MLS Exam #2 (M)
1/381
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
382 Terms
In general, what is an electrocardiogram (ECG)?
A recording of the electrical activity of the heart
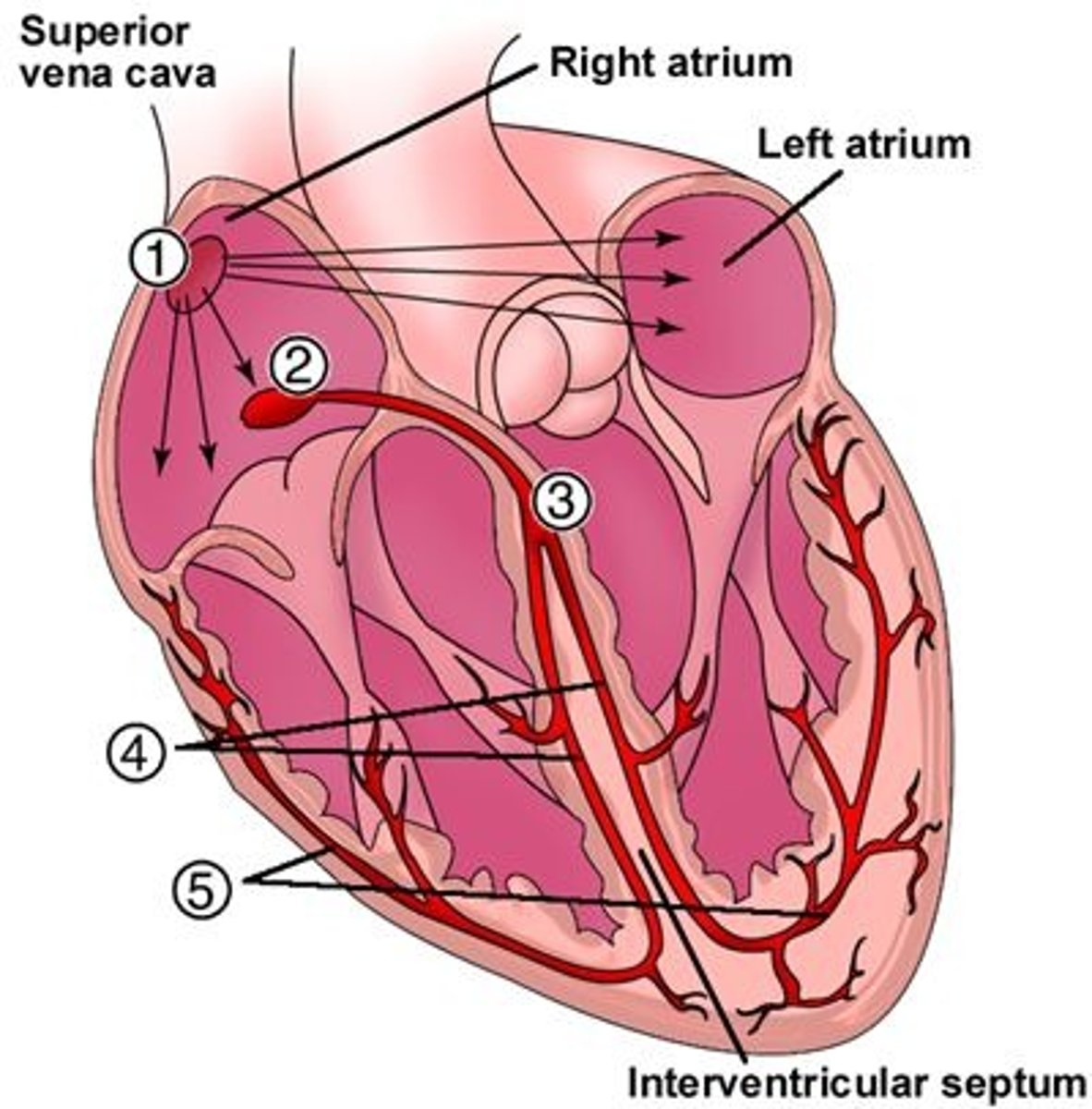
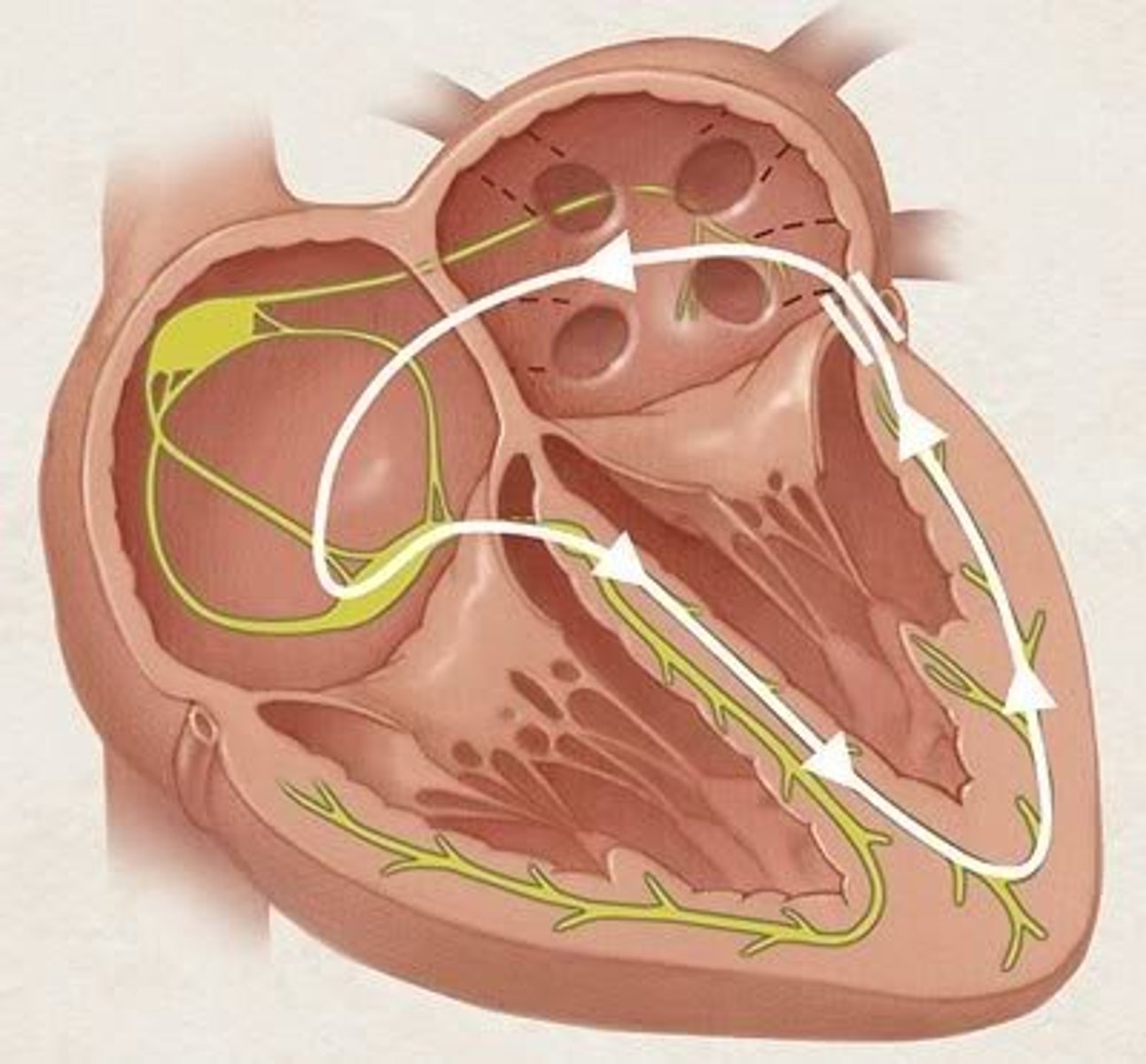
Where is the SA node located, & what is its function?
Right atrium (1); signals the atria to contract ("pacemaker")
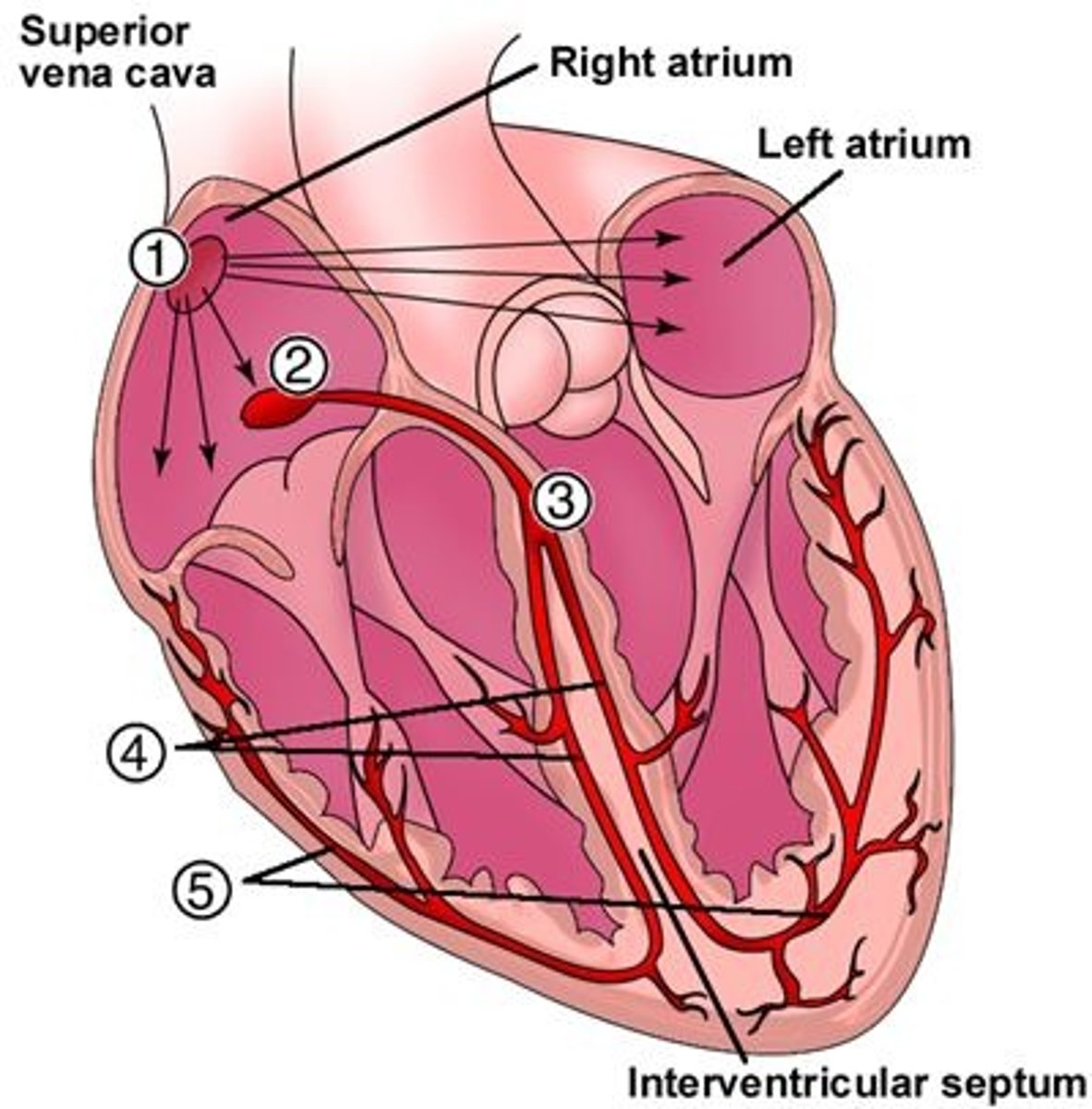
Where is the AV node located, & what is its function?
Between the atria & ventricles (2); conducts electrical signal from the AV valves to the ventricles
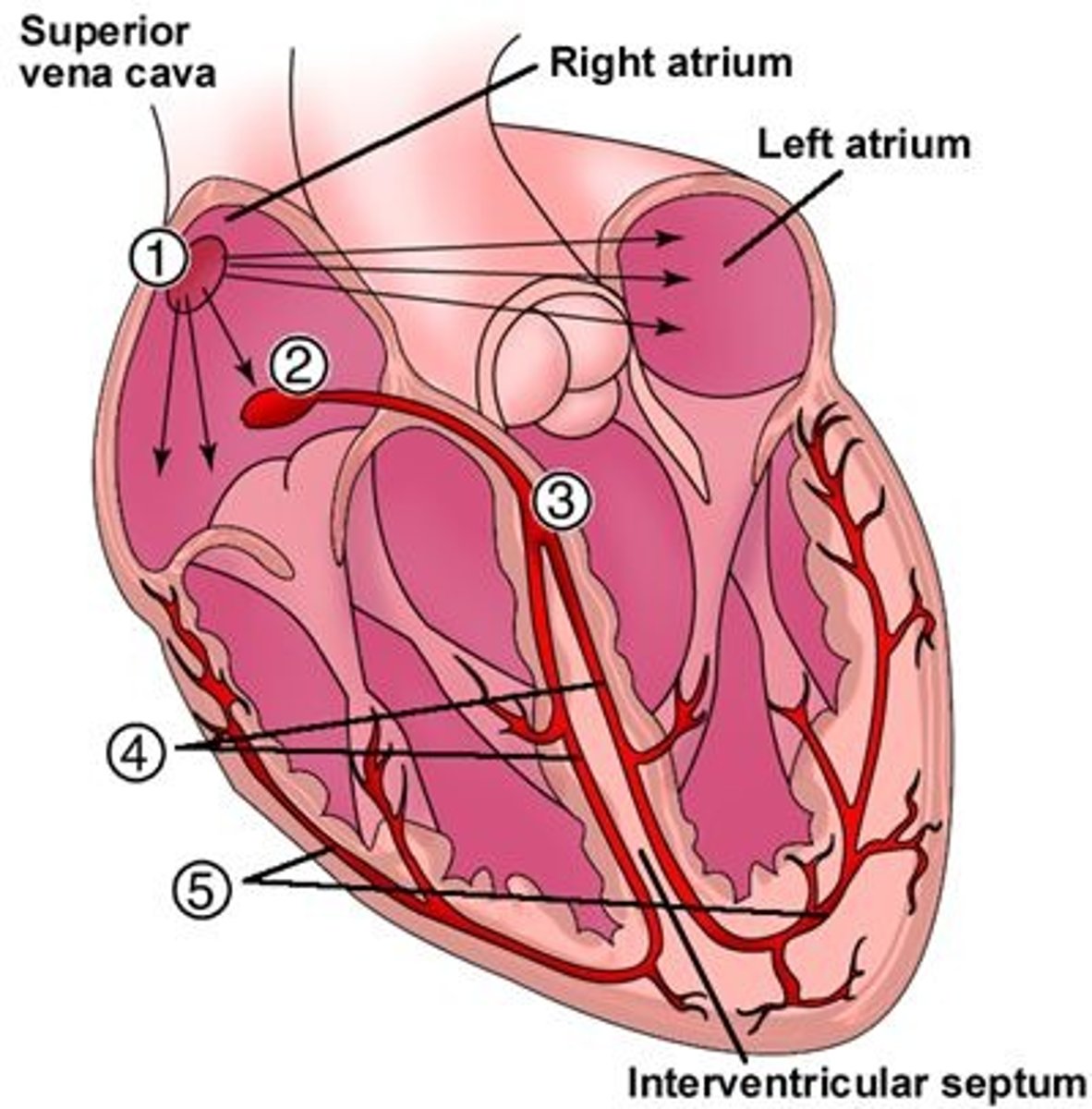
Where is the Bundle of His located, & what is its function?
