OB Step Up
1/65
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
66 Terms
Embroyonic and fetal development begins with
fertilizatoin and takes 38 weeks until maturity occurs
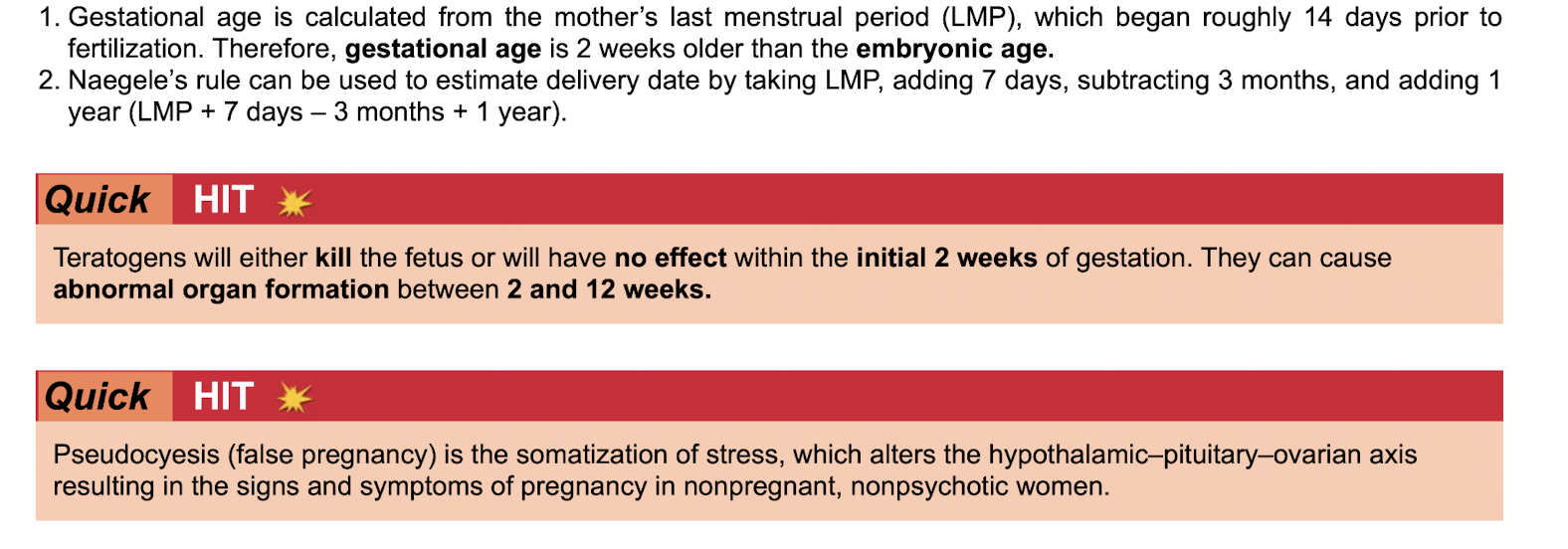
Gestational age vs embryonic age
Naegele’s rule
Teratogens will either
Gestational age is calculated from mothers LMP (usually 2 weeks prior to fertilization)
Gestational age is usually 2 weeks older than the embryonic age
Naegele’s rule can estimate delivery date
(LMP+7 days- 3months + 1 year)
Teratogens will either kill the fetus or have no effect within the initial 2 weeks of gestation.
They cause abnormal organ formation between 2-12 weeks
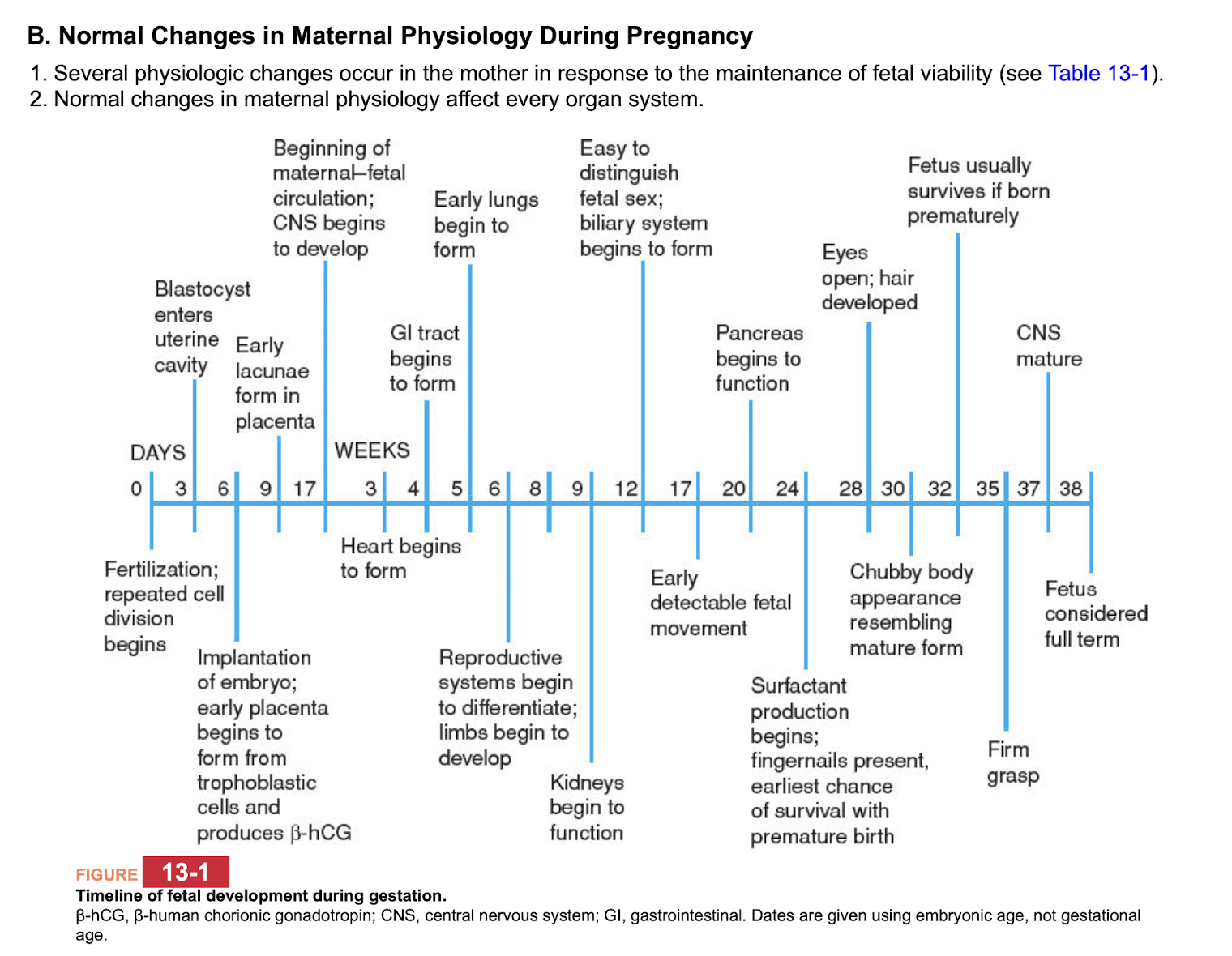
Timeline of fetal development during gestation
3 days after fertilization: blastocysts enters uterine cavity
6 days: implantation and form trophoblastic cells and produce beta HCG
3 weeks: heart begins to form
5 weeks: early lungs form
9 weeks: kidneys begin to function
12 weeks: can tell sex; biliary system begins to form
17 weeks: fetal movement can be detected
20 weeks: pancreas begins to function
24 weeks: surfactant production, fingernails present, earliest chance of survival for premature birth
38 weeks: full term
