7. Hypersensitivity Reaction Type 1
1/6
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
7 Terms
Core Concepts & Definition
Definition: A rapidly developing immune reaction occurring within minutes of re-exposure to an antigen (allergen) to which the individual has been previously sensitized.
Key Mediators: IgE antibodies, Mast cells, and Basophils.
Target Antigens (Allergens): Typically harmless environmental proteins (e.g., pollen, dust mites, animal dander, certain foods, insect venom, specific drugs like penicillin).
Genetic Predisposition: Atopy is the genetic tendency to develop allergic diseases. Atopic individuals have higher baseline levels of IgE and Th2 cells.
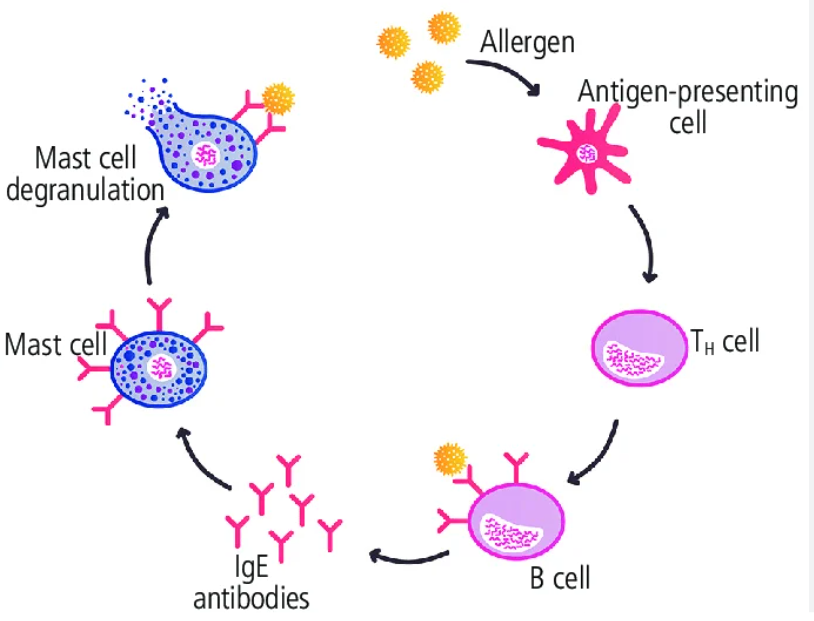
Pathogenesis
Sensitization (first exposure)
Re-exposure and Effector Phase
Phase 1: Sensitization (First Exposure)
The body sees the allergen for the first time and prepares the "weapon."
Antigen Presentation: Allergen enters the body and is picked up by an Antigen-Presenting Cell (APC), usually a dendritic cell, which presents it to a naïve CD4+ T cell.
Th2 Differentiation: Crucially, the CD4+ T cell differentiates into a Th2 helper T cell.
Cytokine Release: The Th2 cell secretes specific, high-yield interleukins (ILs):
IL-4 & IL-13: Stimulates B cells to undergo class switching and produce IgE antibodies (instead of IgM/IgG).
IL-5: Promotes the development and activation of eosinophils.
IgE Binding (Arming the Mast Cell): The newly created IgE antibodies circulate and bind strongly to FcεRI receptors (high-affinity IgE receptors) on the surface of tissue mast cells and circulating basophils.
Result: The mast cell is now "sensitized" or "armed," but no symptoms occur yet.