In the intraventricular septum (3); carries conduction to the right & left bundle branches
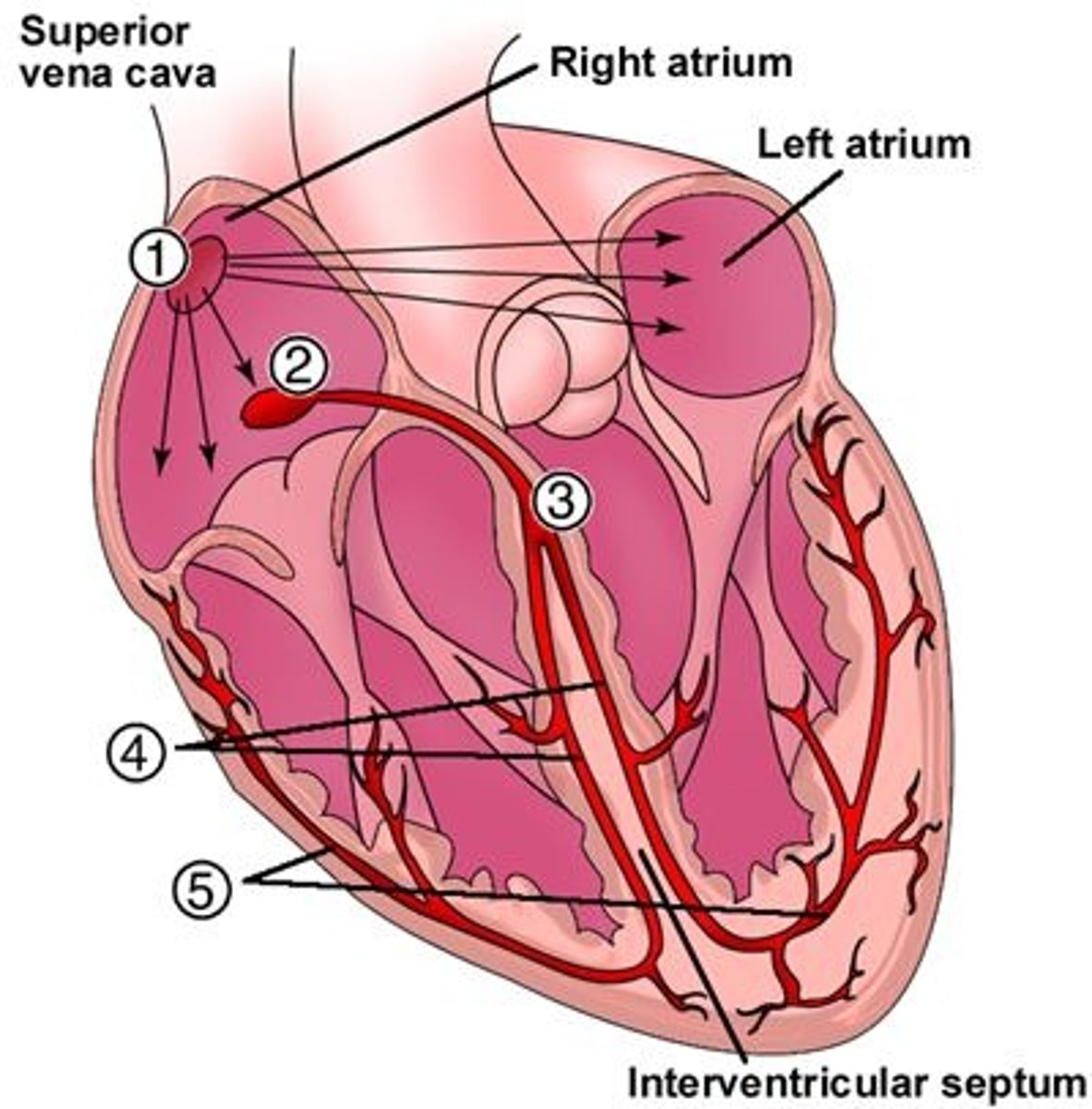
Where are the left & right bundle branches located, & what is their function?
In the intraventricular septum (4); carries conduction to the Purkinje fibers
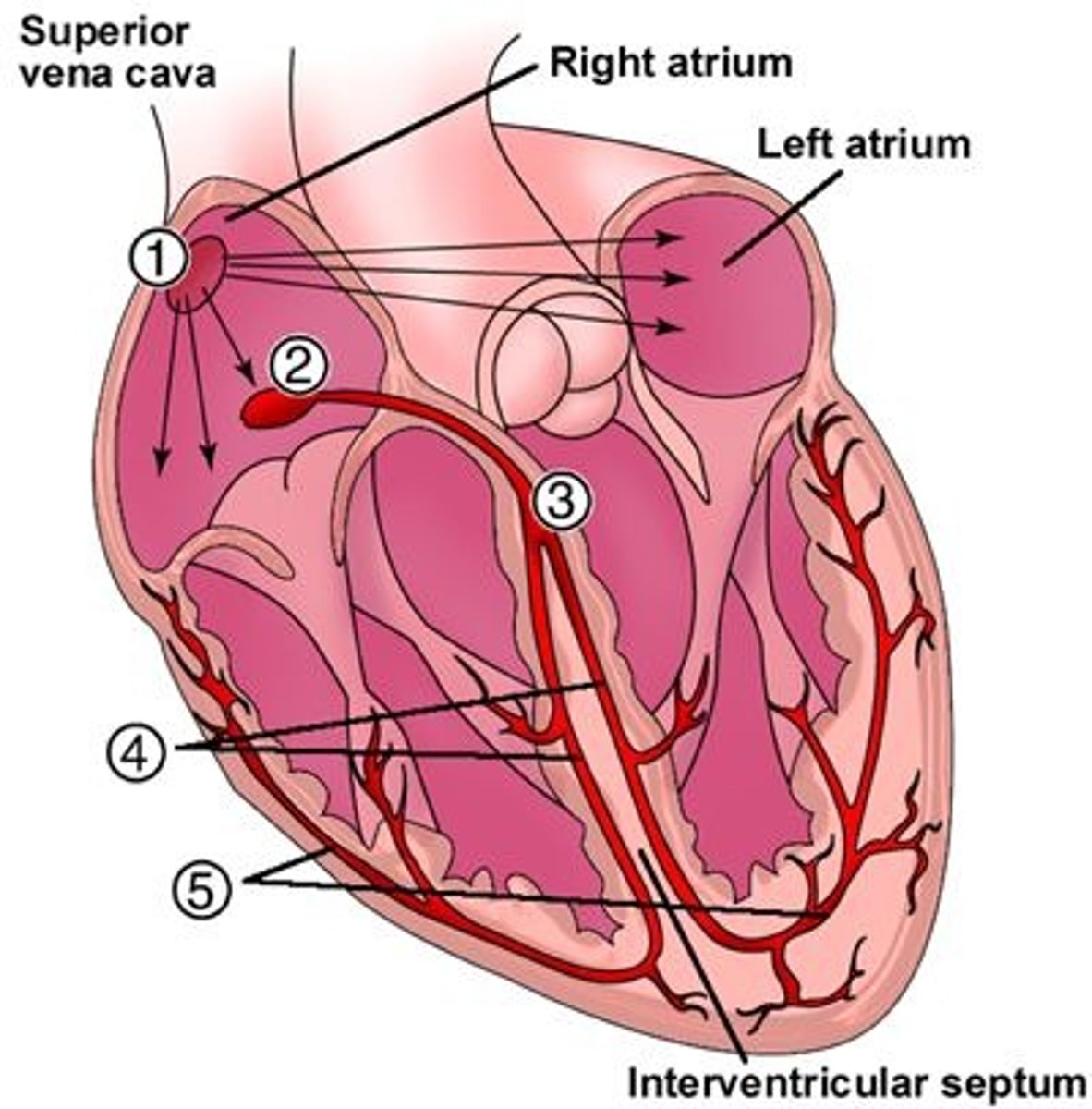
Where are the Purkinje fibers located, & what is their function?
Throughout the myocardium (5); signal ventricles to contract
What state (positively-charged or negatively-charged) do myocytes (heart muscle cells) exist in at rest? What is meant by "depolarization?"
Negatively-charged (polarized); depolarization = becoming positively-charged = contraction
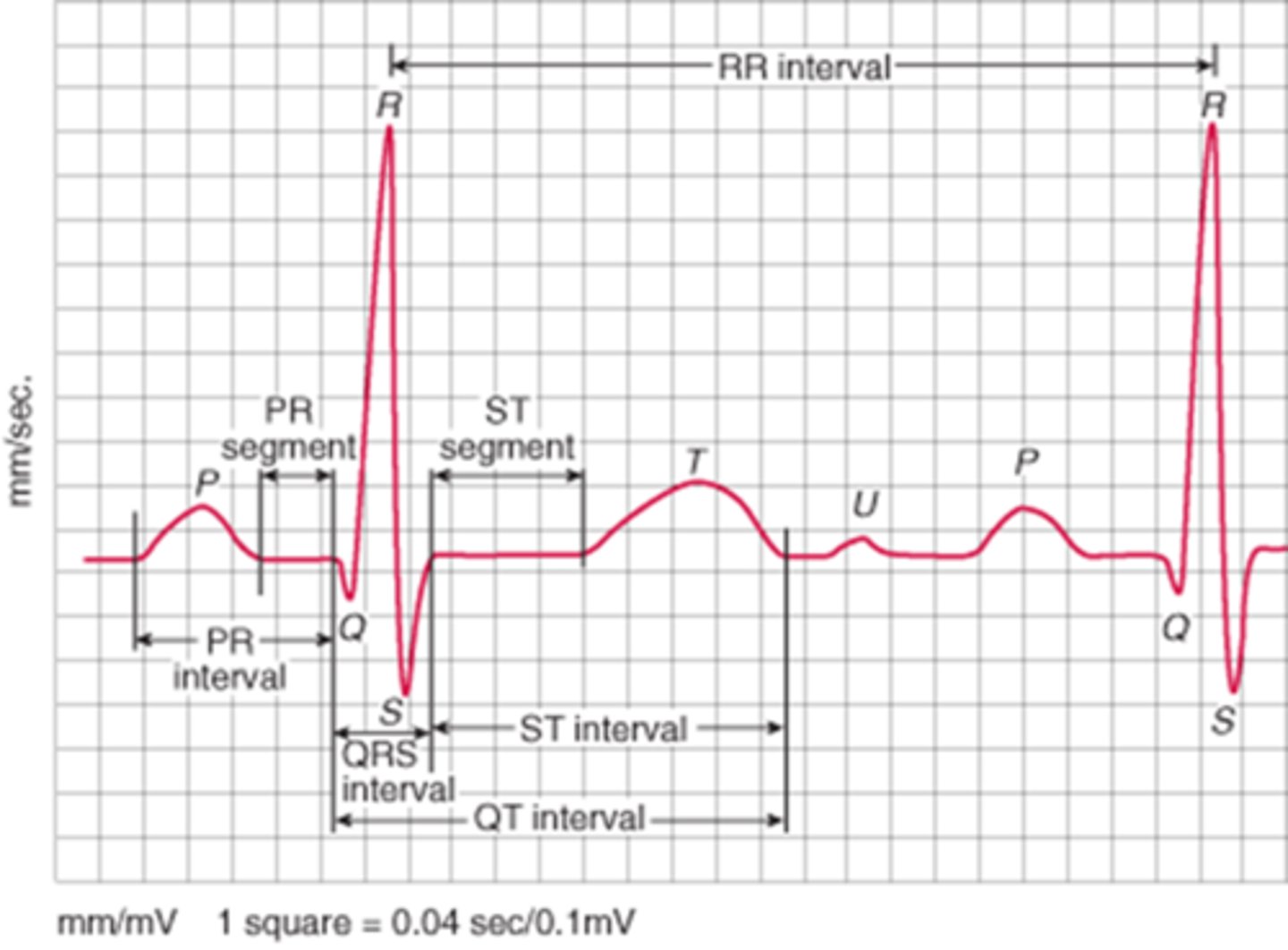
What does the p wave represent?
Atrial depolarization (contraction)

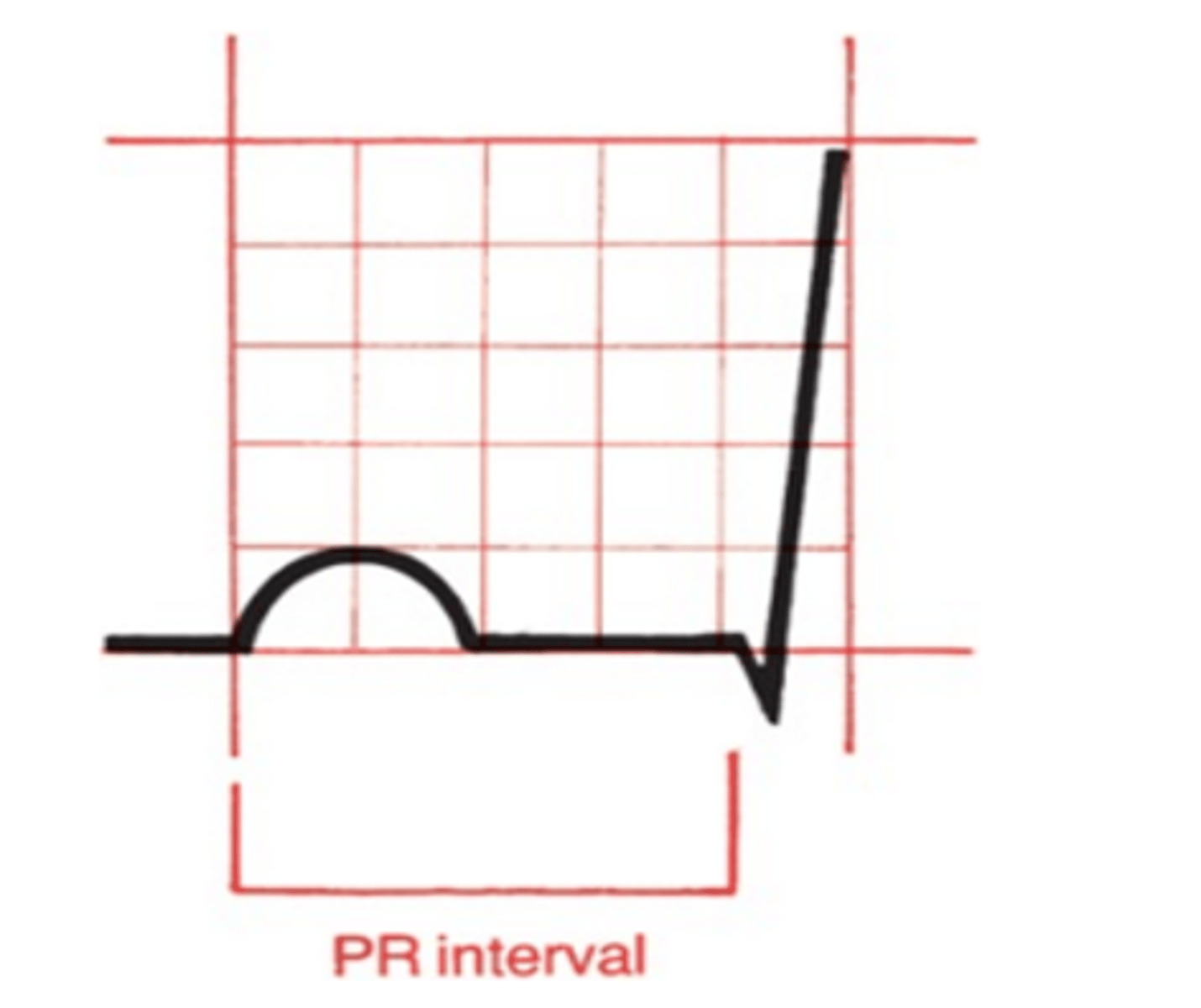
What does the PR interval represent? What is a normal # of seconds/boxes for this interval?