low risk activity during pregnancy
Moderate intensity exercise is encouraged
Sexual intercourse can be continued unless mother is high risk for
spontaneous abortion,
premature labor or
placenta previa

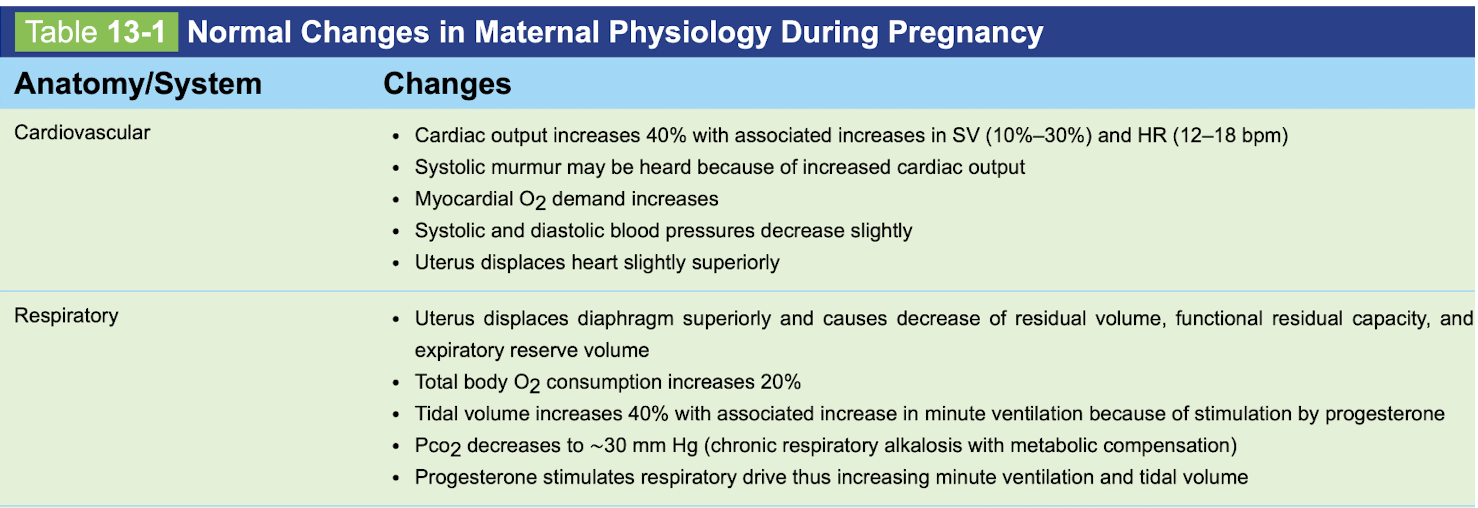
Changes in pregnancy
CV
Respiratory
CV:
-CO increased
-SV increases
-Systolic murmur increases if present
-O2 demand on heart increases
-BP increases
-Uterus can displace heart slightly superiorly
Respiratory:
-Diaphragm displaces superiorly
-RV decreased
-FRC decreased
-Expiratory residual volume decreased
-Total body O2 consumption increases
-Tidal volume increases
-minute ventilation increases
-PCO2 decreases (chronic respiratory alkalosis with metabolic compensation)
-progesterone stimulates respiratory drive
Changes in pregnancy
Renal
endocrine
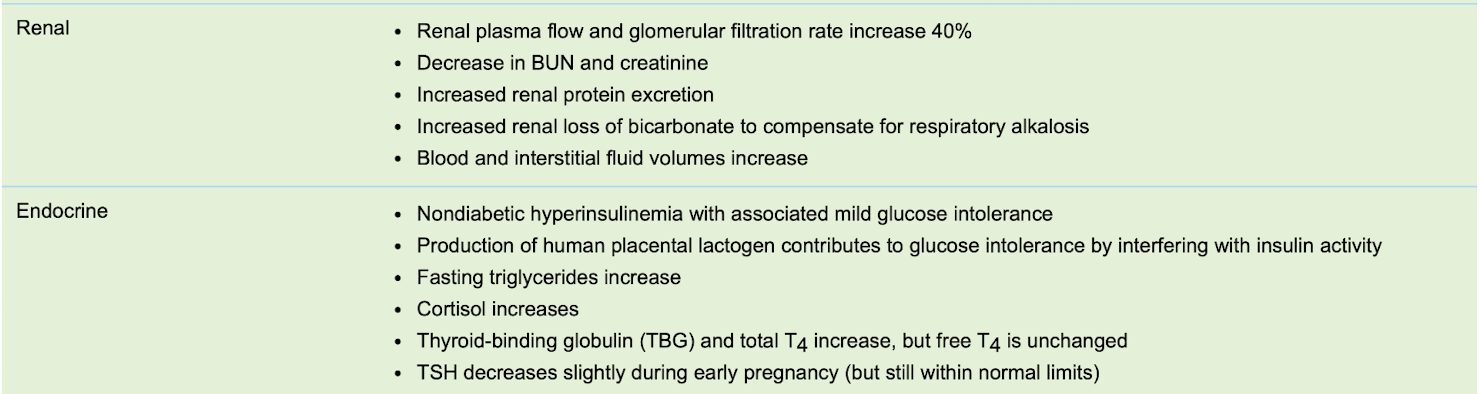
Renal
-plasma flow and GFR increase
-decrease in BUN, cr
-increased renal protein excretion
-increase renal loss of bicarbonate (compensation for respiratory alkalosis)
-blood and interstitial fluid volume increases
Endocrine:
-nonDM hyperinsulinemia
-mild glucose intolerance
-human placental lactogen contributes to glucose intolerance
-fasting TG increases
-cortisol increases
-TBG and total T4 increases
-Free T4 unchanged
