Unit 2 Lesson 1 Hypertrophic cardiomyopathy
1/29
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
30 Terms
What type of heart failure should you understand in HCM?
Diastolic heart failure.
Explain hypertrophic cardiomyopathy. Its a Disease of the _____ characterized by the presence of what and is it caused by another condition?
Disease of the myocardium characterized by the presence of left ventricular hypertrophy (LVH) in the absence of another cause.
List the 2 conditions that should not be causing the LVH if it is true HCM.
Systemic hypertension
Aortic stenosis
Simple reminder:
HCM = thick LV muscle, but not because of HTN or AS.
List the 4 previous/alternative names for HCM.
Idiopathic hypertrophic subaortic stenosis, or IHSS
Muscular subaortic stenosis
Obstructive cardiomyopathy
Asymmetrical hypertrophy
Simple reminder:
Older names for HCM often describe the thick muscle or obstruction below the aortic valve.
Explain the etiology and prevalence of HCM.
How common? (in which group)
the prevalence of HCM of approximately what % in the _____ population?
HCM is the most common genetic cardiomyopathy and has a prevalence of approximately 0.2% in the general population.
HCM is the most common cause of what major event in what age population? and give me a example
HCM is the most common cause of sudden cardiac death in the young, including trained athletes.
High-yield reminder:
HCM is a major cause of sudden cardiac death in young athletes
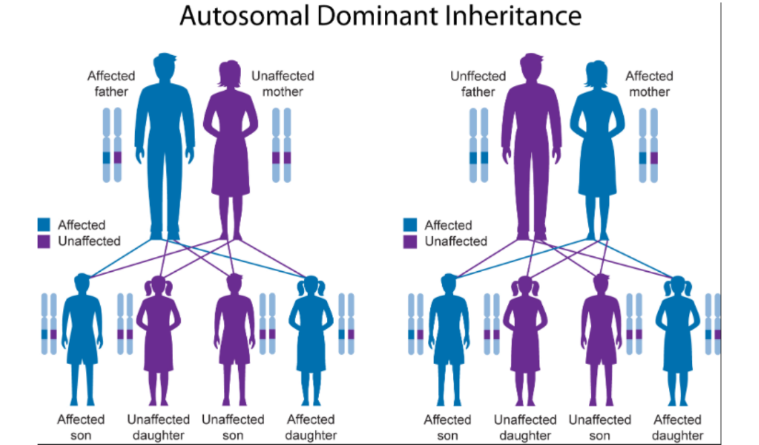
What inheritance pattern is associated with HCM? - which trait?
HCM is associated with an autosomal dominant trait.
An individual will only need to get an abnormal gene from ONE parent to inherit the disease. 50% chance
(Both males & females are affected at the same Rate)
What does idiopathic mean? what is it also called? and is it a result of any other disease?
Idiopathic means a disease has no known cause, also called agnogenic, and is not the result of any other disease.
Simple reminder:
Idiopathic = unknown cause / not caused by another disease.
Where does HCM fit in the AHA classification of cardiomyopathies?
HCM is classified as a primary cardiomyopathy that is genetic.
What does primary cardiomyopathy mean?
It means the disease is predominantly involving the heart.
High-yield reminder:
AHA classification: HCM = primary genetic cardiomyopathy.
Who is genetic testing recommended for in HCM, and what is one limitation?
Genetic testing is recommended for first-degree relatives, but it is limited because all genes causing HCM are not yet identified or may be absent from testing panels.
List the 3 first-degree relatives who may need genetic testing.
Parents
Siblings
Children
Simple reminder:
A negative genetic test does not always fully rule out risk because not every HCM gene is known or tested.
List the 4 main assessment tools used for HCM.
Clinical assessment, including H&P
12-lead EKG
Echo
CMR
CMR = Cardiac Magnetic Resonance imaging.
It is basically an MRI of the heart.
List the 3 symptoms assessed during clinical assessment.
Chest pain
Dyspnea
Syncope (fainting spells or passing out)
List the 5 possible 12-lead EKG findings in HCM. what is the most common one
LVH **** (most common to see)
Repolarization abnormalities
T-wave inversion
Abnormal Q waves
High-voltage QRS
Repolarization abnormalities = abnormal ST/T-wave changes on EKG, meaning the ventricles are not “resetting” electrically in a normal pattern after contraction. In HCM, this can happen because the myocardium is thickened and stressed.
Repolarization abnormalities means the heart’s electrical system is showing an abnormal pattern during the recharging phase of the heartbeat.
What echo findings support HCM? (explain what it is) tell me the wall thickness number, and explain the absence of diseases that mat cause…..in what view
Echo may show a non-dilated LV with LVH in the absence of cardiac or systemic diseases that may cause LVH, with wall thickness greater than 15 mm or 1.5cm in PLAX
Why is CMR used in HCM assessment? (Cardiac Magnetic Resonance imaging)
CMR is used to rule out infiltrative diseases.
(differential)
CMR = Cardiac Magnetic Resonance imaging.
It is basically an MRI of the heart.
In your HCM slide, CMR is listed under assessment because it can help rule out infiltrative diseases—meaning it helps make sure the thick heart muscle is really from HCM and not another disease causing the heart muscle to look thick.