Ventricular filling due to pause at AV node
Normal: 0.12-0.2 seconds (3-5 small boxes)
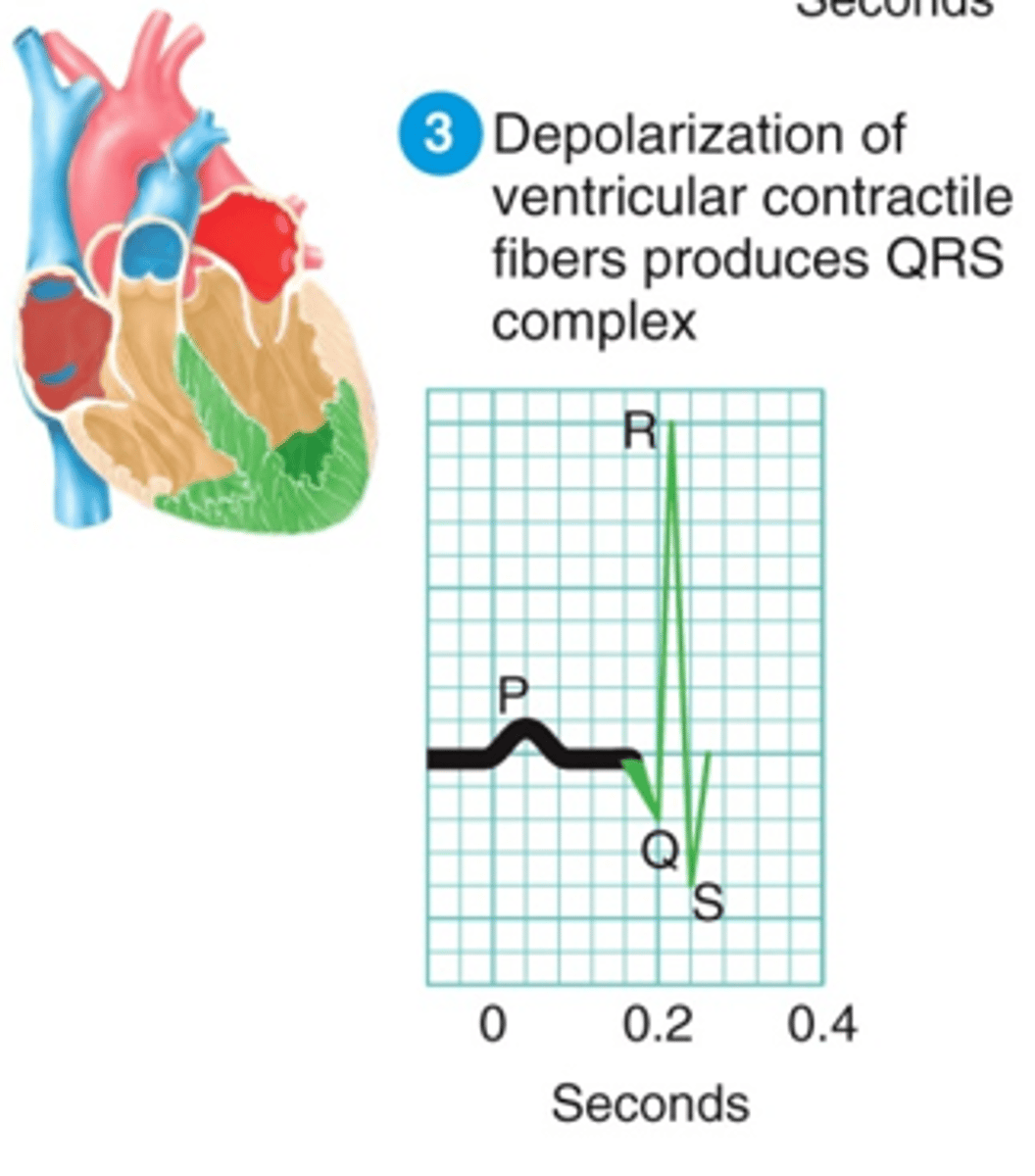
What does the QRS complex represent? What is a normal # of seconds/boxes for this interval?
Ventricular depolarization (contraction)
Normal: 0.04-0.12 seconds (1-3 small boxes)
What does the ST segment represent? How should this segment normally appear?
Beginning of ventricular repolarization (relaxation); should be isoelectric
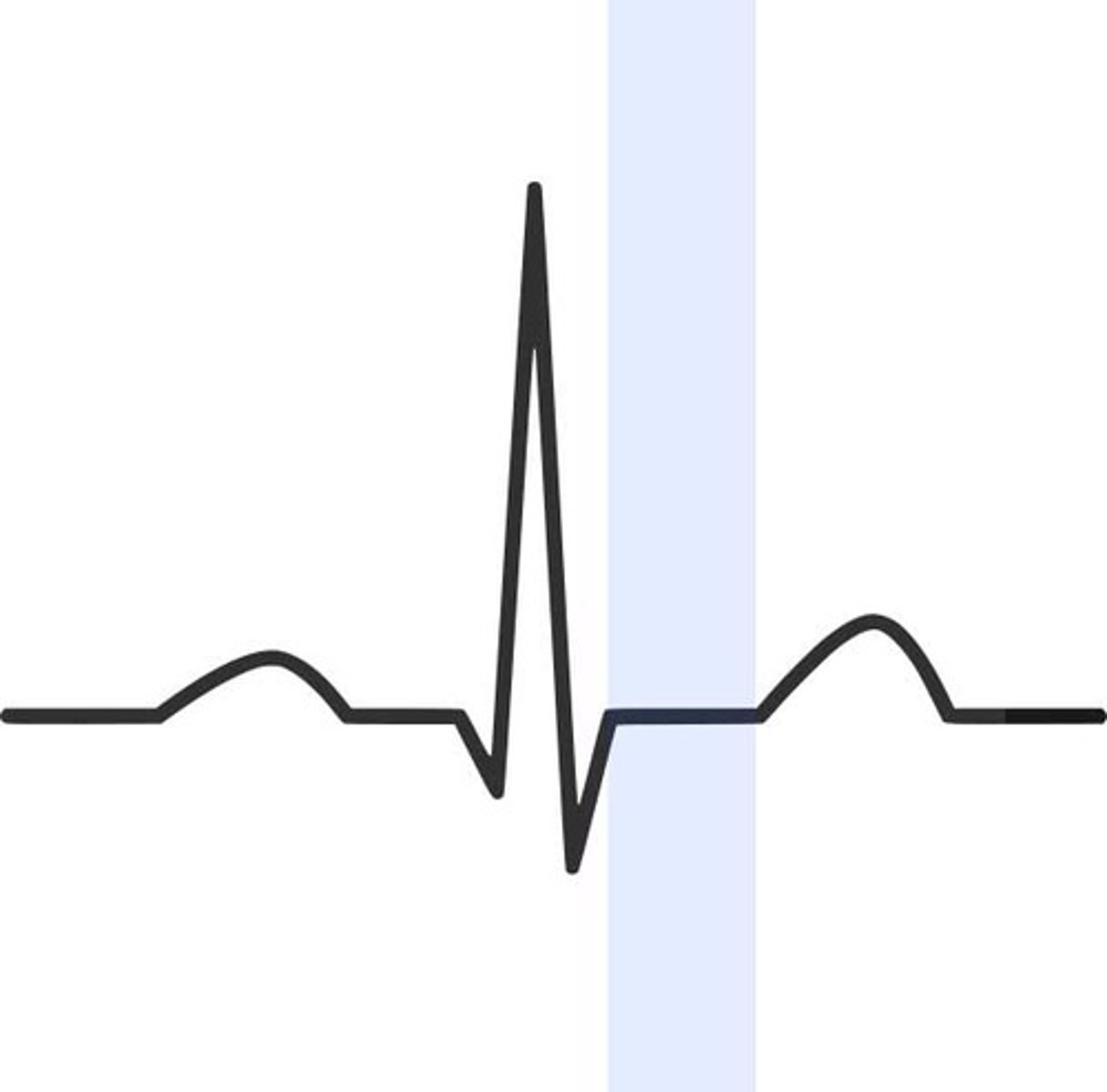
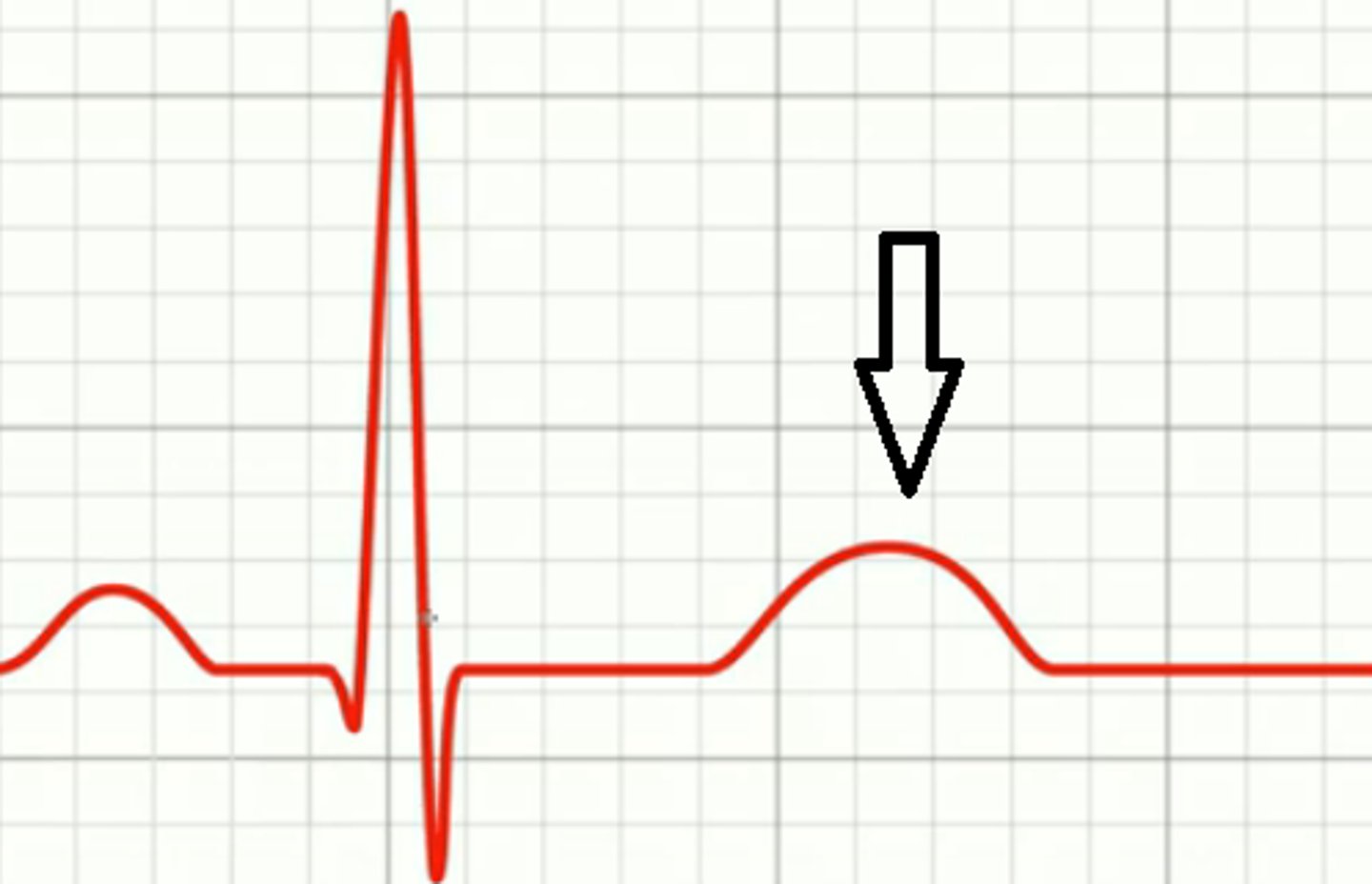
What does the T wave represent?
Ventricular repolarization (relaxation)
What does the QT interval represent? What is a normal duration for this?
Duration of ventricular systole (time it takes ventricles to depolarize & repolarize); should be ~1/2 the R-R interval

What is the R-R interval, & what is it used for?
