L04 The Dopaminergic System
1/64
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
65 Terms
DA once of the most misunderstood NTs
5HT + DA connected and perhaps explains enjoyment state → incorrect oversimplification → it plays a much more complex role
this view leads to idea that it is good thing to raise DA through several ways (thru good foods) → and then leads to idea that some ways are better than others (TV, alcohol, junk food = bad)
leads to view that bad DA increases are associated with TV/substances and ultimately leads to addiction
Dopamine (DA)
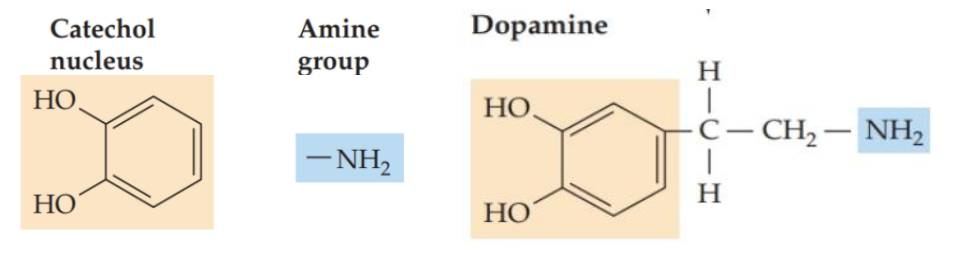
Monoamine (w/5-HT, NA + ADR) and catecholamine (w/NA + ADR)
Catecholamines have a similar structure as well as shared synthesis + metabolism pathways
Shared drug sensitivity
DA fits into 2 categories
this means that something like monoamine oxidase could affect DA because DA is a monoamine; or the enzyme called catechol-methyl transferase could also affect DA because DA is a catecholamine
structural designations matter because compounds structured in the same way tend to be involved in the same synthesis + metabolism pathways as well
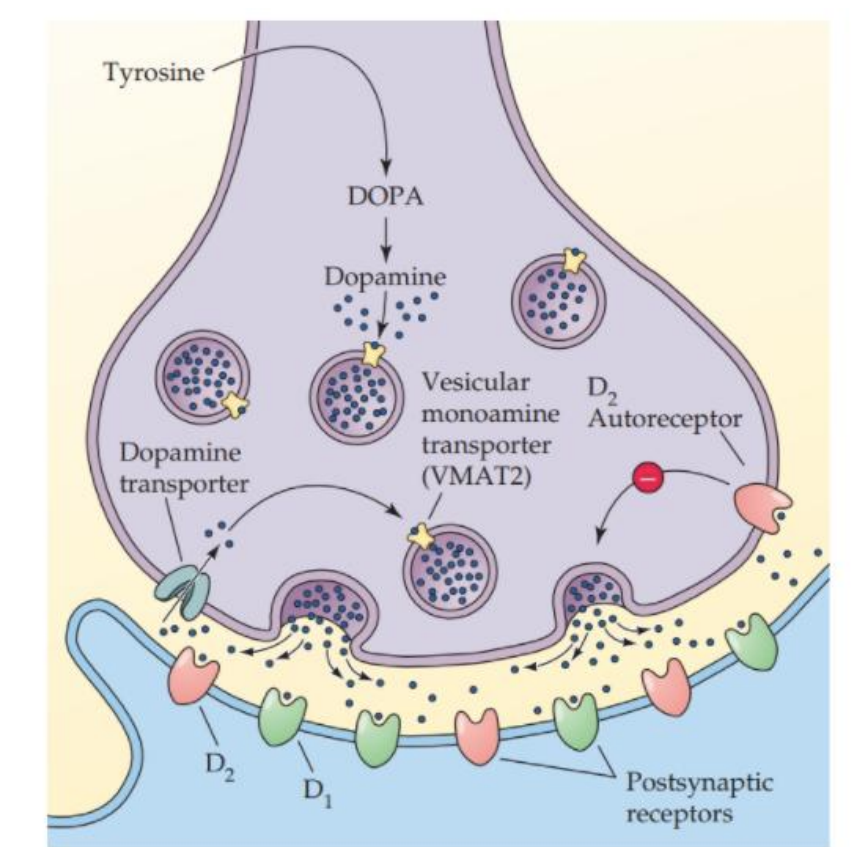
A dopaminergic neuron
Synthesis
Vesicular storage
Transport
Dopamine release
Receptors (including autoreceptors)

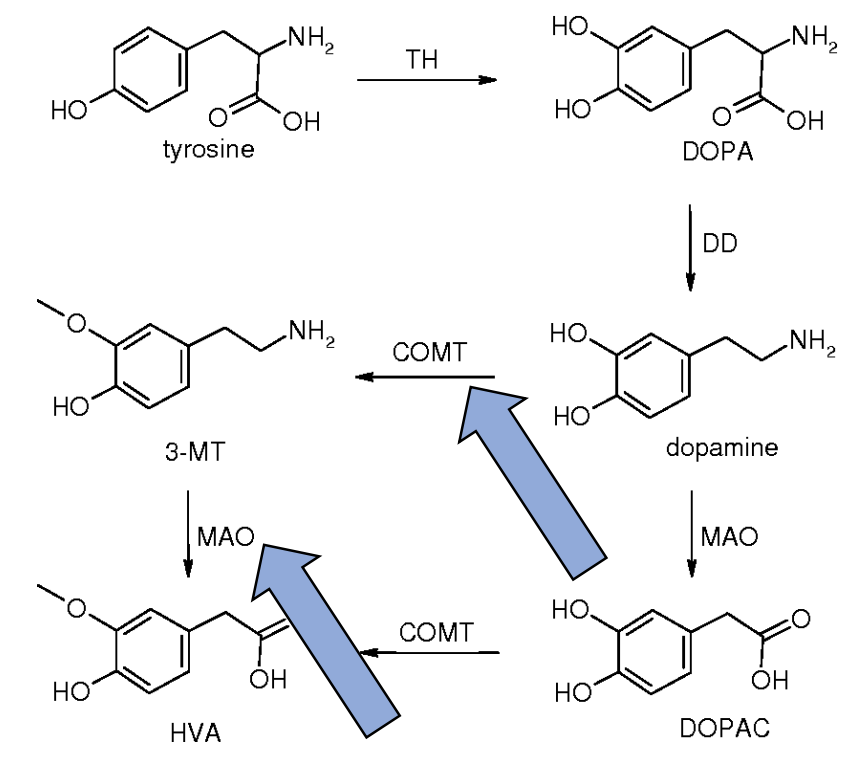
Synthesis + Metabolism (precursor → dopamine)