-TSH decreases slightly during early pregnancy but wnl still
Changes in pregnancy
heme
GI
Heme:
-hypercoaguable
-increased RBC production
-decreased Hct
-increased blood volume
GI:
-increased salivation
-decreased gastric motility

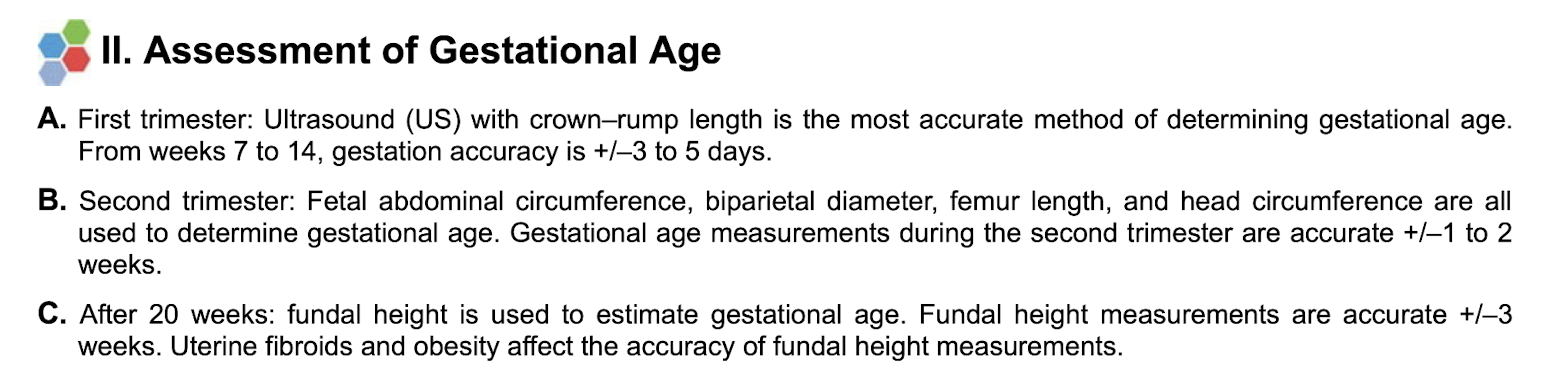
Assessment of Gestational age
-first trimester
-second trimerster
-after 20 weeks
First trimester
-US with crown-rump length is most accurate
Second trimester:
-fetal abdominal circumference
-biparietal diameter
-femur length
-head circumference
Afer 20 weeks:
-fundus height
-note: uterine fibroids and obesity can affect the accuracy of using fundal height measurements
Prenatal care
-nutrition
-weight gain
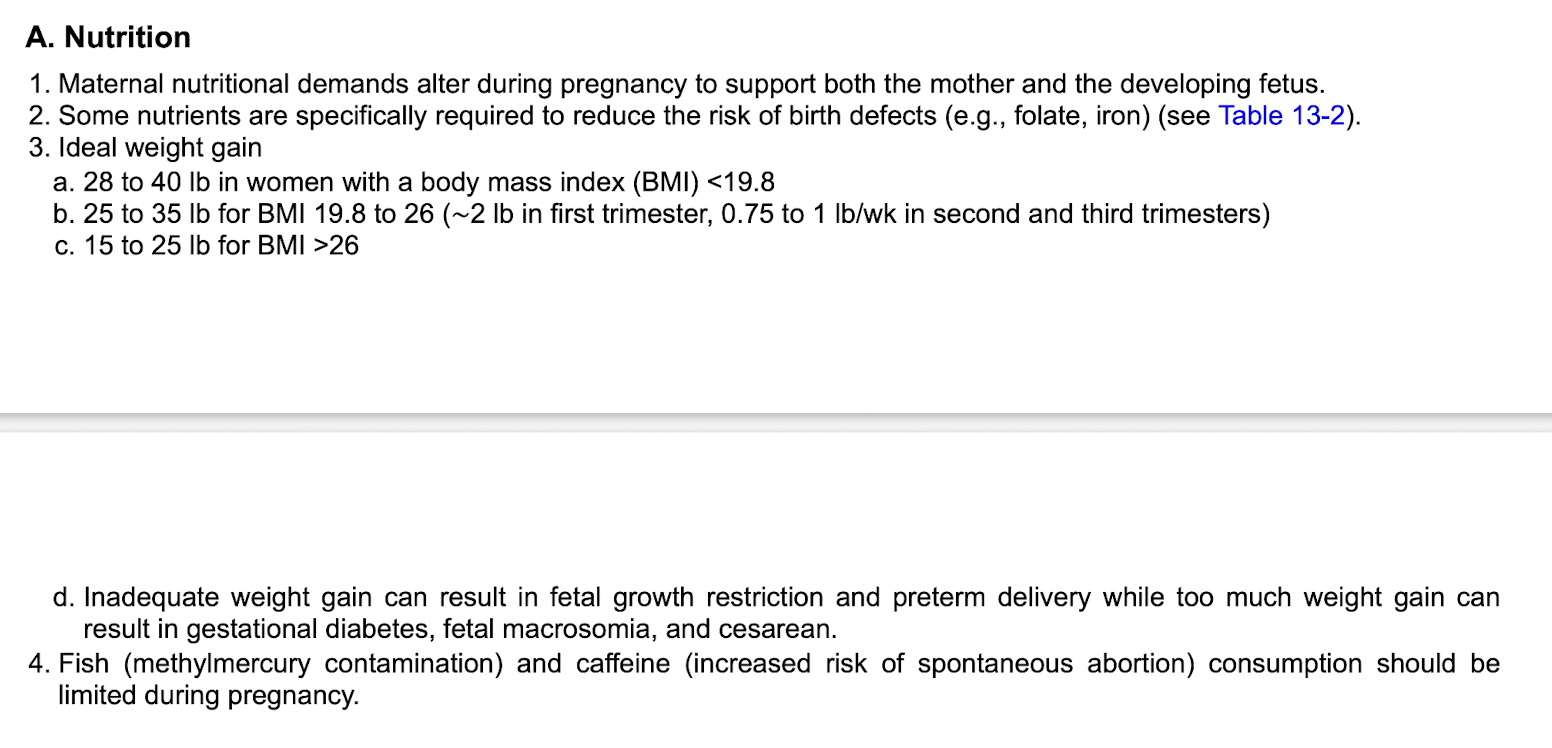
Nutrition
-folate and iron
-avoid fish and caffeine
Weight gain
-Ideal weight gain based on BMI
<19.8 BMI: 28-40 lbs weight gain
19.8-26 BMI: 25-35 lbs
>26 BMI: 15-25 lbs
-inadequate weight gain can result in fetal growth restriction and preterm delivery
-too much weight gain can result in GDM, fetal macrosomia and C-section
Daily caloric intake pregnancy
2500 kcal
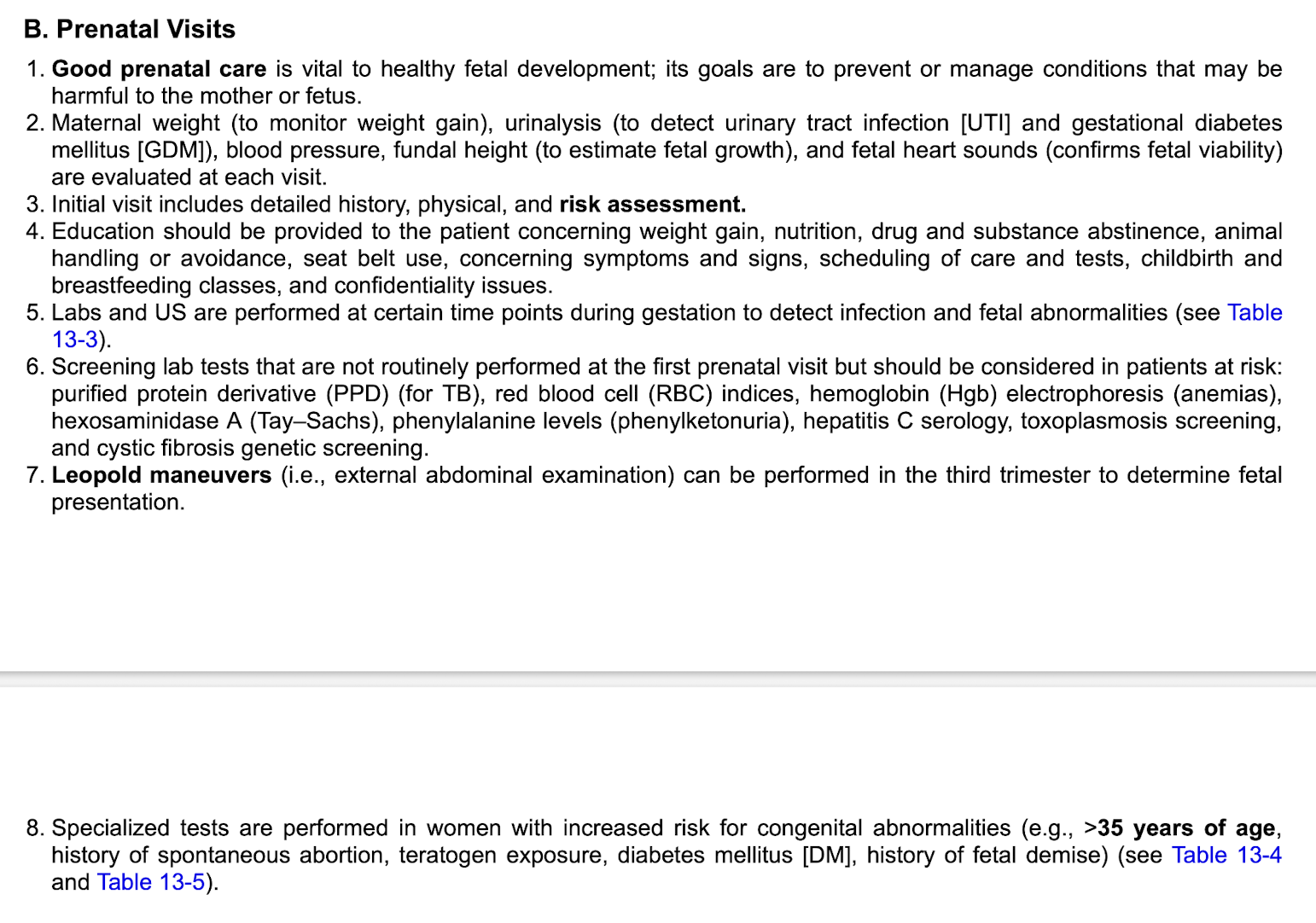
Prenatal visits
-Leopold maneuvers
Leopold maneuvers performed in third trimester to determine fetal presentation
