Pharmacology Exam 3
1/115
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
116 Terms
Sympathomimetic
Imitates nor epinephrine
sympatholytic / parasympathomimetic
Imitates acetycholine
Hypertension
High blood pressure
Increases risk of
– Stroke
– Angina
– Myocardial infarction
– Heart failure
– Kidney disease
Incidence increases with aging
Prehypertension
Sys: 120 to 139 / Dia: 80 to 89
Stage 1 Hypertension
Sys: 140 to 159 / Dia: 90 to 99
Stage 2 Hypertension
Sys: >160 / Dia: >100
a1 receptors
Sympathetic stimulation causes vasoconstriction through
B1 receptors
Increases heart rate and contractility through
a2 receptors
Inhibits sympathetic outflow through
calcium channels
– Allow calcium to enter cells of the heart
muscle, arteries, and arterioles
– Leads to muscle contraction
– Also associated with B1 receptors in heart
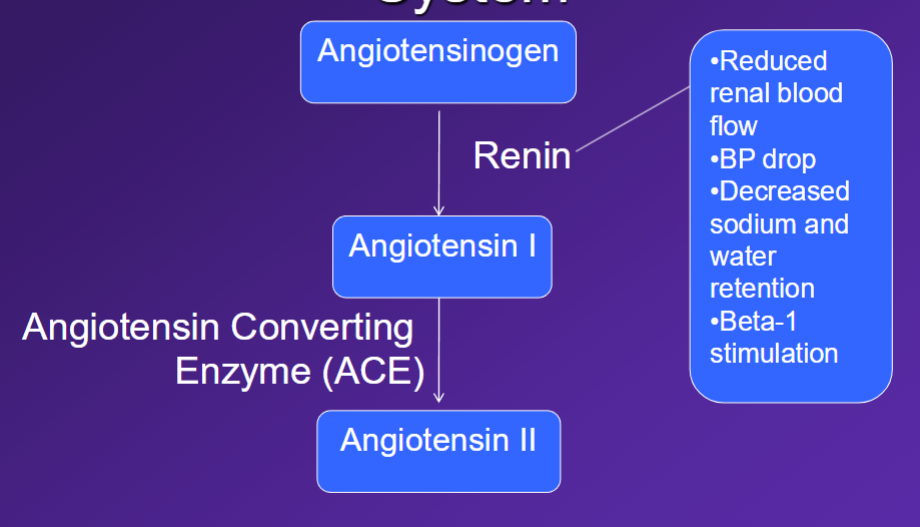
Renin-angiotensin aldosterone system
Diuretics
Medications that increase urine output. Increase excretion of Na and chloride. Leads to increased excretion of water. Used to treat hypertension. Also used for edema. Dilate artery right below the heart
Thiazide diuretics
Preferred for hypertension. Drug of choice for uncomplicated stage 1 hypertension. People allergic to sulfa may not be able to take these drugs. Not good with swelling/fluid decrease. Well-tolerated, with little side effects.
Loop diuretics
More potent as diuretics. Preferred for edema. can be used for hypertension when thiazides are not sufficiently effective
Potassium-sparing diuretics
Weak diuretics. Not good at getting rid of excess fluid. Not as effective, but doesn’t have a sulfa group
Adverse effects of loop and thiazide diuretics
Hypokalemia, increased LDL cholesterol. hyperglycemia, sexual dysfunction.