Precursor is tyrosine
Rate-limiting step is tyrosine hydroxylase (TH)
Metabolized by Dopamine-β-hydroxylase (DBH) to NA
In turn, NA is used for ADR (L05)
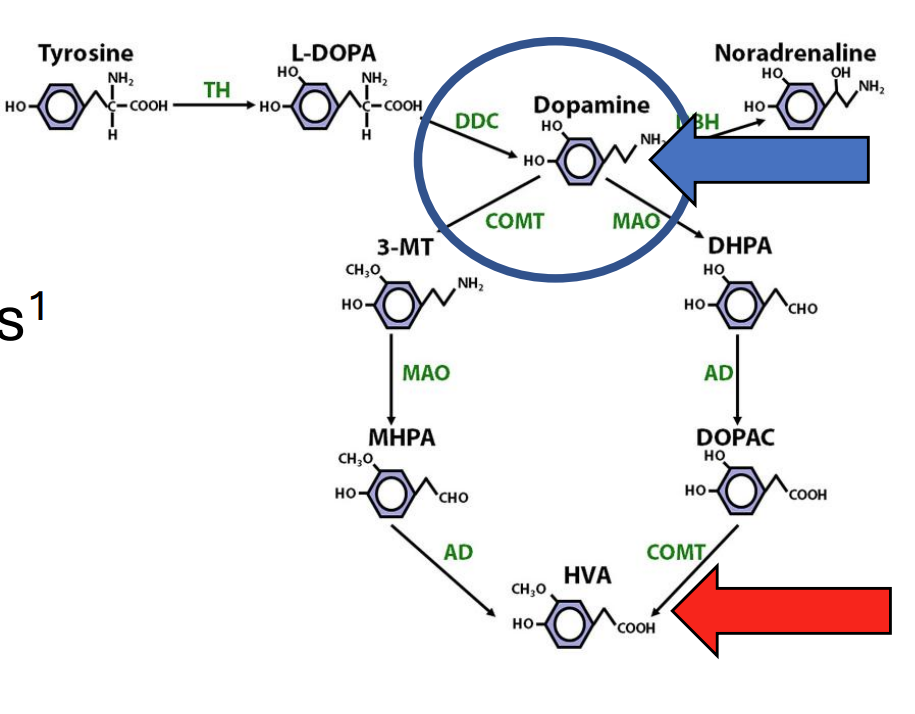
Metabolism (breakdown + metabolite)
Breakdown by catechol-O-methyl-transferase (COMT) and monoamine oxidase (MAO)
Regional variation (e.g. more COMT in PFC)
Potential therapeutic targets
HVA (homovanillic acid) is a metabolite
Sometimes used as a surrogate measure of DA levels
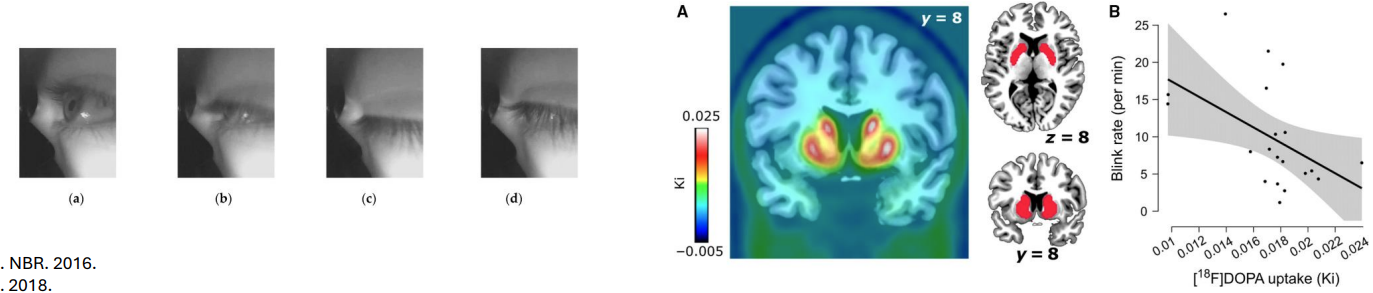
Other measures
Spontaneous eye-blink rate (EBR) was once favored
EBR was correlated with cognitive processes and was thought to be correlated with DA levels
More recent studies question this idea (found reverse)
Individual differences
DA signaling may vary between healthy individuals
Reasons unclear but many possibilities (e.g. Genetic variations in COMT, DA synthesis and more)
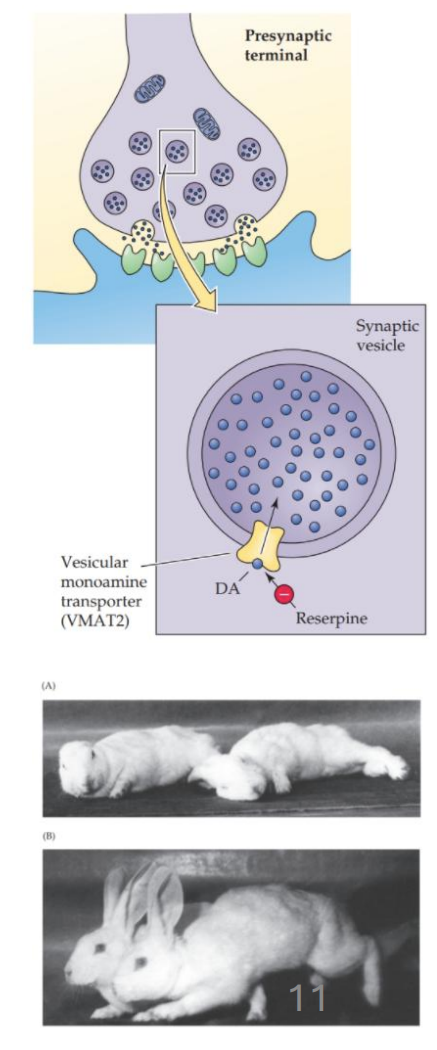
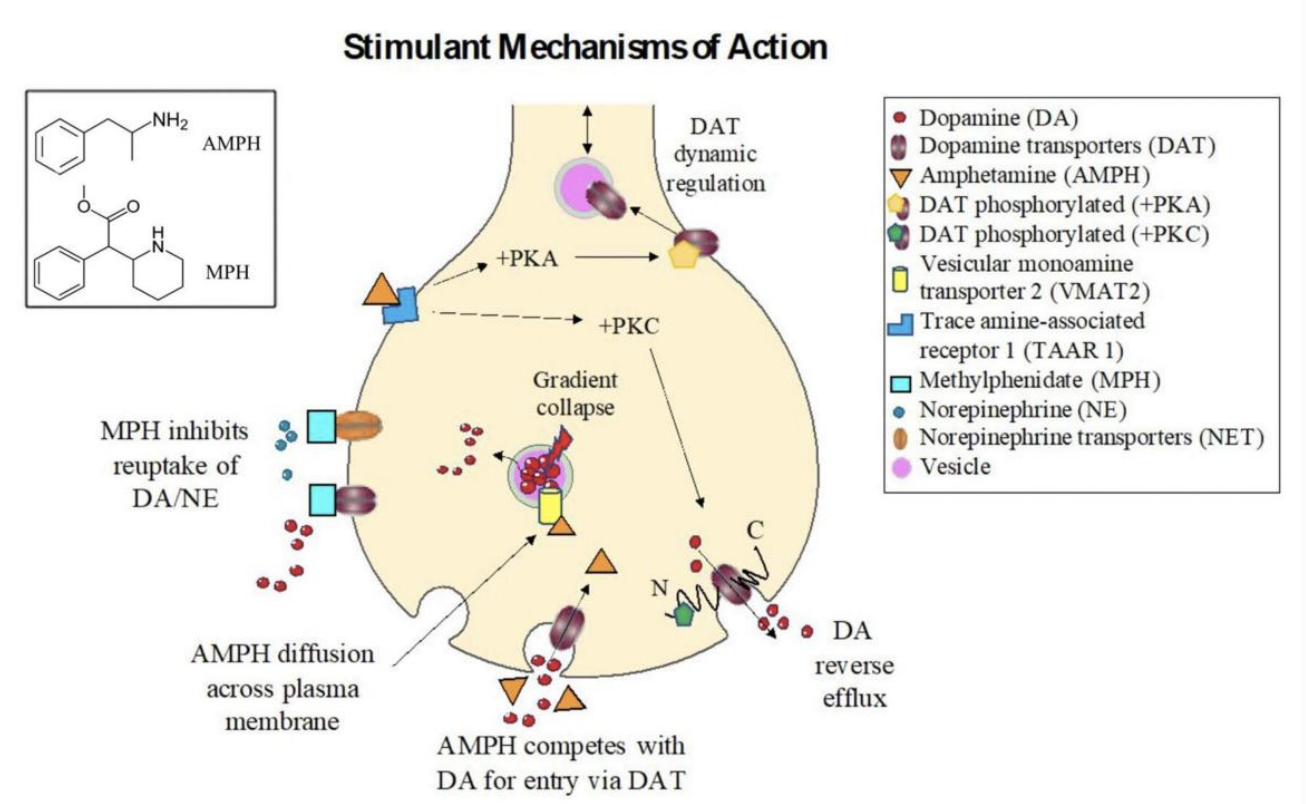
Vesicular storage
DA is transported into vesicles by VMAT2
Reserpine inhibits VMAT2
With reserpine: transmitter levels drop, sedation and depression-like behavior observed
Effects of VMAT2 inhibition are reversed by L-DOPA
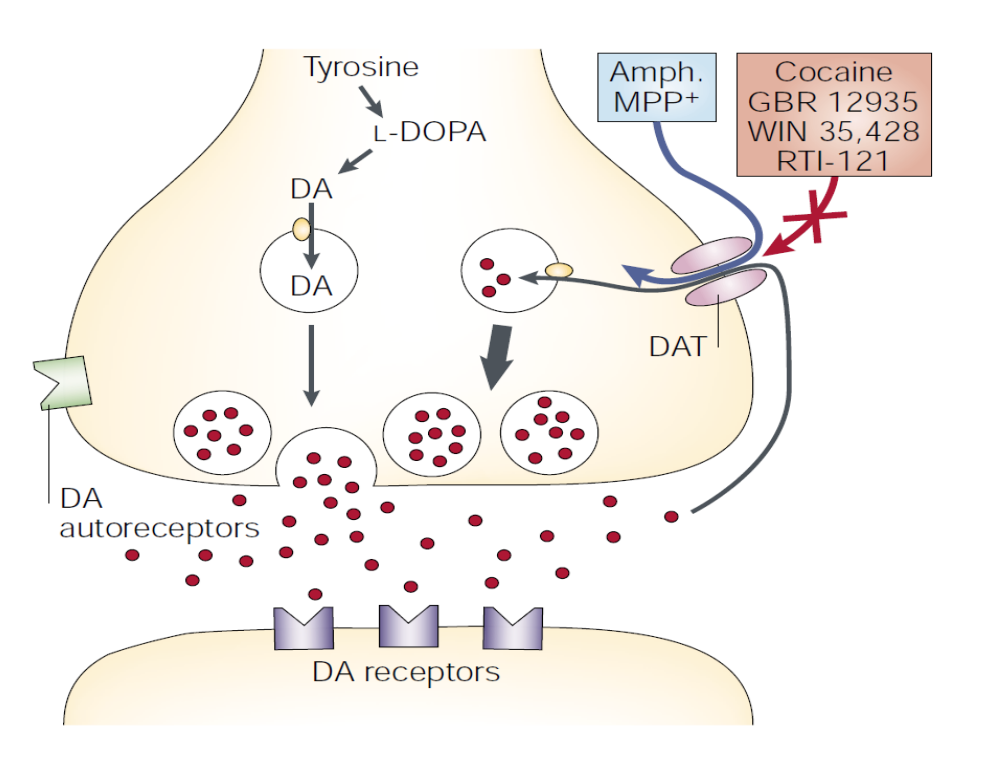
Transport
The dopamine transporter (DAT) brings extracellular DA back into the cell
Many clinical drugs (e.g. for ADHD) and drugs of abuse (e.g. cocaine) affect DAT
