hours or any recent surgeries. On physical exam, her abdomen is largely distended and tympanic. Given the x-ray, what is the most likely diagnosis?

Ogilvie Syndrome
Acute colonic pseudo-obstruction, which usually occurs in hospitalized patients with severe illness
-Associated with anticholinergic, antipsychotic, dopaminergic, opiate drugs, epidural anesthetics
-Sx: abdominal distention, nausea, vomiting, constipation, diarrhea
-Dx: CT with contrast
Compression + LMWH
What two things are suggested for VTE prophylaxis in patients undergoing colorectal surgery?
Compartment Syndrome
A 35 y/o man presents to the ED today with severe pain to his left forearm. The patient was seen by an orthopedic surgeon yesterday and had a short-arm cast placed after he fractured his ulna. The patient’s left hand appears extremely pale, and his cast is immediately removed. He has absent radial pulses to his left arm and 2+ radial pulses on his right arm. The dorsal compartment pressure measures 36 mmHg. What is the most likely diagnosis?
< 50,000
A 66-year-old man presents to the office with several months of bleeding in the gums and easy bruising. He was at the dentist getting his teeth cleaned and was told by his dental hygienist to be evaluated for a possible bleeding disorder. He is concerned because he is scheduled to have a knee replacement next week and needs medical clearance. Upon physical examination, he has some light bruising to his left elbow and right thigh, but no purpura, petechiae, or joint effusions. A complete blood count reveals a platelet count of 100,000/µL. In a patient with evidence of active bleeding who is about to undergo major surgery, what platelet thresholds is an indication for a platelet transfusion?
Hamman Sign
Mediastinal crackling heard with each heartbeat when the patient is in the LLD position
Choledocholithiasis
A 40 y/o woman presents to the ED with RUQ pain. On exam, she is afebrile but has right upper quadrant tenderness. Laboratory testing reveals an alk phos of 640 U/L, AST of 204, and ALT of 220. The common bile duct measures 9mm on transabdominal ultrasound, and the gallbladder is present. What is the most likely diagnosis?
Diverticulitis
A 65-year-old woman with obesity presents with an acute onset of left lower quadrant pain accompanied by nausea, vomiting, and fever. A rectal exam shows a painful mass near the rectum. Laboratory studies reveal leukocytosis with a left shift. An abdominal radiograph is unremarkable. Localized bowel wall thickening and increased soft tissue density in pericolonic fat are demonstrated on an abdominal CT scan. What is the most likely diagnosis?
EGD
A 44 y/o woman presents to the ED with two episodes of hematemesis over the last 5 hours. BP is 100/60, HR 106, and RR 23. Hgb is 11.3. What is the most appropriate initial diagnostic test?