Distance from one R wave to another; used to calculate rate
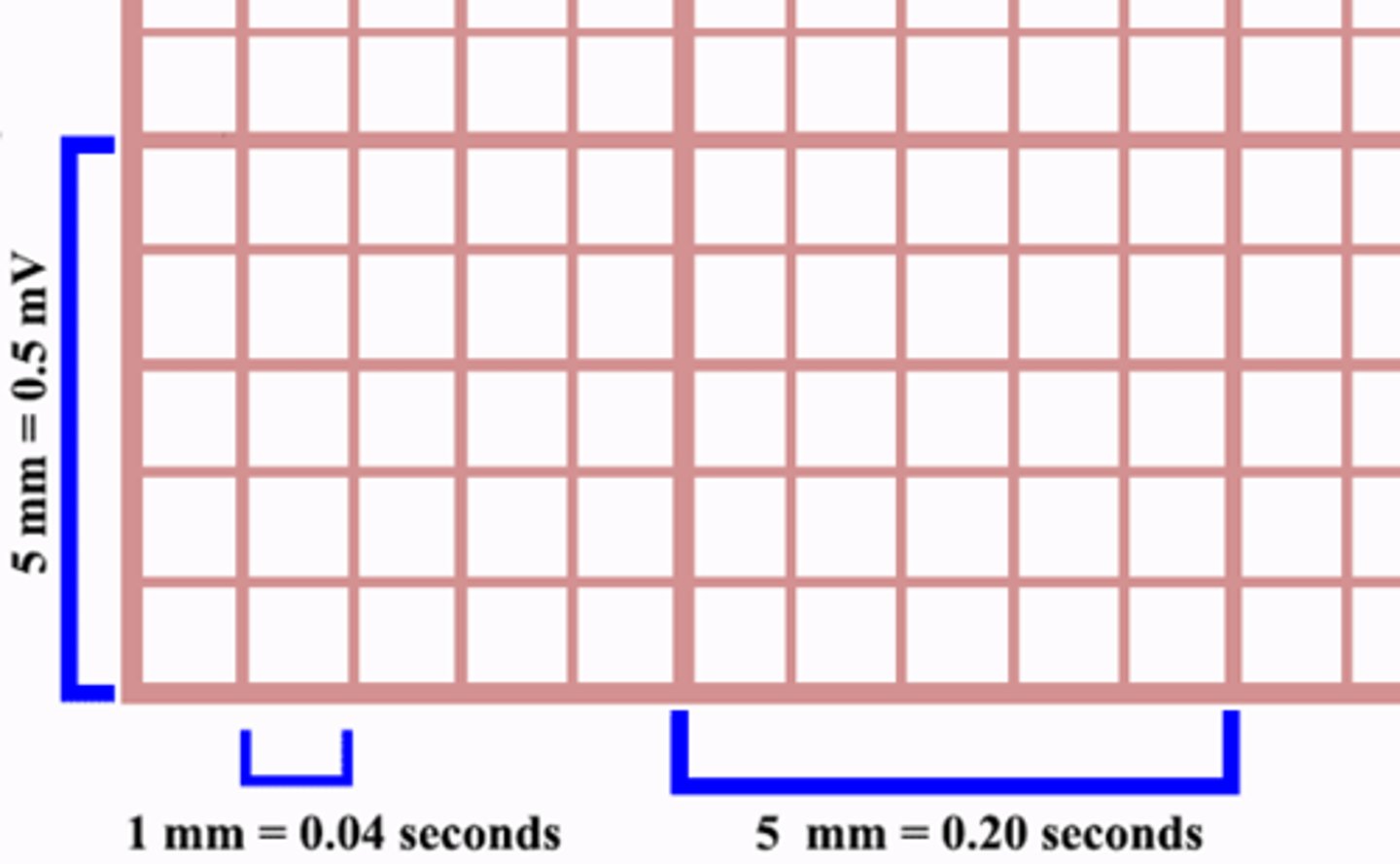
How much time do ECG small boxes & large boxes represent, respectively?
Small: 0.04 seconds
Large: 0.2 seconds
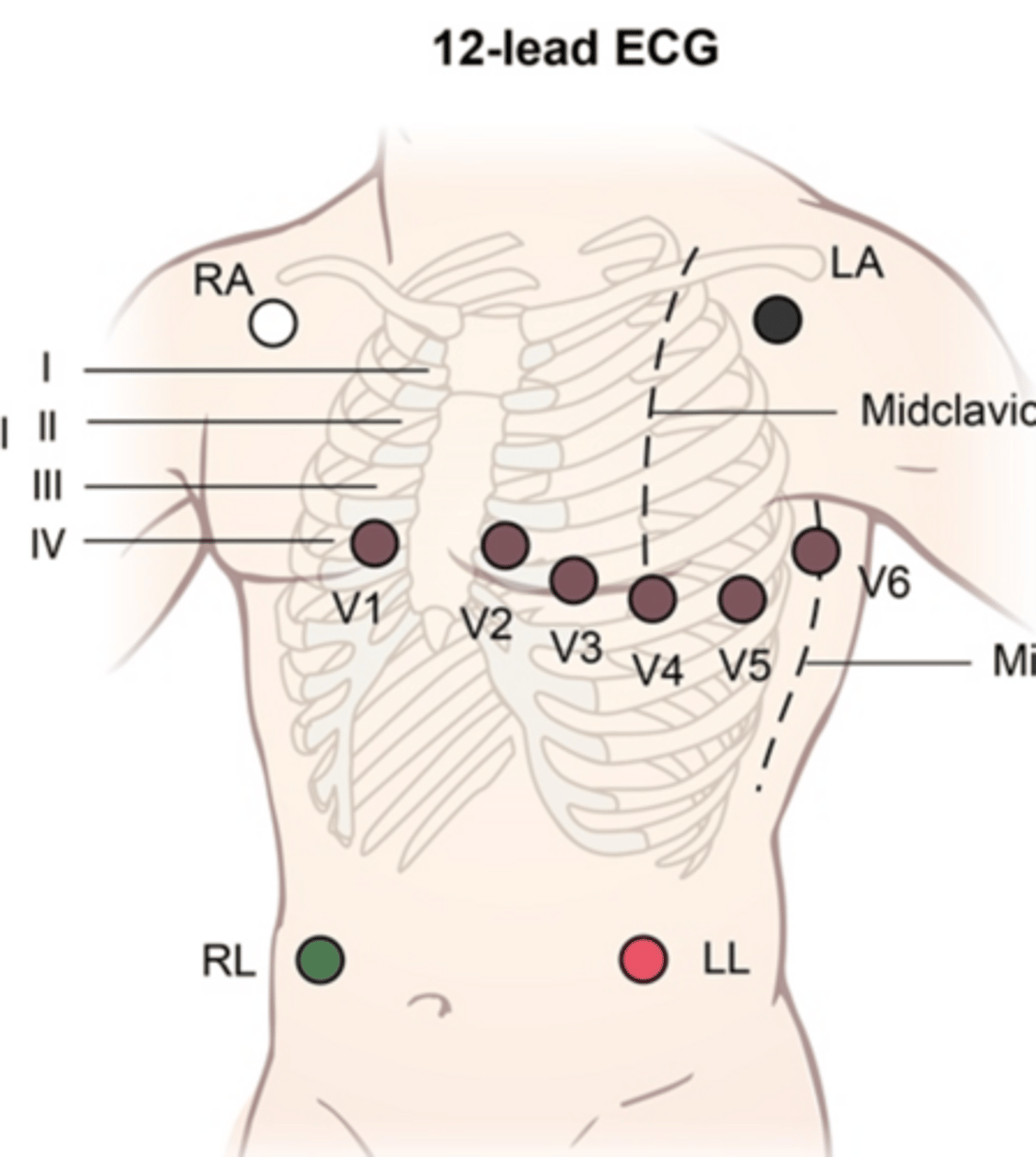
JUST KNOW: ECG leads and electrodes are NOT THE SAME THING! Electrodes are the physical stickers that detect the heart's electrical activity conducted to the skin, while leads are the views of the heart an ECG machine produces from these signals. This is why in a 12-lead ECG, there are only 10 physical electrodes. Some leads are bipolar meaning they look at information from both a positive & negative electrode, while others are unipolar & only use information from a single positive electrode
JUST KNOW: If the electrical signal travels towards a positive electrode, it will produce an upward waveform on ECG. If the signal travels towards a negative electrode (or away from a positive one), it will produce a downward waveform on ECG. This is why the waveforms appear different depending on which lead you're examining - it all depends on which direction the electrical signal is going in respect to which view the lead provides
On a 12 lead ECG, which leads are considered "limb leads" and which are considered "precordial leads?"
Limb: I, II, III, aVR, aVL, aVF
Precordial: V1-V6
Which limb leads are bipolar & which ones are unipolar?
Bipolar: I, II, III
Unipolar: aVR, aVL, aVF
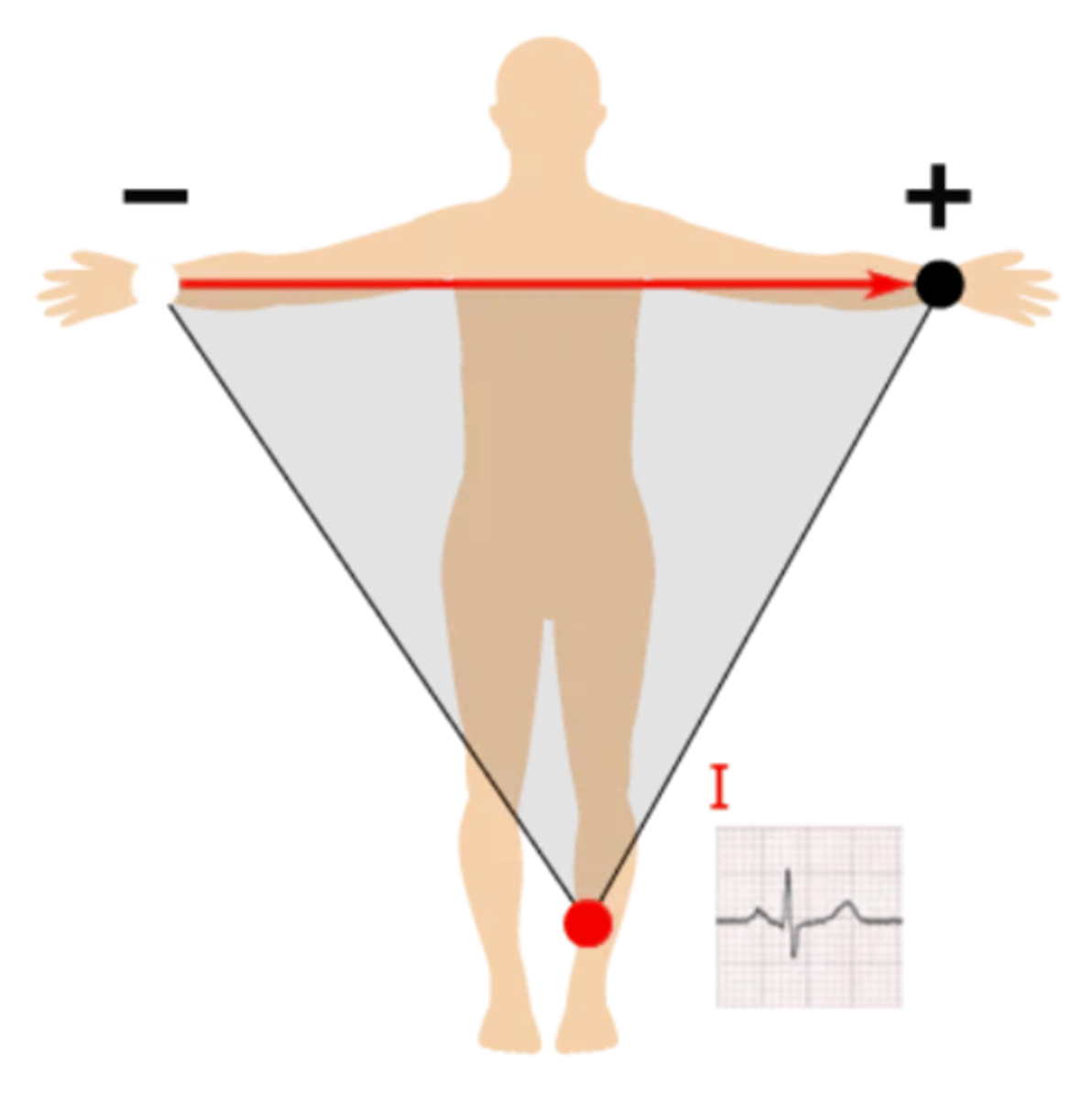
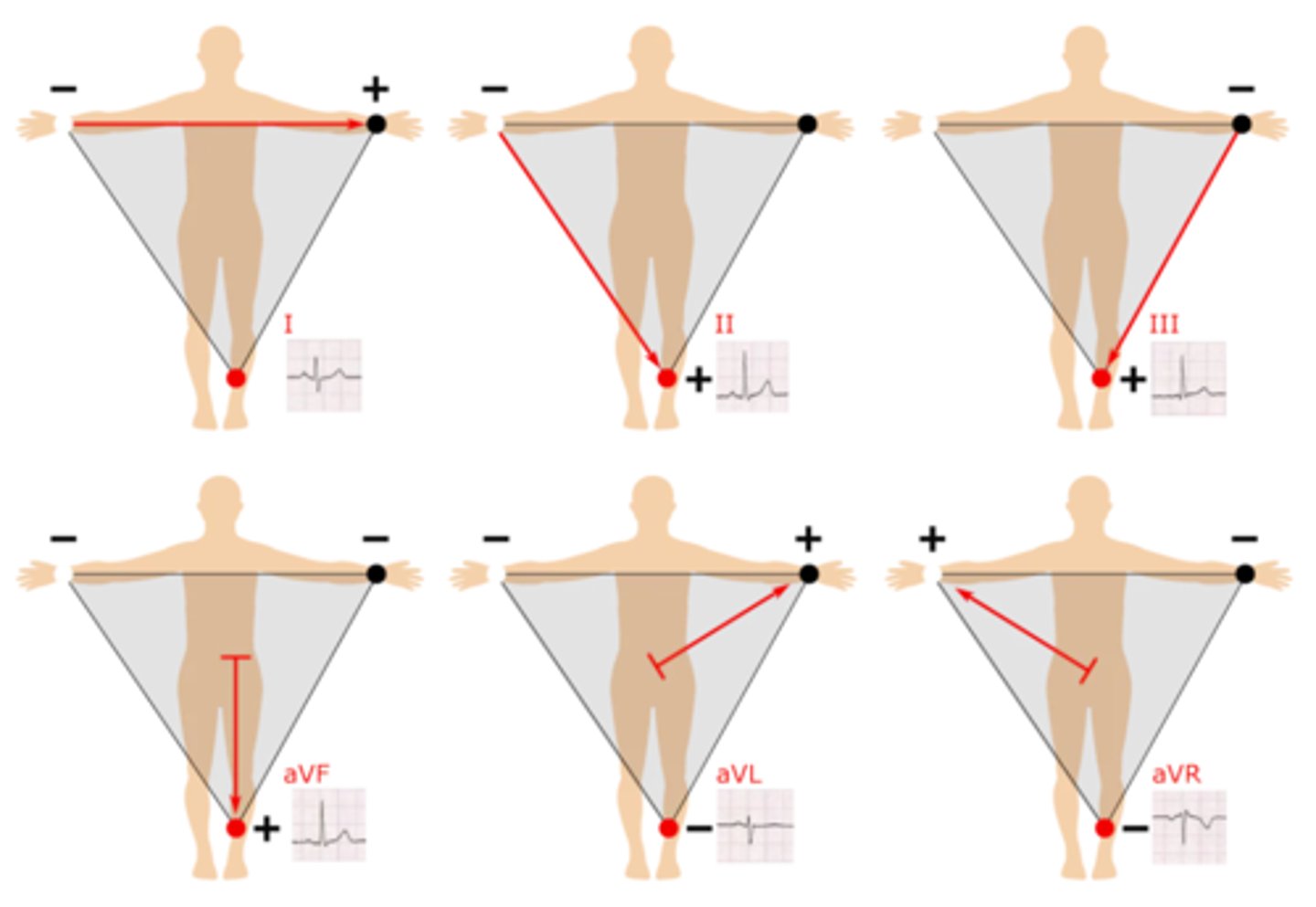
How is lead 1 created?