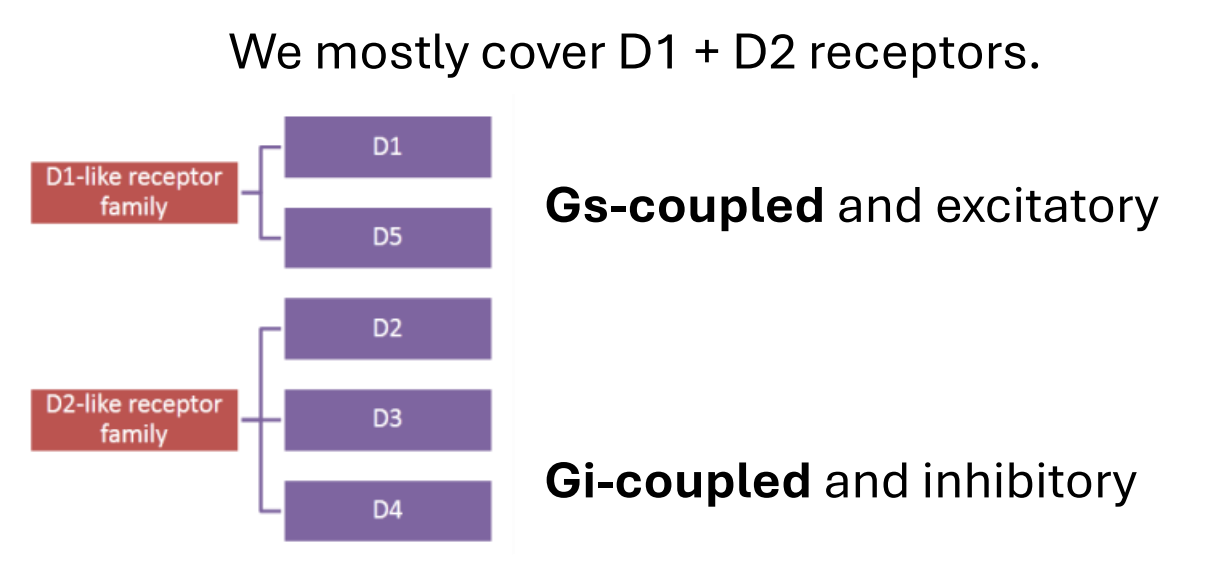
DA receptors
We mostly cover D1 + D2 receptors.
Gs-coupled and excitatory
Gi-coupled and inhibitory
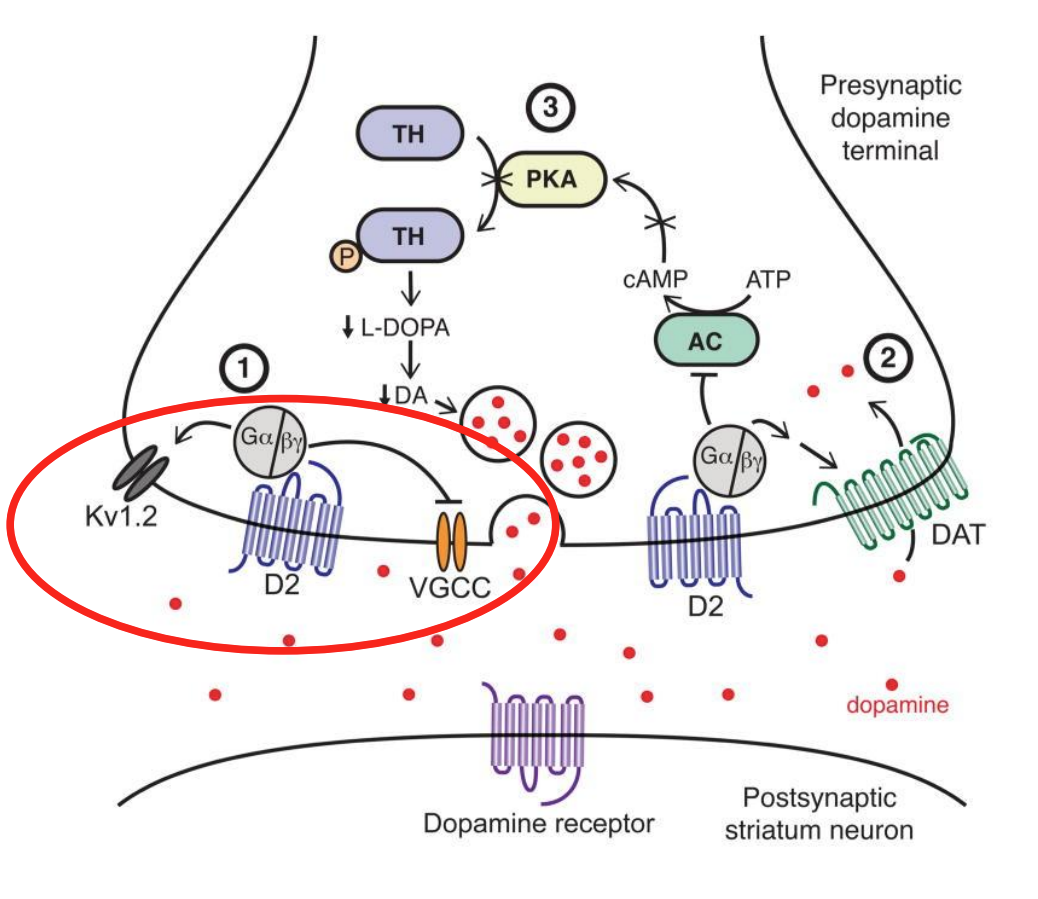
D2 autoreceptors
Inhibitory feedback following DA release
Affect K+ channels and voltage-gated Ca2+ channels to limit future DA release
Dopamine in the body
Peripheral dopamine (outside the brain) has specific functions
Vascular tone, Immune function and more
Neural dopamine (our interest, inside the brain) has different functions
The two compartments are separate
Peripheral DA doesn’t enter the brain (BBB)
Complicates inference of neural DA through peripheral fluids
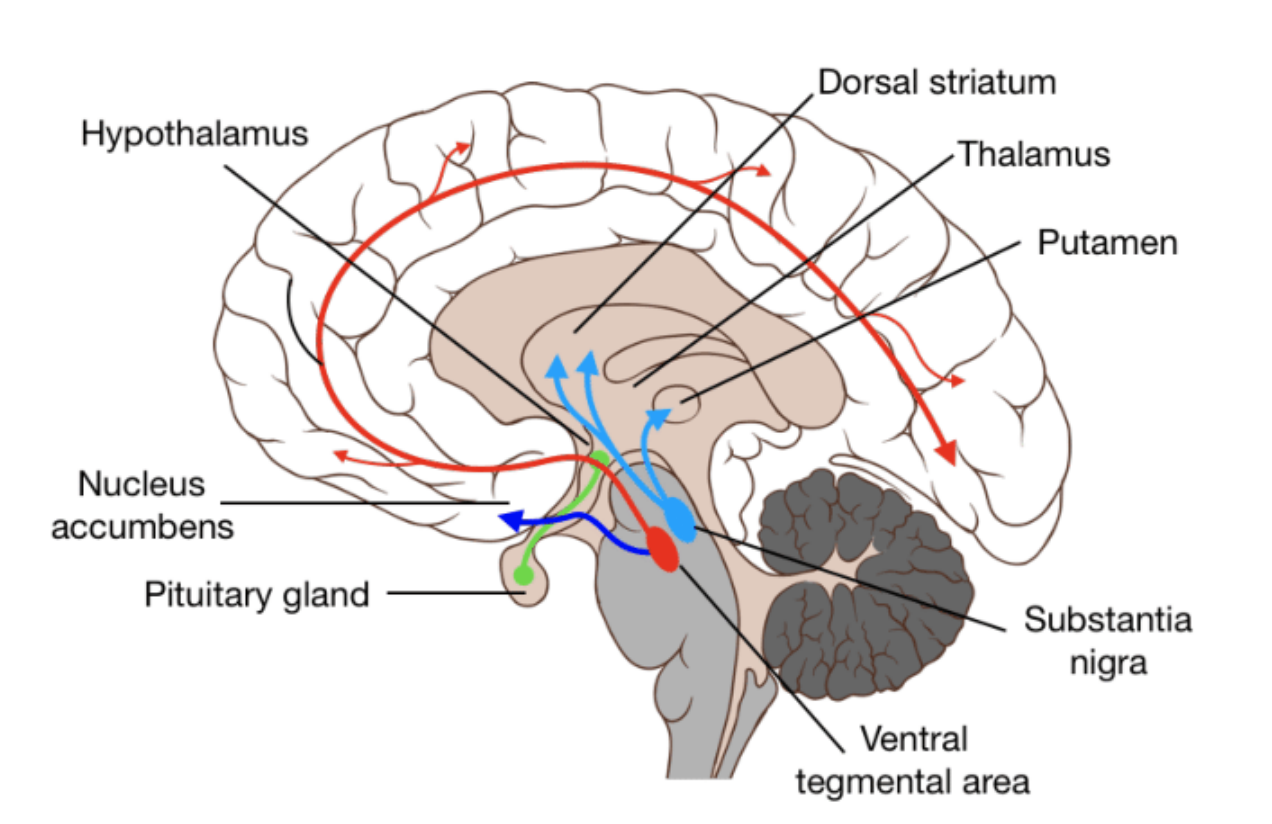
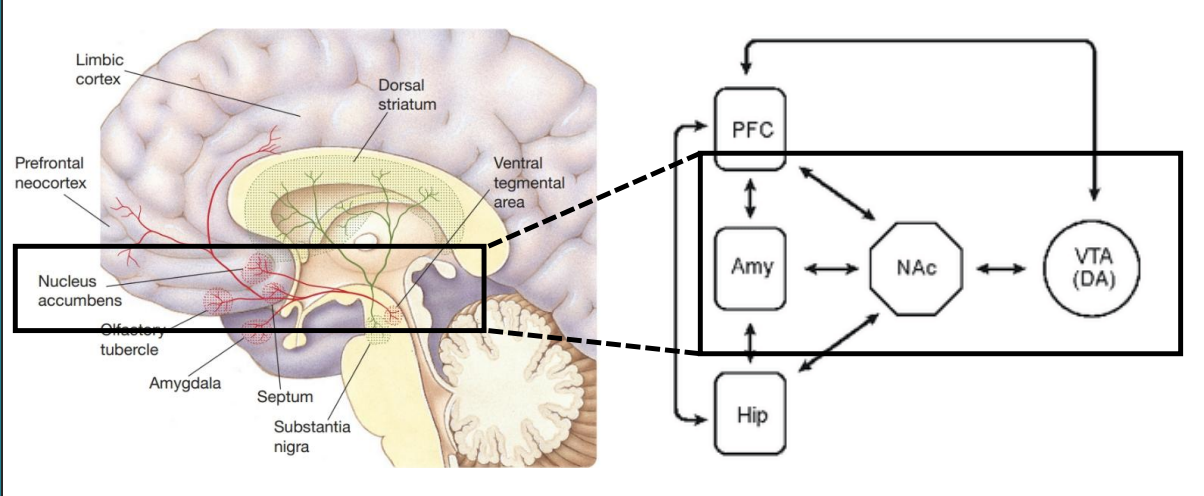
DA Pathways
Four pathways, implicated in different functions and different disorders.
Mesostriatal/Nigrostriatal = midbrain (SN) to striatum
Role in movement
80% of your brain’s DA is in this pathway
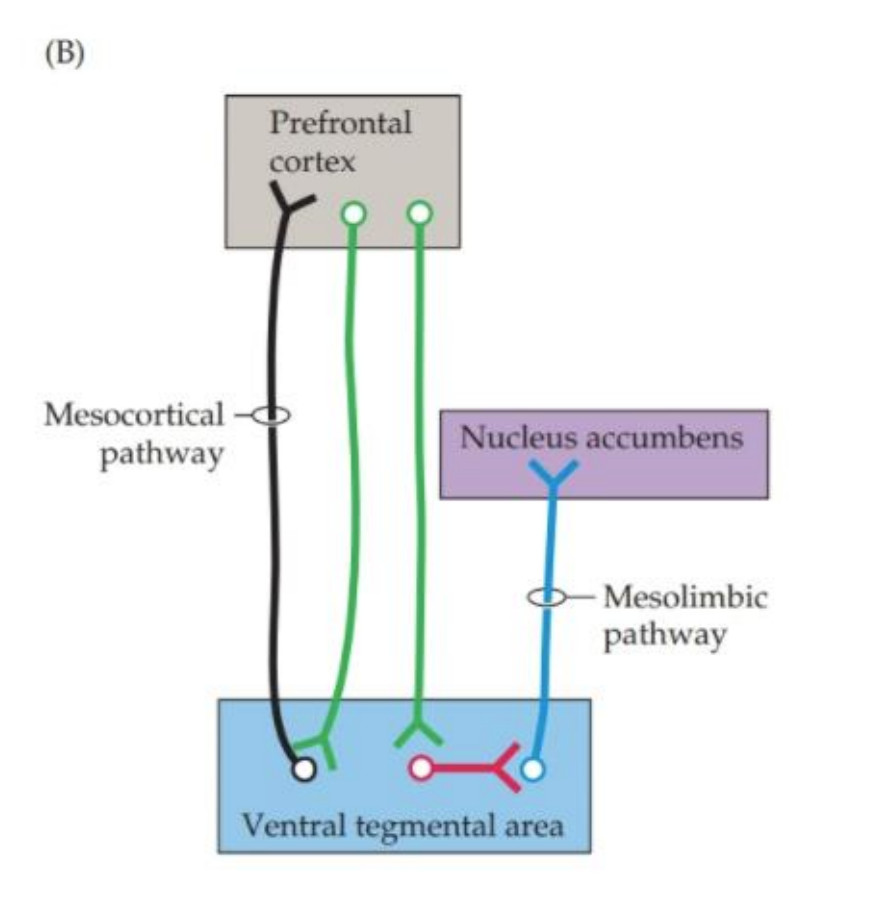
Mesocortical = midbrain (VTA) to cortex (PFC) (boxed)
Role in cognition and other functions
Mesolimbic = midbrain (VTA) to limbic system (BG) (boxed)
Role in motivation and other functions
Tuberoinfundibular = hypothalamus to pituitary
Hormones (prolactin release)
The Nervous System + Movement
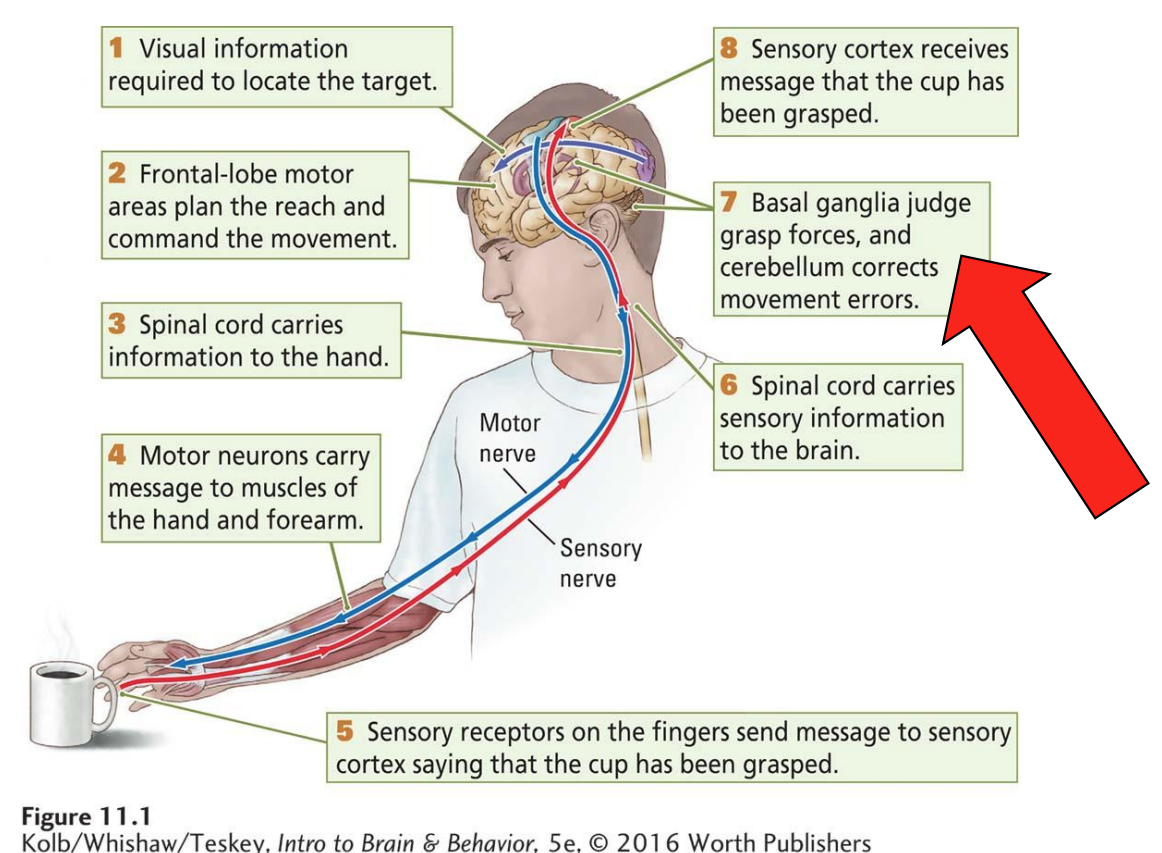
Basal Ganglia (BG)
Group of structures involved in movement
Suppression, facilitation, etc.
