Week 7 L2 - Regulating fertility and HRT
1/70
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
71 Terms
Name seven distinct physiological processes regulated homeostatically by the endocrine system.
1. Growth
2. Metabolism
3. Catabolism
4. Salt retention
5. Bone density
6. Acid secretion
7. Immune system and reproductive system
What are six major clinical pathologies or conditions implicated when homeostatic loss of endocrine regulation occurs?
1. Growth retardation
2. Infertility
3. Hypothyroidism
4. Grave’s disease
5. Diabetes
6. Aberrant salt retention or bone density loss
Which two specific endocrine structures are located entirely within the brain?
hypothalamus
pineal gland
While the pituitary gland is also found in the head, it is situated just beneath the brain in a bony hollow at the base of the skull, rather than entirely within the brain tissue itself
What hormone is released by the hypothalamus to initiate the ovulatory signaling cascade, and what is its specific target tissue?
Gonadotrophin-releasing hormone (GnRH); it acts directly upon the anterior pituitary gland.
Name the two classic gonadotrophins secreted by the anterior pituitary, and state where their target receptors are located.
Follicle-stimulating hormone (FSH) and Luteinising hormone (LH); their receptors are located in the ovary.
Describe the three coordinated stages of ovarian follicle progression mediated by gonadotrophins during the menstrual cycle.
1. Development of the Graafian follicle (which contains the ovum).
2. Release of the ovum from the ovary (ovulation).
3. Further differentiation of the residual follicle into the corpus luteum.
Which two primary steroid hormones are endosynthsised and secreted by the developing follicle and corpus luteum?
Oestrogen and Progesterone.
What homeostatic mechanism do oestrogen and progesterone utilise to control gonadotrophin levels during the majority of the menstrual cycle?
They exert negative feedback loops on both the hypothalamus and the anterior pituitary to prevent premature secretion of gonadotrophins until the appropriate phase of the cycle.
oestrogen feeds back to the anterior pituitary
progesterone feeds back to the anterior pituitary and hypothalamus
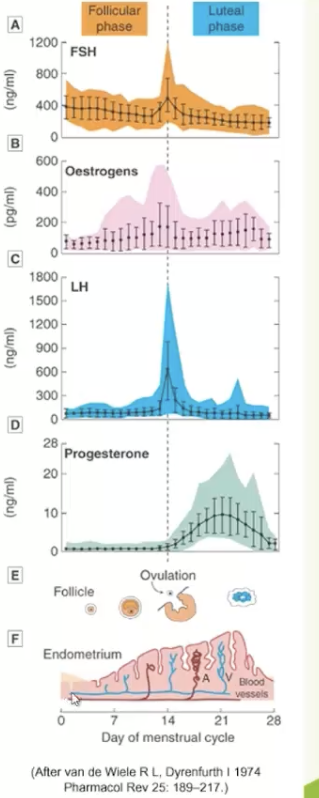
What is the primary role of the high levels of FSH observed relatively early in the menstrual cycle?
To facilitate follicle development and the maturation development of the ovarian follicle.
What endocrine change occurs as the follicle matures, and what is the physiological effect of this change on the uterus?
The follicle develops a secretory capacity to release estrogen, which directly results in endometrial proliferation (thickening of the uterine lining).
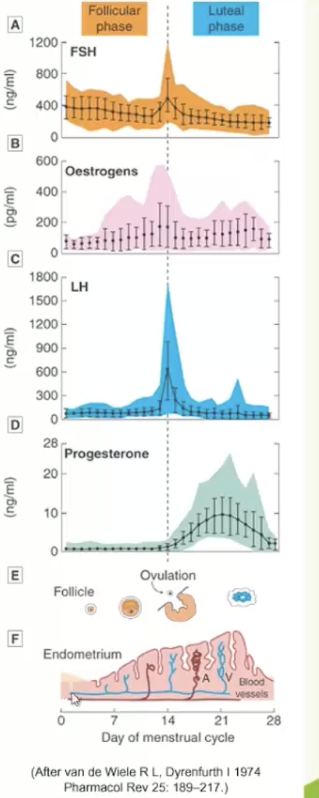
What specific endocrine event is triggered at mid-cycle when estrogen levels meet a high threshold level?
A massive surge in Luteinising Hormone (LH), which causes the follicle to swell rapidly, rupture, and release the ovum into the fallopian tubes (ovulation).