Right arm --> left arm; produces a positive waveform as heart's electrical activity naturally moves down & to the left
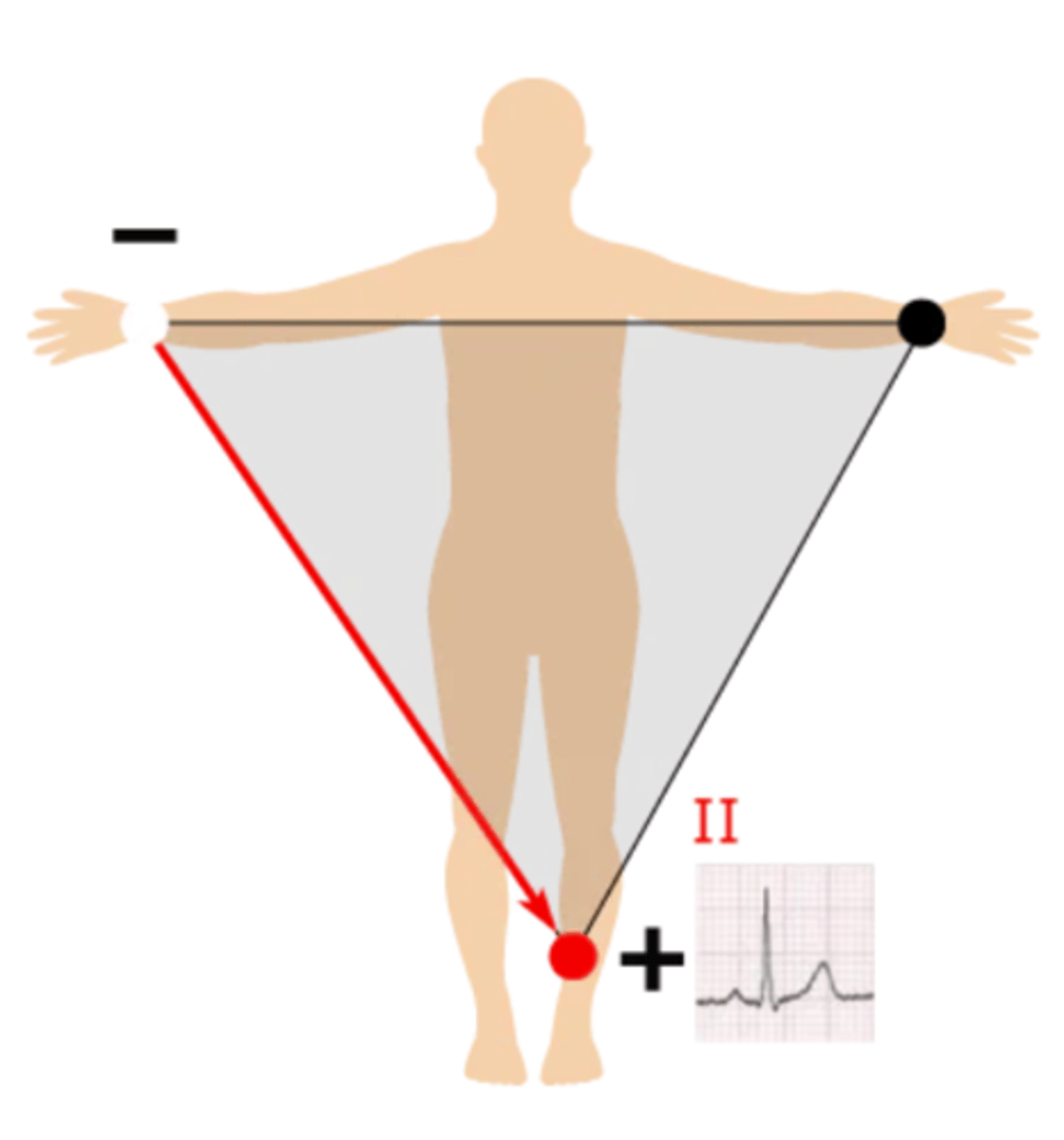
How is lead 2 created?
Right arm --> left leg; produces a positive waveform as heart's electrical activity naturally moves down & to the left
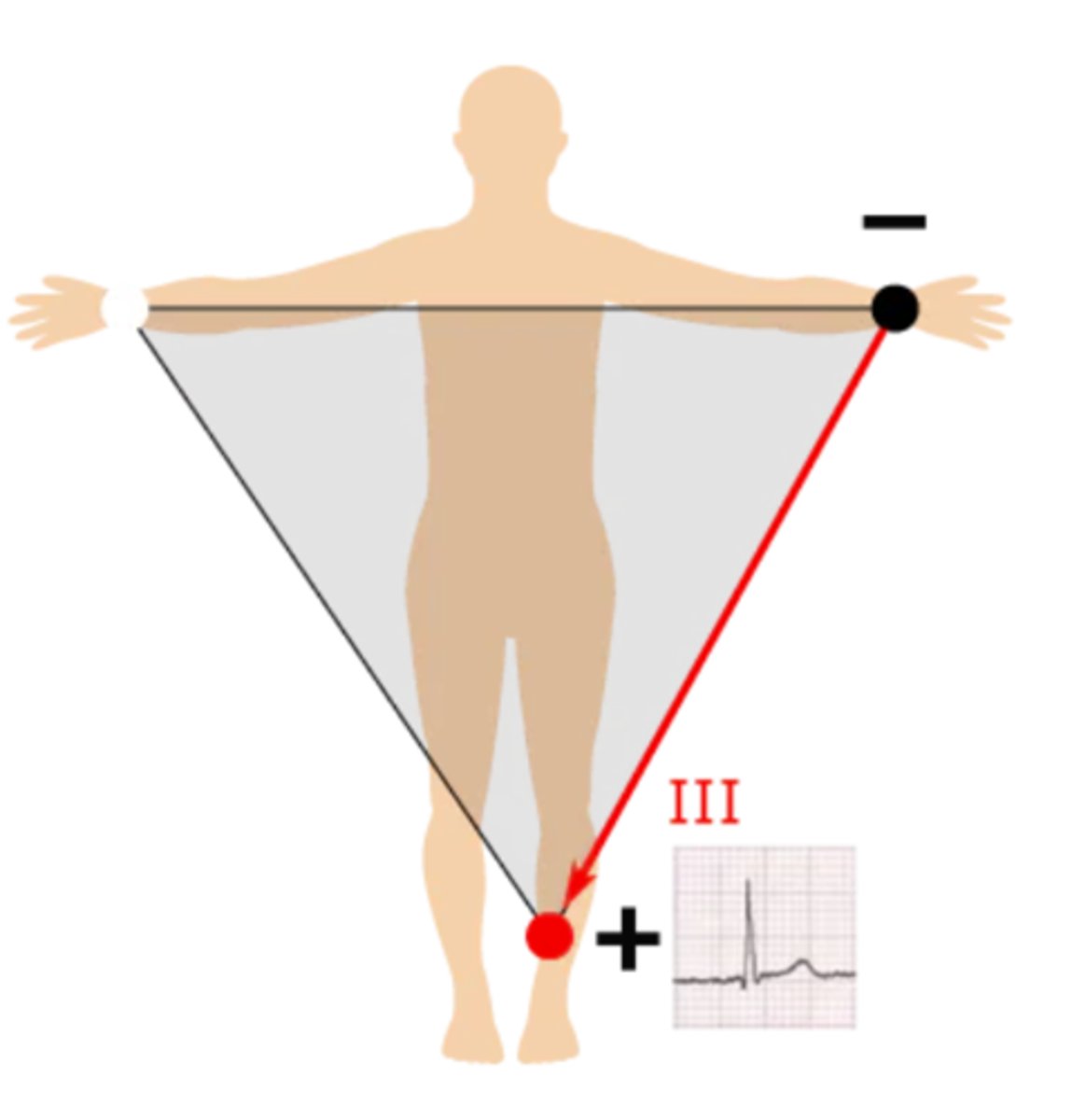
How is lead 3 created?
Left arm --> left leg; produces a positive waveform as heart's electrical activity naturally moves down & to the left
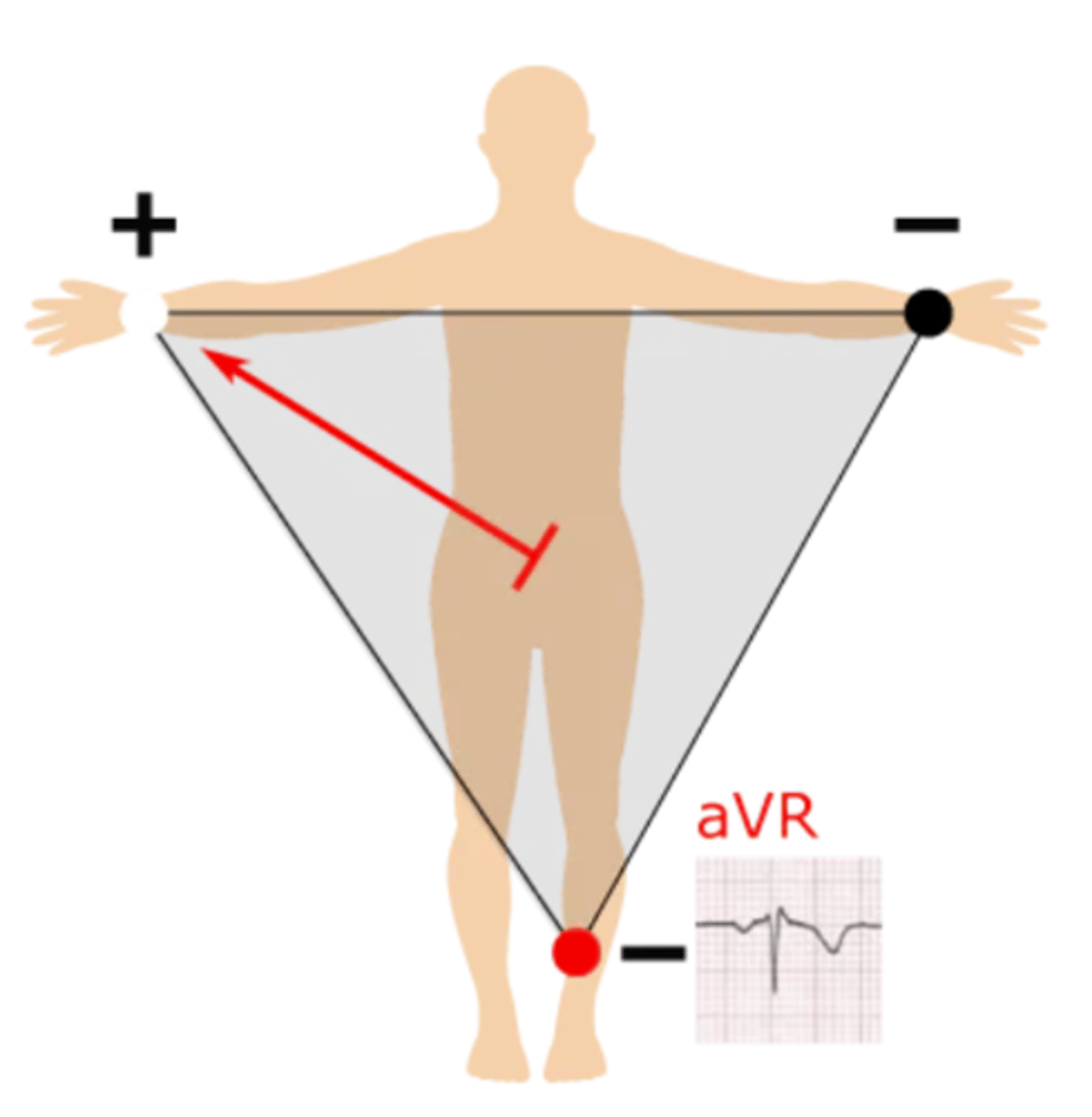
How is lead aVR created?
Left half --> right arm; produces a negative waveform as heart's electrical activity naturally moves down & to the left
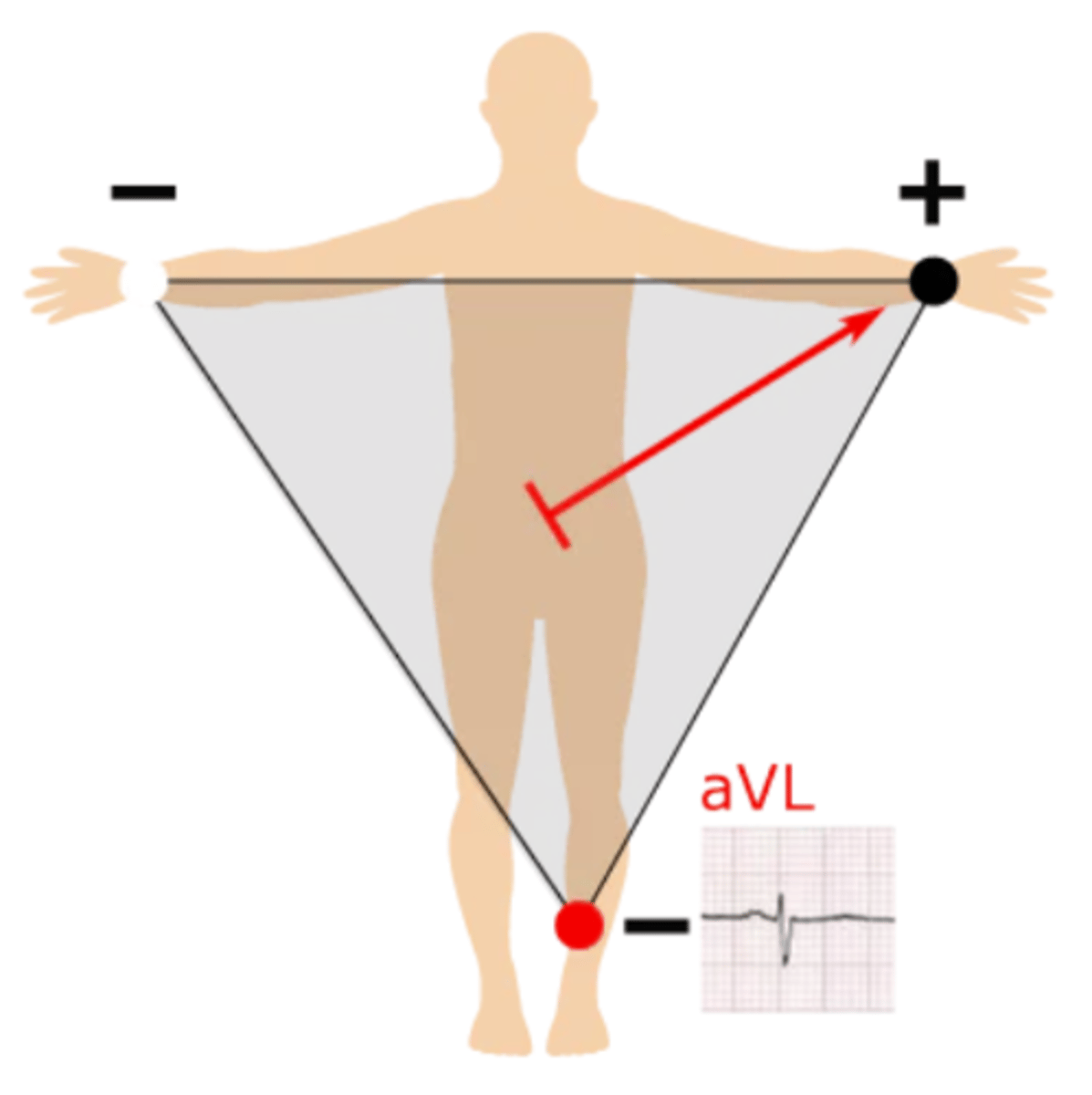
How is lead aVL created?