Diverse inputs
including the frontal cortex
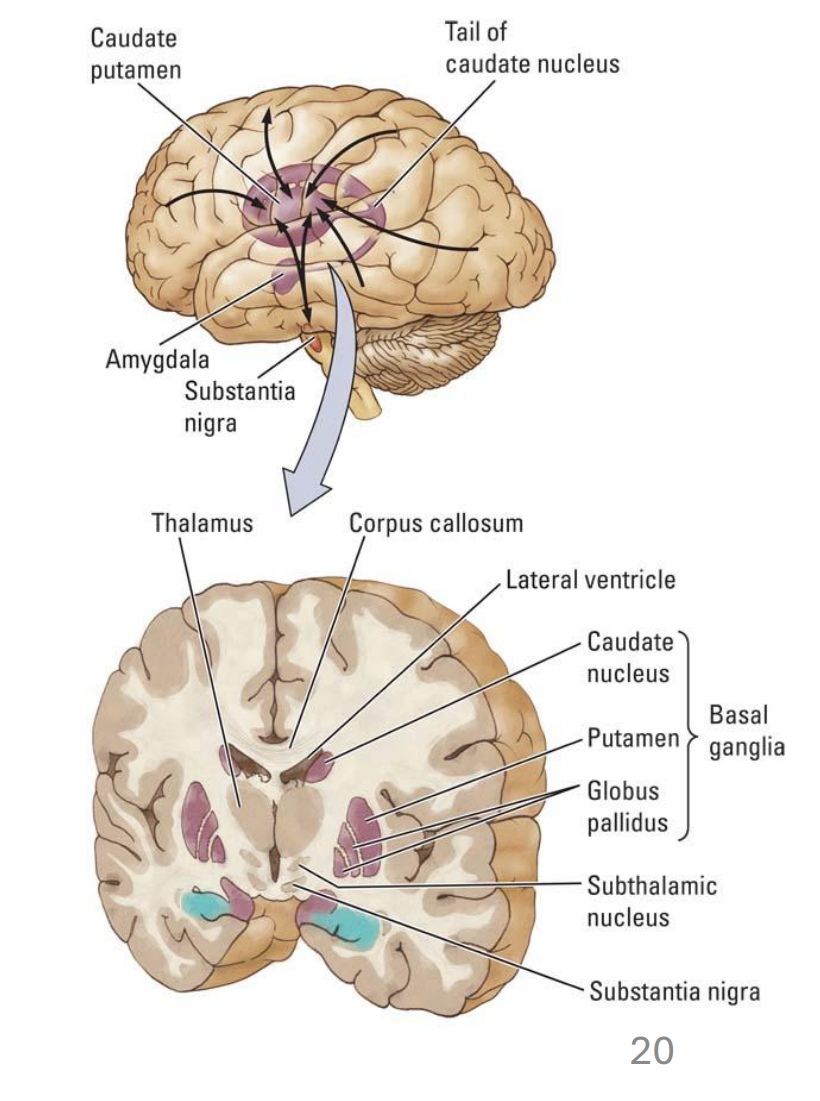
Includes the caudate, putamen (= dorsal striatum), globus pallidus, subthalamic nucleus and substantia nigra
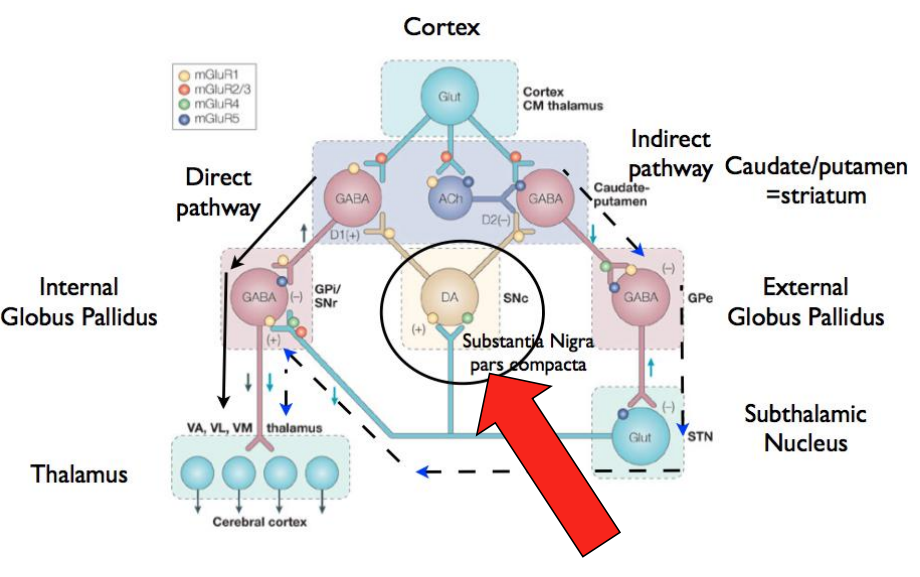
SM in Movement
SN neurons use DA to signal to other structures
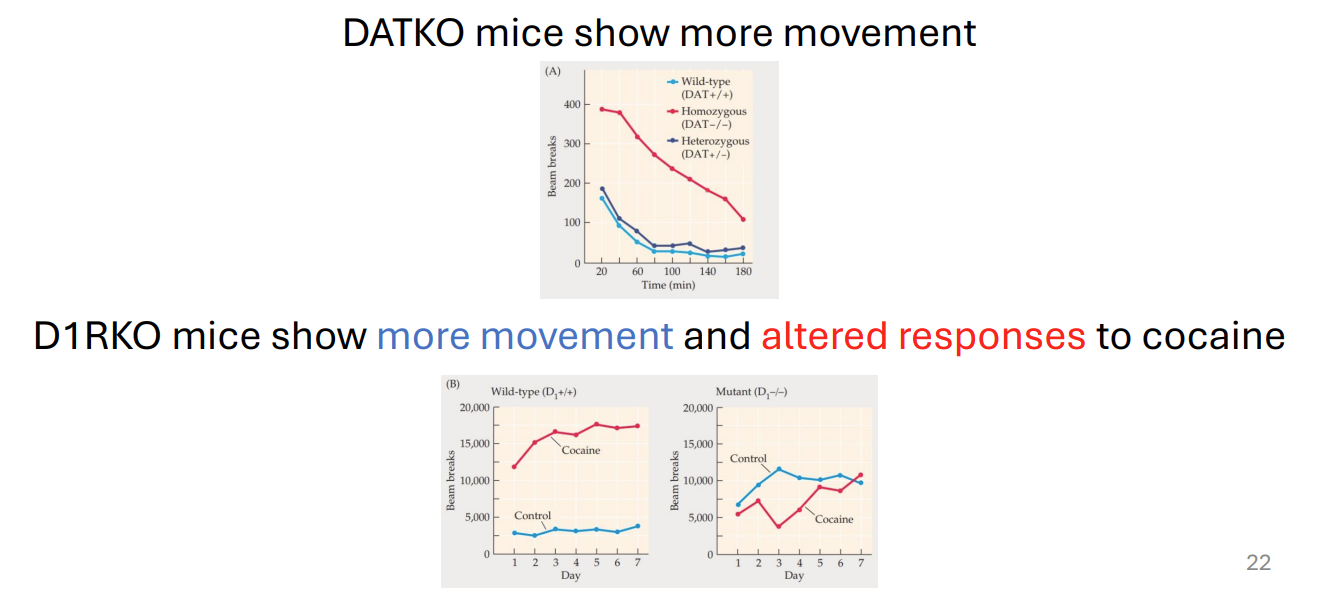
Altered DA, altered movement!
DATKO mice show more movement
D1RKO mice show more movement and altered responses to cocaine
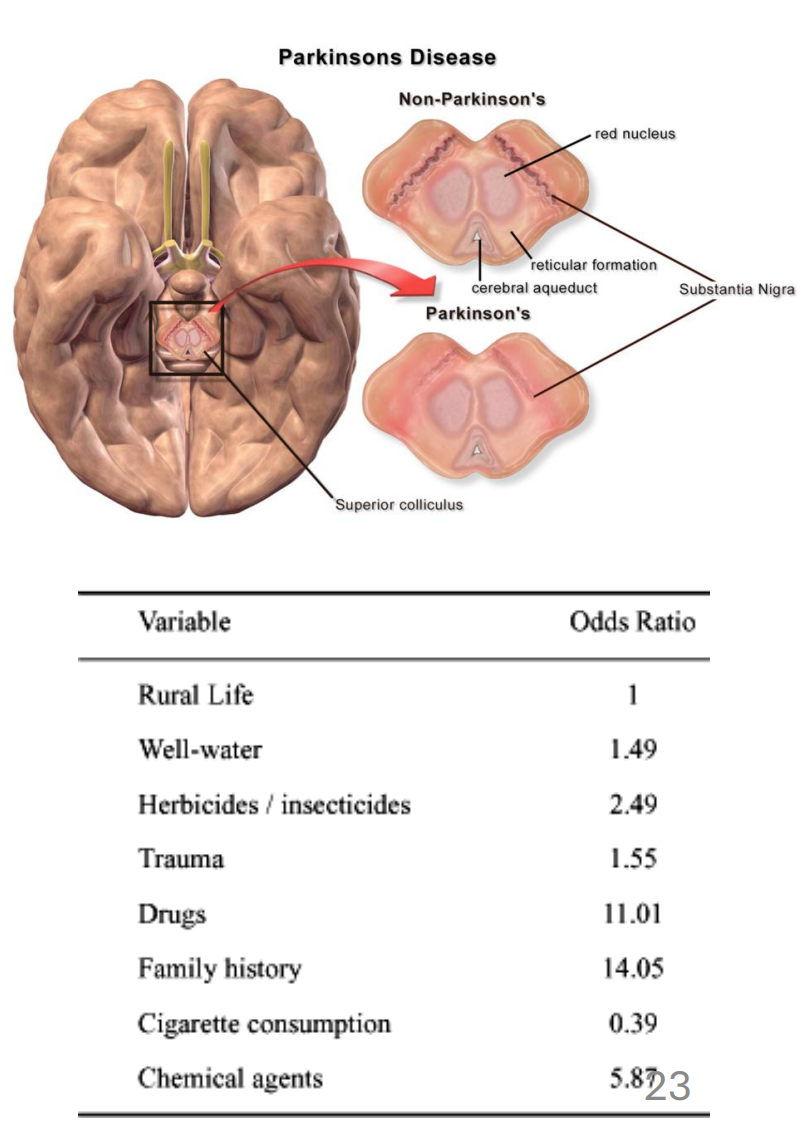
Parkinson’s Disease (PD)
Progressive disorder affecting movement*
Associated with loss of SN neurons (~60% post-mortem)*
Age is a major factor; genetics might contribute also (α-synuclein) as might certain environmental factors
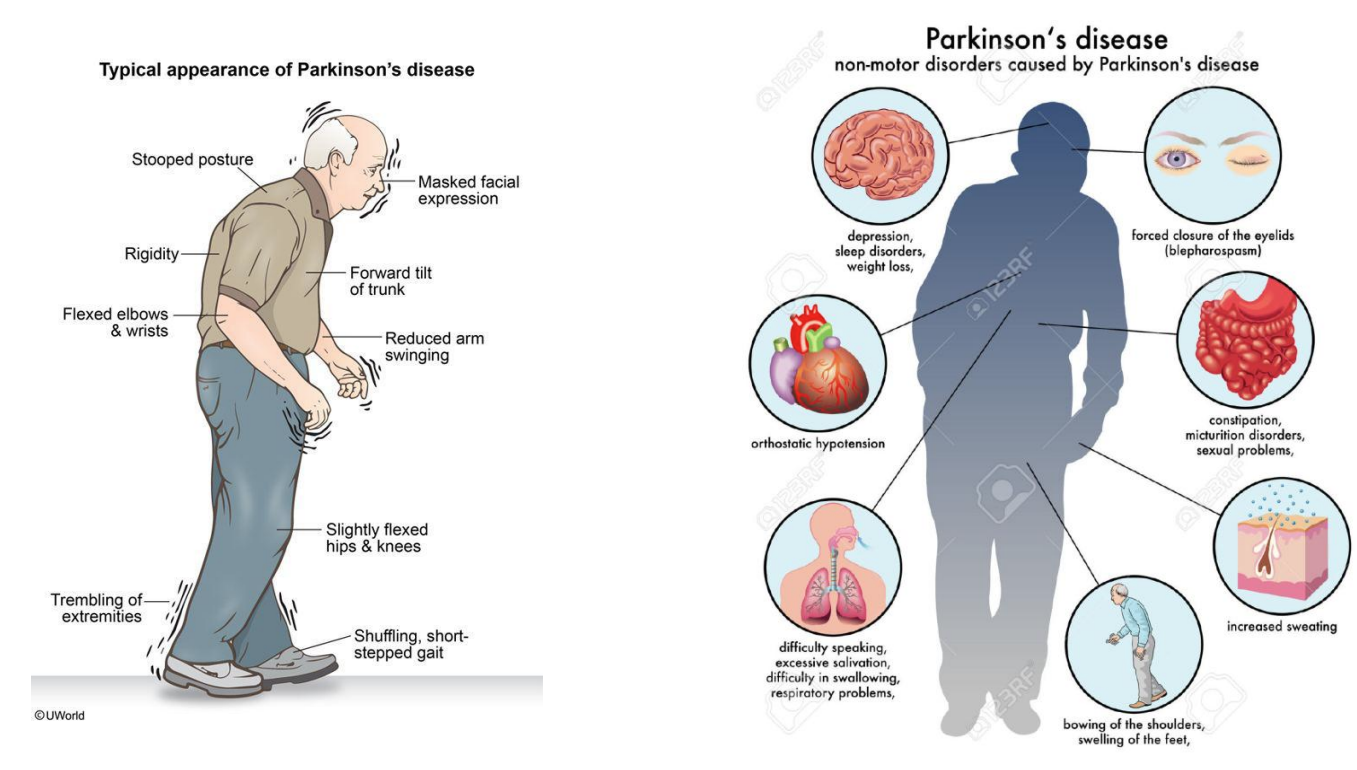
PD symptoms (motor + non-motor)
Increased risk of impulse control disorders has been observed but may be associated with medication.
If the problem is ‘too little’ DA, would pharmacologically increasing DA levels be a treatment?
