Case 11: Richard Strong
1/23
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
24 Terms
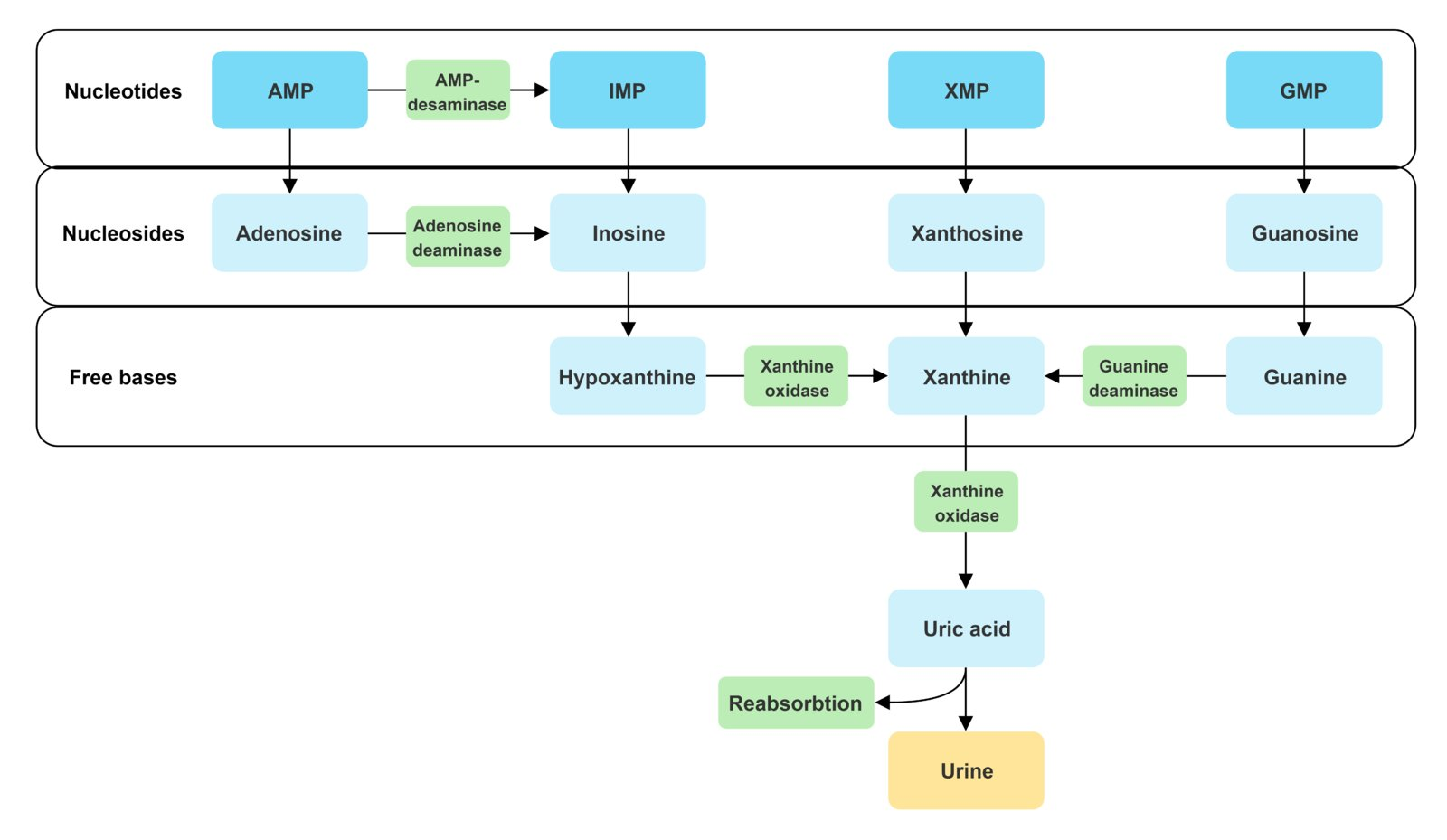
Uric Acid: Production
Purine degradation
AMP/GMP/XMP (xanthosine monophosphate) → Nucleosides (adenosine, guanosine, xanthosine) → Xanine → Uric acid
Xanthis oxidase/dehydrogenase: Xanthine → Uric acid
Uric Acid: Excretion
Urate anion → Urine (60-70%) + GI tract (30-40%)
Glomerulus: Free filtration
PCT: Reabsorption (99%)
PCT: Secretion (50%)
Uric Acid: Renal Handling
Hyperurecemia from…
Underexcretion: Most common
Overproduction
Hyperurecemia: Underexcretion
Decreased glomerular filtration
Increased reabsorption
Decreased secretion
From:
Diuretics
Metabolic dysfunction (hyperinsulinemia, hypovolemia)
Drugs (aspirin)
Hyperuricemia: Overproduction
Increased purine synthesis = Increased purine breakdown
Enzyme deficiency/defects
High cell turnover (malignancy, psoriasis)
Why don’t other mammals get gout?