Right half --> left arm; produces a positive waveform as heart's electrical activity naturally moves down & to the left
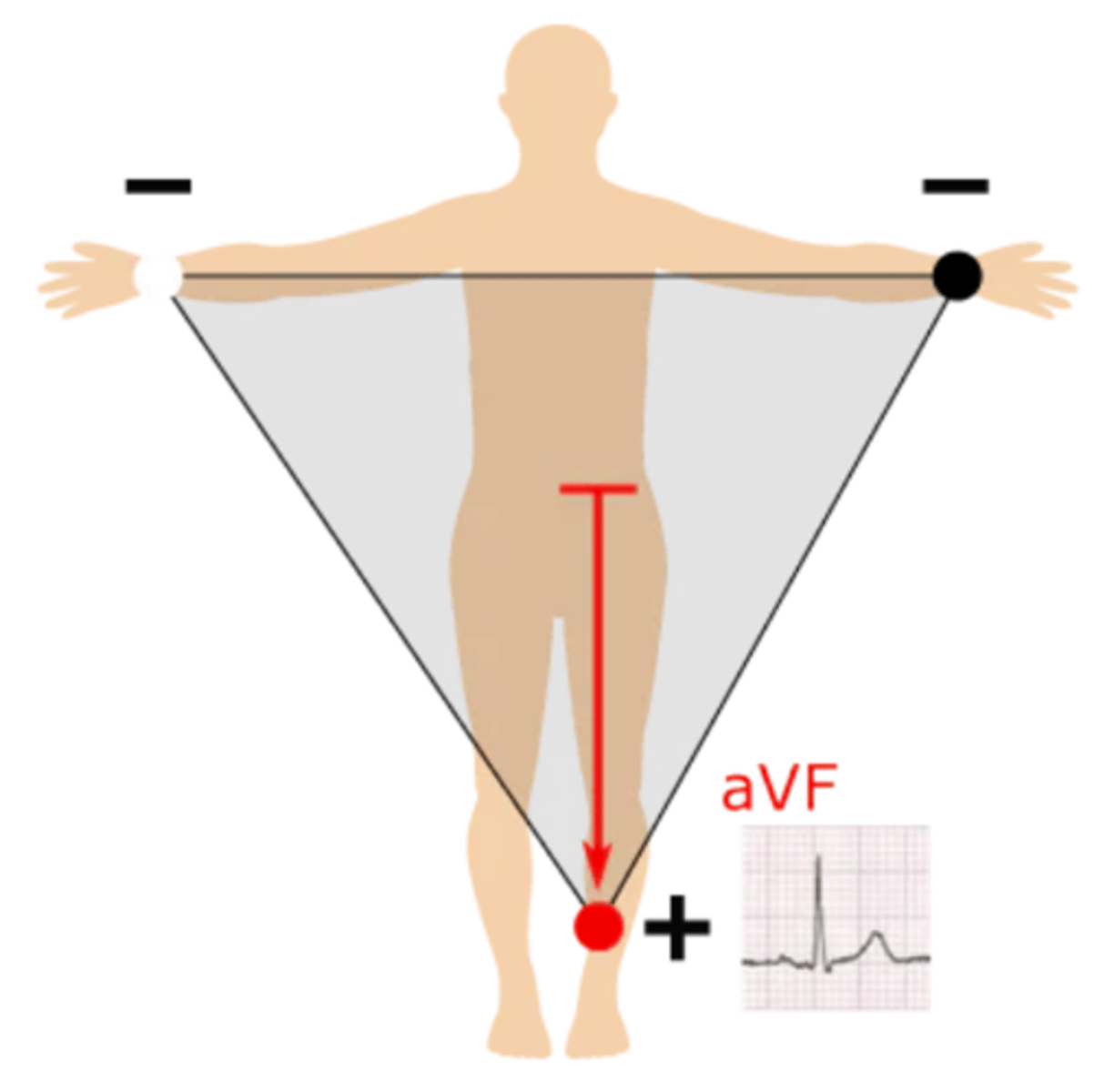
How is lead aVF created?
Top --> left leg; produces a positive waveform as heart's electrical activity naturally moves down & to the left
As a whole, what plane do the limb leads (I, II, III, aVR, aVL, aVF) examine?
The vertical (frontal) plane
Are the precordial leads bipolar or unipolar?
All are unipolar
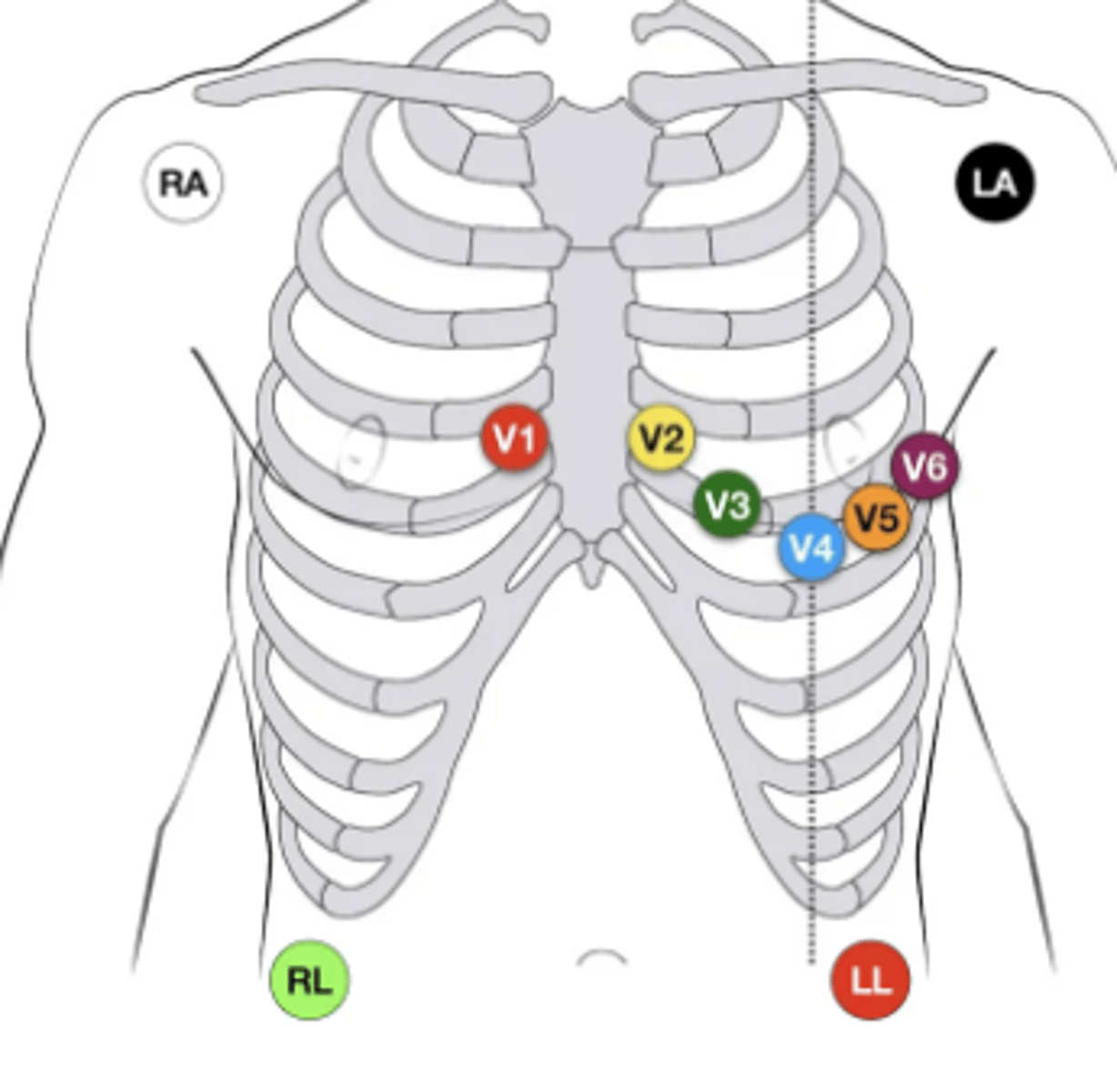
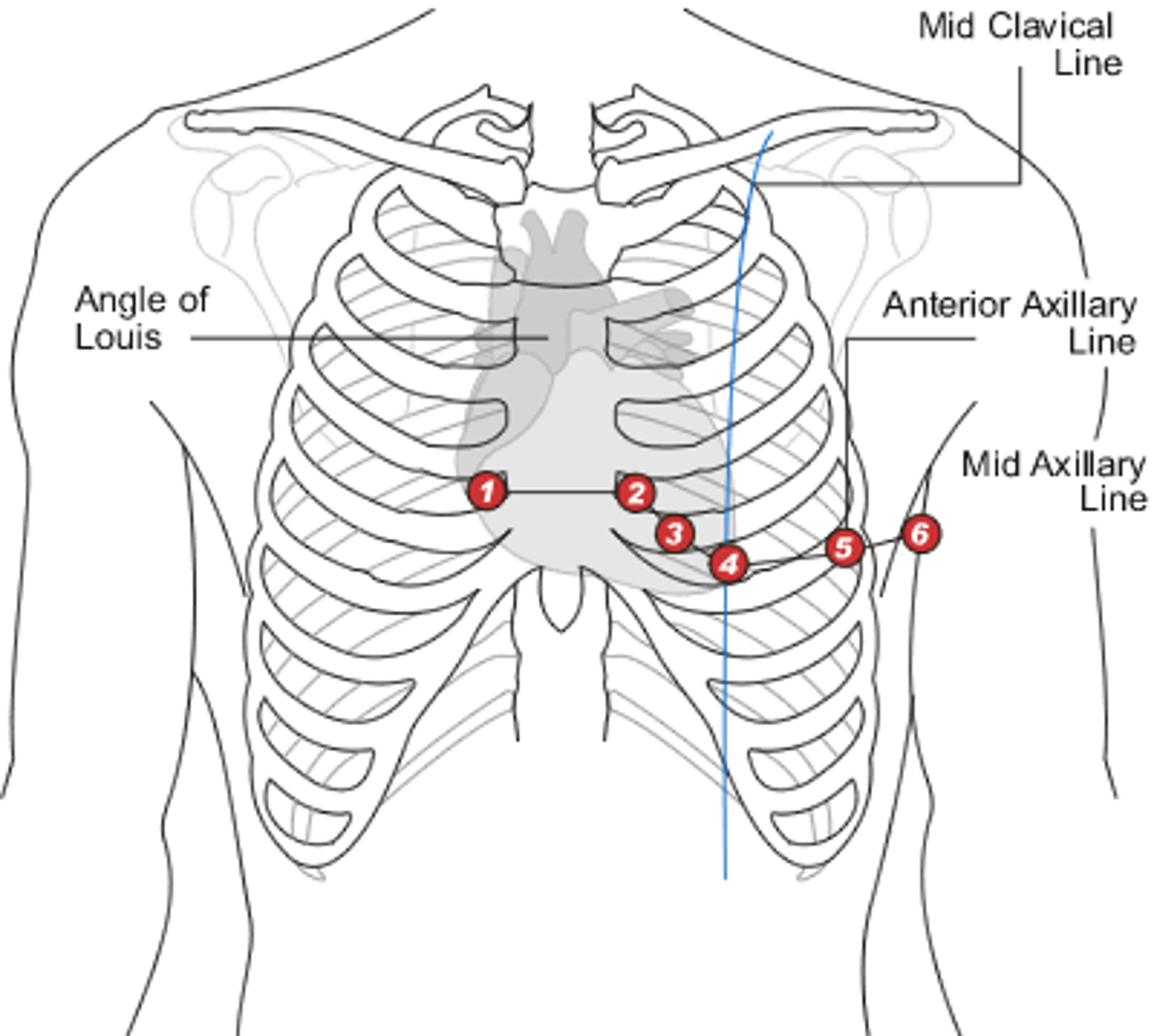