Increasing DA in PD
We cannot administer DA directly as it does not cross the blood-brain barrier
L-DOPA, however, crosses and can be made into DA
Drugs for PD can include L-DOPA (levodopa)

Increasing DA through other targets
Limit metabolism of DA with monoamine oxidase B inhibitors + catechol-O-methyl transferase inhibitors
Concerns about drug approaches
L-DOPA non-selectively increases DA levels non-selectively
Other systems are affected (e.g. mesocortical)
DA modulations by drugs do not restore normal signaling
Imprecise (timing and intensity)
Side effects (e.g. nausea, dyskinesia, psychosis and delusion)
Other treatment strategies being explored (e.g. DBS)
DA, motivation and substance use disorder

Key concepts
Cost: Effort (time and energy) to obtain
High ~ many bar presses, Low ~ few bar presses
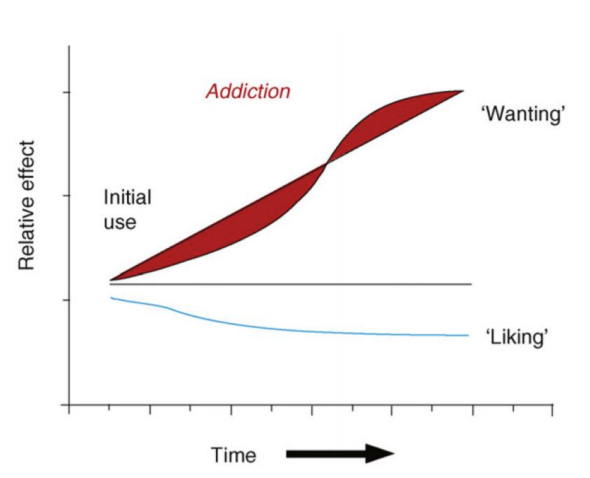
Motivation: Drive to obtain (~ wanting, incentive salience)
More motivated, more willing to tolerate high cost
Pleasure: Emotional response to acquisition (~ liking)
All are inter-related and regulated by striatal DA.
Reward System
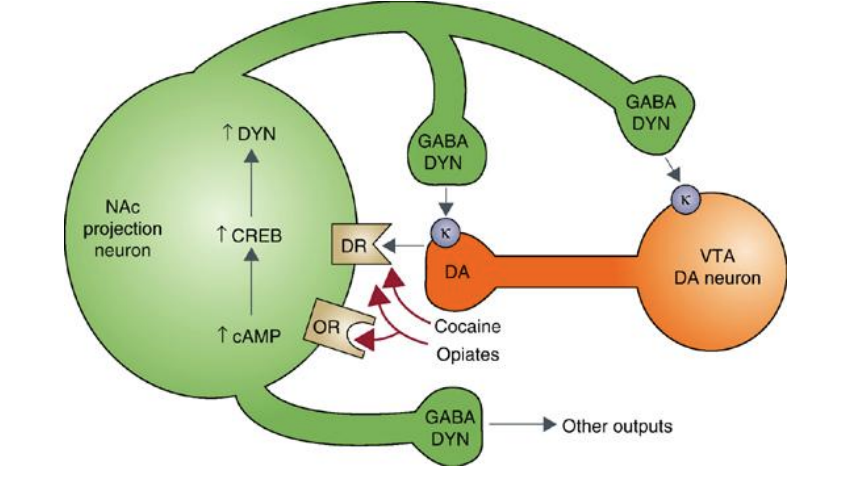
Many structures are in the mesolimbic pathway (DA)
One key synapse is well-studied: Ventral Tegmental Area (VTA) → Nucleus Accumbens (NAc)
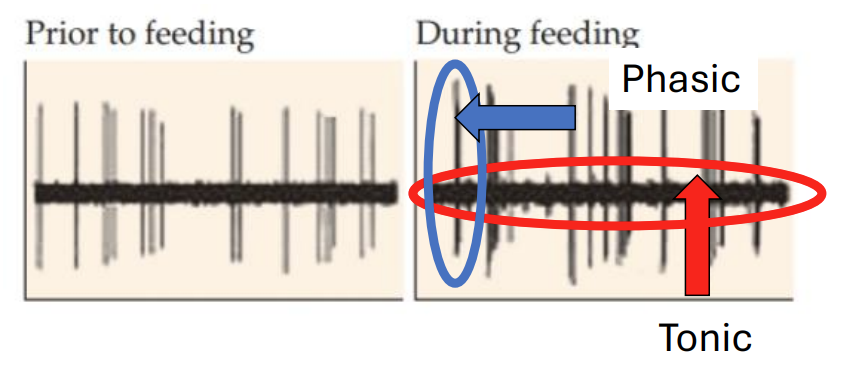
DA neurons in the VTA
Phasic DA: Brief, strong bursts (situational; ~ DA hits)
Tonic DA: Weaker, baseline level over time
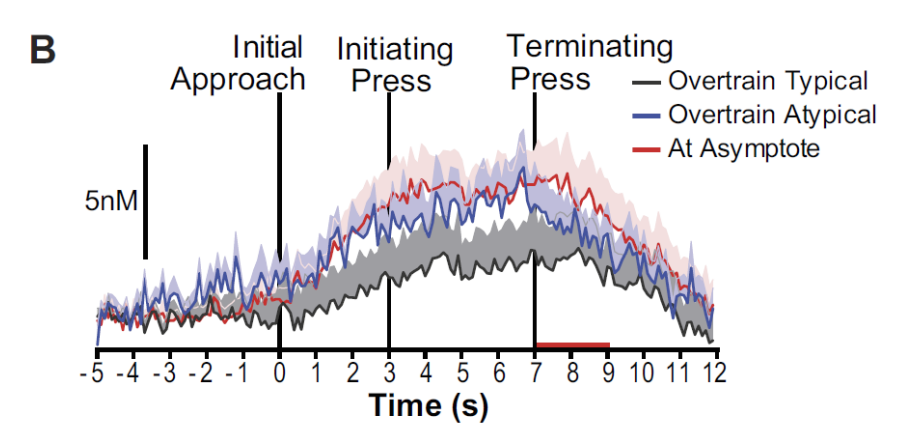
DA ramping
DA concentration increasing leading up to an action performed for reward
Nucleus accumbens
Thought to play a role in liking; contains so-called hedonic hotspots
Circuit for liking may be small, circuit for wanting could be larger and involve dopaminergic transmission
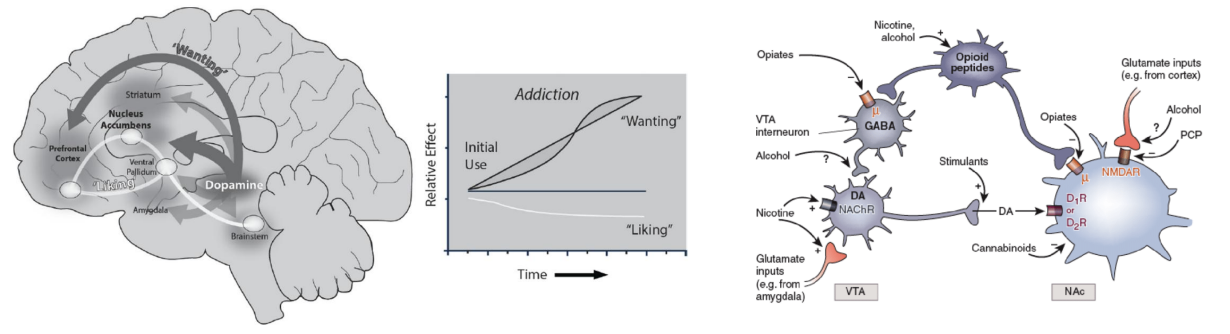
DA in wanting rather than liking
Changes in the reward system and/or cognitive control?
VTA function?
More linked to DA
Tolerance to pleasant effects?
NAc function?
Less linked to DA
Feedback model
Adjustments possible with experience (pleasure deafness theory)
Substance use disorder (formerly addiction) - definition
“complex brain disease in which there is a compulsive engagement in behavior despite knowledge of harmful consequences”
Issues with this approach
“Brain disease” suggests focusing on the brain is productive, even required
“Behavior” can refer to many things (e.g. drug use and gambling, but what else)
“Harmful” is hard to define (e.g. to the user or others)
The term is being phased out as it is seen as vague and stigmatizing
Risk factors
Stability of home environment
Early use + peer groups
Education
Employment
Genetics
Gender