Maternal serium alpha protein level test
-Test is only valid if performed during correct gestational window (16-18 weeks gestation)
-High levels are associated with risk of NTDs, abdominal wall defects, and multiple gestations
-Low levels are associated with inc risk of trisomies 21 and 18

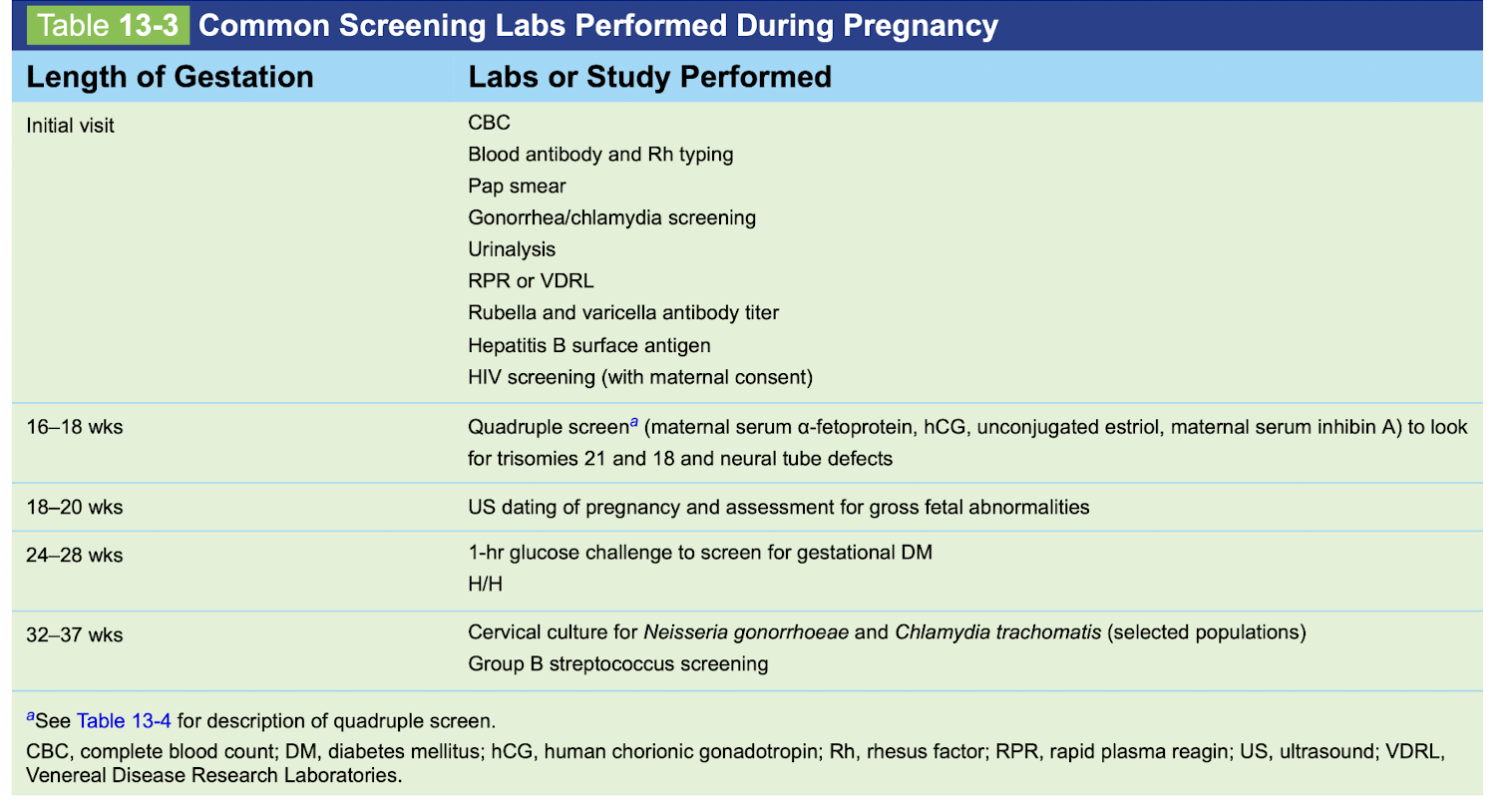
Screening labs vs length of gestatio n
-initial visit
-16-18 weeks
-18-20 weeks
-24-28 weeks
-32-37 weeks
Initial visit:
-CBC
-Rh typing
-Pap smear
-STI screening
-UA
-RPR or VDRL
-Rubella and varicella AB titer
-HBsAG
-HIV screening (with maternal consent)
16-18 weeks:
-Quad screen (maternal AFP, hCG, Estriol, inhibin A)
18-20 weeks:
-US dating
-assessment for gross fetal abnormalities
24-28 weeks:
-1-hr glucose challenge for GDM
32-37 weeks:
-cervical culture for N. Gonnorhea and chlaymdia
-GBS screen
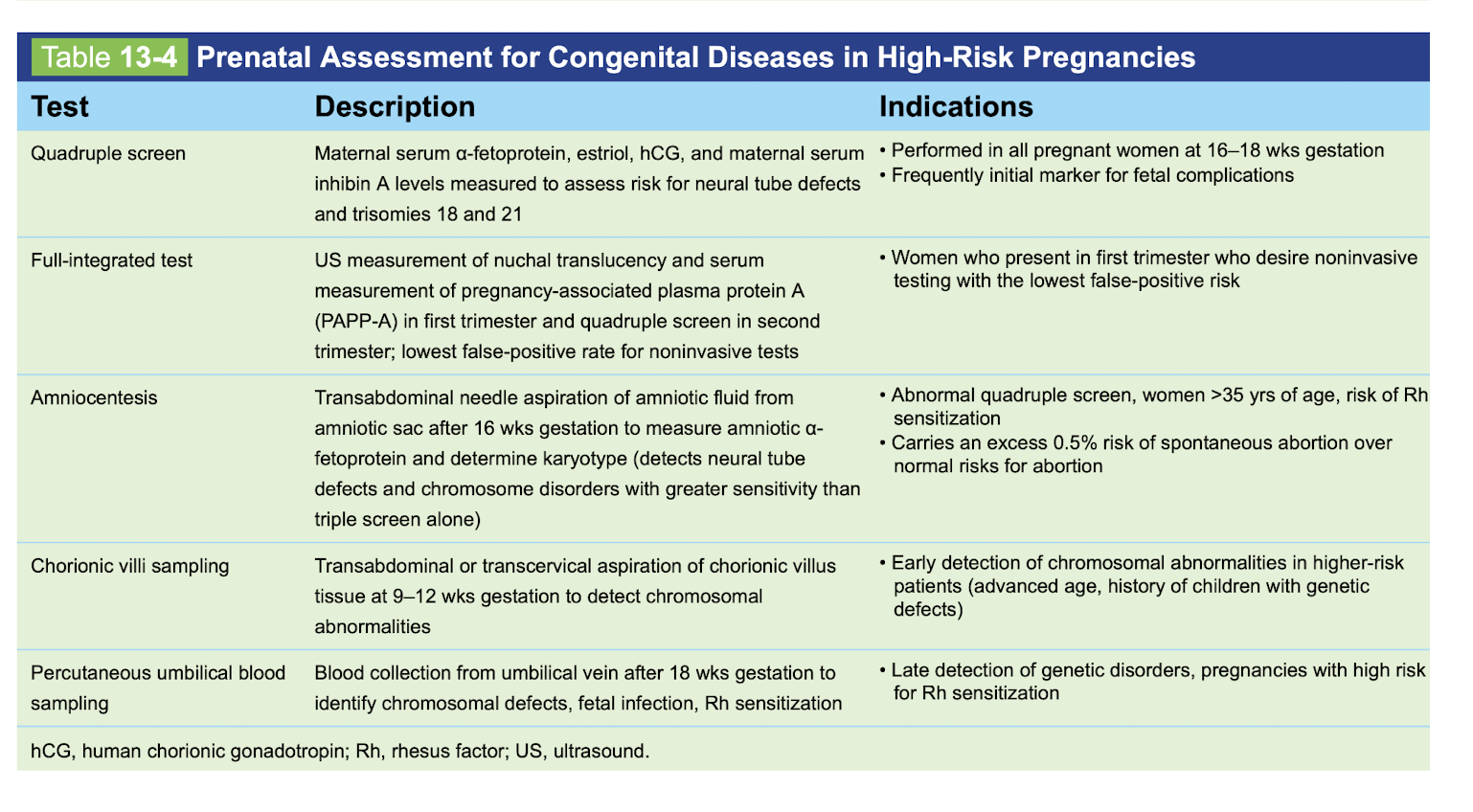
High risk pregnancy tests: description and indications
quadruple screen
full integrated test
amniocentesis
chorionic villi sampling
precutaneoous umbilical blood sampling
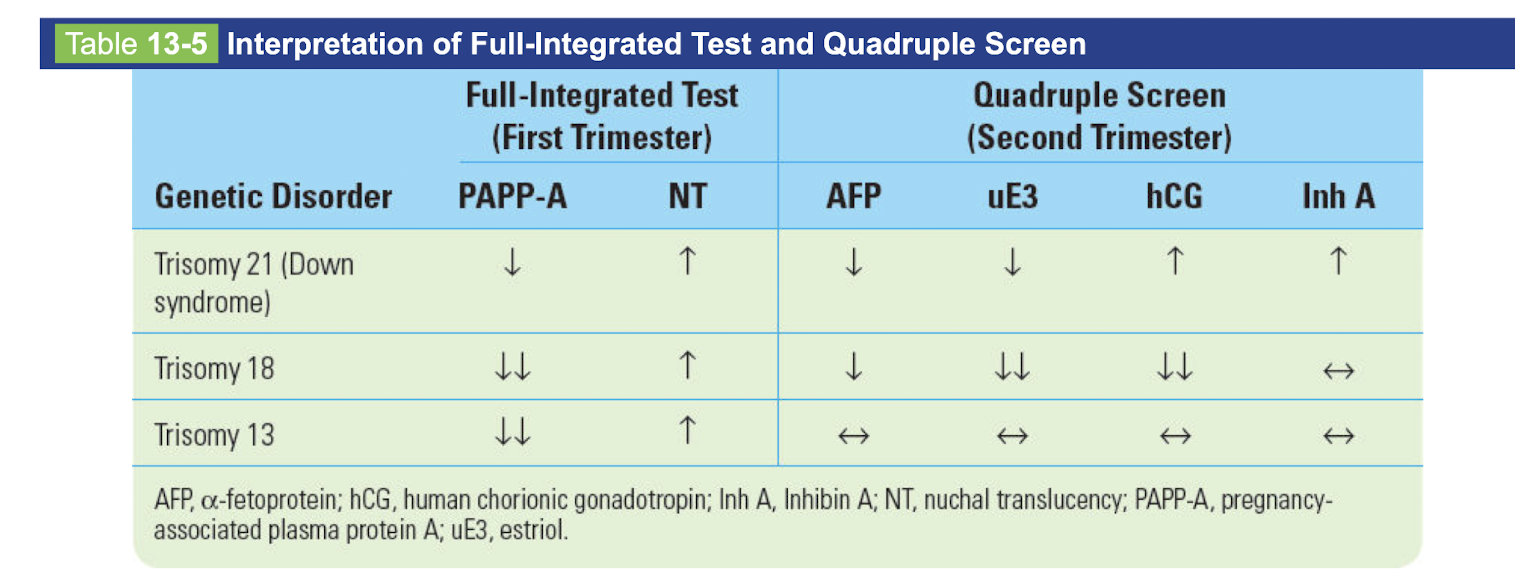
Full integrated test and quad screen
-trisomy 21
-trisomy 18
-trisomy 13
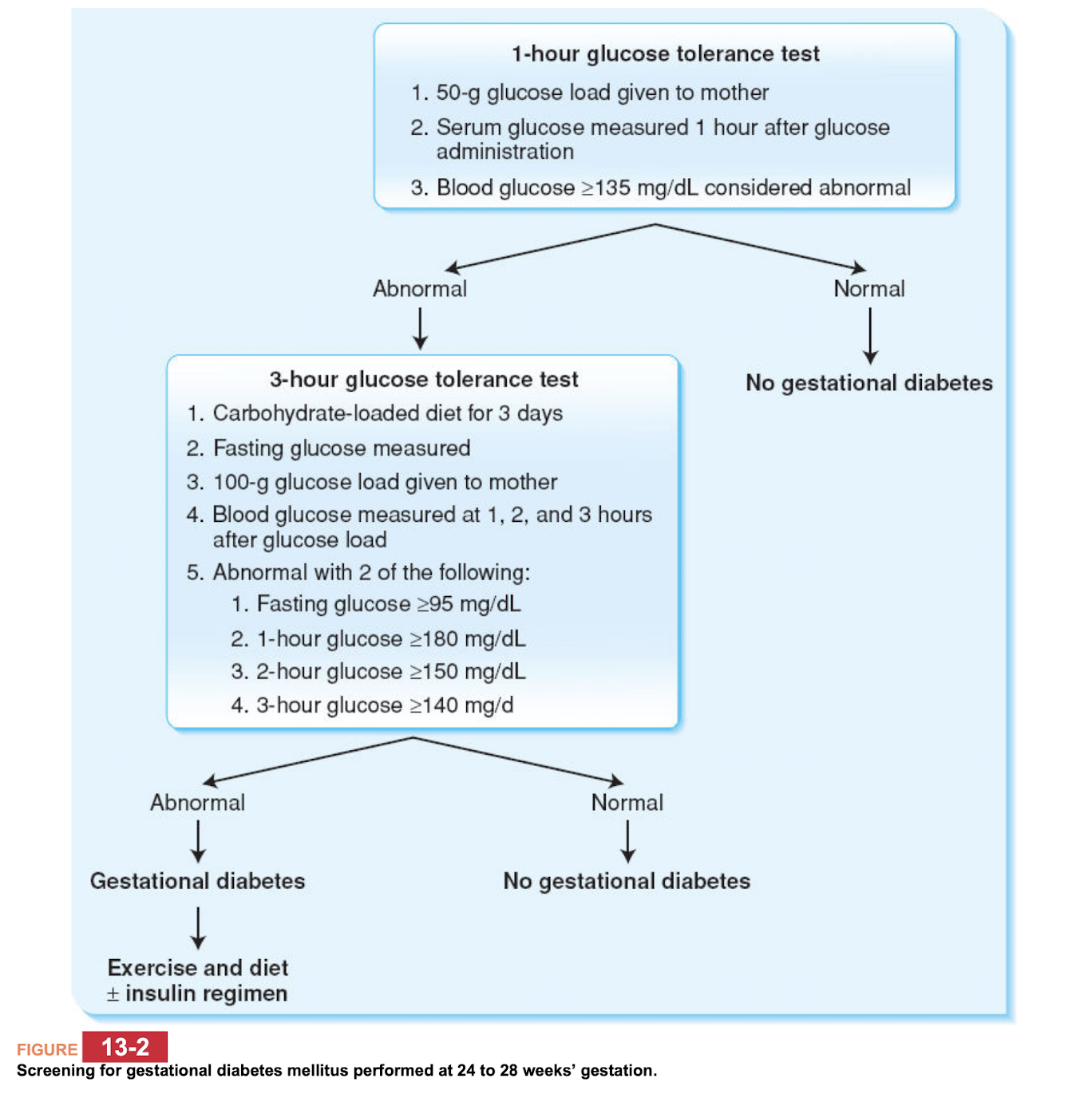
Gestational DM
-most frequently occurs in the