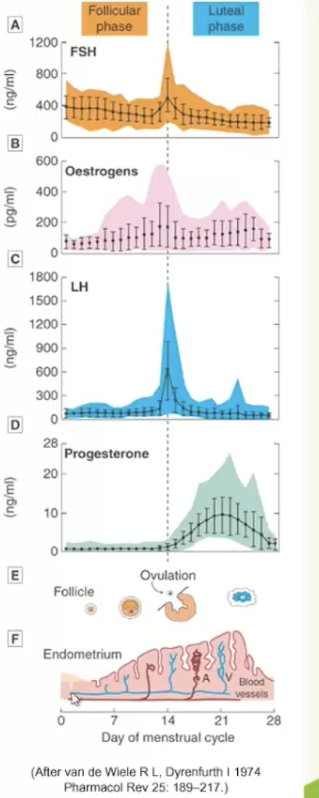
How do the secretory roles of the ruptured follicle differ during the luteal phase, and what phase of the endometrium does this promote?
It transitions into the corpus luteum and shifts to secreting progesterone, which stimulates the secretory phase of the endometrium to render it suitable for embryo implantation.
What homeostatic mechanism occurs to progesterone and the corpus luteum if a fertilized ovum successfully implants into the endometrial lining?
The corpus luteum continues to secrete progesterone, which maintains the endometrial lining and activates negative feedback loops to prevent further ovulation.
What triggers the onset of menstruation if blastocyst implantation does not occur by the end of the luteal cycle?
The corpus luteum stops secreting progesterone, causing the functional endometrial layer to break down and shed during menstruation.
What neuroendocrine mechanism triggers the mid-cycle surge of gonadotrophins (LH and FSH) around day 14 of the menstrual cycle?
Sustained high levels of oestrogen secreted by the mature follicle reach a threshold that switches the hypothalamic-pituitary-gonadal axis from a negative feedback loop to a positive feedback loop, causing a massive release of GnRH and increasing pituitary sensitivity.
Why is the mid-cycle FSH surge significantly smaller and more moderate in amplitude compared to the explosive LH surge?
The developing granulosa cells simultaneously secrete inhibin, a peptide hormone that selectively targets the anterior pituitary to suppress FSH synthesis and secretion, acting as a partial brake on the FSH surge while leaving the LH surge uninhibited.
What are the two primary biological functions of the moderate FSH surge that occurs concurrently with ovulation?
1. It upregulates LH receptor expression on the granulosa cells of the mature Graafian follicle so it can respond to the LH surge.
2. It promotes the expansion and loosening of the cumulus oophorus matrix surrounding the oocyte to facilitate its physical release.
What are the typical hormonal components and dosage ranges found in standard combination contraceptive pill preparations?
A synthetic oestrogen derivative (usually ethinylestradiol, 20-50 mg) plus a synthetic progestogen derivative (several types, ranging from 0.1-1 mg).
Why are the hormone levels in some combination contraceptive pills varied throughout a 28-day cycle?
To mimic the cyclical progesterone and estrogen levels required to permit the necessary physiological effects of these hormones on reproductive and peripheral tissues.
What is the primary neuroendocrine mechanism of action by which contraceptive pill doses prevent ovulation?
They activate negative feedback loops that suppress the secretion of the gonadotrophins FSH and LH from the anterior pituitary, thereby preventing follicular maturation and ovulation.
What physiological event is triggered by the withdrawal of progesterone after 21 days of combination pill administration?
It stimulates menstruation (withdrawal bleeding).
How does the mechanism of the "mini-pill" differ from standard combination therapies, and why is it prescribed?
It relies solely on progesterone rather than a combination of hormones; it is often prescribed because some patients tolerate it better than oestrogen-containing preparations.
What defines a monophasic oral contraceptive pill regimen in terms of daily hormone concentrations?
A regimen where every active tablet in the pack contains the exact same fixed dose and concentration of oestrogen and progestogen throughout the 21-day active cycle.
How do multiphasic (biphasic, triphasic, or quadriphasic) contraceptive pills differ from monophasic preparations?
The 21 days of active pills are divided into distinct phases where the ratio and concentration of estrogen and progestogen alter to more closely mirror a natural menstrual cycle.
What is the administrative and concentration pattern of a progesterone-only "mini-pill" pack?
Every single pill contains the exact same low dose of progestogen (constant concentration), and the tablets are taken continuously without a pill-free or placebo break.
What dictates whether a SERM acts as an estrogen receptor agonist or antagonist?
Tissue location (tissue-specific expression of co-activators or co-repressors).
What is the primary goal of most pro-fertility drugs
to promote ovulation before using methods such as IVF
What dictates whether a SERM acts as an estrogen receptor agonist or antagonist?
Tissue location (tissue-specific expression of co-activators or co-repressors).