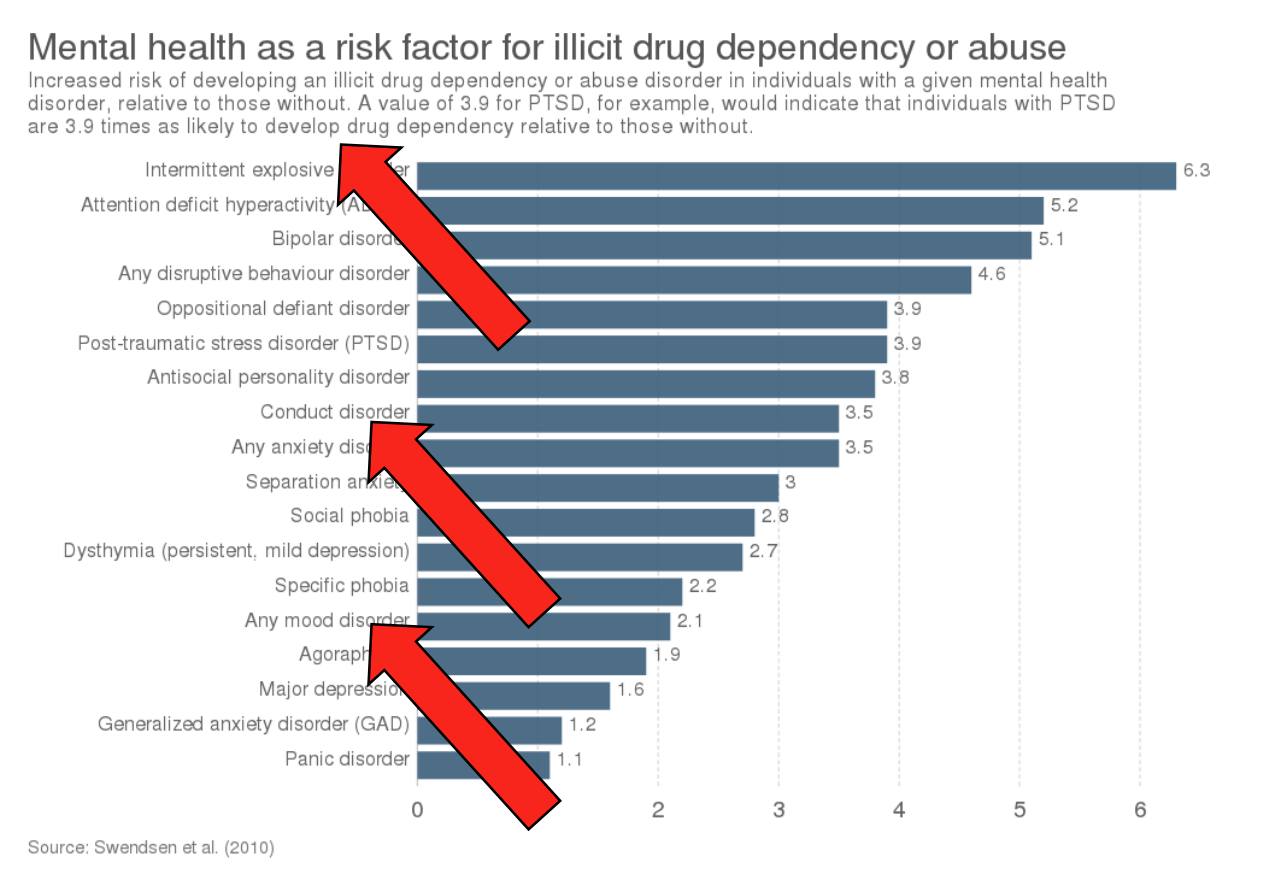
Mental health status
Co-morbidities frequent
Potential neural basis
SUD could be associated with systems for…
…mood, affect and personality (PFC and amygdala)
Mental health comorbidities are common
Drug use sometimes is related to personality
…motivation/reward (PFC and striatum/DA neurons key)
Behaviors may be more “appealing”
The evaluation of benefits and costs may be different
…cognitive control (PFC, in particular the OFC)
Difficulty regulating behavior is part of the disorder
The DA hypothesis
“Reward signal”
DA signal ~ “better than expected” outcome (prediction error models
DA signals might be associated with drugs* and many other rewards
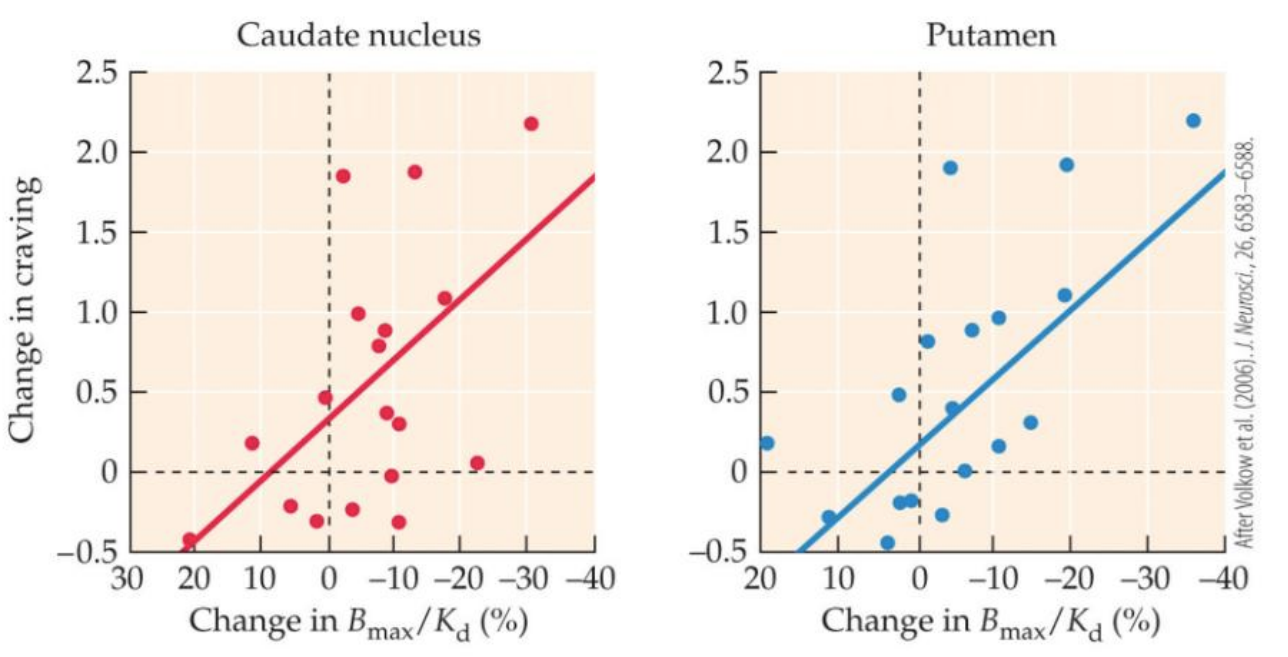
Craving
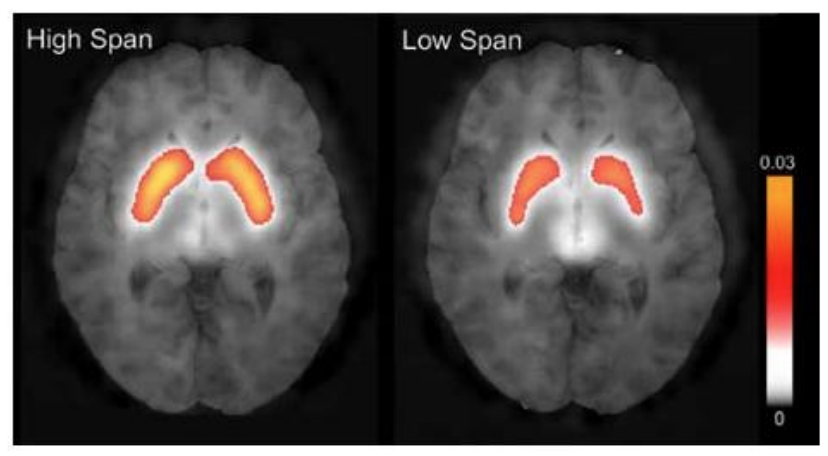
Drug cravings in SUD are linked to DA release in the dorsal striatum
Greater cravings ~ lower DAR availability for the radioligand
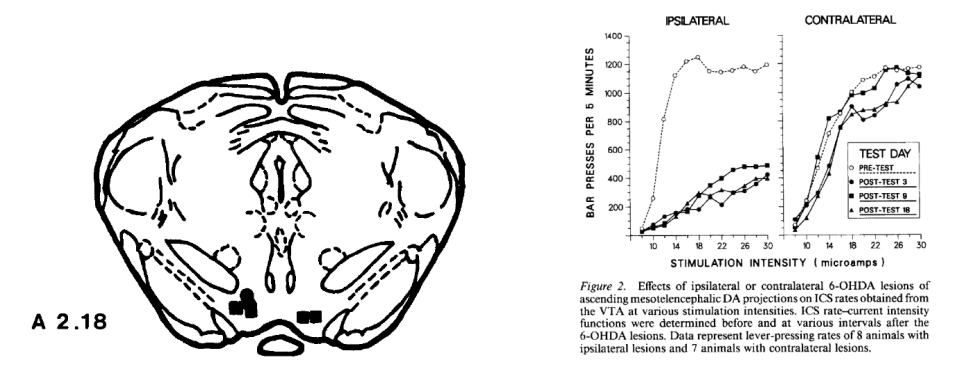
DA neurons in the VTA
Self-stimulation of VTA neurons using implanted electrodes (via bar pressing) is reinforcing
Reinforcing properties of self-stimulation are absent if dopaminergic projections are lesioned
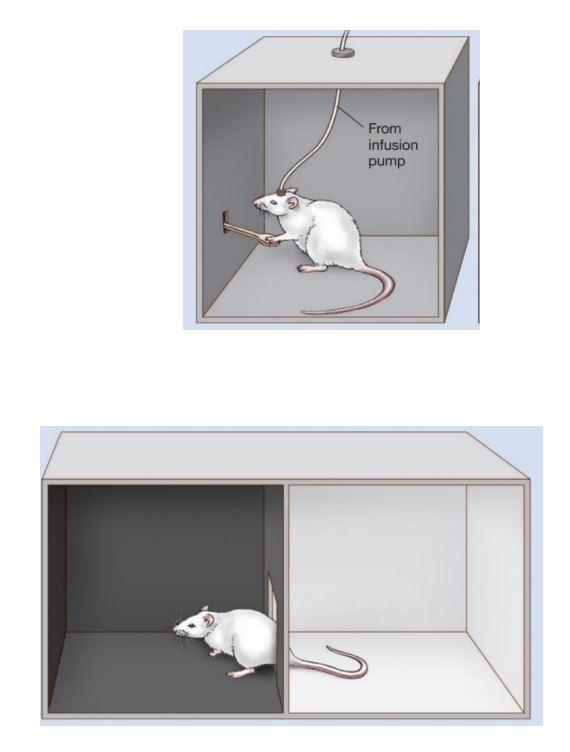
DA antagonists in animal models
Self-administration tests for reinforcing properties (top)
# of bar presses
Conditioned place preference tests assess preference (bottom)
Time spent in drug-paired chamber vs. another chamber
Self-administration and CPP for some drugs in animals can be blocked by dopamine antagonists
DA signaling in addiction
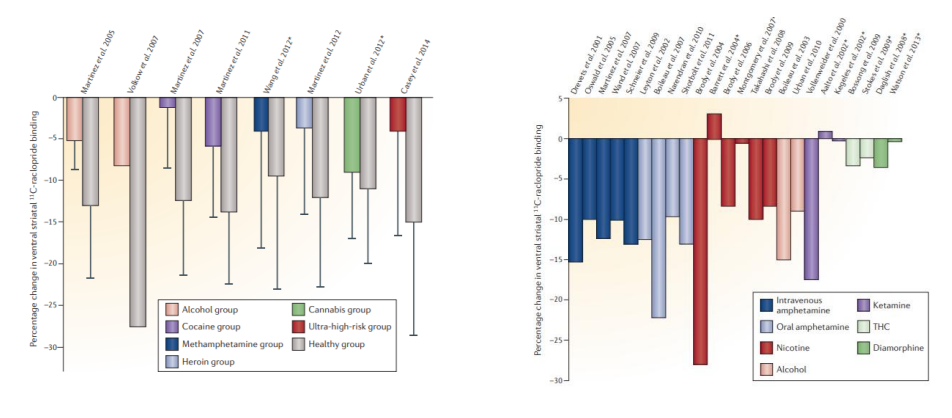
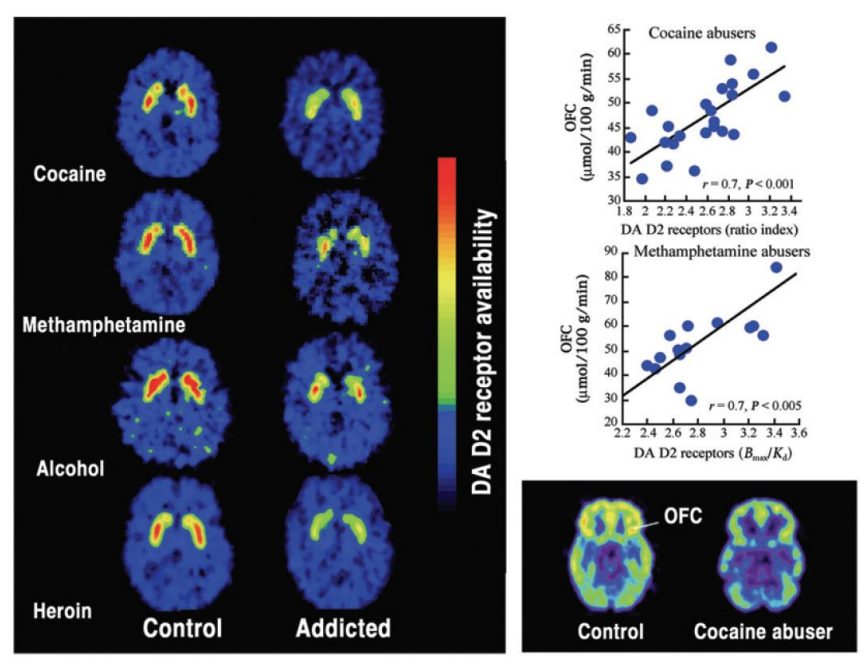
In many* addictions, there is reduced striatal DA release and reduced D2 receptor availability
May suggest pervasive changes in reward value
DA signaling in addiction
DA hypothesis – Evidence
Rewards and cravings are accompanied by DA release
Stimulation of DA neurons is reinforcing
Antagonism of DA receptors can prevent self-administration of substances
Abnormalities in DA transmission occur in SUD
Striatal DA release + D2/3 receptor availability is reduced
DA hypothesis – Problems
Studies in humans are fewer and correlational
DA changes could come before (risk factor) or after (a result
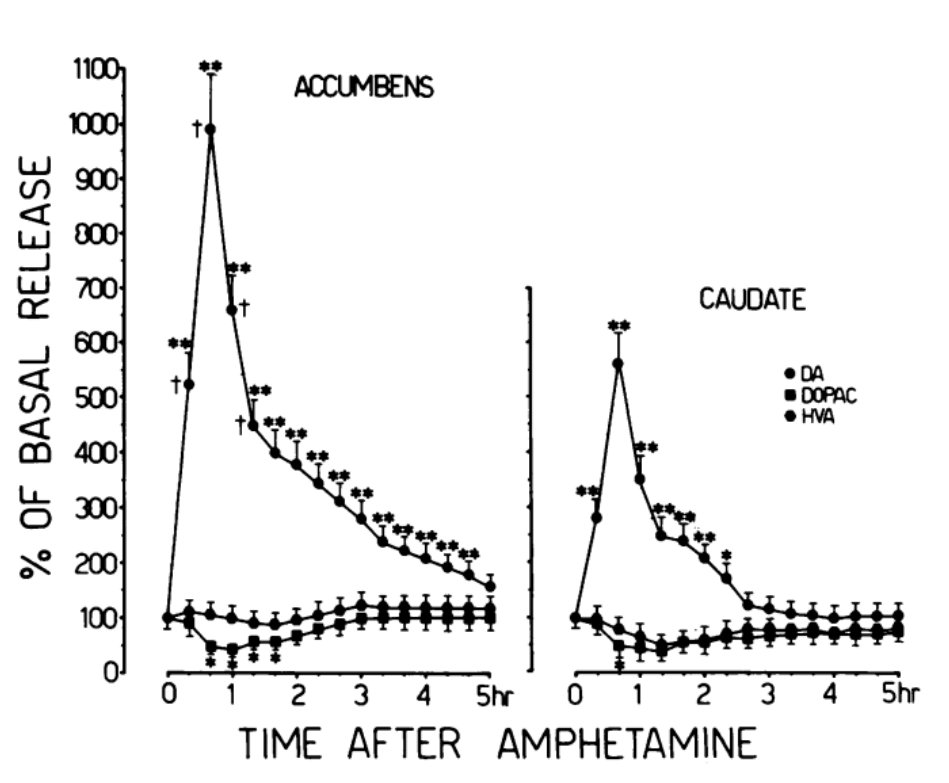
Best evidence comes from dopaminergic drugs (e.g. amphetamines)
Effects small/non-existent for non-DA drugs (nicotine, opioids and cannabis)
DA release linked to a drug doesn’t predict its pleasurable properties
DA firing can be linked to other things, like the probability of reward delivery (e.g. cost, overall motivational state)
Potential neural basis
From earlier slide:
