PTE 756: exam 2
1/66
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
67 Terms
what is chronic limb-threatening ischemia (CLTI)?
the most severe, advanced stage of PAD; occurs when severe plaque buildup drastically restricts blood flow to the legs and feet, starving tissues of necessary oxygen and nutrients
what is the most common cause of peripheral artery disease (PAD)?
arteriosclerosis
what’s the difference between atherosclerosis and arteriosclerosis?
atherosclerosis: plaque builds up inside the large arteries
arteriosclerosis: hardening or thickening of the small artery walls, which causes them to lose their flexibility and elasticity
what are the three critical phases of ischemia?
phase I: the collateral circulation is insufficient for the metabolic needs of the affected extremity → decreased skin perfusion
phase II: when activity or exercise causes relative ischemia and pain (intermittent claudication)
phase III: may experience rest pain, gangrene, or nonhealing wounds in the extremity below the occlusion
what’s the difference between anatomical obstruction of arterial flow and functional obstruction?
anatomical obstruction includes thromboemboli and vasculitis
functional obstruction includes Raynaud’s disease
what is Raynaud’s disease?
a common vascular disorder characterized by temporary spasms in small blood vessels, which significantly restricts blood flow to the extremities
what is Buerger disease?
an immune and inflammatory disease of the peripheral arteries accompanied by vasospasm and thrombi in the arterial segments to the feet and/or hands; symptoms include thin/shiny skin, thickened malformed nails, pain, tenderness, erythema caused by dilated capillaries, and cyanosis caused by deoxygenated blood cells
what is wet gangrene?
gangrene with an active infection requiring urgent debridement
describe the clinical presentation of arterial insufficiency wounds.
small and round wounds with smooth, well-demarcated borders; usually at distal digits
wound base is typically pale, lacks granulation tissue, and may be wet or dry
increased pain at night; reduced pain with BLE in dependent position
hairless, dry, fissured skin
what is the WIfi Lower Extremity Threatened Limb Classification?
a classification system to permit a more meaningful analysis of outcomes for various forms of therapy in patients who have critical limb ischemia by taking into consideration the extent of the wound, the degree of perfusion, and the presence of infection
what are some noninvasive vascular tests for arterial insufficiency?
pulse checks, doppler examination, capillary refill time, rubor of dependency test, ABI, toe and segmental pressures, pedal acceleration time. transcutaneous oxygen perfusion calculation, exercise stress test, arterial dupelx, and MRI/CT with contrast
what does an absent pulse suggest?
a proximal critical stenosis or occlusion
what’s the difference felt between vessels with high outflow resistance and low outflow resistance?
high: pulse upstroke of the vessel will be slowed
low: pulse downstroke of the vessel will be slowed
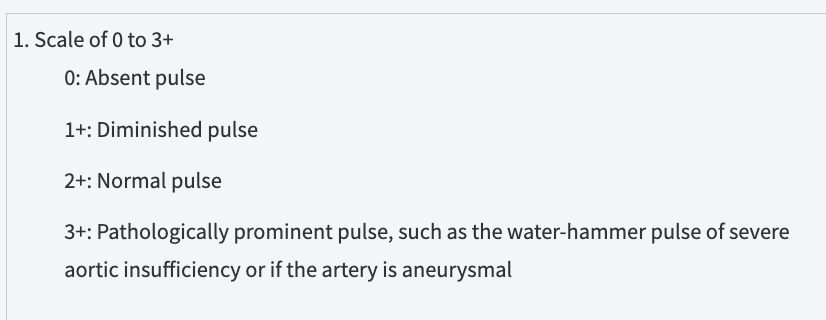
pulse grading scale
when utilizing a doppler examination (AHHD), what is indicated with a monophasic signal?
stenotic or occlusive diseases
describe the capillary refill time test (CRT).
it is measured by pressing the end of the skin just proximal to the wound until the color disappears and by measuring the time for recovery to the original color
what is the normal CRT?
3 seconds; prolonged time = microvascular disease
T or F: CRT is only a screening test and will need more precise vascular testing to rule in/out PAD.