Why does Clomiphene trigger an increase in FSH and LH secretion?
It blocks ERs in the hypothalamus and anterior pituitary, preventing estrogen's normal negative feedback mechanism.
What is the primary clinical indication for Clomiphene?
Female infertility due to anovulation (e.g., prior to IVF).
How do the primary clinical indications for Clomiphene and Tamoxifen differ today?
Both originally for stimulating ovulation. Now:
Clomiphene: Ovulation induction (pro-fertility).
Tamoxifen: ER-positive breast cancer treatment (acts as an antagonist in breast tissue).
What type of drugs are selective oestrogen receptors, what can they be used for?
SERMS
can be used to stimulate ovulation
Which phase of the HPG axis feedback loop do pro-fertility SERMs target to "trick" the CNS?
The inhibitory (negative) feedback loop of endogenous estrogen on the hypothalamus and anterior pituitary.
What type of receptor mediates estrogen's diverse systemic actions outside of reproductive tissues?
Nuclear estrogen receptors (ER), which are located across diverse tissue types and alter gene transcription.
What is estrogen's role in skeletal physiology?
Promotes calcium deposition to bone (maintains bone mineral density and inhibits bone resorption).
How does estrogen affect lipid profiles and cardiovascular health?
Regulates HDL/LDL balance (promotes cardioprotection by maintaining higher HDL and lower LDL levels).
What haematological effect does estrogen exert that is clinically relevant to clotting risk?
It modulates blood coagulation pathways (influencing the synthesis of clotting factors).
What are the gastrointestinal and fluid-balance effects of systemic estrogen?
Bowel motility: Regulates GI transit time.
Salt/water balance: Influences renal fluid retention and electrolyte handling.
What causes the "vasomotor effects" (e.g., hot flushes) seen in estrogen deficiency or SERM therapy?
Disruption of estrogen's normal action on the thermoregulatory center in the hypothalamus.
List the 7 non-reproductive systems/effects regulated by nuclear estrogen receptors (ER).
1. Calcium deposition to bone
2. HDL/LDL balance
3. Blood coagulation
4. Bowel motility
5. Salt/water balance
6. Vasomotor effects
7. A range of metabolic effects
What is the primary physiological aim of Hormone Replacement Therapy (HRT) in post-menopausal women?
To overcome decreased ovarian function and the consequent clinical reduction in endogenous estrogen (and sometimes progesterone) levels.
Why does post-menopausal estrogen decline lead to hot flushes, and how does HRT correct this?
Estrogen decline disrupts the hypothalamic thermoregulatory center (wide-ranging vasomotor symptoms); HRT stabilizes this system to minimize/prevent vasomotor flushing.
What is the mechanism behind post-menopausal vaginal dryness, and how does HRT alleviate it?
It is caused by a loss of ER-mediated vaginal secretions due to low estrogen; HRT restores receptor activation to maintain tissue lubrication and health.
How does post-menopausal estrogen deficiency lead to osteoporosis, and what is the role of HRT?
Low estrogen diminishes ER-mediated calcium deposition to bone (accelerating bone resorption); HRT preserves bone mineral density by restoring this regulatory mechanism.
List 3 common post-menopausal symptoms improved by HRT and the underlying ER-mediated mechanism for each.
1. Hot flushes: Loss of hypothalamic vasomotor regulation.
2. Vaginal dryness: Loss of ER-mediated vaginal secretions.
3. Osteoporosis: Loss of ER-mediated calcium deposition in bone tissue
What is the Million Women Study (2003) in terms of its study design?
A landmark, large-scale longitudinal cohort study tracking a massive dataset of women's health outcomes over time with high statistical power.
Beyond oncology, what other clinical factor categories were investigated by the Million Women Study?
Cardiovascular risk
Mental health
Dietary intervention
General health-related matters
What was the major, widely publicized finding of the 2003 Million Women Study regarding HRT?
It indicated that post-menopausal women taking HRT faced an elevated risk of certain cancers, specifically those linked to female reproductive hormone function (e.g., breast cancer).
What is meant by a "hormone-sensitive" breast cancer in the context of HRT risk?
Tumors that are ER-positive (Estrogen Receptor positive), meaning their growth can be actively driven by estrogen signaling.
What is the biological mechanism by which HRT could potentially accelerate hormone-sensitive breast cancer?
Enhanced stimulation of ER (Estrogen Receptors) by exogenous HRT estrogen can feasibly drive excess cellular proliferation and tumor development in a neoplastic environment.
Aside from hormone-sensitive cancers, what other major systemic vascular concern was raised regarding HRT use?
An elevated risk of stroke.