SUD could be associated with systems for…
…mood, affect and personality (PFC and amygdala)
Mental health comorbidities are common
Drug use sometimes is related to personality
…motivation/reward (PFC and striatum/DA neurons key)
Behaviors may be more “appealing”
The evaluation of benefits and costs may be different
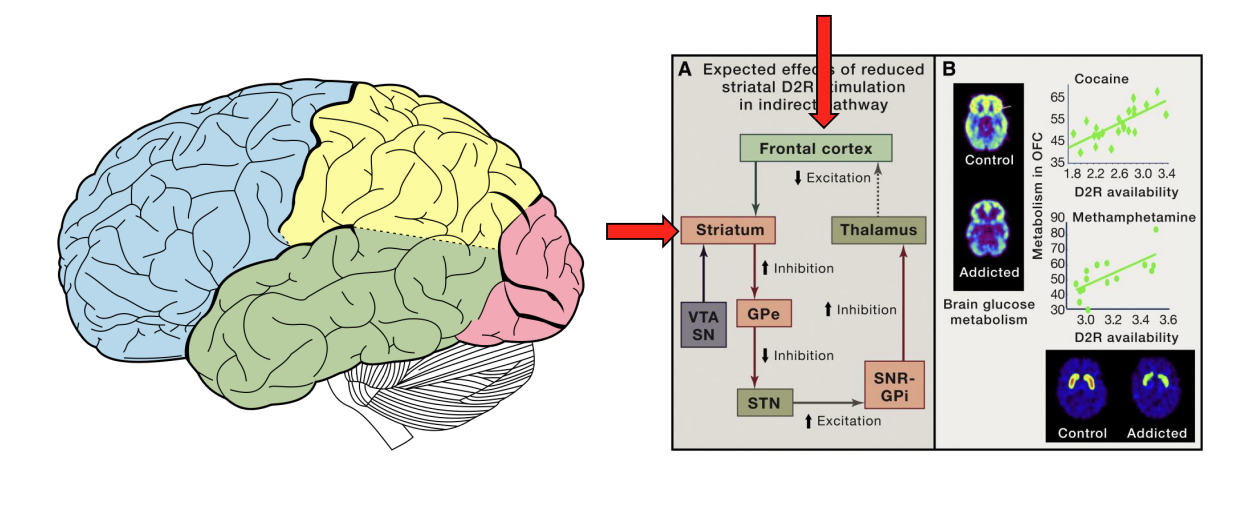
…cognitive control (PFC, in particular the OFC) → highlighted
Difficulty regulating behavior is part of the disorder
Role of the frontal cortex
Reduced activity (particularly in the orbitofrontal cortex) may be associated with reduced ability to assess value and control behavior
Treating SUD
Many barriers (stigma, legal implications); many do not seek treatment
Idea of addiction is a “choice” or “a disease” has implications
Societal level: support for treatment programs, laws and policies
Clinician level: treatments offered and how they are administered
Individual level: well-being and recovery
Prognosis good; majority seeking treatment recover
Treatment takes many forms; including some pharmacological methods
Pharmacological treatments
Drug vaccines (controversial, efficacy uncertain)
Switching to a less active/longer half-life form of drug
Methadone for opioid use disorder, varenicline and nicotine patches for smokers
Counteract “pleasurable” effects of drug
Naltrexone for opioid use disorder and alcoholism (L02)
Mitigate withdrawal effects of the drug
Acamprosate for alcoholism
Symptoms of SZ
Positive symptoms
Hallucinations (seeing/hearing things not there)
Delusions (beliefs not based in fact)
Disorganized speech
Negative symptoms
Lack of emotion (pleasure, motivation)
Impaired social interaction
Cognitive deficits
Impaired attention, memory and executive function
Each symptom cluster may have its own mechanism
Features of SZ
~1% of the population (similar worldwide)
Onset and severity differs by sex (males affected earlier, worse outcomes)
Multiple risk factors (e.g. cannabis, L08)
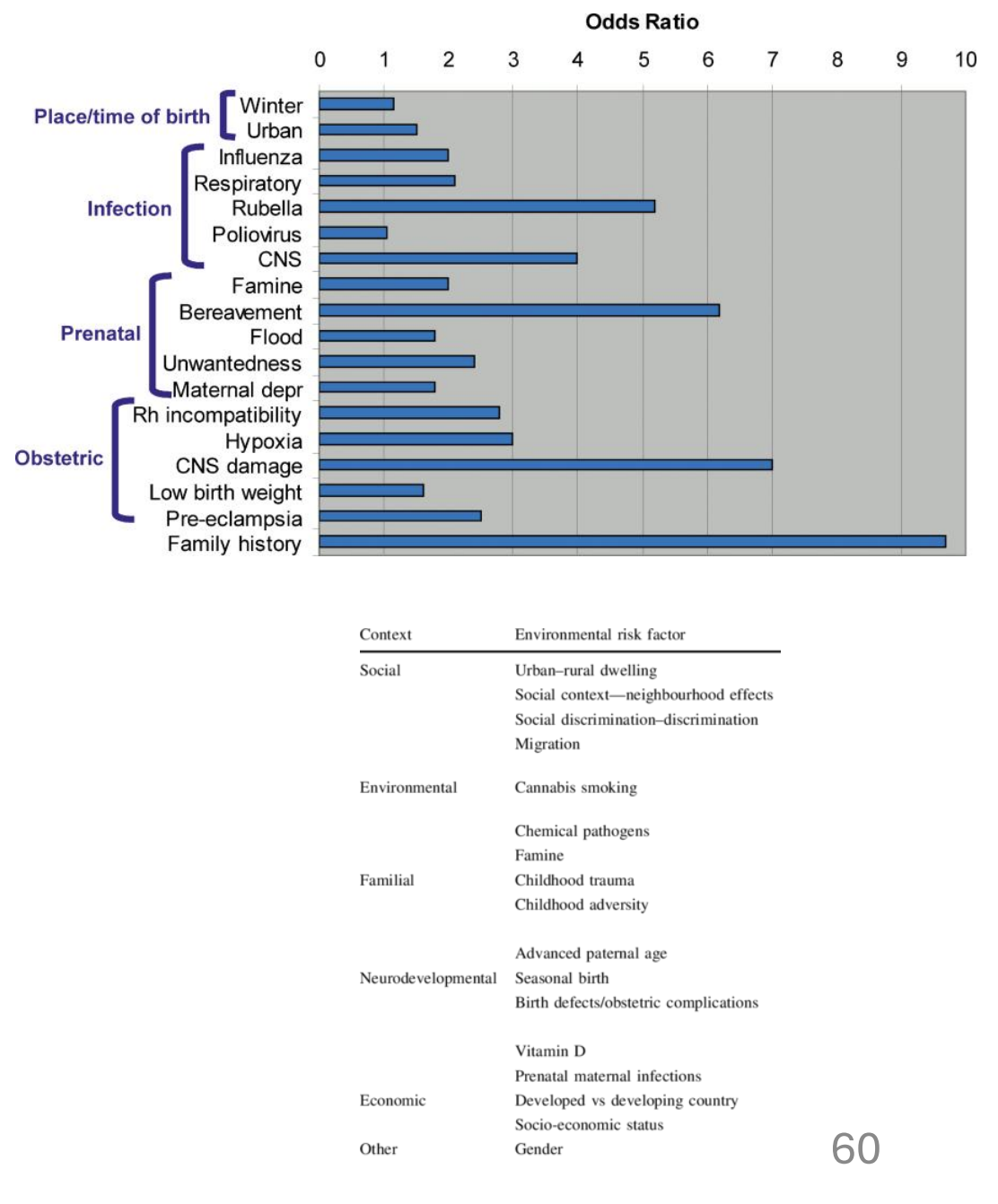
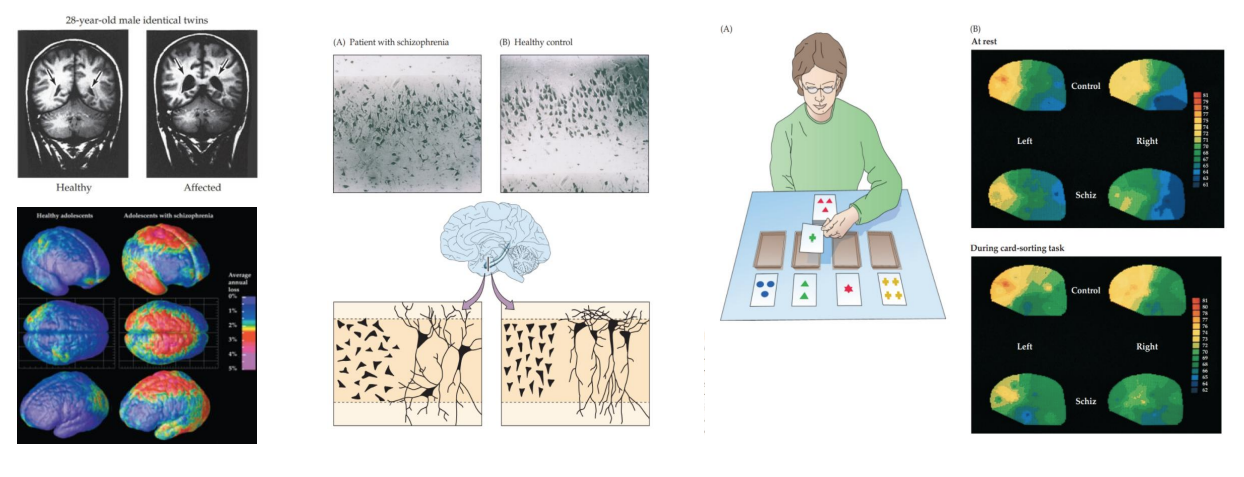
Neural features of SZ
Cortical atrophy (temporal cortex, HPC and PFC)
Abnormal cell organization (HPC)
Hypofrontality
DA hypothesis of SZ
Higher levels of DA metabolites (HVA)
More D2 receptors
Positive symptoms are similar to the effects of drugs that increase DA signaling (e.g. amphetamine, L-DOPA)
Positive symptoms reduced by drugs that block DA signaling (DA antagonists; antipsychotic drugs such as haloperidol)
Dopamine Hypothesis of SZ
Higher DA activity in mesolimbic
Lower DA activity in mesocortical
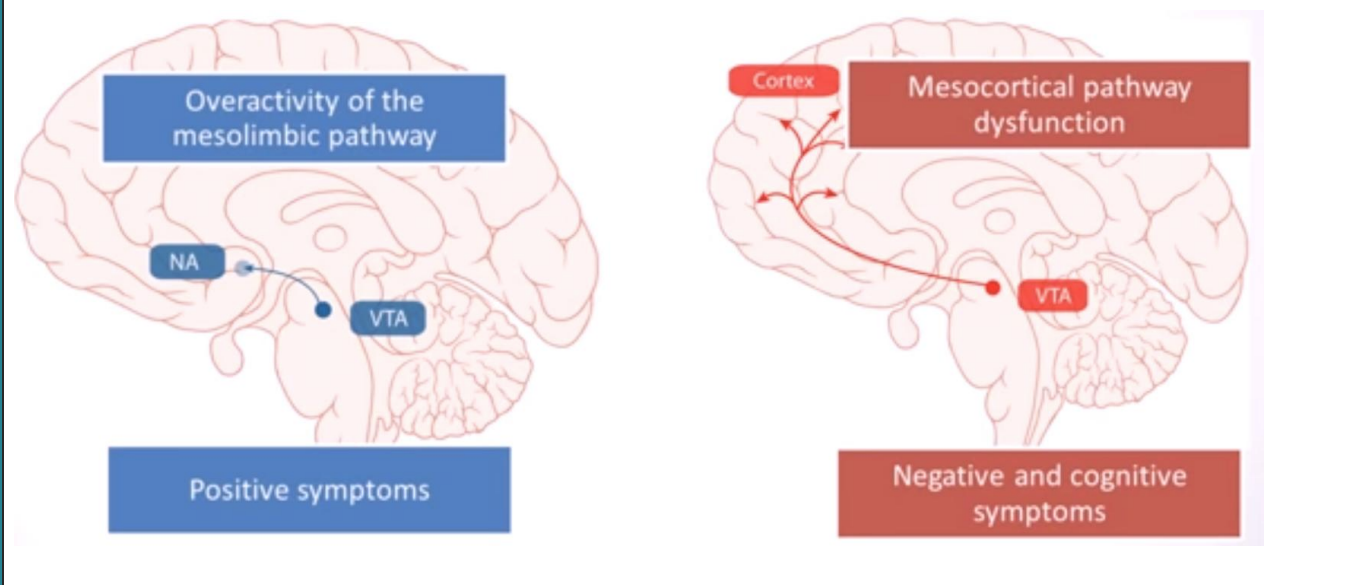
How can we get two different effects on DA pathways?