Adverse effects of potassium-sparing diuretics
Hyperkalemia, spironolactone (gynecomastia and sexual dysfunction in males) (deepening of the voice, hirsutism [hair growth in unusual areas], and menstrual irregularities in females
Beta-Blockers
Block beta-adrenergic receptors. Noselective and cardioselective (B1 receptor)
Beta-Blockers
Decrease heart rate and force of contraction. Slow impulse conduction through AV node, decrease release of renin by kidney, bronchoconstriction through B2-receptor blockade, inhibit glycogenolysis due to B2-receptor, affect metabolism of triglycerides and fatty acids, decrease peripheral vascular resistance
Beta-blockers
hypertension, angina, heart failure, migraine prevention, acute panic symptoms, pheochromocytoma, cardiac dysrhythmias, acute myocardial infarction and preventing recurrent myocardial infarction, glaucoma
Beta blocker adverse effects
Bronchoconstriction (do not use in patients with asthma), mask symptoms of hypoglycemia, delay recovery from hypoglycemia (use caution in patients with diabetes), beta-blockers should not be abruptly discontinued, bradycardia, insomnia, sexual dysfunction, depression, nightmares, increased triglycerides, reduced HDL, fatigue, decreased exercise tolerance
ACE Inhibitors
Inhibit the action of angiotensin converting enzyme
Therapeutic uses
– Hypertension
– Heart failure
– Myocardial infarction
ACE Inhibitors
– Arterial and venous vasodilation
– Decreased systemic vascular resistance
– Increased sodium and water excretion
– Increased potassium retention
– Increased blood flow to kidney
ACE Inhibitors and hypertension
Effective alone or in combination
– All ACE inhibitors have similar efficacy
Mechanism of antihypertensive effect
– Vasodilation through reduced angiotensin II
– Vasodilation through increased bradykinin
– Reduced blood volume
More effective in patients with high renin
blood levels
ACE inhibitors adverse effects
Usually well tolerated, persistent dry cough, angioedema (swelling in the blood vessels), first-dose hypotension, contraindicated in pregnancy
Angiotensin II Receptor Blockers (ARBs)
Block the action of angiotensin II at its receptor. similar to ACE inhibitors, no effect on bradykinin
Calcium channel blockers
Block calcium channels and decrease influx of calcium into vascular smooth muscle and cardiac muscle cells (peripheral vasodilation, decreased heart rate, decreased force of contraction, dilate arterioles of the heart). Two types: non-selective (heart and vascular muscle) and selective (vascular muscle) — for those with heart failure
Calcium channel blockers
Recommended for use post-heart attack for black males instead of beta blockers. Also preferred for those with a lot of side effects while on beta blockers
Calcium channel blockers adverse effects
Gingival hyperplasia (growth of gums)
Uncomplicated stage 1 hypertension
Thiazide diuretic. May consider ACE inhibitor, ARB, calcium channel blocker
Stage 2 hypertension
Two-drug therapy. Thiazide diuretic plus ACE inhibitor, ARB, or calcium channel blocker
Angina
B-blockers or calcium channel blockers
History of myocardial infarction
B-blockers, ACE inhibitors, possibly calcium channel blockers
Heart failure
ACE inhibitors, diuretics, B-blockers, ARBs
Renal insufficiency
ACE or ARB
Diabetes mellitus
ACE inhibitors + ARBs first line. Diuretics second line
Asthma
B-blockers are contraindicated
Pregnancy
Drugs affecting the renin-angiotensin-aldosterone system are contraindicated
Angina Pectoris
Myocardial oxygen demand exceeds oxygen supply (results in occurrence of chest pain)
Angina Pectoris
Sudden pain that originates behind breast bone, pain radiates to left shoulder and arm, pain or discomfort may also be felt in neck and jaw
Angina pectoris treatment
Beta-blockers, calcium channel blockers, and nitrates
Nitroglycerin
Used to treat acute anginal attacks. Long-acting forms can be used regularly to reduce frequency of anginal attacks. Causes vasodilation and primarily affects veins
Myocardial infarction
Occlusion of a coronary artery. Prevents sufficient blood from reaching a portion of heart muscle. Persistent ischemia leads to death of some myocardial cells. Caused by platelet aggregation and clot formation at site of atherosclerotic plaque
Heart failure
Heart cannot pump with enough force to adequately supply blood to the tissues. Progressive disease.