What group was established as the baseline control (Relative Risk = 1.00) in the Million Women Study dataset?
"Never users" of Hormone Replacement Therapy (HRT).
What did the study find regarding the relative risk of breast cancer in current HRT users compared to baseline?
Current users had a significantly elevated Relative Risk (RR) of 1.66 (with a 95% Confidence Interval of 1.60–1.72).
What happens to breast cancer risk after a patient ceases HRT use for 5 or more years?
The relative risk returns to baseline levels (RR approx 1.00), showing no statistically significant increased risk compared to "never users.
What major clinical real-world impact resulted from the publication of this persuasive HRT data?
Clinical care of the menopause was greatly affected, as both clinicians and patients lost confidence in the safety profile of HRT, leading to a sharp decline in prescriptions.
What is the specific epidemiological study design of the Million Women Study, and what is it not?
It is a prospective cohort study. It is not a randomly-assigned clinical trial (Randomized Controlled Trial/RCT) or a case-control study.
Why does the lack of random assignment make the Million Women Study data controversial?
Because it is observational, meaning it cannot fully control for confounding variables or establish direct causality the way an RCT can.
What is the "prior exposure" flaw or selection bias critique of the Million Women Study?
The study takes no account of prior hormone exposure. Women who chose to start HRT might, due to their underlying post-menopausal symptoms and baseline physiology, already have been at a inherently greater risk for developing breast cancer.
When the Million Women Study data was combined with other trials in subsequent meta-analyses, what did the results show?
The pooled data showed a much smaller risk of breast cancer than what was originally reported in the isolated 2003 study findings.
State the three primary methodological critiques that keep the Million Women Study controversial.
1. It is an observational prospective cohort study, not a randomized controlled trial (RCT).
2. It fails to account for prior hormone exposure/baseline physiology (selection bias).
3. Subsequent meta-analyses consistently demonstrated a much smaller relative risk.
Front: What is the generational consequence of the Million Women Study on medical education and clinical training?
A whole generation of clinicians has not been properly trained in HRT prescribing due to the massive drop in clinical confidence following the 2003 data.
Why is the institutional memory regarding HRT's efficacy currently at risk of being lost?
As older clinicians retire, the clinical expertise and first-hand institutional knowledge that HRT is highly effective at controlling severe menopausal symptoms is fading.
What is the current status of clinical guidelines for menopause management and HRT prescribing?
Guidance remains in flux because different bodies and experts interpret the original study data, confounding variables, and subsequent meta-analyses differently.
What commercial and political force actively influences the ongoing debate and guidance surrounding HRT?
Powerful lobbying by pharmaceutical HRT manufacturers seeking to restore market confidence and highlight safer, modern delivery methods (e.g., transdermal gels).
List the 4 distinct long-term institutional and social impacts resulting from the legacy of the HRT risk studies.
1. A generation of clinicians untrained in HRT prescribing.
2. Loss of institutional memory regarding HRT's clinical efficacy as older doctors retire.
3. Clinical guidance remains in flux due to varying data interpretations.
4. Continuous powerful lobbying by HRT manufacturers.
Why do current media guidelines emphasize reporting absolute risk over relative risk when discussing medical interventions?
Because headlines shouting a "double" or "triple" risk can be highly misleading to patients, as they sensationalise the change without acknowledging the incredibly low baseline (existing) risk already present
When assessing the risk of taking HRT, what demographic-specific question must a clinician ask to frame the statistical risk accurately?
What is the actual absolute risk of taking HRT compared with the existing baseline risk of being a woman aged 55?
Why is contextualising HRT data against other everyday risks crucial during patient consultations?
It allows patients to evaluate the relative threat accurately; for example, the increase in cancer risk from HRT is often small compared to many common lifestyle risk factors (such as chronic alcohol consumption, obesity, or smoking).
What is the clinical benefit of communicating risk using absolute data and comparative lifestyle scales?
It permits better-informed decisions that effectively balance the clinical severity of menopausal symptoms against potentially elevated, but contextually minor, cancer risks.
List the 4 key principles of balanced medical risk communication highlighted in the lecture.
1. Emphasize absolute risk over relative risk.
2. Contextualize data against the existing baseline risk of the specific age group (e.g., age 55).
3. Compare the intervention's risk directly with other lifestyle risks.
4. Balance the severity of current symptoms against the statistical probability of elevated risks.
What distinction did Prof. David Spiegelhalter highlight regarding the evidence vs. the absolute risk of processed meat causing cancer?
The strength of evidence that processed meat causes cancer is as strong as the evidence for tobacco, but the actual absolute risk from tobacco is vastly higher.