Uricase (urate oxidase) enzyme convert uric acid → Allontoin = No uric acid buildup
Allontoin: More soluble substrate in urine = Increase excretion in kidneys
Gout: Description
Inflammatory crystal arthropathy
4 Stages:
Hyperuricemia: Asymptomatic
Acute Flares/Attacks: Self-limiting symptoms
Intercritical: Asymptomatic period between flairs
Chronic Tophaceous Gout: Persistent symptoms
Gout: Epidemiology
Risk factors…
Diet (high purine)
Red meat
Seafood
Alcohol
Sweet beverages
Drugs
Diuretics
Cyclosporins
ACE inhibitors
Beta-blockers
Aspirin
Obesity
Male
Older age
Gout: Etiology
Hyperuricemia (> 0.4 mmol/L)
Primary: Idiopathic
Secondary:
Decreased Excretion
Drugs (aspirin, loop diuretics, thiazides, niacin)
CKD
Ketoacidosis
Lactic acidosis
Post-menopause
Increased Production
High cell turnover (tumor lysis syndrome, hemolytic anemia, chemo)
Enzyme defects
Purine-rich diet
Obesity
Hypercholesterolemia
Combined Decreased Excretion + Increased Production: Alcohol consumption + lactic acid
Purine-rich alcohol = Alcohol metabolism products compete for excretion = Decrease uric acid excretion
Gout: Pathophysiology
Hyperuricemia = Uric acid crystals coated in IgG precipitate + deposit in synovial fluid
Triggered by acidosis + low temp (peripheral joints)
Immune cells phagocytose IgG-covered crystals = Release inflammatory markers = Joint inflammation
Chronic: Repeated attacks = Urate crystals + large cells (tophi) aggregate in joint = Deformities + arthritis
Gout: Clinical Presentation
Hyperuricemia: Asymptomatic
Acute Gout Attacks:
Severe joint pain, erythema, decreased ROM, swelling, warmth
At night → Wake from pain
Peak 12-24h + regress after
Fever
Joint skin desquamation (flaking) during recovery
Joints Affected:
Monoarthritis
Asymmetrical
Peripheral joints
Podagra: Big toe MTP
Gonagra: Knee
Chiragra: Finger joints
Intercritical: Asymptomatic
Chronic Gout:
Gouty tophi: Painless hard nodules on joints
Bone tophi: Crystal deposition in bones
Soft tissue tophi: Crystal deposition in external ear, subcutis, tendon sheaths, bursae
Nephrolithiasis (uric acid stones)
Nephropathy
Gout: Investigations
Arthrocentesis + synovial fluid analysis
Blood test
Imaging
Gout Investigations: Arthrocentesis + Synovial Fluid Analysis
Gold standard
Polarized light microscopy: Needle-shaped urate crystals
Parallel optical axis = Yellow
Perpendicular optical axis = Blue crystals
WBC > 50 000/mm3
Gram stain: Neg
R/O septic arthritis
Gout Investigations: Blood Test
CBC
Increased WBC + ESR
Serum uric acid
Usually increased (> 6.8 mg/dL)
Screening:
Creatinine → CKD
Lipid → Dyslipidemia
Glucose → DM
Gout Investigations: Imaging
Supportive
US:
Joint inflammation
Bone erosions
Double contour sign: Hyperechoic band of crystals covering hypoechoic articular cartilage
XR:
Acute: Normal
Chronic:
Periarticular erosions: Punched-out lytic bone lesions + spiky overhanging edges
Radiopaque soft tissue: Swelling
Gout: General Treatment
Lifestyle changes
Limit alcohol
Diet changes: Limit purine-rich foods + high-sugar drinks
Weight loss
Acute Gout: Treatment
Nonpharmacological
Pharmacological
Acute Gout Treatment: Nonpharmacological
Rest
Ice
Acute Gout Treatment: Pharmacological
Initiate ≤ 24h
NSAIDs
Ex: Naproxen, indomethacin, ibuprofen
Glucocorticoids
Systemic (oral, parenteral, intramuscular) or intraarticular
Ex: Prednisone, prednisolone
Colchicine
Urate-lowering therapy (ULT)
Ex: Xanthine oxidase inhibitors (allopurinol), uricosurics
Acute Gout Treatment: Colchicine
MOA: Inhibit microtubule polymerization = Inhibit urate crystal phagocytosis + inhibit WBC migration = Decrease inflammation
Acute Gout Treatment: ULT
Indications:
≥ 2 attacks/year
Chronic gout imaging
Tophi development
Chronic Gout: Treatment
ULT
Chronic Gout Treatment: ULT
First-line
Indications: Same as acute
Contraindications:
Acute gout flare
Asymptomatic hyperuricemia
Agents:
First-Line: Xanthine oxidase inhibitors (allopurinol)
Second-Line: Uricosurics (probenecid)
Third-Line: Recombinant uricase (pegloticase)
Anti-Inflammatory Prophylaxis: 1 week before ULT prevent worsening symptoms
Colchicine
NSAIDs
Glucocorticoids
Gout: Complications
Nephrolithiasis: Uric acid stones
Uric acid nephropathy: Stone deposition in kidney = Inflammation
HTN
Renal failure
Bursitis