Symptoms
– Water retention and edema
– Fatigue
– Exercise intolerance
– Shortness of breath
– Tachycardia
Class I heart failure
No limitation of ordinary physical activity
Class II heart failure
Slight limitation of physical activity. Normal physical activity causes symptoms
Class III heart failure
Marked limitation of physical activity. Even mild activity causes symptoms
Class IV heart failure
Symptoms at rest. Increased discomfort with any physical activity
Digoxin (lanoxin)
Cardiac glycoside. Therapeutic uses: heart failure and cardiac dysrhythmias. No longer considered first-line therapy. Low therapeutic index drug. Many drug interactions. Does not prolong survival in heart failure. Improves quality of life
Diabetes mellitus
Endocrine disorder characterized by hyperglycemia
Type 1 diabetes (IDDM)
<10% of diabetes cases. Do not make insulin
Type 2 diabetes (NIDDM)
Most common form of diabetes. Insulin resistance and altered secretion. Managed with diet, exercise, oral medications, and insulin
Diabetes symptoms
Polydipsia (excessive thirst), polyuria (urinates often), polyphagia (excessive hunger), weight loss, fatigue, blurred vision, irritability
Type 2 diabetes
Continued production of insulin. Characterized by insulin resistance and altered secretion. Patient may be asymptomatic. Can go undiagnosed for years
Incretins
Hormones released by the GI tract in response to absorption of food. Increase release of insulin, preserve insulin-producing capacity of B-cells, decrease appetite, reduce glucagon release. Diminished response in diabetics.
Amylin
Co-secreted with insulin by B-cells. Decreases GI motility, slow rate of glucose absorption, reduces glucagon release, decreases appetite. Insufficient regulation from ____ in diabetics
Risk factors for type 2 diabetes
Obesity, abdominal obesity, sedentary lifestyle, age, genetic link
Complications of diabetes
Acute hypoglycemic episodes, hypertension, heart disease, stroke, kidney disease, neuropathy, amputations, sexual dysfunction, periodontal disease
Mild hypoglycemia
Sweating, intense hunger, inability to concentrate, palpitations, tachycardia, tremor, and anxiety
Moderate hypoglycemia
Mood changes, headache, irritability, confusion, blurred vision, drowsiness
Severe hypoglycemia
Poor responsiveness, unconscious, coma
Nocturnal hypoglycemia
Morning headache, nightmares, lips/tongue tingling, profuse sweating, restless sleep
Sulfonylureas
Increase release of insulin. 2nd gen are more potent and more predictable. Adverse effects: hypoglycemia, weight gain
Meglitinides
Similar to sulfonylureas. Lowers glucose levels by stimulating release of insulin from the pancreas. Generally well tolerated but can cause hypoglycemia and weight gain
Biguanides
Antihyperglycemic agent: lowers blood glucose by decreasing glucose production in the liver and increasing glucose uptake and utilization. Reduces release of glucose by liver. Does not cause hypoglycemia. Adverse effects: GI effects, lactic acidosis
Thiazolidinediones
Adverse effects: liver dysfunction, fluid retention, heart failure, effects on plasma retention, increased risk of MI and heart-related death. Withdrawn from market. Stimulated more production of insulin
Alpha-Glucosidase Inhibitors
Delays absorption of dietary carbohydrates. Adverse effects: GI
DPP-4 Inhibitors
Inhibit dipeptidyl peptidase IV (prolongs activity of incretins). Stimulate insulin secretion. Inhibit glucagon release. Reduce postprandial glucose. Injectable
Incretin mimetics
Reduce postprandial glucose. Reduce A1c. May cause weight loss. May preserve B-cell function. Adverse effect: pancreatitis, nausea, vomiting, diarrhea
Pramlintide
Amylin-like drug. Used for type 1 and type 2. injectable
Insulin
Can be used alone. Often in combination with oral antidiabetic drug therapy in type 2
Primary neurotransmitters
Norepinephrine, serotonin, dopamine
Norepinephrine
Alertness, concentration, energy, attention, anxiety, impulse, irritability, mood, cognitive function
Dopamine
Pleasure, reward, motivation/drive, attention, appetite, sex, aggression, mood, cognitive function
Serotonin