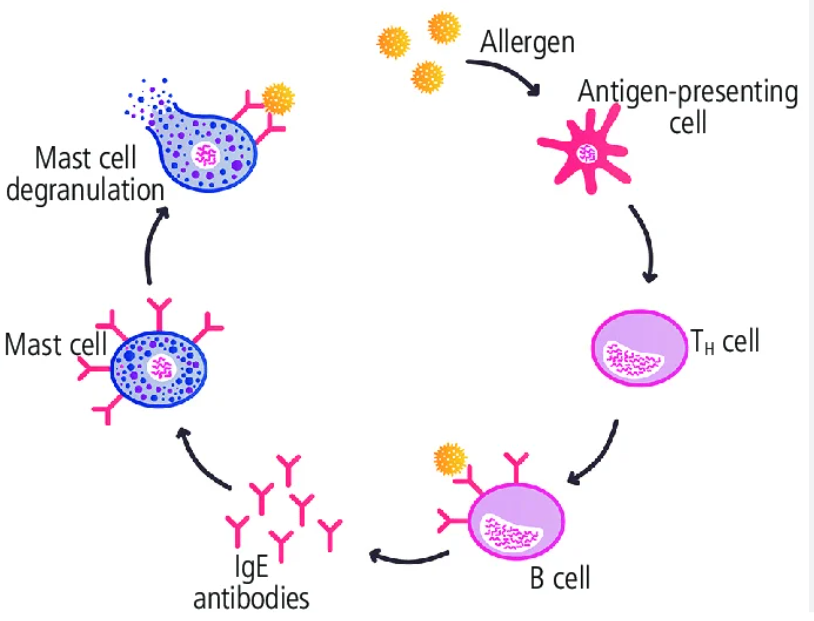
Phase 2: Re-exposure and Effector Phase
The allergen returns, triggering the armed mast cells.
Cross-linking: The allergen enters the body and binds to the IgE antibodies currently sitting on the mast cell.
The Trigger: The allergen must bind to at least two adjacent IgE molecules. This cross-linking of IgE receptors is the mechanical signal that activates the mast cell.
Degranulation: The mast cell rapidly releases its contents. This occurs in two distinct waves (Immediate vs. Late phase).
A. Immediate Response (Minutes)
Driven by the release of preformed mediators stored inside mast cell granules.
Histamine (Most Important):
Causes profound vasodilation (erythema/redness).
Increases vascular permeability (edema/swelling/hives).
Causes smooth muscle contraction (bronchospasm).
Stimulates nerve endings (itching/pruritus).
Proteases (Tryptase & Chymase): Cause local tissue damage. (Note: Serum tryptase levels can be measured clinically to confirm severe anaphylaxis).
Chemotactic factors: Eosinophil Chemotactic Factor (ECF) and Neutrophil Chemotactic Factor (NCF) call other immune cells to the area.
Late-Phase Reaction (2 - 24 hours later)
Driven by newly synthesized lipid mediators and cytokines. This phase causes tissue damage without additional allergen exposure.
Arachidonic Acid Metabolites:
Leukotrienes (C4, D4, E4): Extremely potent vasoactive and spasmogenic agents. They are 1000x more potent than histamine at causing bronchospasm and increased vascular permeability.
Leukotriene B4: Highly chemotactic for neutrophils, eosinophils, and monocytes.
Prostaglandin D2: Causes severe bronchospasm and increased mucus secretion.
Cytokines: Continued release of TNF, IL-4, and IL-5 sustains the inflammatory response and brings in a massive wave of Eosinophils (which release Major Basic Protein, damaging host tissue).
Clinical Manifestations
Localized Reactions (Atopic allergy)
Skin (Contact/Ingestion): Urticaria (hives), atopic dermatitis (eczema).
Respiratory tract (Inhalation): Allergic rhinitis (hay fever), Allergic asthma.
GI tract (Ingestion): Food allergies (diarrhea, vomiting).
Systemic Anaphylaxis
Definition: A life-threatening emergency caused by systemic mast cell degranulation (often via IV drugs, bee stings, or severe food allergies).
Pathophysiology: Systemic vasodilation leads to a massive drop in blood pressure (anaphylactic shock). Increased vascular permeability causes laryngeal edema (airway obstruction), and severe smooth muscle contraction causes massive bronchoconstriction.
Treatment: Epinephrine (Adrenaline) is the immediate antidote. It reverses the pathophysiology: causes vasoconstriction (raises BP), bronchodilation (opens airways), and directly inhibits further mast cell degranulation.