T
what two results from the rubor of dependency test are indicative of PAD?
if the reperfusion takes 30 seconds or longer and causes a dark-red or rubor appearance
the faster the pallor appears in the elevated position or the longer it takes for the rubor to appear in the dependent position
what is the only contraindication for using the ankle brachial index (ABI) test?
if there is an ulcer near the ankle
in what circumstances may the ABI value appear normal when the lower extremity circulation is actually poor?
in patients with diabetes, severe chronic kidney disease, or other diseases that cause vascular calcification → the pedal vessels at the ankle become noncompressible resulting in higher ankle pressures
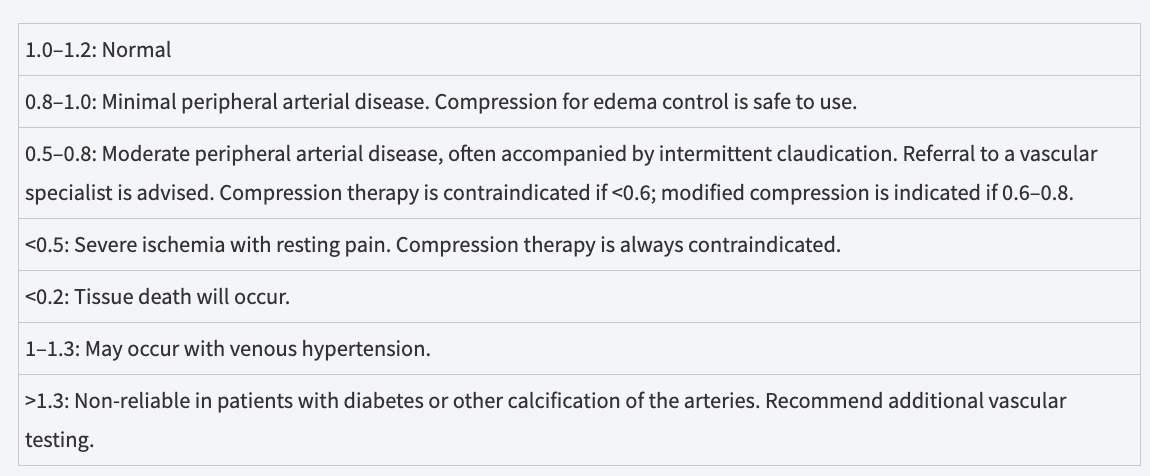
ABI value scale
what method should be used when patients have calcified vessels and abnormally high ABIs?
toe pressure
a toe pressure of ___ infers severe ischemia or critical limb ischemia.
< 30 mmHg
what is segmental pressures?
pressure measured by combining doppler ultrasound or plethysmography with blood pressure measurements at various locations on the arms and legs illustrating differences in blood pressure at specific sites in the extremities and identifying gradients
a normal variation in the pressures between limb segments is ____.
20-30 mmHg
what is pedal acceleration time?
non-invasive vascular ultrasound measurement that evaluates foot perfusion by tracking how quickly blood accelerates in the arteries of the foot (from the onset of systole to peak systole)
what factors does the measurement of transcutaneous oxygen perfusion (skin oxygenation) depend on?
the cutaneous blood flow, the oxyhemoglobin dissociation, and the diffusion of oxygen through the tissues
what values taken during an exercise stress test with ABIs will indicate sufficient claudication caused by PAD?
drop in the ankle pressure of at least 25 mmHg
25% decline of the resting ankle pressure
decrease in the ABI > 0.15
what are the three components of a normal ultrasound waveform that correspond to arterial flow?
rapid antegrade flow reaching a peak during systole due to left ventricle contraction
transient reversal of flow during early diastole due to reflection caused by peripheral resistance
slow antegrade flow during late diastole after closure of the aortic valve generated by large and medium compliant arteries
how are lesions or occlusions identified using a duplex ultrasound?
changes in US waveform characteristics or an increase in peak systolic velocity followed by low velocity
what must be taken into consideration before a patient undergoes an MRI or CT with contrast?
the patient’s renal function and any presence of significant arterial disease
_______ is the gold standard for pre-surgical evaluation of diseased arteries.
arteriography
what is considered “controlled hypertension” in a patient diagnosed with HTN?
systolic pressure less than 130 mmHg and diastolic pressure less than 80 mmHg
what is negative pressure wound therapy (NPWT)?
an advanced medical treatment that uses controlled suction (sub-atmospheric pressure) to pull fluid out of a wound and accelerate the healing process
what are the benefits of NPWT?
increased granulation tissue, exudate management, removal of infectious material, promotion of angiogenesis and perfusion, and a decrease in wound size
what are some endovascular interventions?
balloon angioplasty, stents, and subintimal angioplasty
what is revascularization surgery?
restores blood flow in blocked or narrowed arteries or veins by unblocking, bypassing, or creating new pathways for blood to travel to vital organs and tissues
what are the main focuses of post-surgical care of a patient with revascularization?