Most commonly occurs in the 2nd and 3rd trimesters
(Usually if presentation is earlier then suspect non GDM)
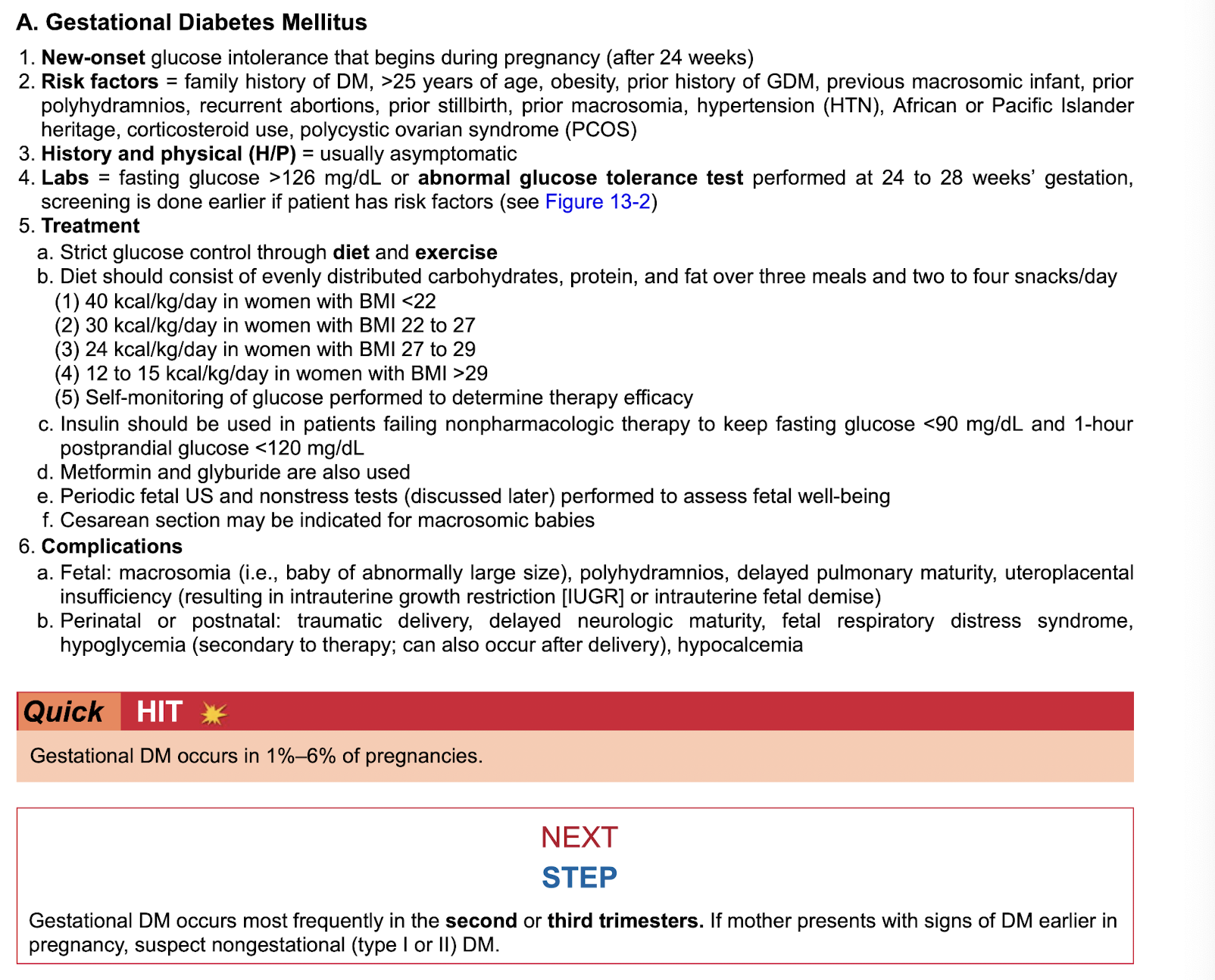
Continue glucose assessment in patients gestational DM
after birth

Gestational DM pathway
Preeclampsia
-def
-rf
-sxs
-labs
-definitive cure
-tx
-complications
Eclampsia
-def
-sxs
-labs
-tx
-complications
-do not confuse witih
-anticonvulsant use in prgnancy
Maternal asthma (pre-existing)
-def
-sxs
-tx
-complications
Maternal n/v
-timeline
-caused by
-sxs
-tx
-Hyperemesis gravidum
Maternal DVT
-def
-sxs
-dx
-radio
-tx
-complications
Anticoagulation during active labor
stop all anticoagulation during active labor until 6 hours after delivery to prevent severe hemorrhage
Maternal UTIS
-more common because
-sxs
-labs
-tx
-what should you not use for tx
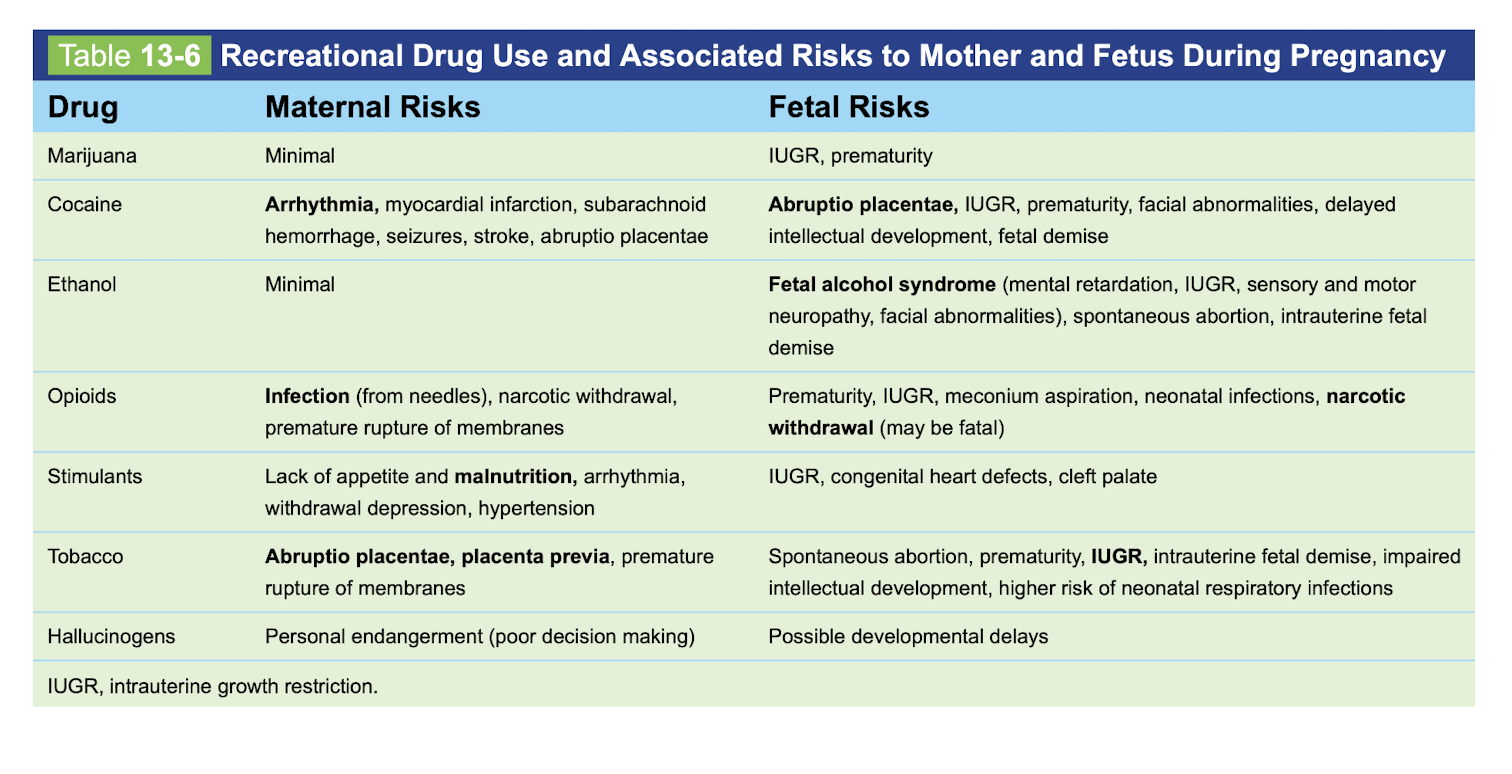
Drug use in mother durign pregnancy
-maternal risks vs fetal risks
weed
cocaine
ETOH
opiods
stimulants
tobacco
hallucinogens
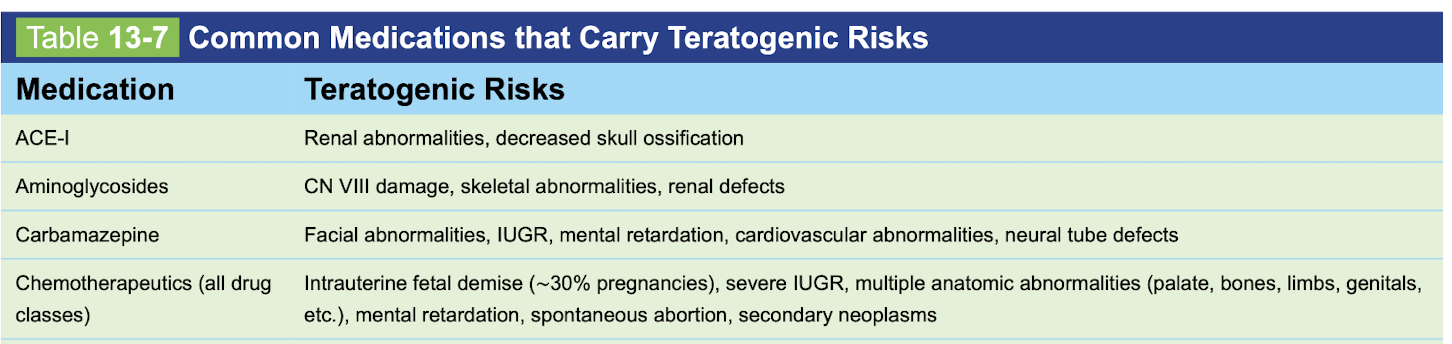
Teratogens
ACE-I
Aminoglycosides
Carbamazepine
Chemotherapies
Teratogens
ACE-I
Aminoglycosides
Carbamazepine
Chemotherapies
Teratogens
-diazepam
-DES
-Fluroquinolones
-Lithium

Teratogens
-phenobarbital
-phenytoin
-retinoids