Simple way to remember:
Echo = main test to diagnose/monitor HCM
CMR = heart MRI used when we need a more detailed look or to rule out other causes of thick myocardium.
List the 6 signs/symptoms of HCM
Chest pain
Syncope
Dyspnea
Fatigue
Arrhythmias, including PVCs and atrial fibrillation
Sudden cardiac death — #1 cause in young patients****
List the 8 physical, auscultation, EKG, or heart failure findings
Systolic apical impulse
Systolic ejection murmur
Prominent jugular venous A wave
EKG: high-voltage QRS
LVH
Prominent Q waves in inferior and lateral leads
Inverted T waves
Diastolic heart failure
Simple reminder:
HCM can show up with symptoms like chest pain, syncope, dyspnea, fatigue, arrhythmias, and sudden cardiac death. On exam/EKG, think systolic murmur, high-voltage QRS, LVH, Q waves, inverted T waves, and diastolic heart failure.
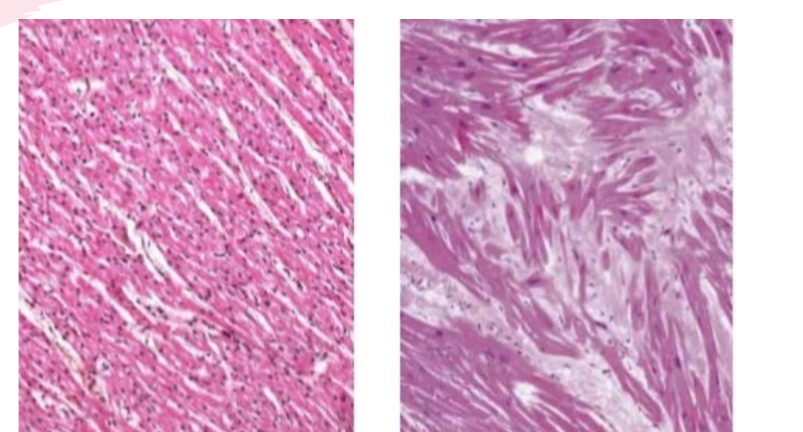
What is being compared on the histology slide? explain what histology is? - its how the what are structure? how HCM is orgainzed in the myocardium and list two things it can affect?
The slide compares normal myocardium with myocardium in HCM.
(histology is how the tissues are structure in HCM, in a normal heart the myocardium will have a uniform structure, myocardium in HCM will have myocardial Disarray, so this is a strucal abnormaility in the myocardium, in HCM the tissue is going to be disorganized can affect how the muscle function and cause electerical issues)
The HCM myocardium appears abnormal/disorganized compared with normal myocardium.
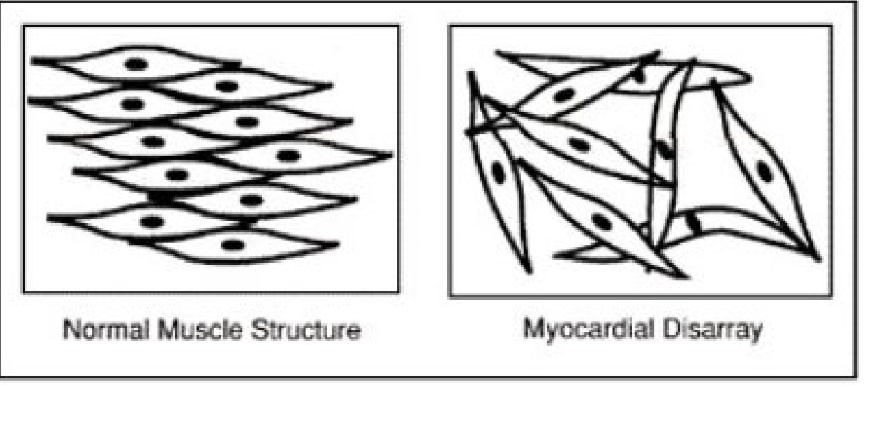
Compare normal muscle structure to myocardial disarray.
Normal muscle structure is organized and lined up. In myocardial disarray, the muscle fibers are disorganized.
Simple reminder:
HCM = thickened myocardium + disorganized muscle fibers.
List the 4 key features of HCM
describe the LV
what disorder is this
describe the myocardium and relaxation
describe the filling pressure with _______ dysfunction
Non-dilated LV
Genetic disorder
Thickened, stiff myocardium with impaired ventricular relaxation
High diastolic filling pressures with diastolic dysfunction
Simple reminder:
The LV is thick and stiff, so it does not relax well during diastole.
What is the modality of choice for screening, diagnosis, and monitoring of HCM?
Echo is the modality of choice.
describe the apparence of the hypertrophy and the with wall thickness ratio of what is strongly associated with HCM
Asymmetric septal hypertrophy with a wall thickness ratio
of 1.3 cm or greater is strongly associated with HCM.
________________________________________________________________
Asymmetric septal hypertrophy ratio ≥ 1.3
This is not just asking how thick one wall is. It is comparing two walls.
