Echo - Test 4
1/36
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
37 Terms
bacterial causes of infective endocarditis
staphylococci
streptococci
enterococci
fungal causes of infective endocarditis
candida (most common)
asperigillus
histoplasma
risk factors for infective endocarditis
pts who have undergone cardiac surgery
pts with AV disease, MR, PDA, VSD, coarctation of the aorta, Marfan’s syndrome
pts with prosthetic valves
pts receiving IV drug therapy
IV drug abusers
pts with staph infections
pts with atherosclerotic changes
hemodialysis pts
symptoms of endocarditis
fever, chills, night sweats
new or changed murmur
fatigue, aching joints and muscles
SOB, persistent cough
swelling in feet, legs, abdomen
unexplained weight loss
frank or microscopic hematuria
painful spleen
osler’s nodes
petechiae
sepsis
osler’s nodes
red, tender spots on fingers
petechiae
purple or red spots on skin, whites of eyes, inside mouth
sonographic appearance of endocarditis
valvular vegetation: oscillating mass with independent motion
valvular regurgitation
chamber dilation
paravalvular abscesses
pericardial effusion
causes of non-infective endocarditis
trauma (may be due to a catheter passing through the right heart, may injure TV or PV)
systemic lupus erythematous
other hypercoagulative states
mucin-producing metastatic carcinomas
indications for FoCUS (focused cardiac ultrasound)
chest pain
hypotension
dyspnea
chest trauma
cardiac arrest
contrast echo brands
definity
optison
lumason
suboptimal image for contrast echo
at least 2 out of 6 myocardial segments of the left ventricle cannot be visualized in the apical views
contraindications for contrast echo
lumason: allergy to sulfur hemafluoride
definity: allergy to perflutren
optison: allergy to perflutren/blood products
contrast echo optimization - mechanical index
indicator of cavitation
a low value of < 0.3 will produce nonlinear acoustic signals, so we utilize harmonic imaging
higher valve: microbubble oscillation causes microbubble destruction (inertial caviation)
contrast echo optimization - focal zone
placement at the mitral valve level allows for optimal visualization of entire left ventricle and minimizes microsphere disruption
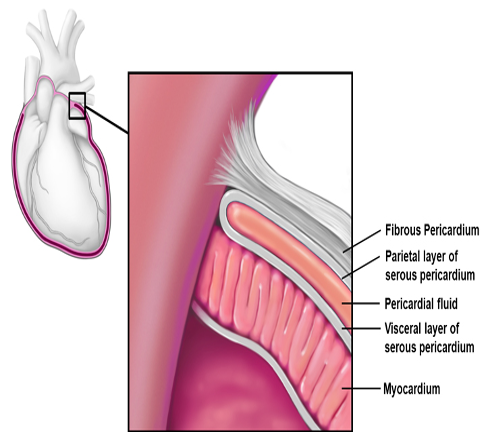
pericardium
double-layered, thin sac around the heart
fibrous pericardium
outer layer that is contiguous with the adventitia of the great vessels
serous pericardium
inner portion of the pericardium that is double-layered
visceral (epicardium) - inner
parietal - outer
between these 2 layers lies the pericardial cavity which normally contains a small amount of serous fluid
layers of pericardium
function of the pericardium
fix cardial position anatomically
prevent exvcess movement
reduce friction between heart and surrounding organs
acts as a barrier to infection, or malignancy from surrounding organs
criteria for pericarditis diagnosis
pericardial chest pain
pericardial friction rub (scratchy sound on auscultation)