Obsessions & compulsions, memory, appetite, sex, aggression, anxiety, impulse, irritability, mood, cognitive function
Major depression
Cause not completely understood. Decreased serotonin (5-HT) and NE. Diminished ability to function. Twice as frequent in women. Not age-dependent. Onset can be due to meds or medical conditions
Major depression
Depressed mood, loss of interest or pleasure in activities, change in appetite, change in sleep patterns, loss of energy, feelings of worthlessness or guilt, diminished ability to concentrate, thoughts of suicide
Selective serotonin reuptake inhibitors (SSRI’s)
Most commonly used antidepressents
SSRI’s
Usually well-tolerated. adverse effects: sexual dysfunction, nausea, vomiting, CNS stimulation, headache, potential “serotonin syndrome”
SSRI
Slow onset of effect (4-6 weeks for maximum effect). Can’t quite cold turkey
Serotonin/Norepinephrine reuptake inhibitors (SNRI’s)
Similar in mechanism to TCAs, better side effect profile, newest products
Tricyclic antidepressants (TCA’s)
Block reuptake of serotonin and NE. Also block cholinergic receptors
Tricyclic antidepressants
Adverse effects: orthostatic hypotension, anticholinergic effects, sedation, cardiac toxicity, seizures, weight gain, sexual dysfunction, increased sweating
Bupropion
Approved for major depression and smoking cessation. Mild NE/DA reuptake inhibitor. Well tolerated and could be used in combo. Can cause seizures at higher doses
Tetracyclics
Affects multiple receptors (increase in 5HT and NE). Adverse effects: somnolence, dizziness, weight gain, increased cholesterol, mild anticholinergic effects
Trazadone (Desyrel)
Less effective than other agents. Causes significant sedation. Used to treat insomnia. Other adverse effects: dizziness + orthostatic hypotension
Antidepressants and Bipolar
Treat acute depressive episodes.Use lower doses and shorter duration of therapy than for major depressive disorder
Lithium (Li+)
Treats acute manic episodes. Prevents recurrent episodes of mania and depression. Mechanism of action is unclear.
Lithium adverse effects
Nausea, diarrhea, confusion, muscle weakness, headache, polydipsia, polyuria, fine hand tremor. Long term use: renal toxicity, goiter, hypothyroidism
Lithium
Dosed multiple times per day. low therapeutic index; can be toxic. Advise patient to avoid dehydration (drink 2 to 3 L water daily)
Valproic Acid (VPA)
Mood stabilizer. Mechanism unknown. Used for acute manic episodes and for maintenance therapy. Higher therapeutic index than lithium. Faster onset than litium
Valproic acid adverse effects
Nausea, vomiting, diarrhea, indegestion, sedation, weight gain, headache, prolonged bleeding time, alopecia, hepatitis, thrombocytopenia
Carbamazepine
Mood stabilizer. Used for treatment in acute mania and maintenance therapy. Mechanism of action unknown
Carbamazepine adverse effects
Nausea, vomiting, diarrhea, anorexia, constipation, drowsiness, confusion, headache, dizziness, vertigo, blurred vision, slurred speech, vertigo, blood dyscrasias
Carbamazepine drug interactions
Induces P450 enzymes. Increases metabolism of other drugs. Increases its own metabolism. Interacts with drugs that inhibit P450 (increase concentration of carbamazepine. Grapefruit juice increases absorption
Antipsychotics and Bipolar
Used alone or in combination with mood stabilizer. Effective in treatment of acute manic episode and for maintenance therapy. Atypical preferred
Anxiety disorders
Norepinephrine, serotonin, dopamine, GABA
Generalized anxiety disorder (GAD)
Excessive/uncrontrollable worry. Symptoms persist for 6 months or more. Most patients develop another psychiatric disorder
Panic disorder
Recurrent, spontaneous panic attacks. Persistent concern about another panic attack, worry about consequences of another attack, or significant behavior change after panic attack
Social anxiety disorder (SAD)
Most common anxiety disorder. Intense but irrational fear of being negatively evaluated or scrutinized in a social interaction. Interferes with daily routine, work performance, or social interaction. Interferes with daily routine, work performance, or social life. Patients tend to avoid situations that will cause anxiety