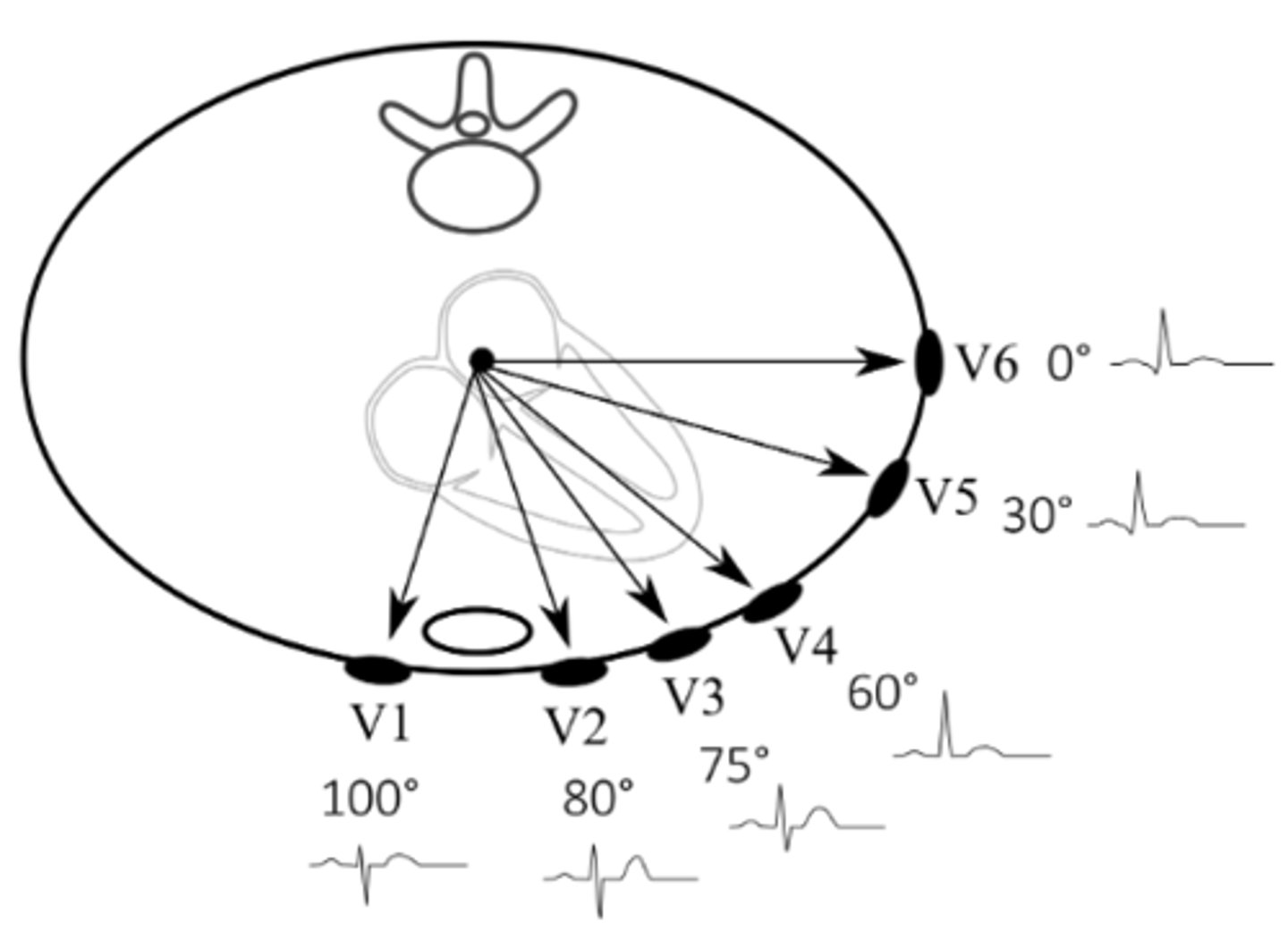
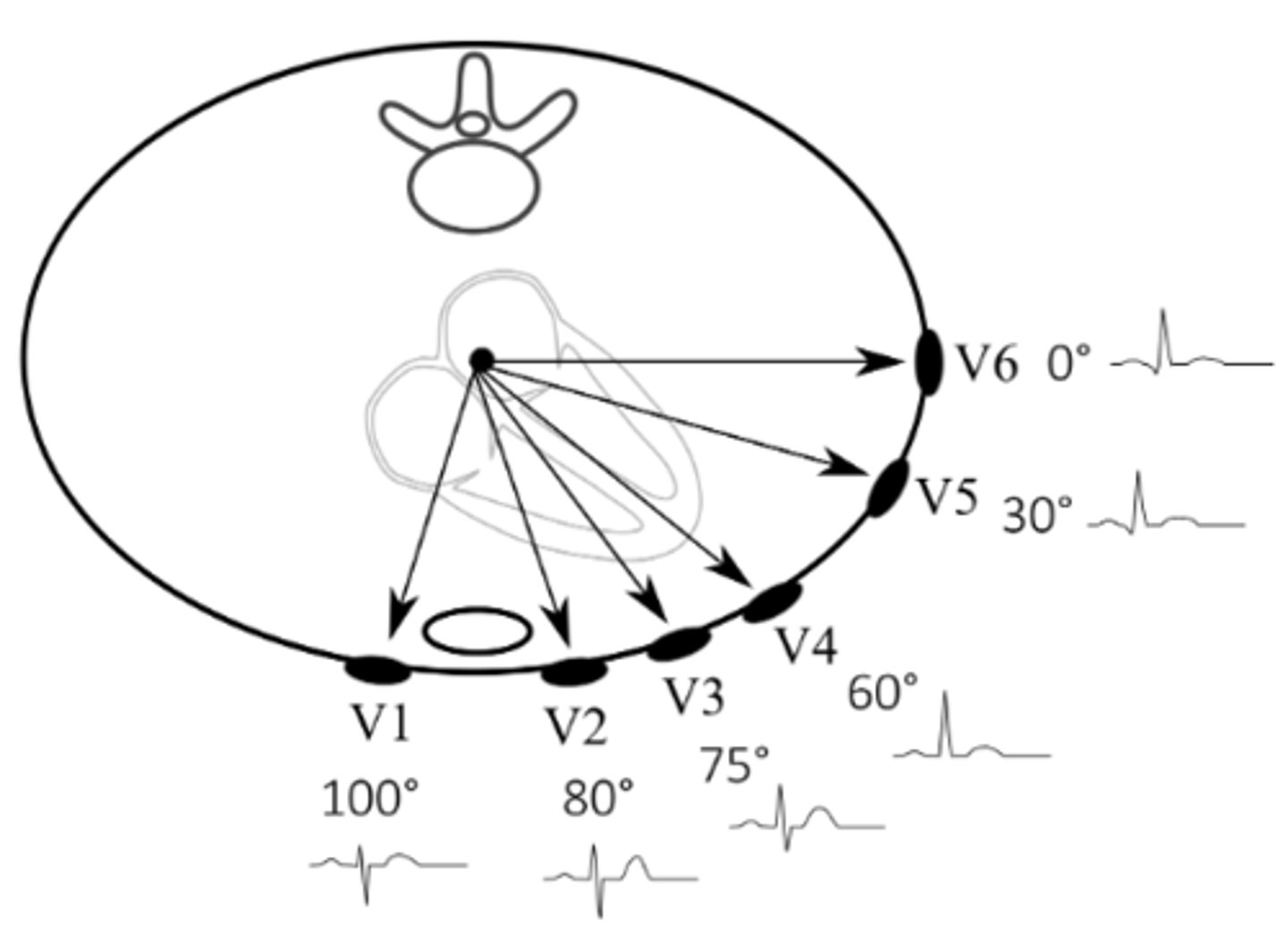
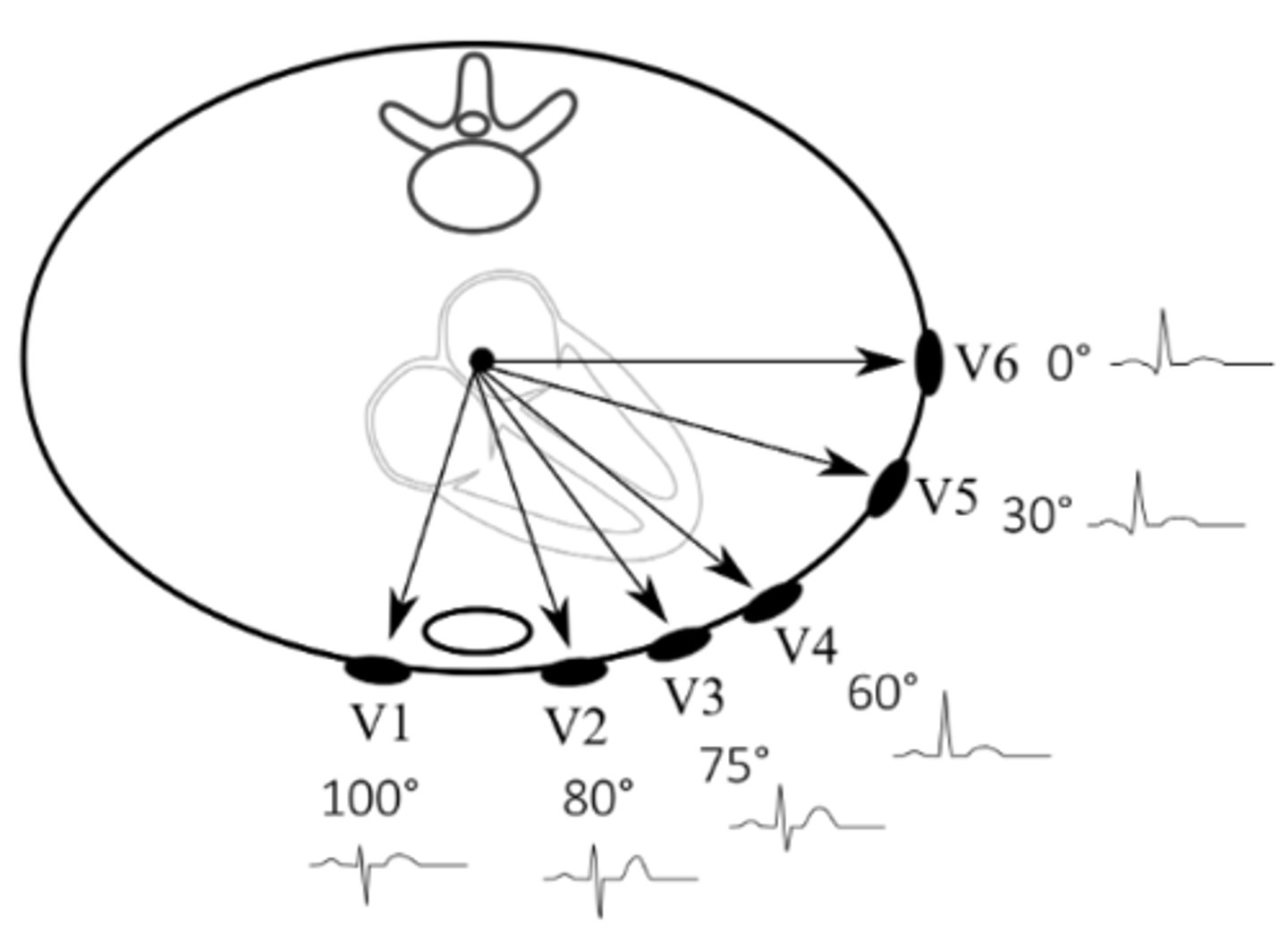
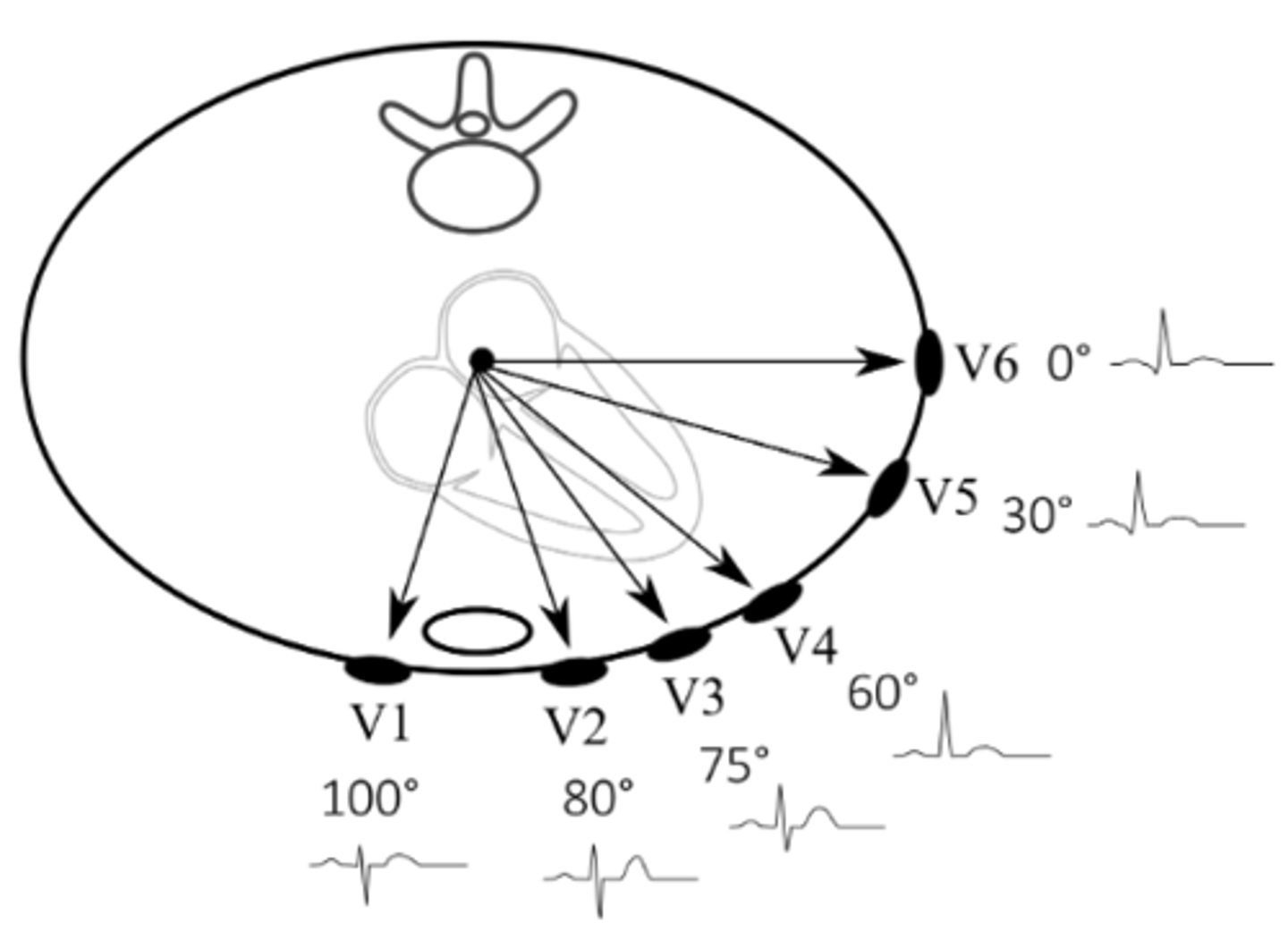
Where are leads V1 & V2 situated, respectively? What part of the heart do these help us examine?
V1: right side of sternum, 4th intercostal space
V2: left side of sternum, 4th intercostal space
Together, give us a view of the right side of the heart
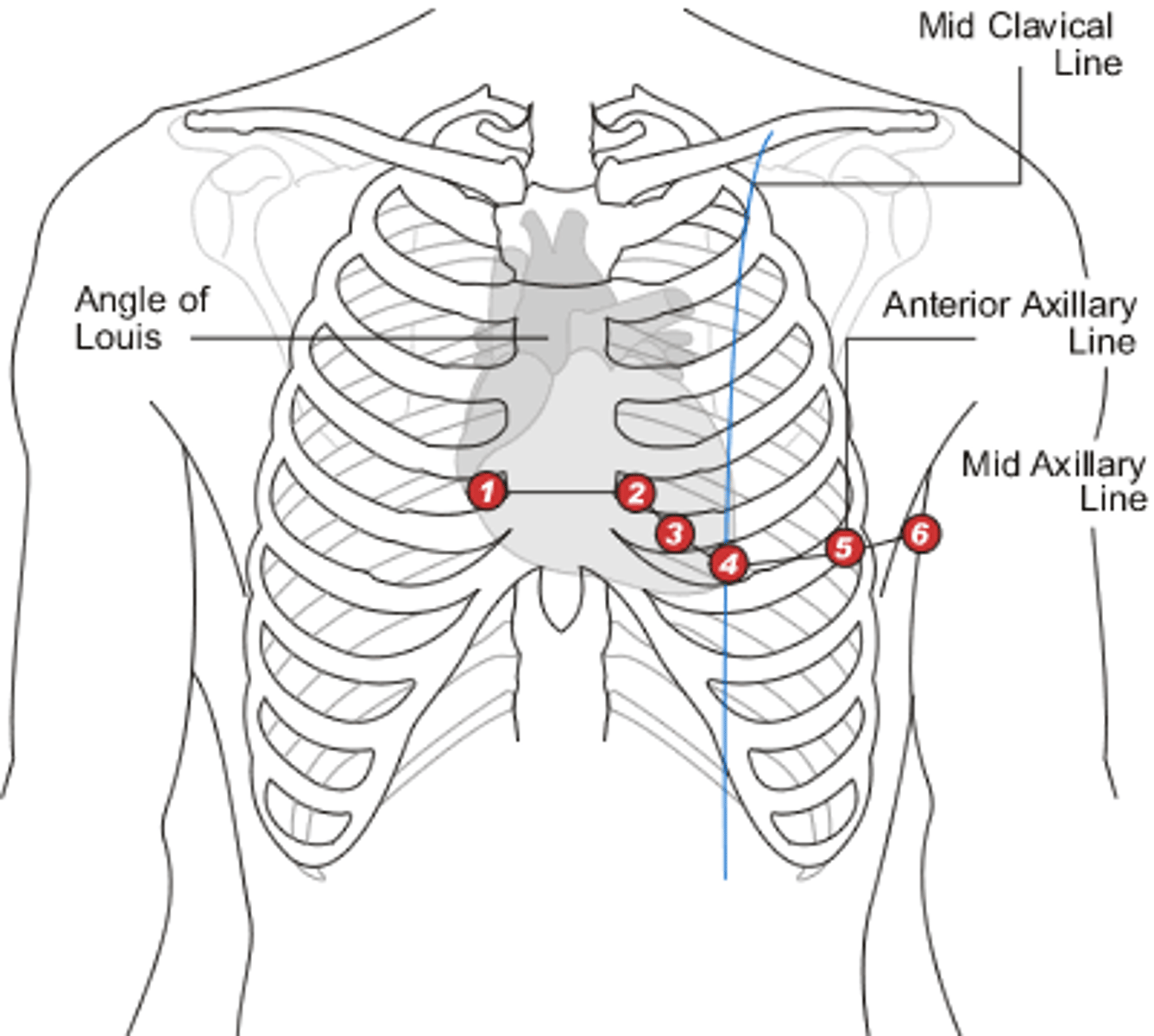
Where are leads V3 & V4 situated, respectively? What part of the heart do these help us examine?