EKG features
widespread ST elevation
diffuse PR depression
diffuse T wave inverison
normalization
new or increasing pericardial effusion
pericardial effusion
abnormal accumulation of pericardial fluid
may be diffuse or loculated
leads to an increased intrapericardial pressure which can negatively affect heart function
echo evaluation for pericardial disease
ventricular interdependence (dysfunction of one ventricle secondary to a disorder of the other)
MV & TV PW inflow respiratory variation
annulus versus (medial > lateral mitral annular tissue doppler velocities)
expiratory hepatic venous diastolic flow reversal
cardiac tamponade
hemodynamic compromise (hypotension and/or decreased cardiac output) due to compression of the cardiac chambers by fluid in the pericardial space
acute cardiac tamponade
rapid accumulation of fluid
abrupt bleeding
leads to cardiogenic shock
causes of acute cardiac tamponade
penetrating chest wounds
cardiac contusion
invasive procedures
myocardial rupture s/p MI
ruptured proximal aortic dissection
subacute cardiac tamponade
develops gradually
stretching of pericardium can allow for large accumulation of fluid (> 1000 mL)
echo findings of tamponade
pericardial effusion
chamber collapse
IVC plethora (dilated and does not collapse)
hepatic venous flow pattern change
respiratory variation of TV and MV PW inflow patterns
swinging heart
pericardial vs pleural effusion
pericardial = fluid between heart and aorta
pleural = fluid behind aorta
restrictive cardiomyopathy
a non-compliant LV associated with elevated diastolic pressures; systolic function usually preserved with impaired diastolic function
least common type of CM
restrictive
signs and symptoms of restrictive CM
peripheral edema
ascites
atrial arrhythmia
bi-atrial enlargement
MR/TR
dyspnea
palpitations
fatigue
poor exercise tolerance
anorexia
2D echo of restrictive CM
LVH with bright, shiny echogenic appearance
RV free wall thickening
apical obliteration
normal systolic function with impaired diastolic function
biatrial enlargement
pericardial effusion often present
doppler echo of restrictive CM
MR/TR often moderate to severe
pulmonary HTN often present with elevated RA pressure
LVOT gradient may be present
diastolic dysfunction
infiltrative CM
form of RCM
hereditary or acquired
abnormal substances are deposited in the myocardium causing LV stiffening » impedes normal diastolic filling
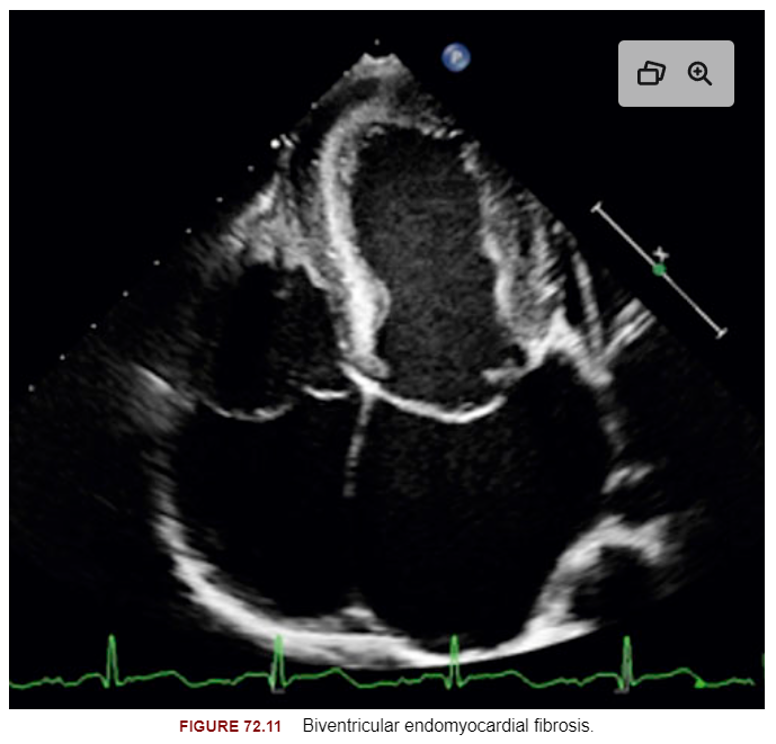
endomyocardial fibrosis (EMF)
RCM
dense scarring of the mural endocardium
fibrosis predominated at the apieces and moved up toward the inflow tract
Rt side key EMF echo features
severe RV diastolic dysfunction
severe TR
high RA pressure
systolic reversal in hepatic veins
Lt side key EMF echo features
increased apical echogenicity
posterior MV leaflet is often tethered down or plastered to the LV posterior wall
echogenic papillary muscles
apical obliteration in advanced cases
LA enlargement
prethrombotic smoke or thrombus