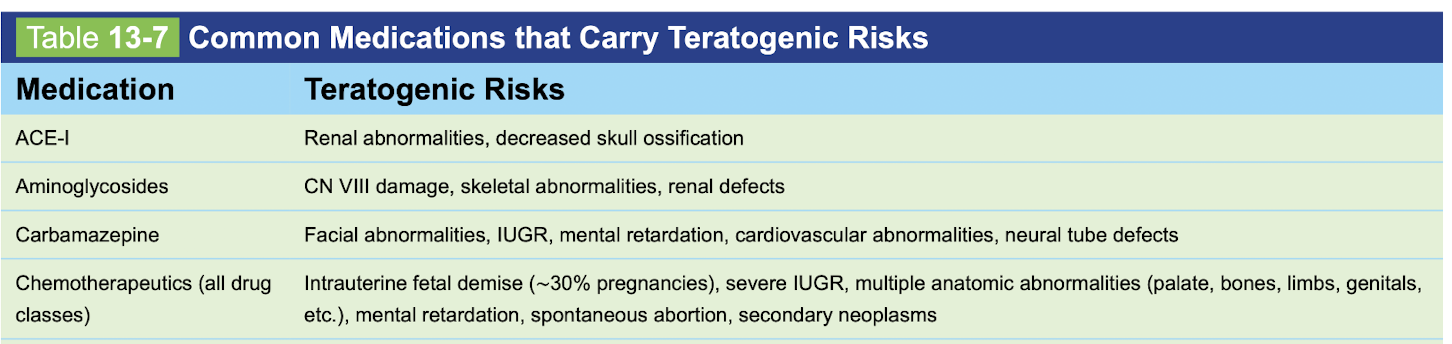
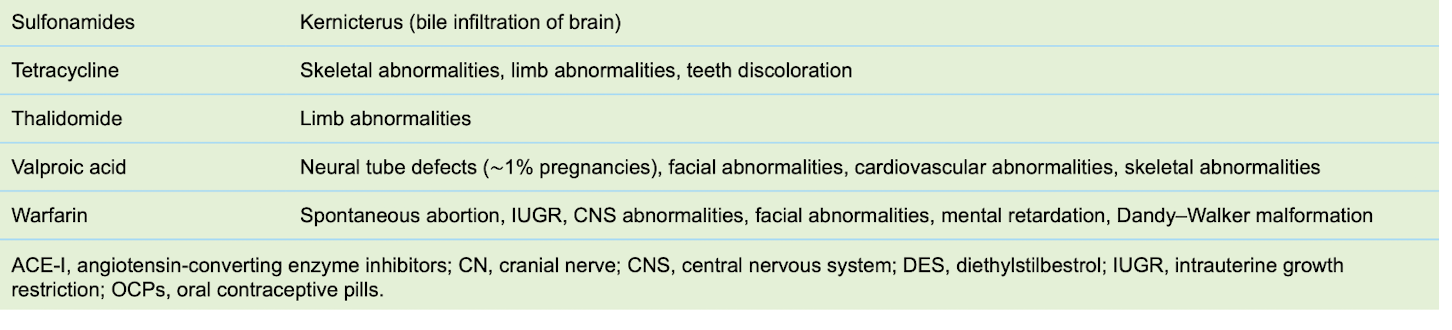
Teratogens
-sulfonamides
-tetracycline
-thalidomide
-valproic acid
-warfarin
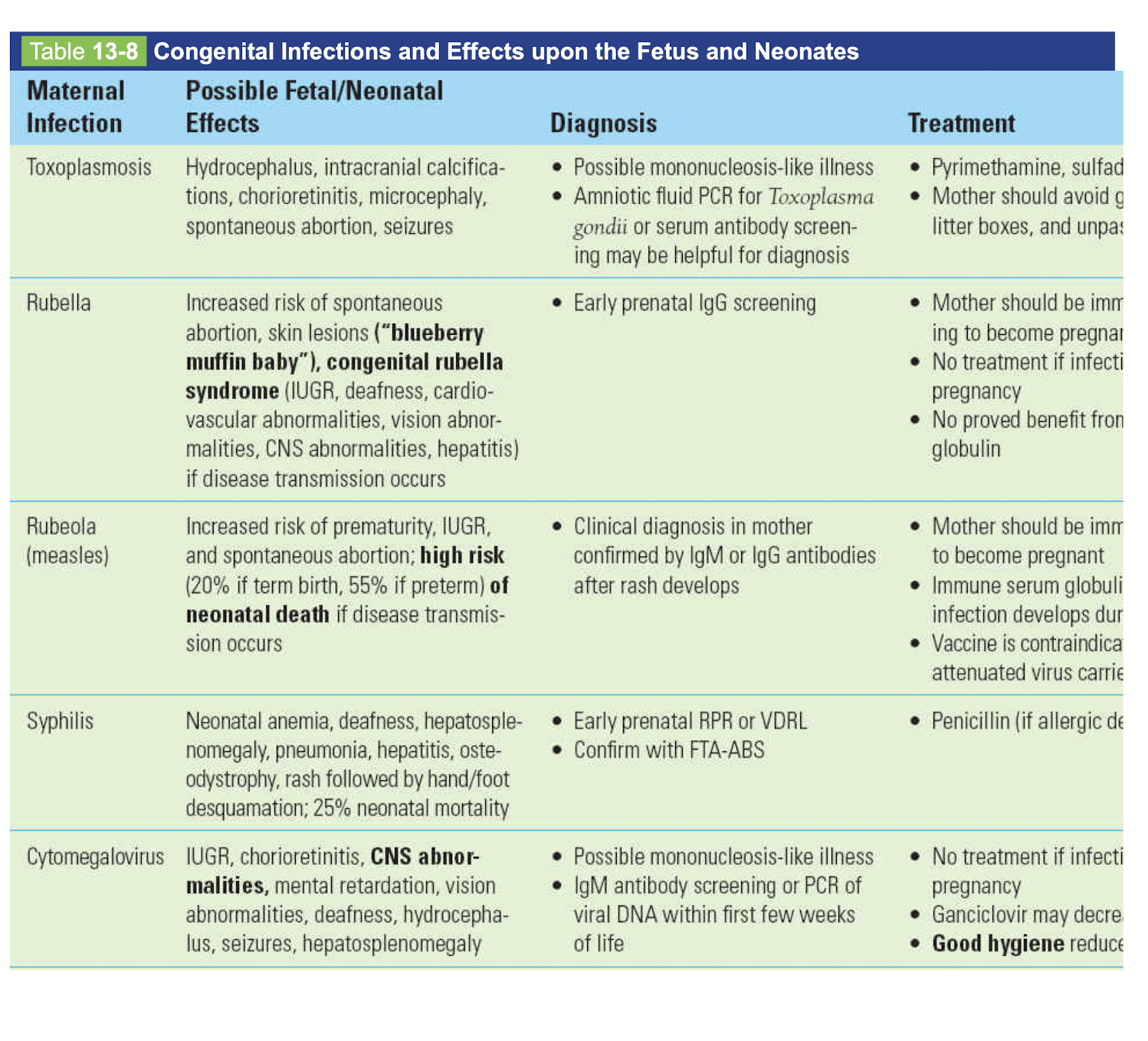
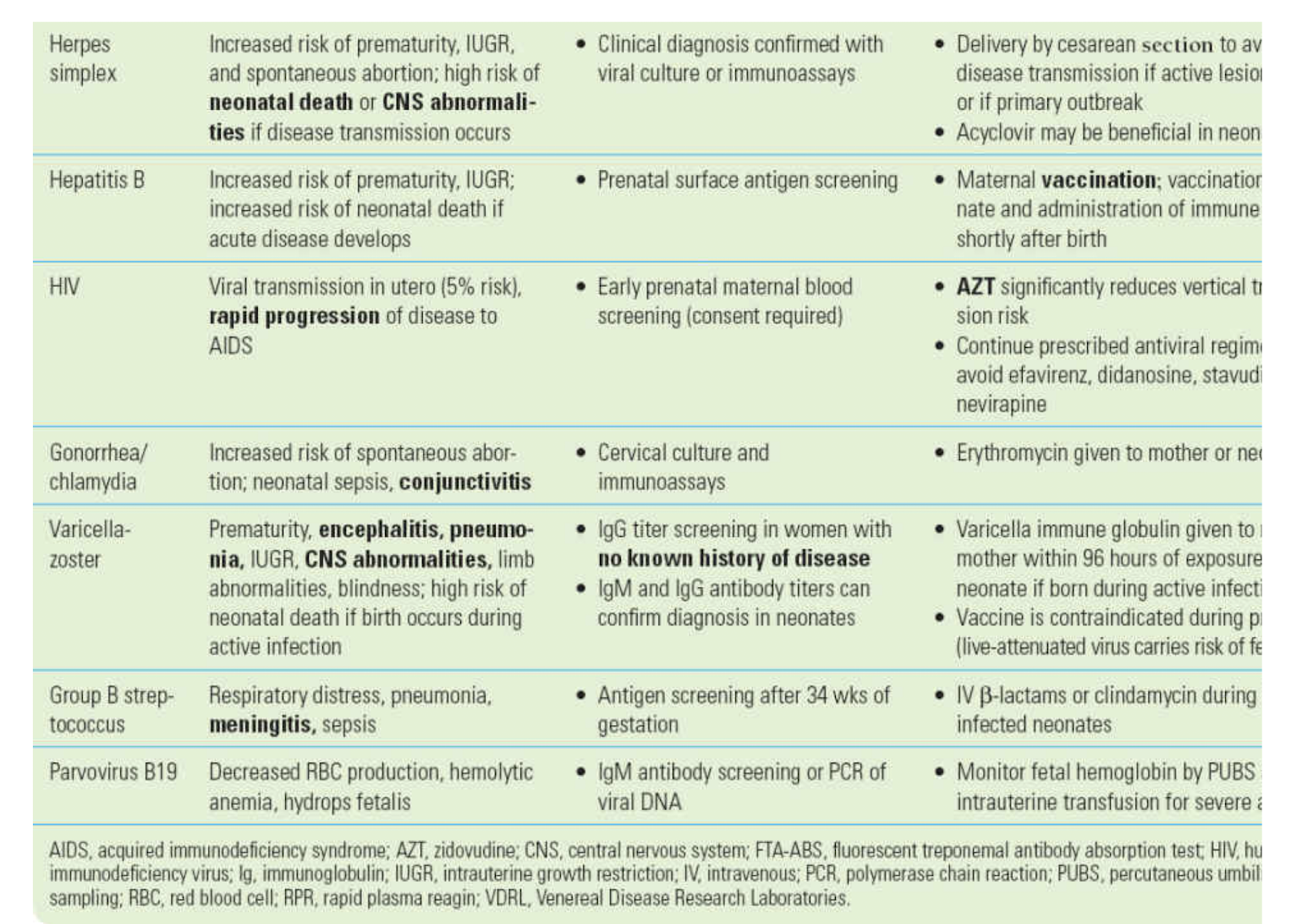
TORCHES
-baby effect
-dx
-tx
Toxo
rubella
rubeola-measles
syphilis
cmv
TORCHES
-baby effect
-dx
-tx
HSV
HBV
HIV
Gonorrhea/chlaymydia
VZV
GBS
Parvovirus B19
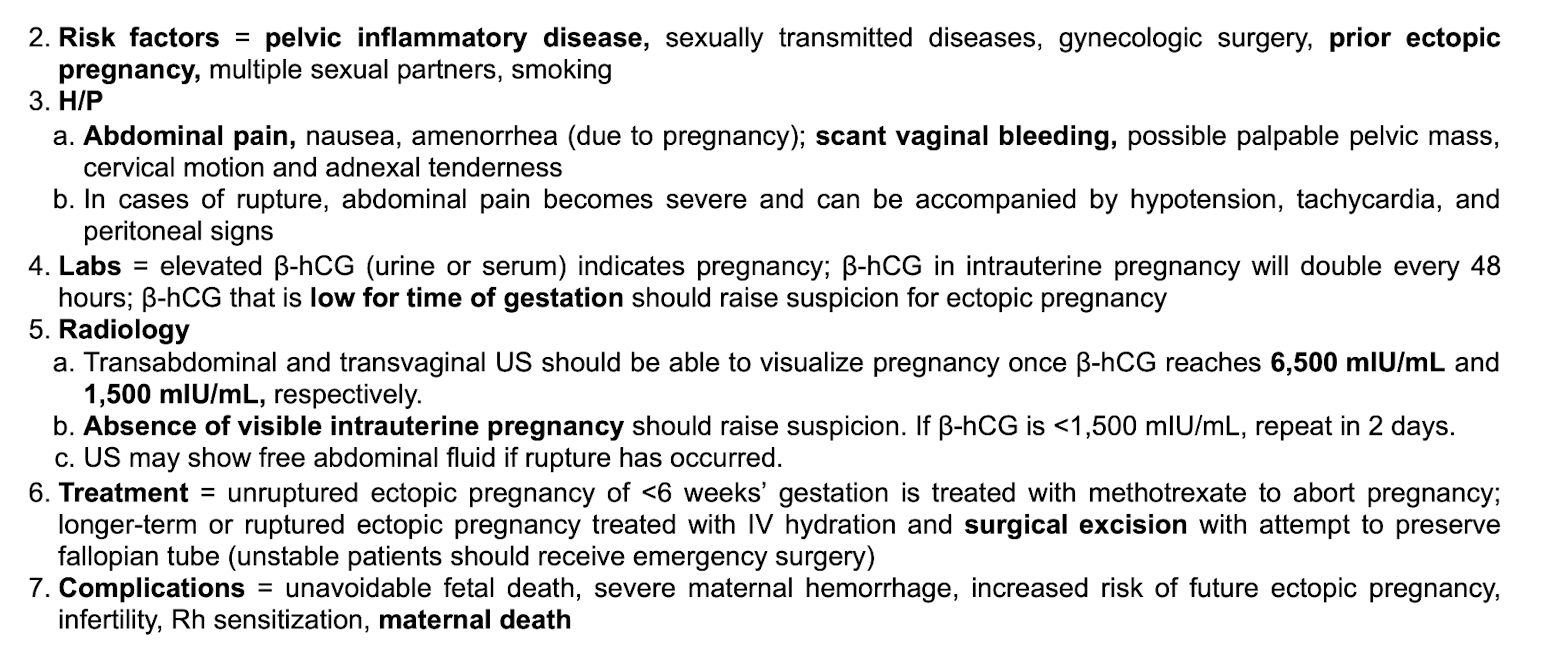
Ectopic pregnancy
-rf
-sxs
-labs
-radio
-tx
-complications
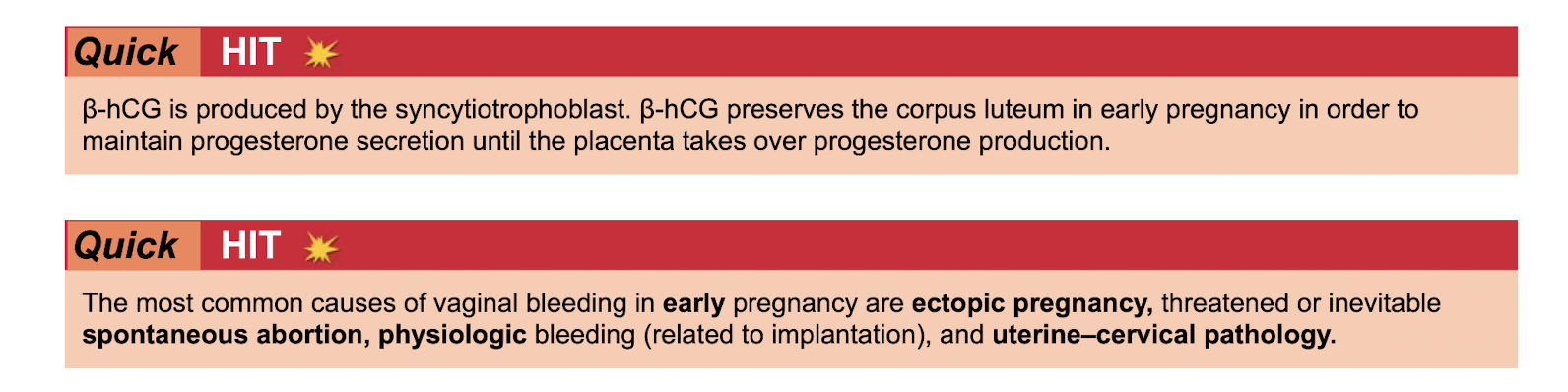
Bhcg is produced by
most common cause of vaginal bleeding in early pregnancy
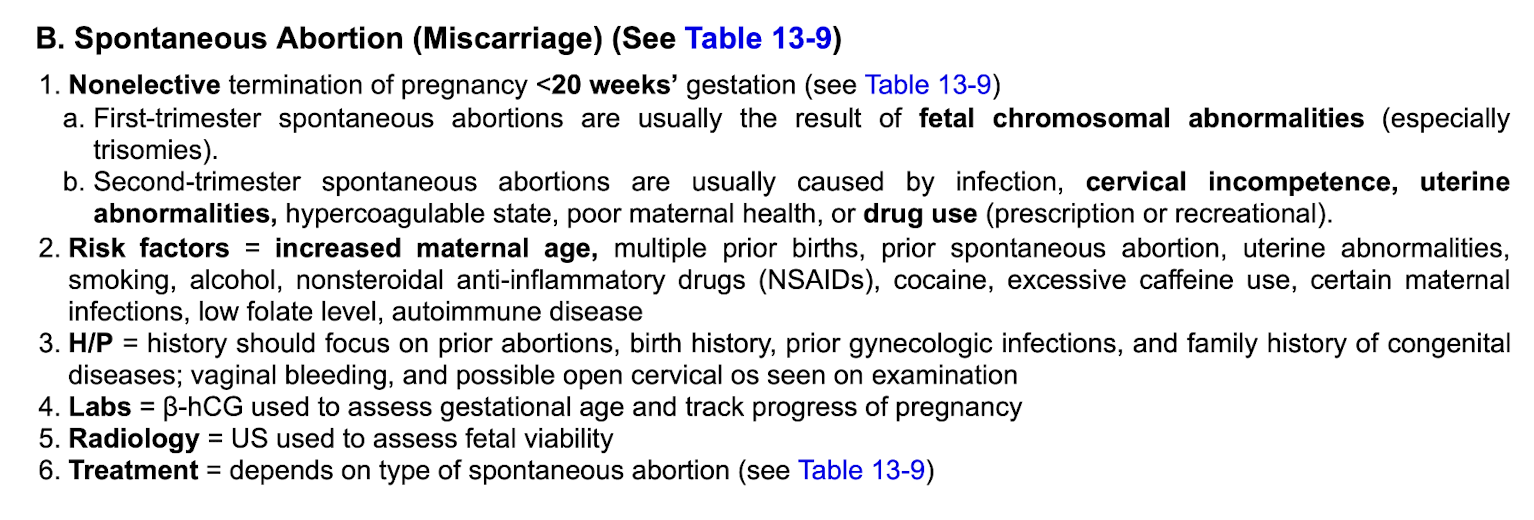
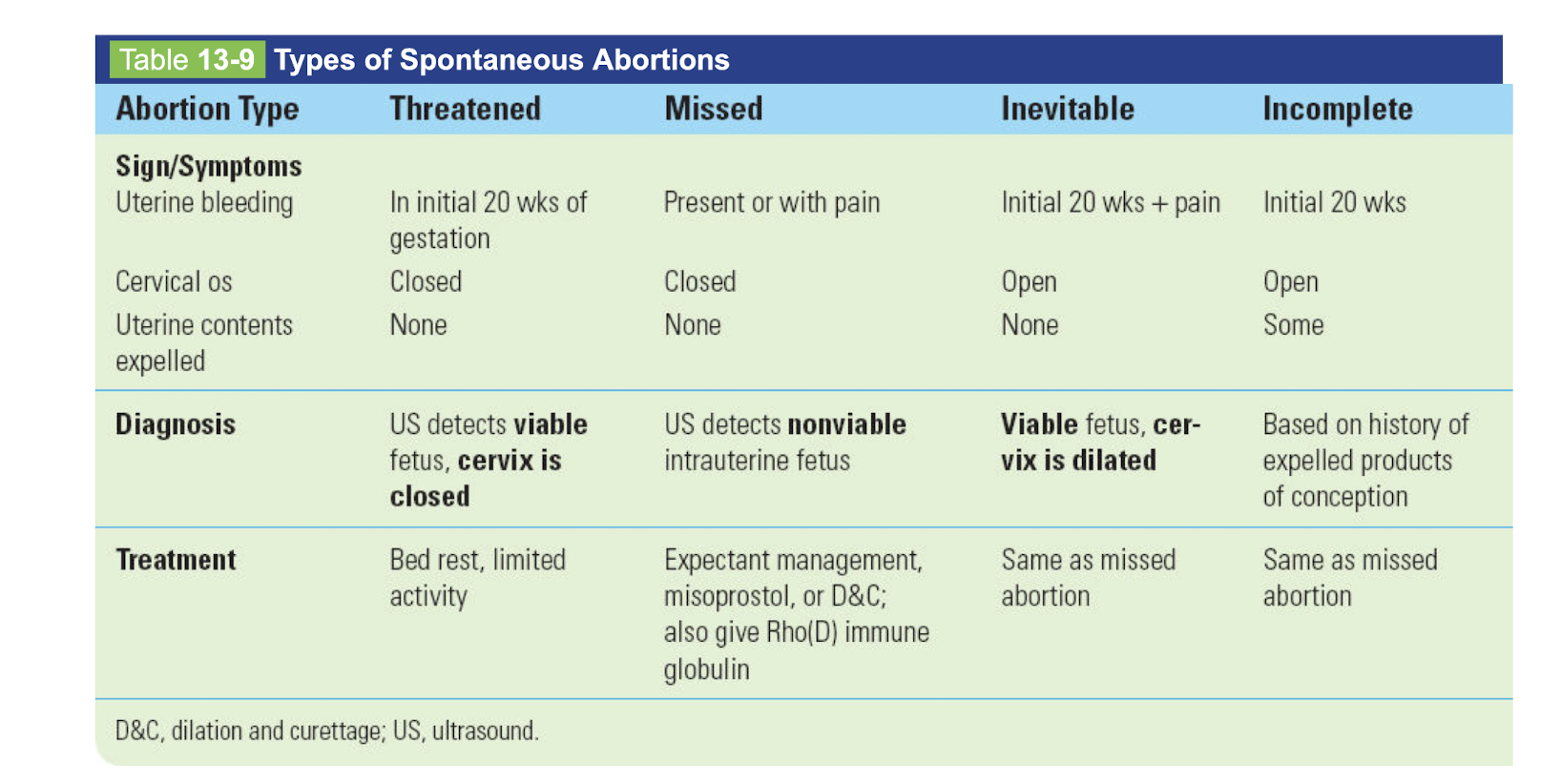
Spontaneous abortion/ Miscarriage
-def
-first tri vs second tri
-rf
-sxs
-labs
-radio
-tx
Sxs/Dx/Tx
threatened abortion
missed abortion
inevitable abortion
incomplete abortion
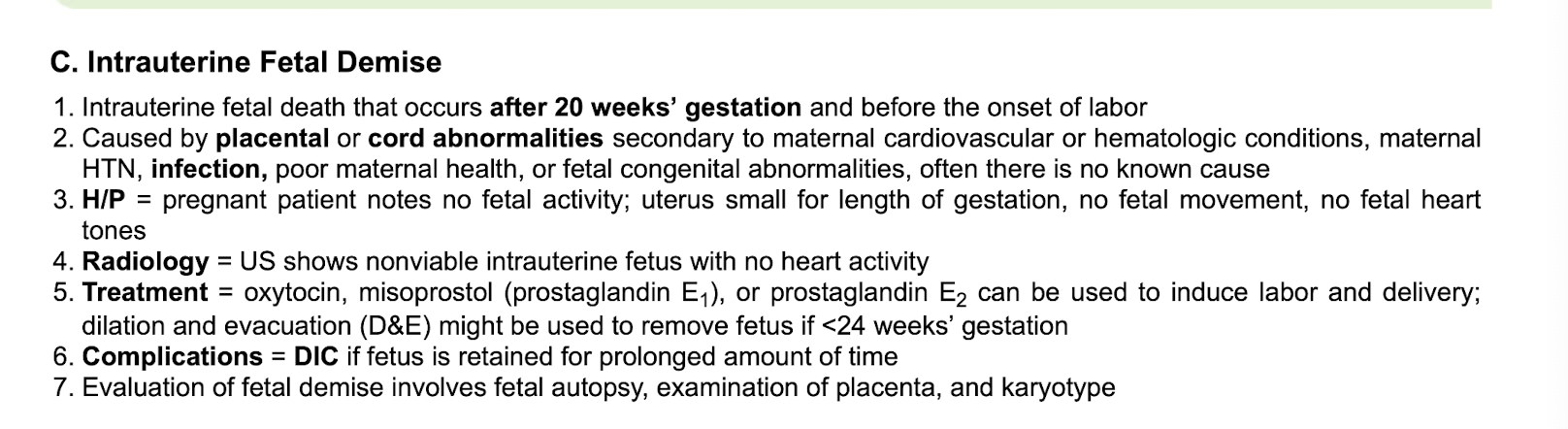
Intrauterine fetal demise
-def
-caused by
-sxs
-radio
-tx
-complications
-evaluation involves
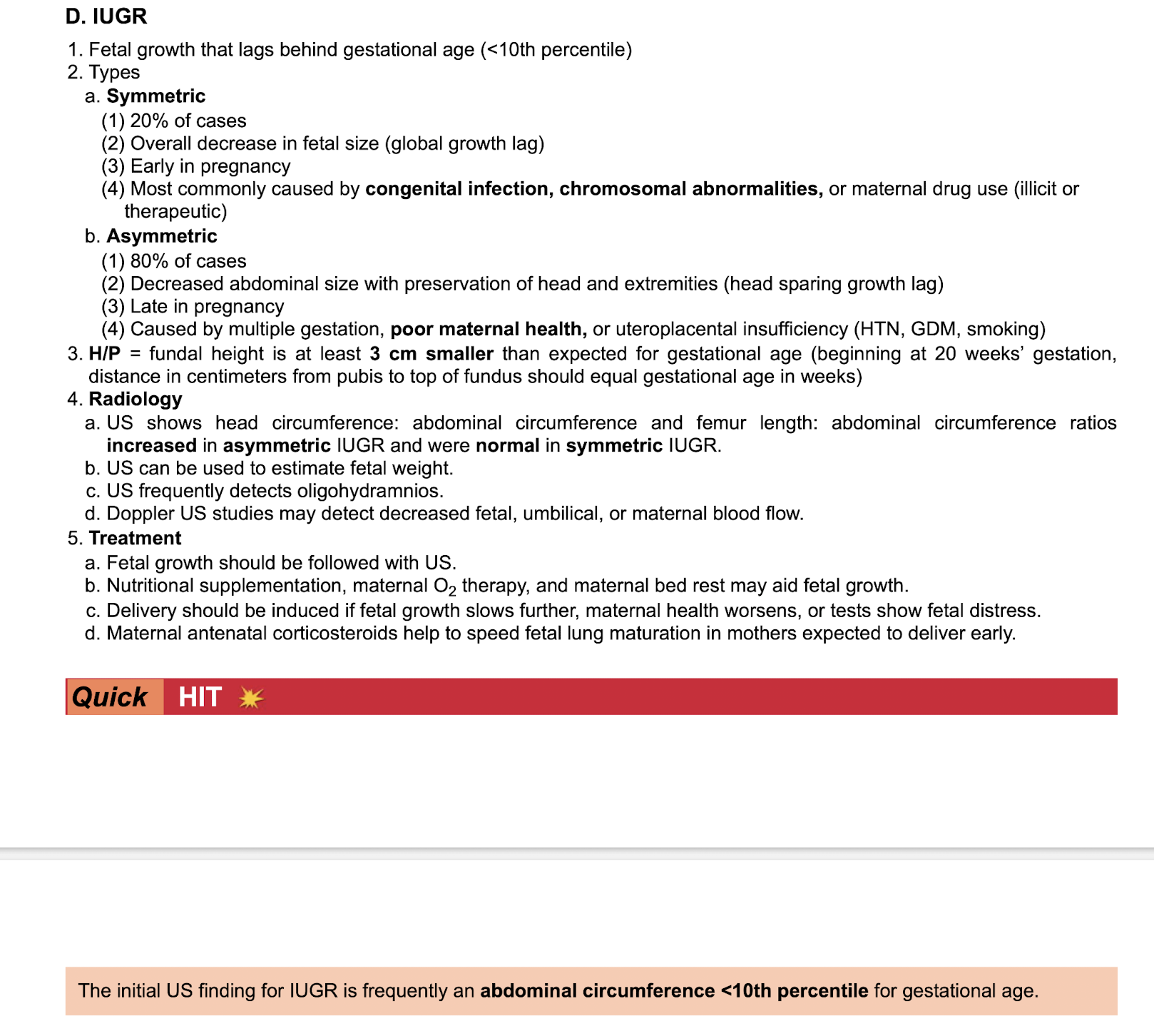
IUGR
-types symmetric vs asymetric
-sxs
-radio
-tx
-initial us finding
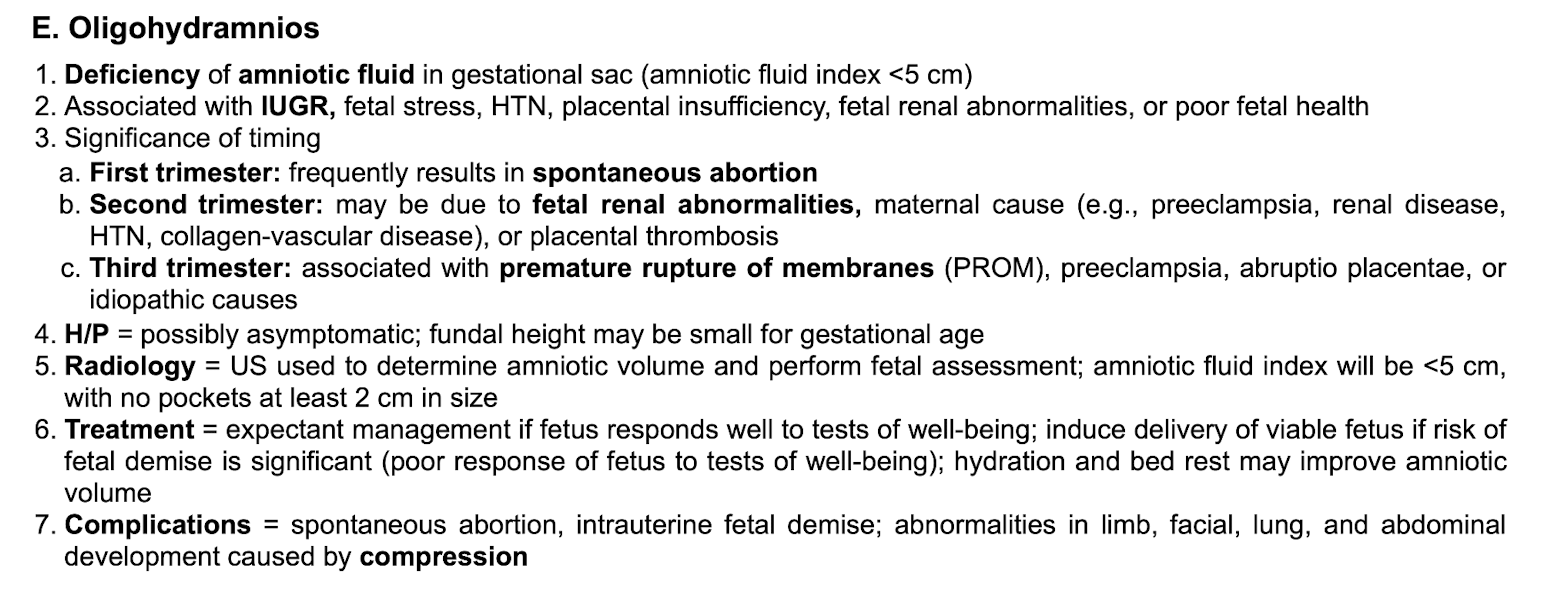
Oligiohydraminos
-def
-associated with
-timing per tri
-sxs
-radio
-tx
-complications