Usually it compares:
Septal wall thickness ÷ posterior wall thickness
So this is asking:
“Is the septum much thicker than the other LV wall?”
Example:
Septum = 1.6 cm
Posterior wall = 1.0 cm
Ratio = 1.6 ÷ 1.0 = 1.6
That is greater than 1.3, so it means the septum is disproportionately thick, which is called asymmetric septal hypertrophy.
Simple difference
Wall thickness ≥ 1.5 cm = the wall is thick enough to suggest HCM.
Ratio ≥ 1.3 = the septum is thicker compared to the other wall, which suggests the thickening is asymmetric.
A simple card sentence:
Max wall thickness ≥ 1.5 cm tells us the LV wall is abnormally thick. A septal/posterior wall ratio ≥ 1.3 tells us the septum is thicker than the posterior wall, which supports asymmetric septal hypertrophy seen in HCM.
What maximum wall thickness supports HCM, and what range is borderline?
A maximum wall thickness of 1.5 cm or greater supports HCM.
A wall thickness of 1.3–1.4 cm is borderline diagnosis
What ___% of HCM patients have what obstruction, and what gradient is typical?
About 30% of patients with HCM have a resting LVOT obstruction, typically 30 mmHg or greater.
High-yield numbers:
HCM max wall thickness: ≥1.5 cm
Borderline: 1.3–1.4 cm
Resting LVOT obstruction: 30% of patients
LVOT gradient: ≥30 mmHg
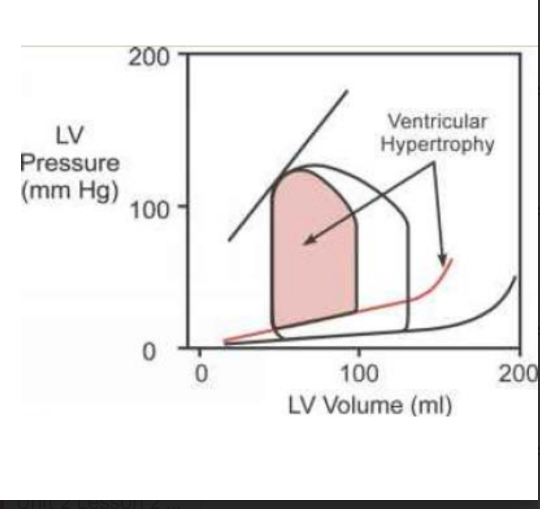
Explain why HCM causes diastolic heart failure.
In HCM, at any diastolic volume, the ventricular pressure is greater than normal because the ventricle is thick and stiff.
What happens to EDV in HCM?
EDV decreases.
Simple reminder:
The LV is stiff, so it fills with less blood / reduce filling and pressure rises faster
List the 2 main types of HCM.
Answer:
Non-obstructive HCM (thickened walls no affects on hemodynamics)
Obstructive HCM, or HOCM (LVOT obstruction)
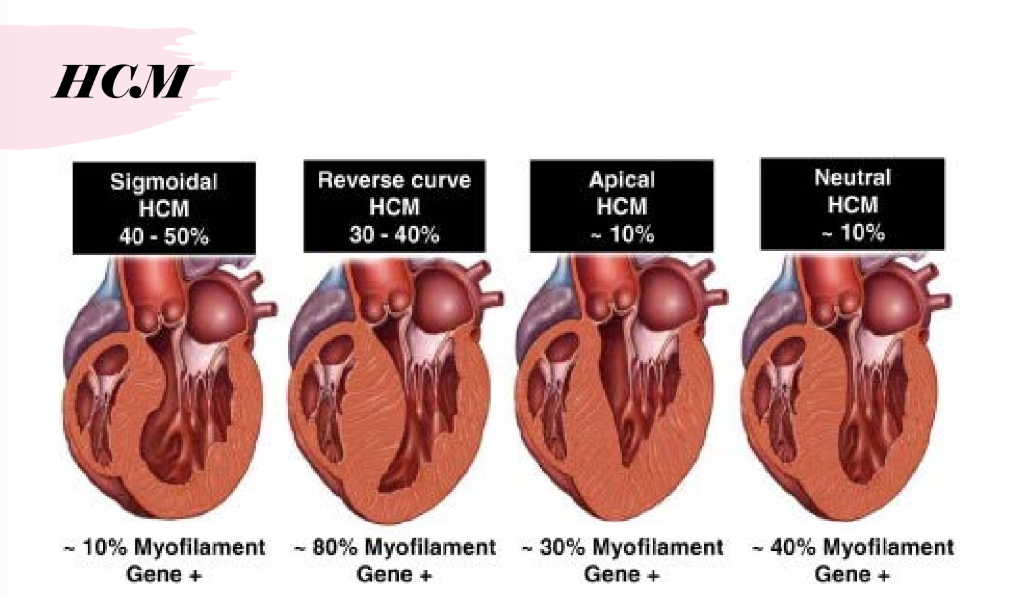
List the 4 ventricular septum/pattern types (this tells us the shape and direction of the ventricular septum??))) and list another HOCM
Reverse curvature
Sigmoid
Neutral
Apical
Mid-ventricular (kissing walls)