Things might start in the PFC
PFC differentially regulates both pathways
PFC neurons are less active in SZ (hypofrontality)
Downstream effects:
increased mesolimbic (higher DA)
decreased mesocortical (lower DA)
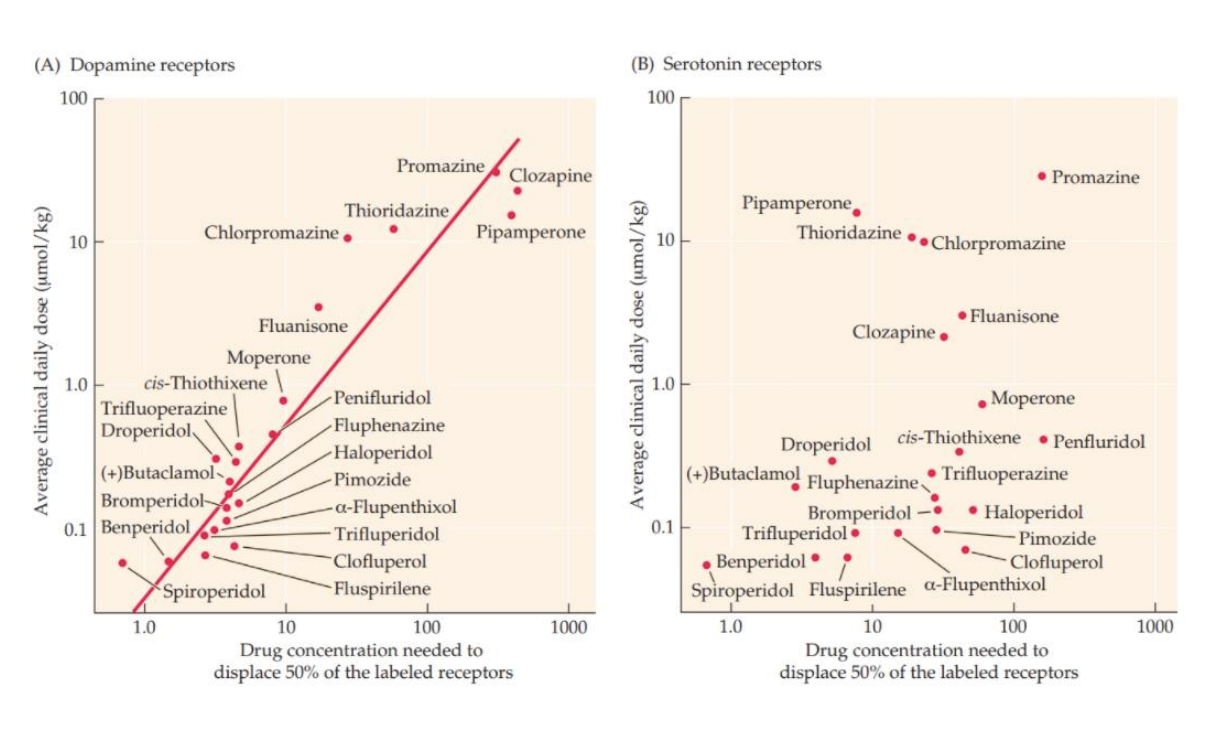
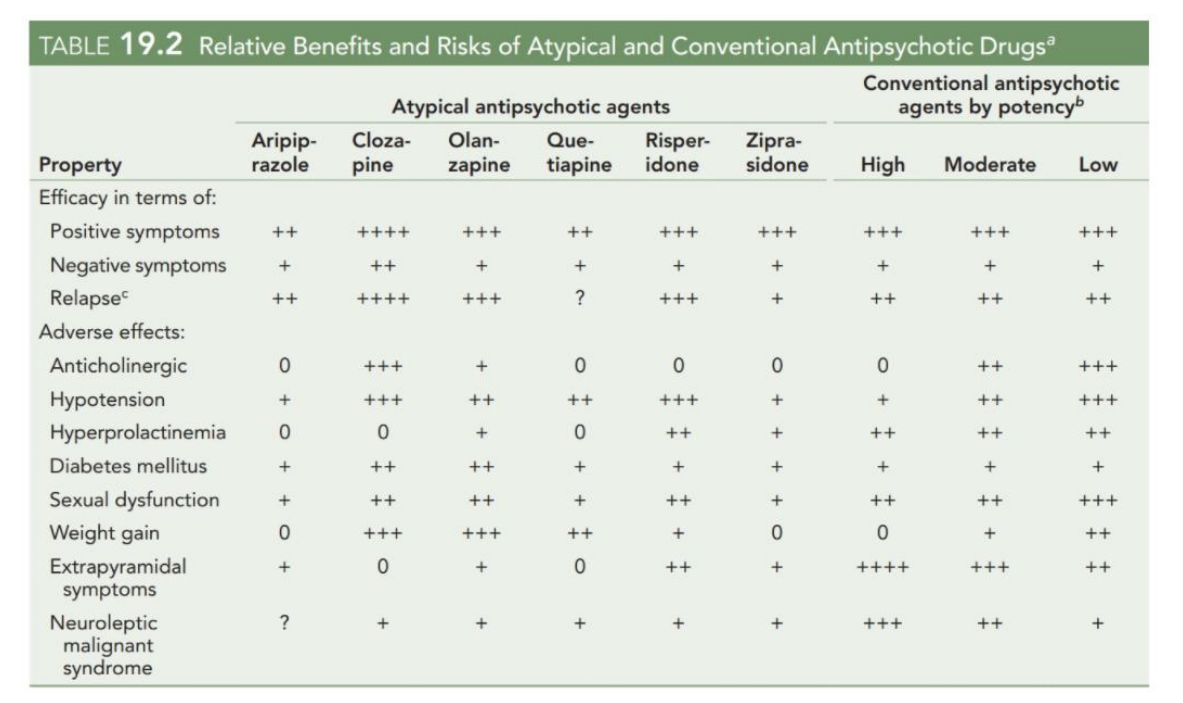
Antipsychotic drugs
Most antipsychotics block D2Rs
Typical antipsychotics are relatively selective for D2
Atypical antipsychotics (e.g. clozapine, risperidone) block other targets (e.g. 5-HT2 receptors)
For conventional antipsychotics, extrapyramidal motor symptoms (esp. tardive dyskinesia) are common
DA, memory and cognition
In monkeys:
DA depletion in the PFC impairs working memory
Effects reversed by DA agonists
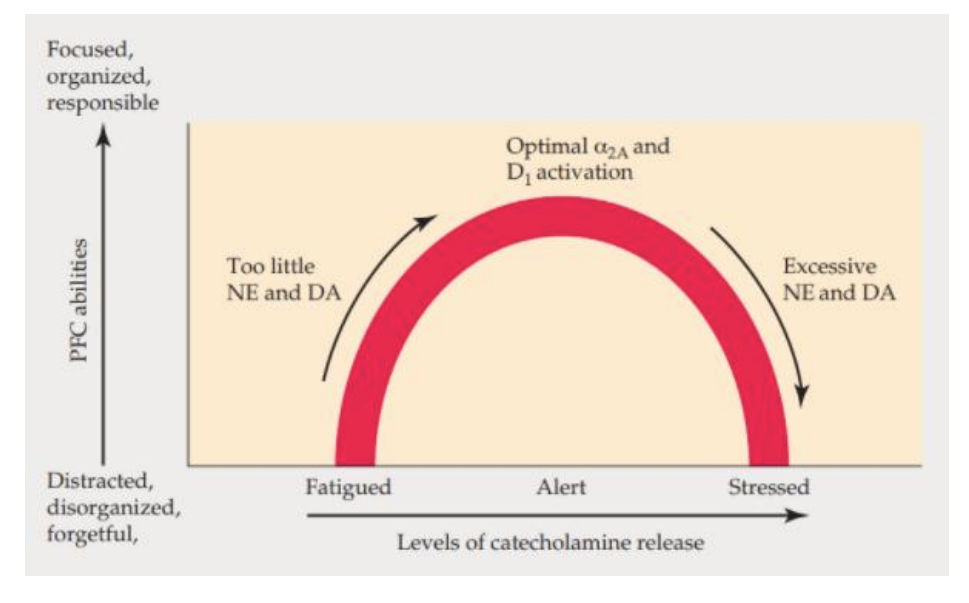
In healthy humans, DA agonists (e.g. bromocriptine):
Improve outcomes for people with poor “undrugged” performance
No benefit in people with strong “undrugged” performance
…we’ve seen this pattern before…
The inverted U relationship
ADHD
In the case of inattention, many examples:
Lack of attention to details or careless mistakes
Does not seem to listen when spoken to directly
In the case of hyperactivity/impulsivity:
Excessive fidgeting
Running, climbing, restlessness in inappropriate situations
Three forms (2 predominant forms + combined form)
Why are ADHD rates rising?
Neural features of ADHD
Reduced PFC volume/maturation (+ other effects)
Brain scans not part of diagnosis
Complex alterations in the DA system
Transport and synthesis
Treated with psychostimulants and non-stimulants
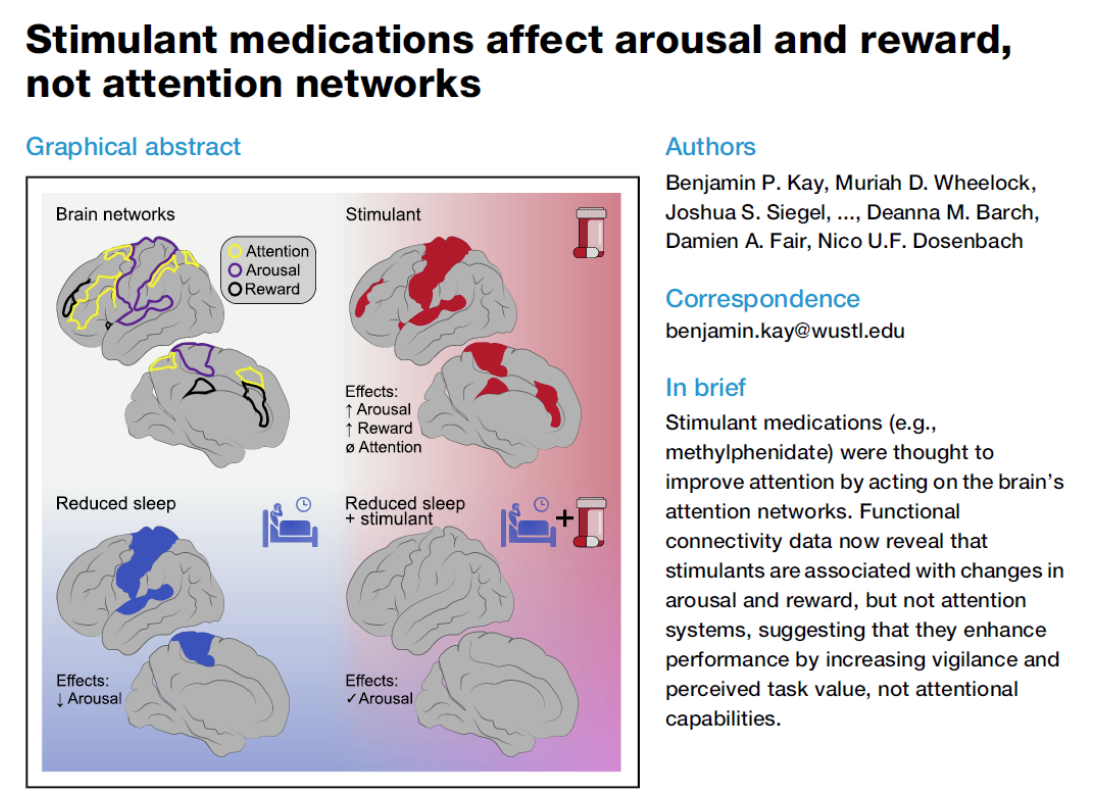
Psychostimulants
Most work by increasing DA or NA transmission
Amphetamine (Adderall) and methylphenidate (Ritalin) both inhibit DAT and NA transporters
Long-term effects could include changes in DAT levels
Why do these drugs work?
Non-stimulant use for ADHD
30% of people may not respond to stimulants
Other people might be at risk for interactions
Non-stimulants for ADHD are also available: atomoxetine (targets noradrenaline re-uptake), guanfacine and clonidine (which target α2 receptors, activated by noradrenaline)
Different side effects for these particular drugs
If they help with ADHD…
4 – 8% of University students report non-medical use for performance
Not limited to “bad students”, diligent students use it too
Cognitive benefits in neurotypical people are modest
Benefits may go beyond cognition (e.g. reducing fatigue)
Increase motivation, but may decrease quality
An important factor may be initial DA levels
Other effects of DA drugs
Altered time perception with dopaminergic drugs (faster with agonists, slower with inhibitors)
May contribute to altered temporal perception in ADHD
Temporal perception is fascinating – more next week (again, L05)