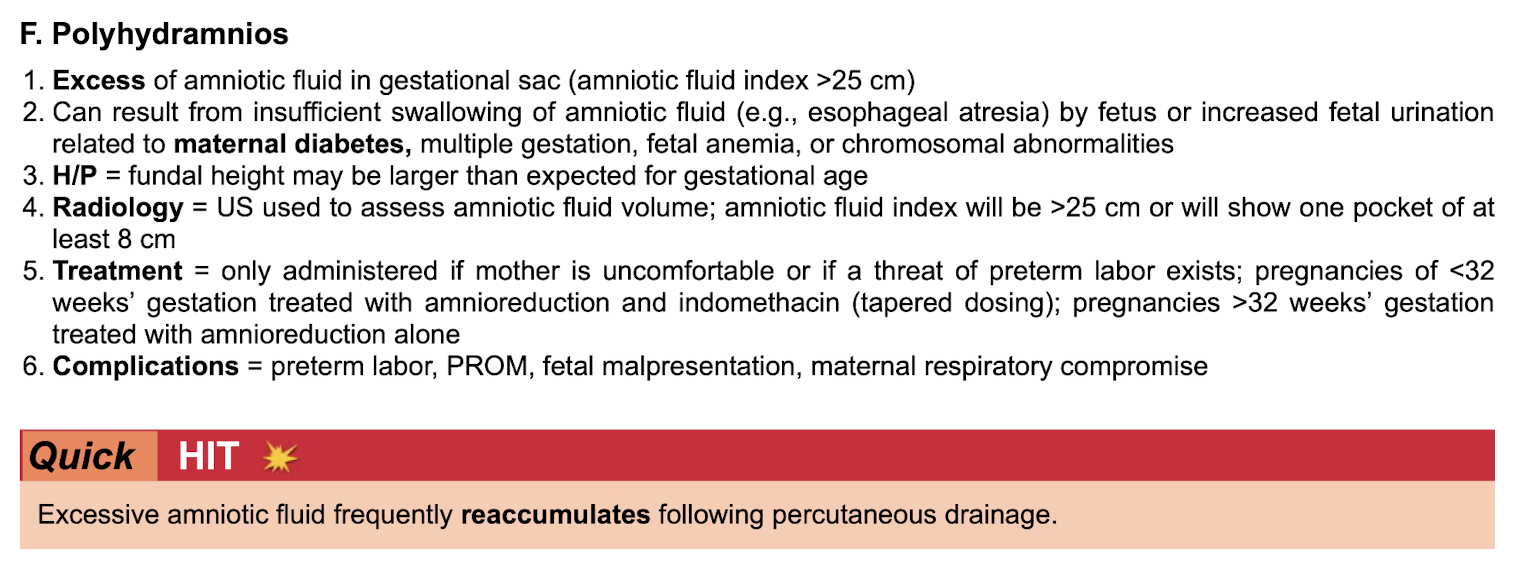
Polyhydraminos
-def
-can result from
-sxs
-radio
-tx
-complications
-can reaccumulate following
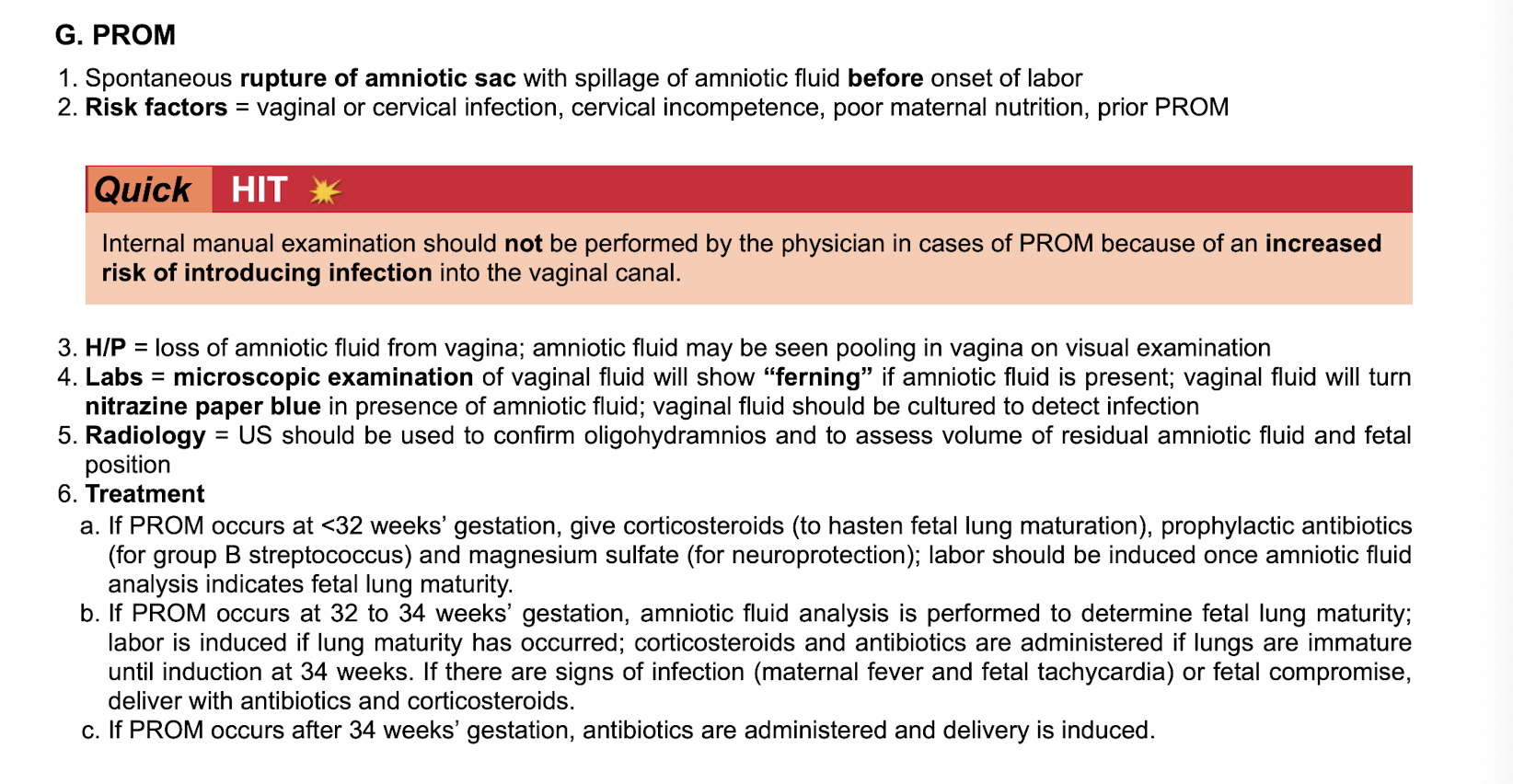
PROM
-def
-rf
-what do you not perform
-sxs
-labs
-radio
-tx based on timing
Fetal lung maturity quantified by

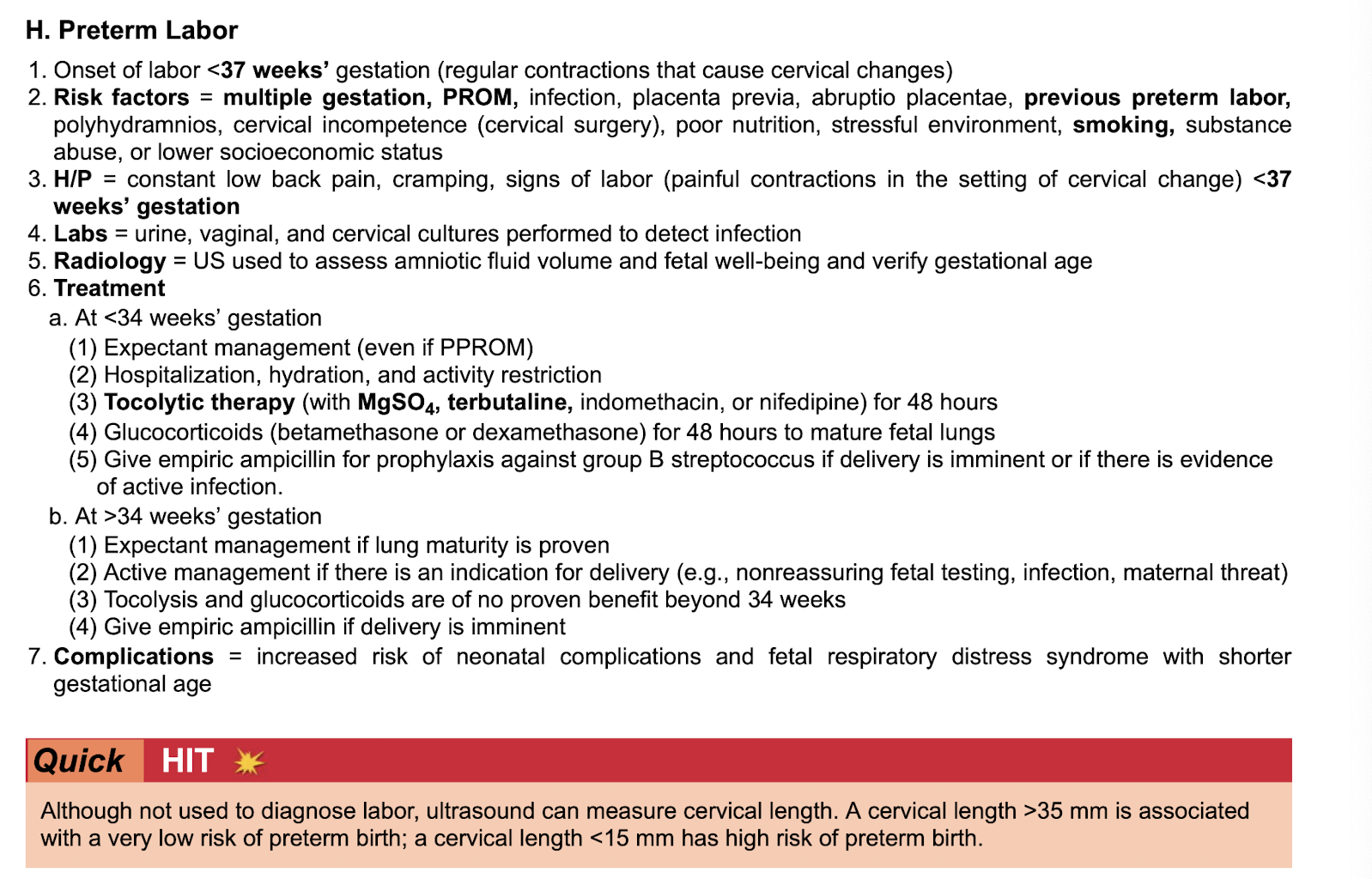
Preterm labor
-def
-rf
-sxs
-labs
-radoi
-tx based on timing
-complications
-cervical length
Placenta previa
-def
-types
low
partial
complete

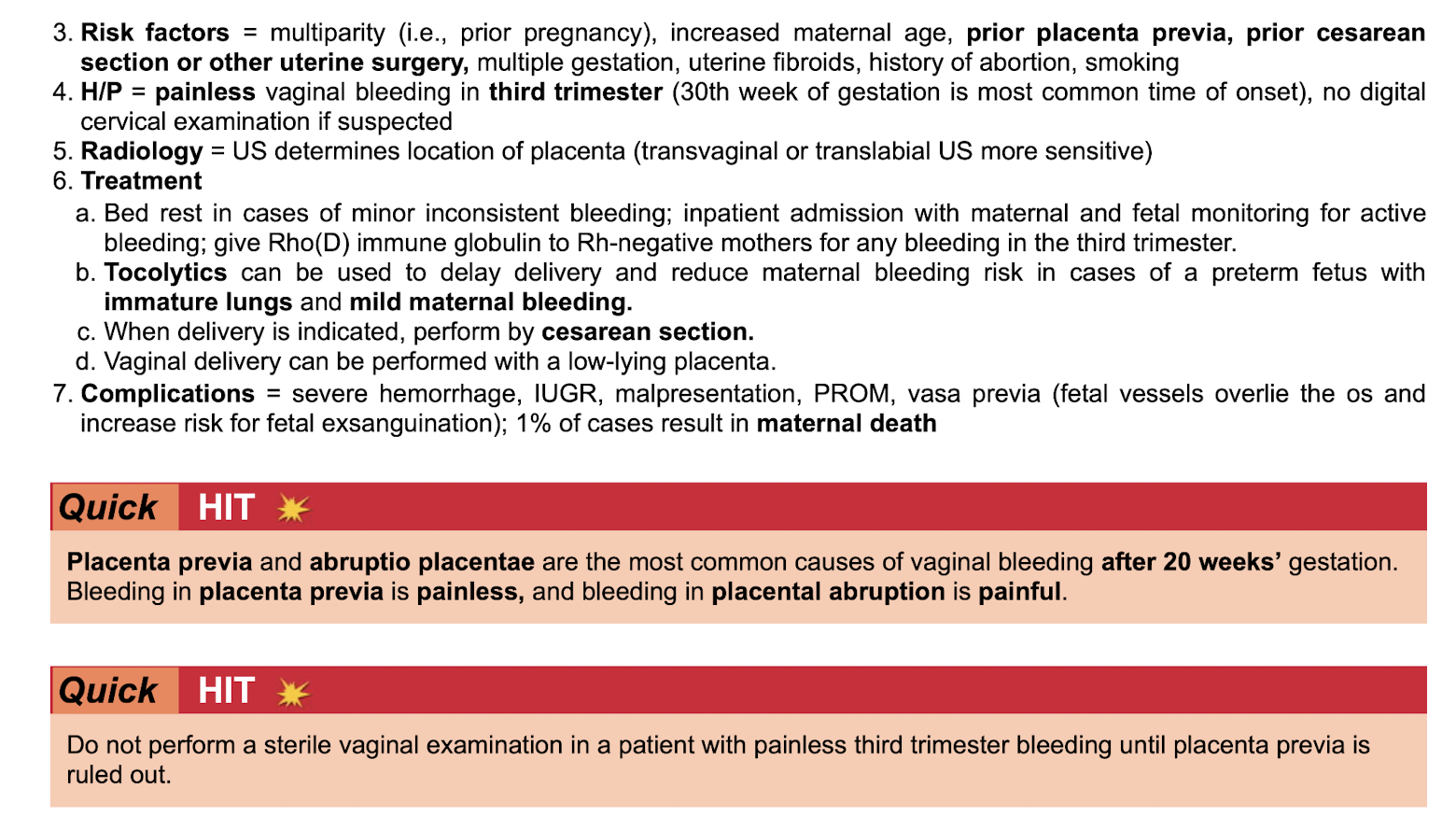
Placenta previa
-rf
-sxs
-radio
-tx
-complications
-after 20 weeks gestation
-do not perform
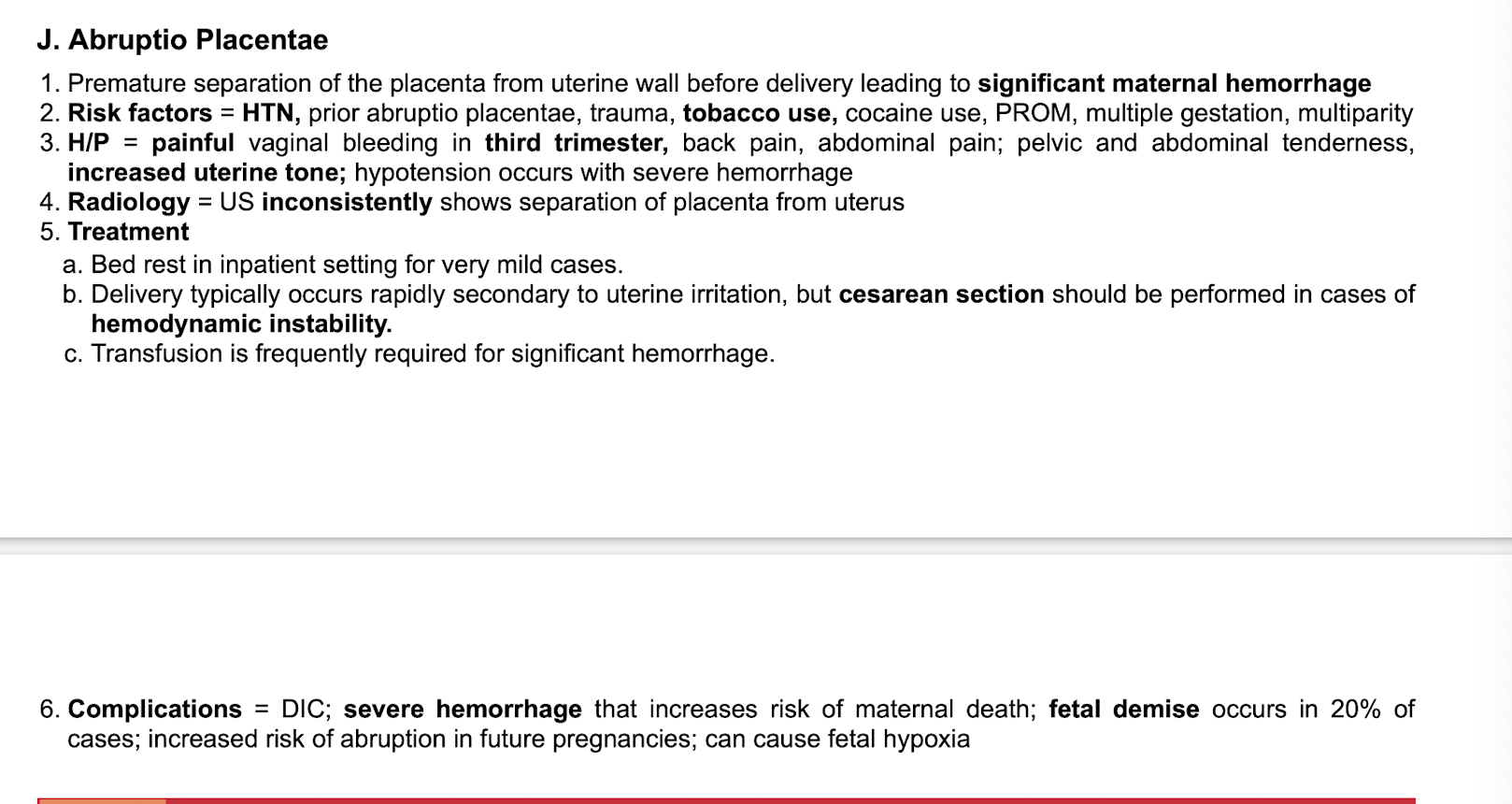
Abruptio placentae
-def
-rf
-sxs
-radio
-tx
-complications
Benign low back pain in pregnancy
radiates to thighs
worsens with activity
improves with rest
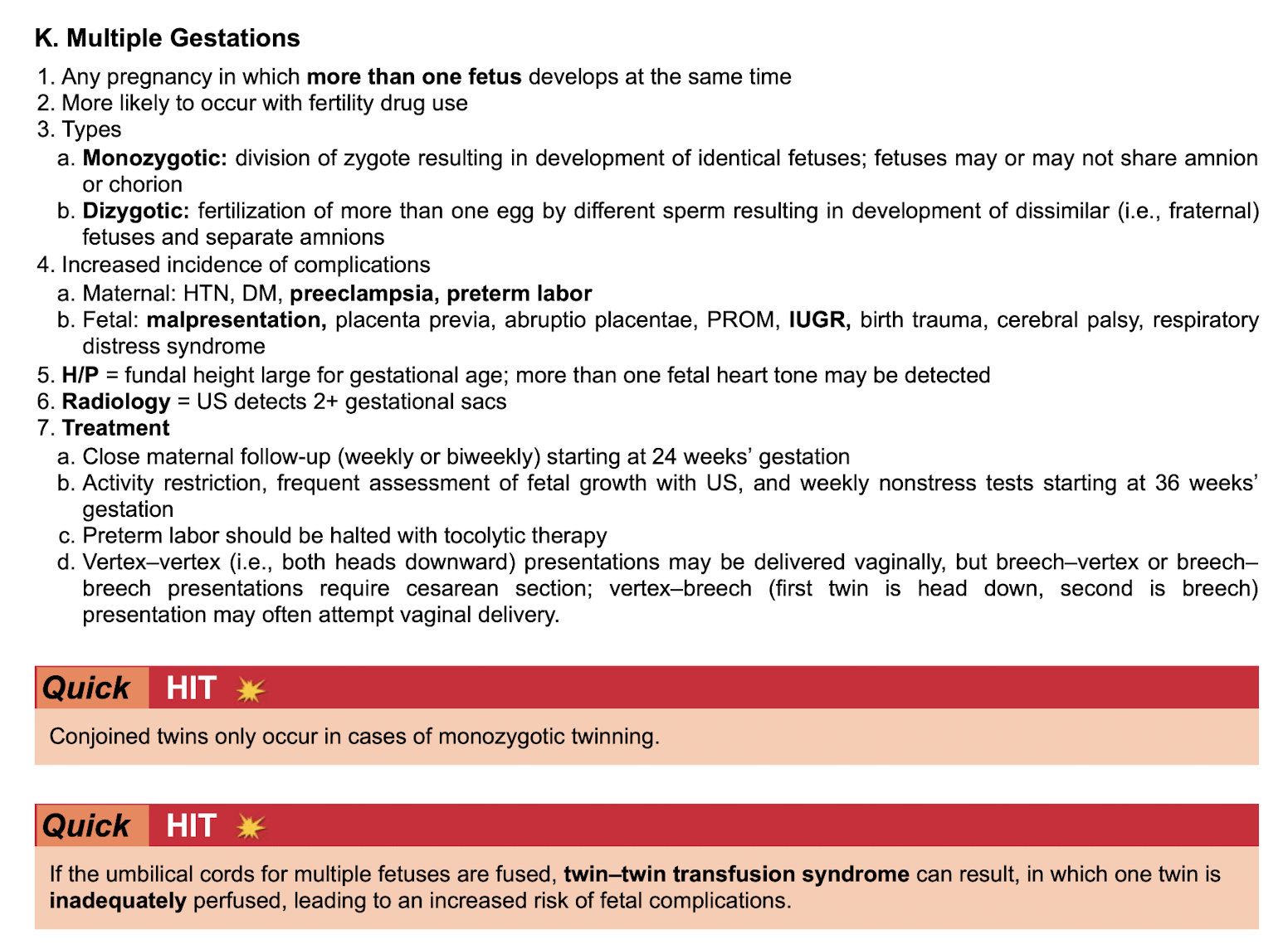
Multi gestaton
-more likely with
-types
-increased incidence of complications mom vs baby
-sxs
-radio
-tx
-conjoined twins only occur in
-twin-twin transfusion syndrome if
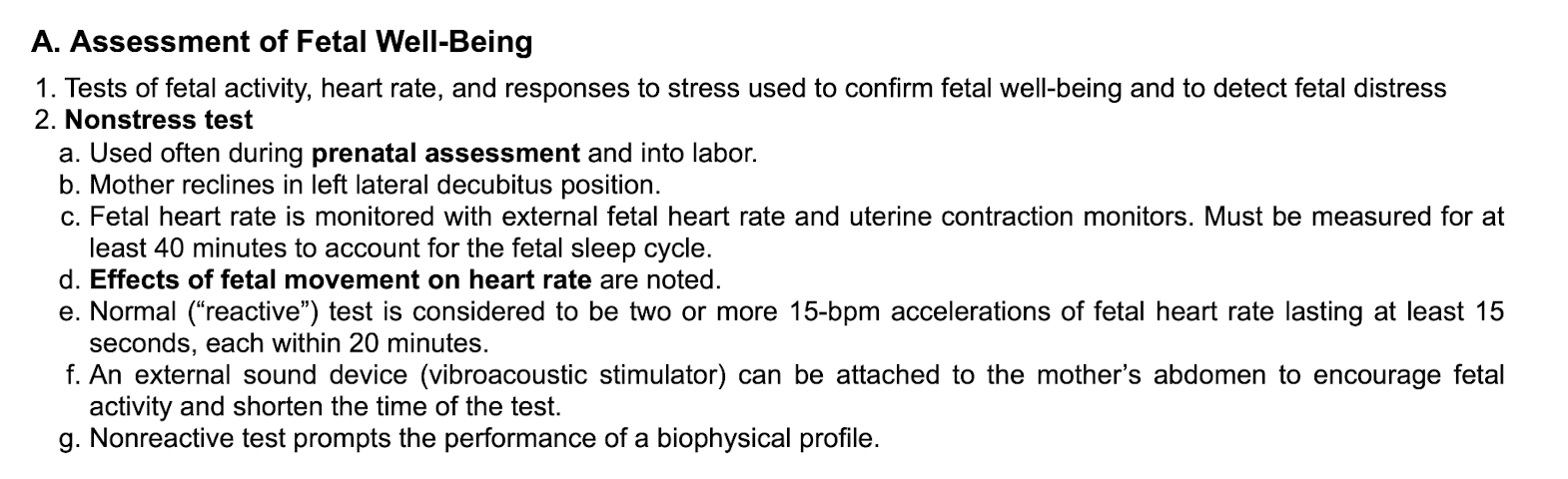
Asessment of fetal well being
-nonstress test
Normal fetal HR
120-160
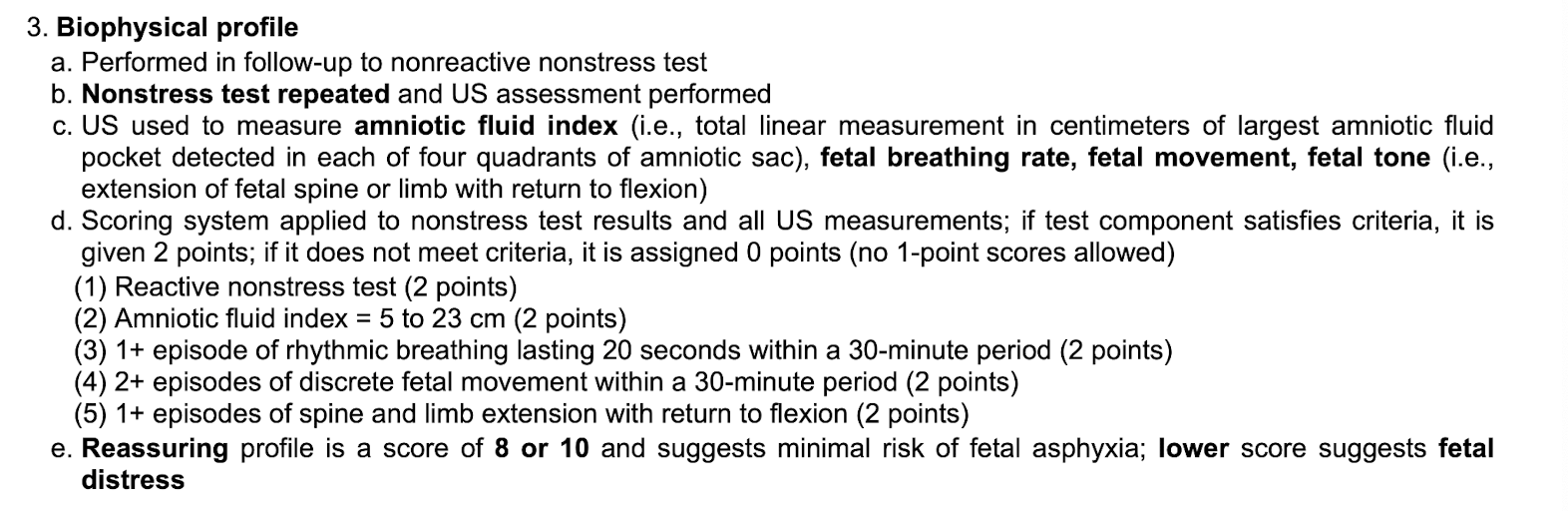
Biophysical profile
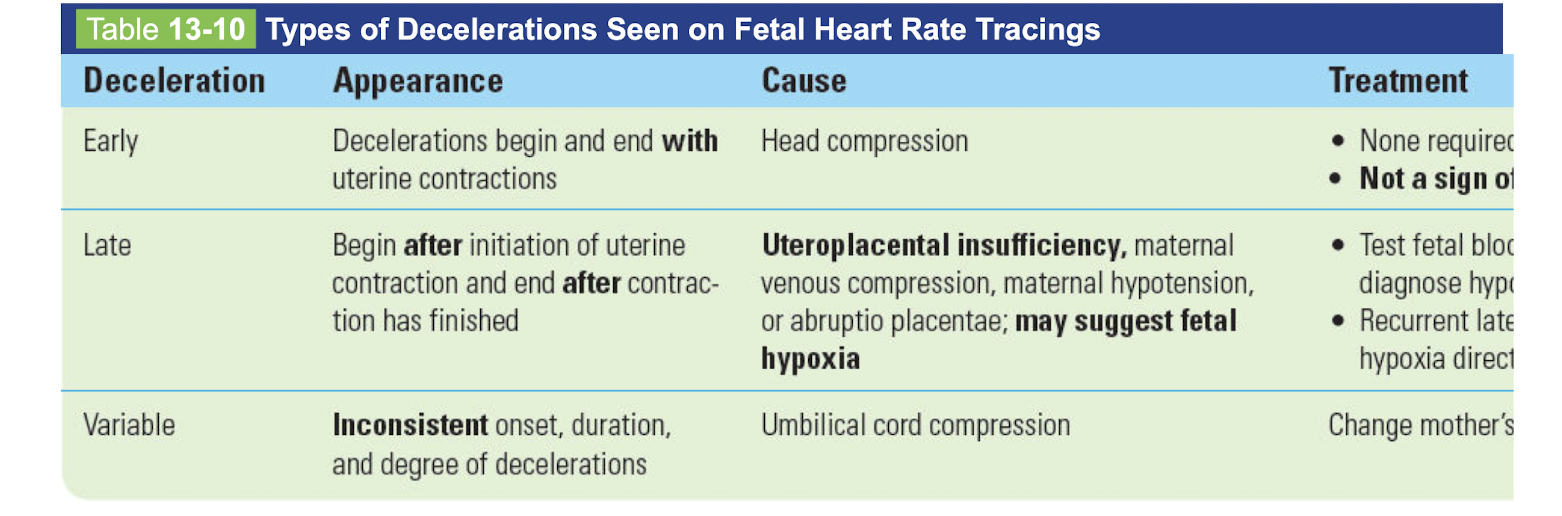
Fetal heart rate tracings
-cause and treatment