prevention of edema, prevention of infection, control of medical conditions, and meticulous wound care
describe the incision care process following a BKA and AKA.
postoperatively: apply a residual limb wrap with short stretch bandages
with a BKA: fit LE with a special boot or cast to prevent knee flexion contractures
after incisional healing and removal of sutures/staples: use shrink socks
what are some mechanisms that can cause venous insufficiency?
venous hypertension, vein valve incompetence, gastroc muscle dysfunction, genetic predisposition, and venous obstruction (DVT or stenosis
how does venous hypertension occur?
when the veins fill from both arterial flow and retrograde flow due to dysfunctional valves
T or F: venous function is influenced by family history, physical activity, ankle injury or immobility, and changes in estrogen and progesterone.
T
list the three classifications of CVI (chronic venous insufficiency)?
primary CVI: valve failure is the result of weakness in the vessel wall or valve leaflets
secondary CVI: failure in response to a previous event (intra-venous vs. extra-venous damage)
congenital CVI: results from venous angiodysplasias and vascular malformations
what are the three theories of CVI pathophysiology?
fibrin cuff formation
growth factor trapping
white blood cell trapping
what’s the difference between the origination of the superficial and deep venous systems?
superficial: originate at the dorsal and deep plantar veins of the foot, emptying into the dorsal venous arch
deep: originate within the digital veins of the foot, emptying in to the deep venous arch
how do the superficial and deep venous systems connect?
via perforating veins that cross through the fascial layers at various points in the LEs
what are varicose veins?
swollen, twisted, and bulging blood vessels that develop when damaged vein walls and valves cause blood to pool or flow backward, stretching the veins and forcing them to swell
where are varicose veins usually located?
around the saphenofemoral and saphenopopliteal junctions and in the perforating system
what factors can alter venous tone and therefore venous return/flow?
sympathetic discharge, thermoregulatory centers in the brain, temp changes, pain, emotional stimuli, and volume canges
T or F: all veins, including the superior and inferior vena cavas, have valves to prevent retrograde blood flow.
F; the SVC and IVC do not have valves
what is post-thrombotic syndrome?
occurs when a blood clot damages the veins and valves, causing blood to pool, and creates lasting venous pressure → chronic leg pain, swelling, heaviness, and skin changes
list the signs and symptoms associated with post-thrombotic syndrome?
aching or cramping in the leg
feeling that the leg is heavy or tired
itching or tingling
chronic edema
varicose veins
hemosiderin staining of the skin
ulceration
what is May-Thurner syndrome?
a vascular condition where the right iliac artery compresses the left iliac vein against the lower spine slowing blood flow from the left leg → blood pooling, leg swelling, and significantly increasing the risk of DVTs
what causes the classic CVI sign of hemosiderin staining.
as venous pressure increases, the vessel breaks down and spills serum proteins and red blood cells into the interstitial areas where they are trapped by the interstitial edema → by-products of the dead RBCs cause the dark discoloration
name some skin changes associated with CVI.
lipodermatosclerosis, atrophie blanche, brawny edema, champagne-bottle leg, and fibrotic/hypertrophic skin
edema associated with venous pathology is usually _______.
unilateral
edema is a common indicator of CVI, but when should it raise concern for another pathology?
edema that has a sudden onset, is hard and indurated, and does not respond to compression may indicate obstruction of the pelvic or abdominal lymph nodes by malignancy
describe the clinical presentation of venous insufficiency wounds.
located in the distal 1/3 of LE
present with uneven edges, shallow depth, changes in periwound skin, and a fibrotic/granular wound base
serous drainage is likely and may be painful (according to the book)
what does the CEAP CVI classification look at?
Clinical signs
Etiology
Anatomy
Pathophysiology
CEAP: C0
no visible or palpable signs of venous disease
CEAP: C1
telangiectasia or reticular veins—small dilated veins (0.5–1 mm in diameter) that develop in the superficial skin as a result of venous hypertension
CEAP: C2
varicose veins—dilated, tortuous veins in the lower leg that signify the progression of CVI due to venous hypertension
2R = recurrent varicose veins
CEAP: C3
edema without ulceration
CEAP: C4
skin and subcutaneous changes ascribed to venous disease
4A = pigmentation or eczema
4B = lipodermatosclerosis or atrophie blanche
4C = corona phlebectatica
CEAP: C5
C4 with healed ulceration signs
CEAP: C6
skin changes as defined above with active ulceration
6R = recurrent venous ulceration (symptomatic vs. asymptomatic)