early
late
variable
Contraction stress test

Fetal scalp blood sampling
Fetal scalp monitoring

During last few weeks of gestation

Stages of labor
Induction of labor
Malpresenttaion
-normal
-face
-brow
-breech: frank, complete, footling/incomplete
RF
sxs
radio
tx
complications
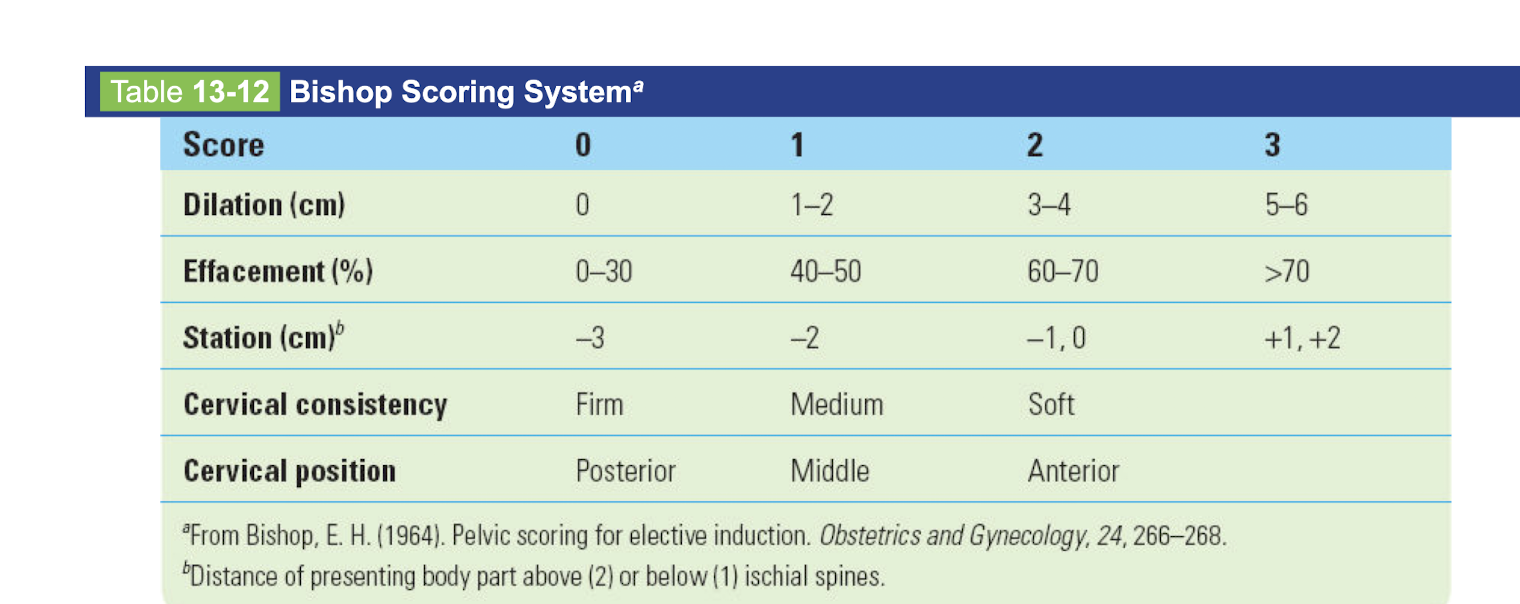
Bishop scoring system
Dilation, effacement percent, station, cervical consistency, cervical position
0-3
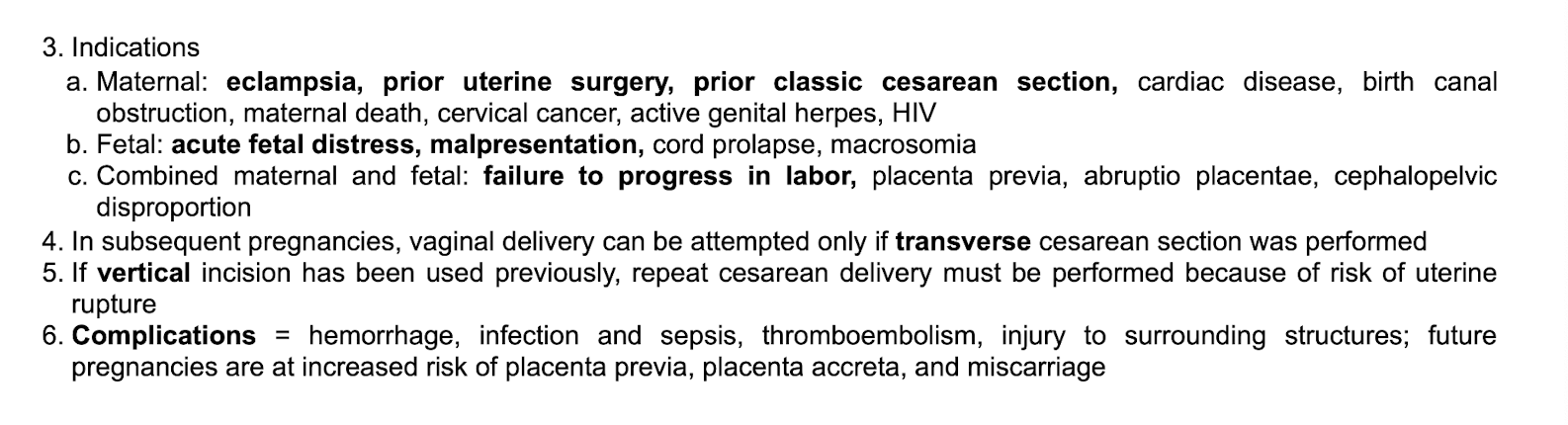
Vertical vs low transverse C-section

csection indications mom vs baby
subsequent pregnancies
-if vertial incision used previously
-complications
breast milk ideal infant nutrient because
contains IgA Abs for newborn
sufficient supply
cost free
mother-infant bonding
colostrum

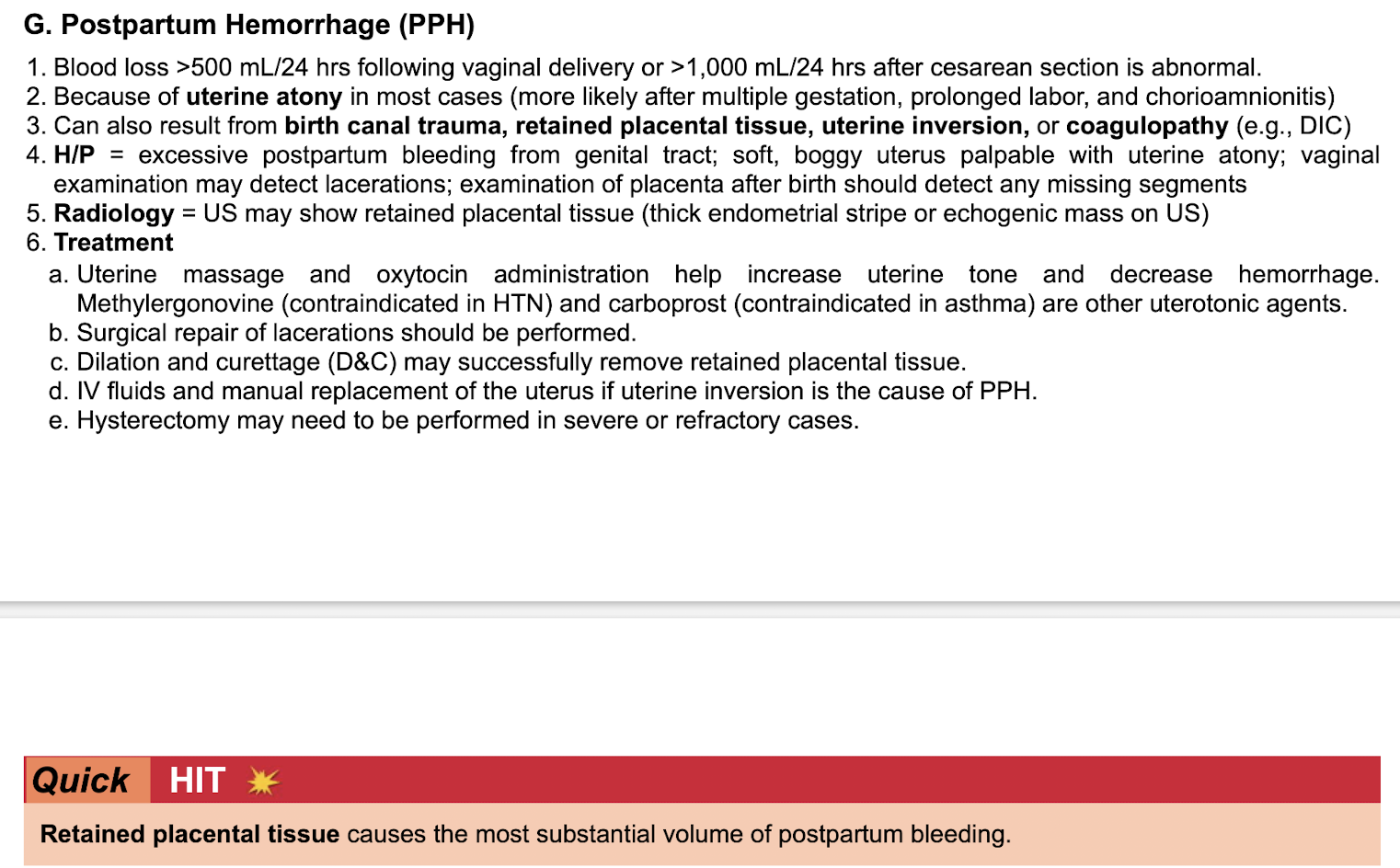
Postpartum hemorrhage
-def
-because of
-can also result from
-sxs
-radio
-tx
-retained placental tissue causes
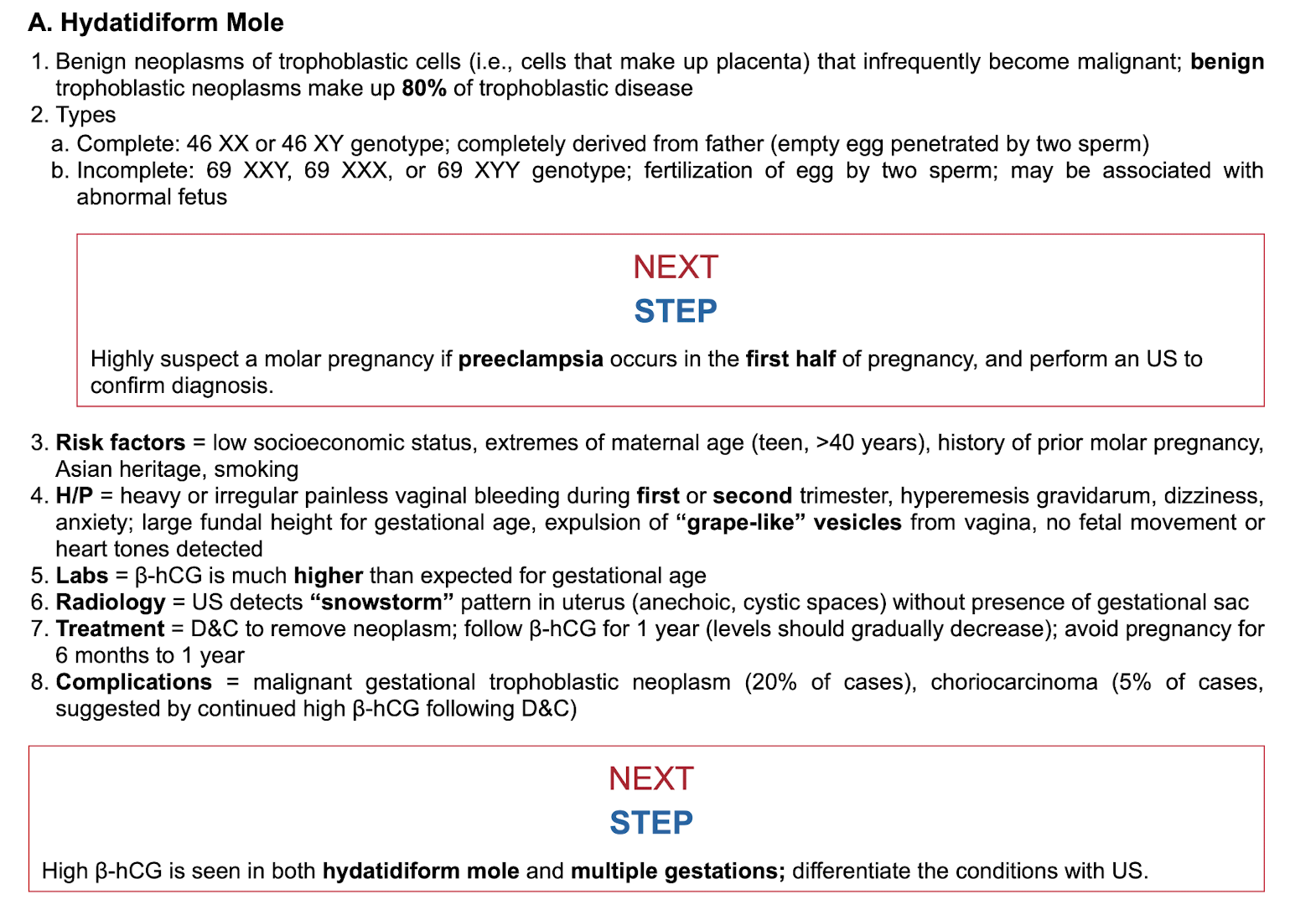
Hydatidiform mole
-def
-types complete vs incomplete
-highly suspect molar prengancy if
-rf
-sxs
-labs
-radio
-tx
-complications
-what is seen in both mole and multigestational pregnancies, differentiate how?
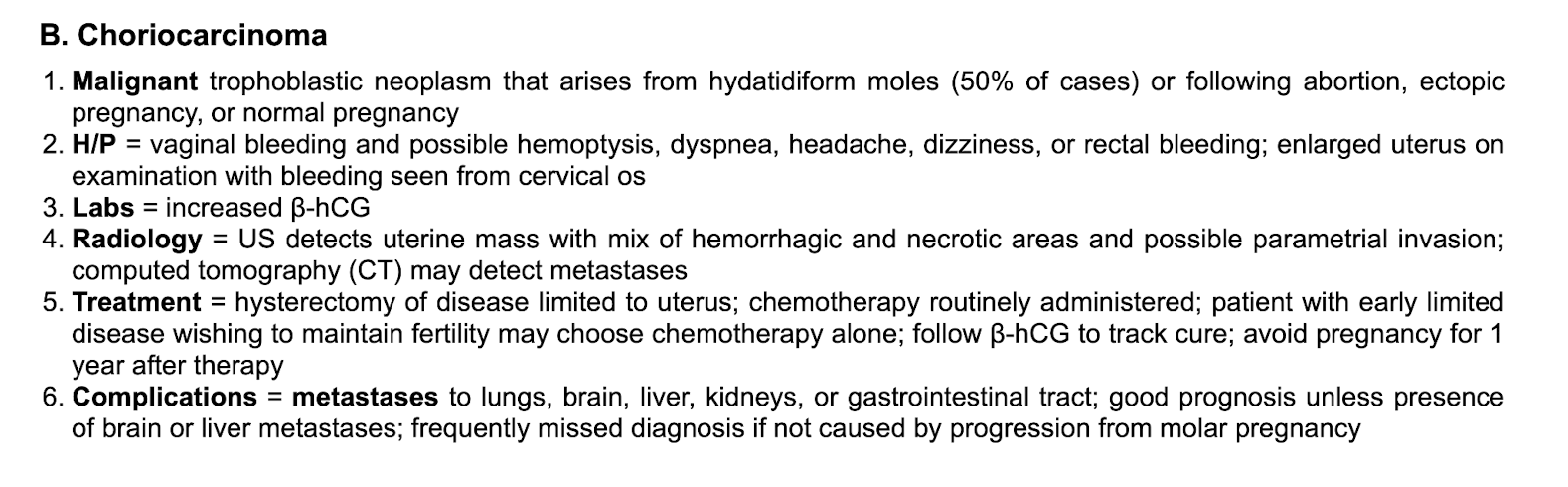
Choriocarcinoma
-def
-sxs
-labs
-radio
-tx
-complications