V3: between V2 & V4
V4: left 5th intercostal space, midclavicular line
Together, give us a view of the intraventricular septum
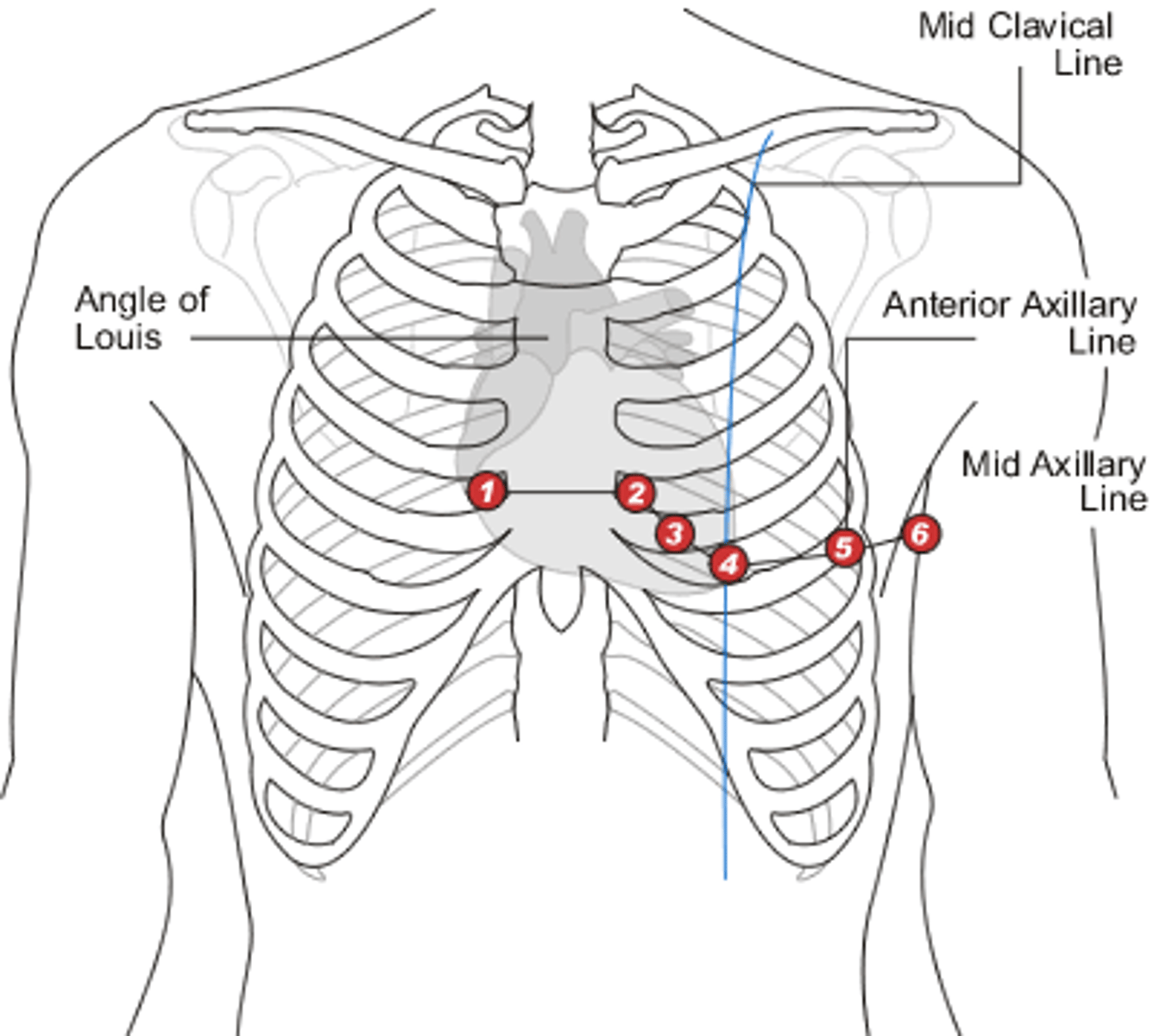
Where are leads V5 & V6 situated, respectively? What part of the heart do these help us examine?
V5: anterior axillar line, at the level of V4
V6: midaxillary line, at the level of V4
Together, give us a view of the left side of the heart
As a whole, what plane do the precordial leads (V1-V6) examine?
The horizontal (transverse) plane
What is a normal heart rate?
60-100 bpm
What is meant by "automaticity foci?"
Areas that can take over for the SA node if it fails ("potential pacemakers")
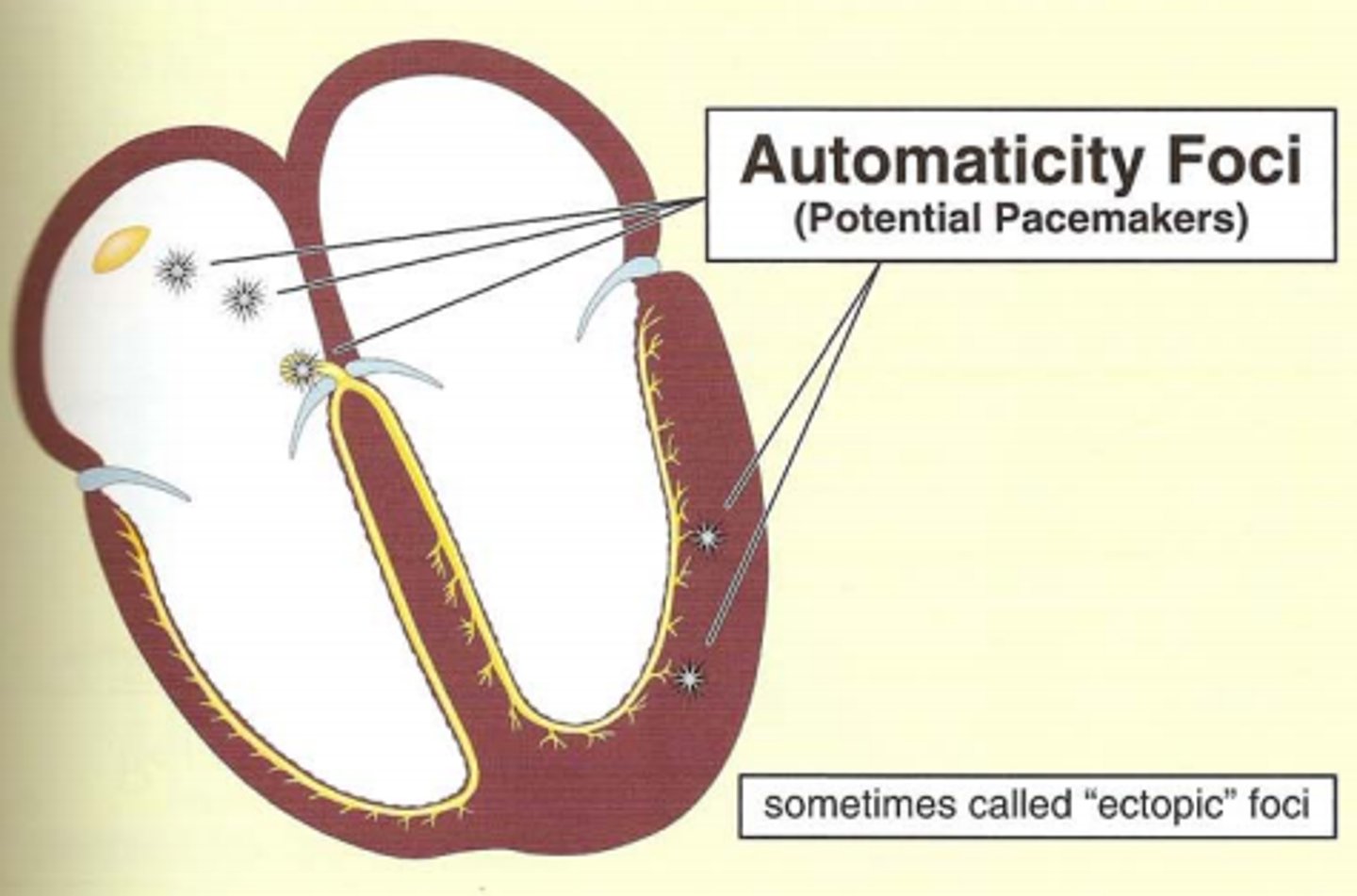
What are normal heart rates for atrial, AV/junctional, & ventricular automaticity foci, respectively?
Atrial: 60-80 bpm
AV/Junctional: 40-60 bpm
Ventricular: 20-40 bpm
What is a downside to both the "300, 150, 100, 75, 60, 50" method & the "large square" method to calculate heart rate?
They only work on regular rhythms
What is a benefit of the "6-second strip" method to calculate heart rate?
It works well for irregular rhythms
What is a normal sinus rhythm (definition)?
Rhythm that originates in the SA node
What is the difference between arrythmia & dysrhythmia?
Arrythmia: without rhythm
Dysrhythmia: abnormal rhythm
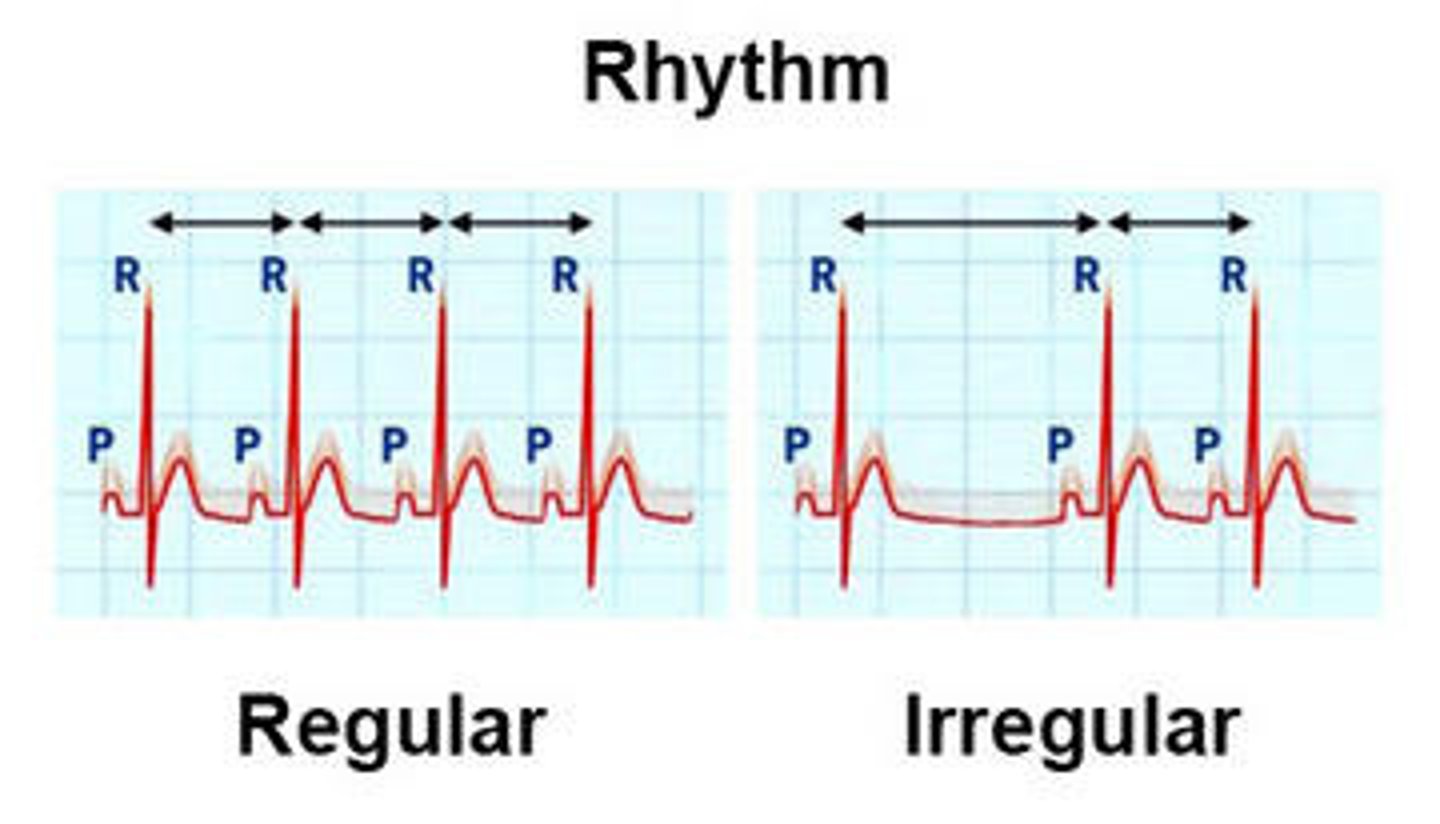
What is the difference between a regular & irregular rhythm?
Regular: same distance between similar waves forms (ex. R wave to R wave)
Irregular: different and/or irregular distance between same wave forms
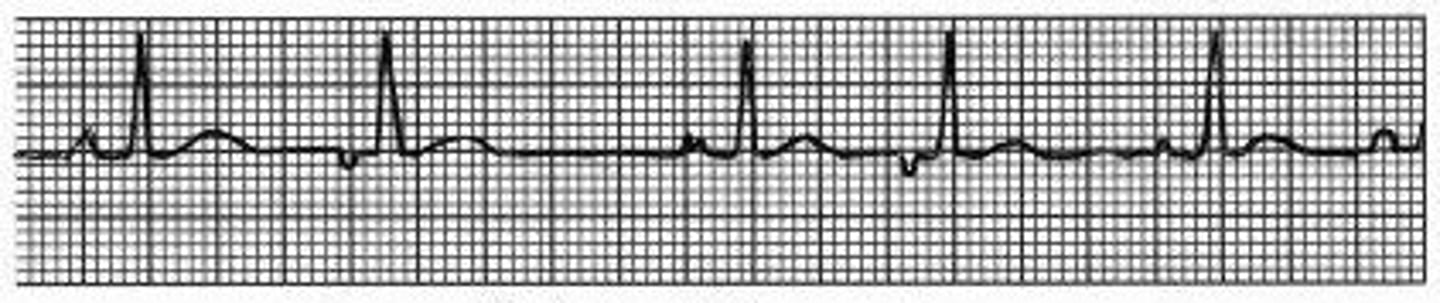
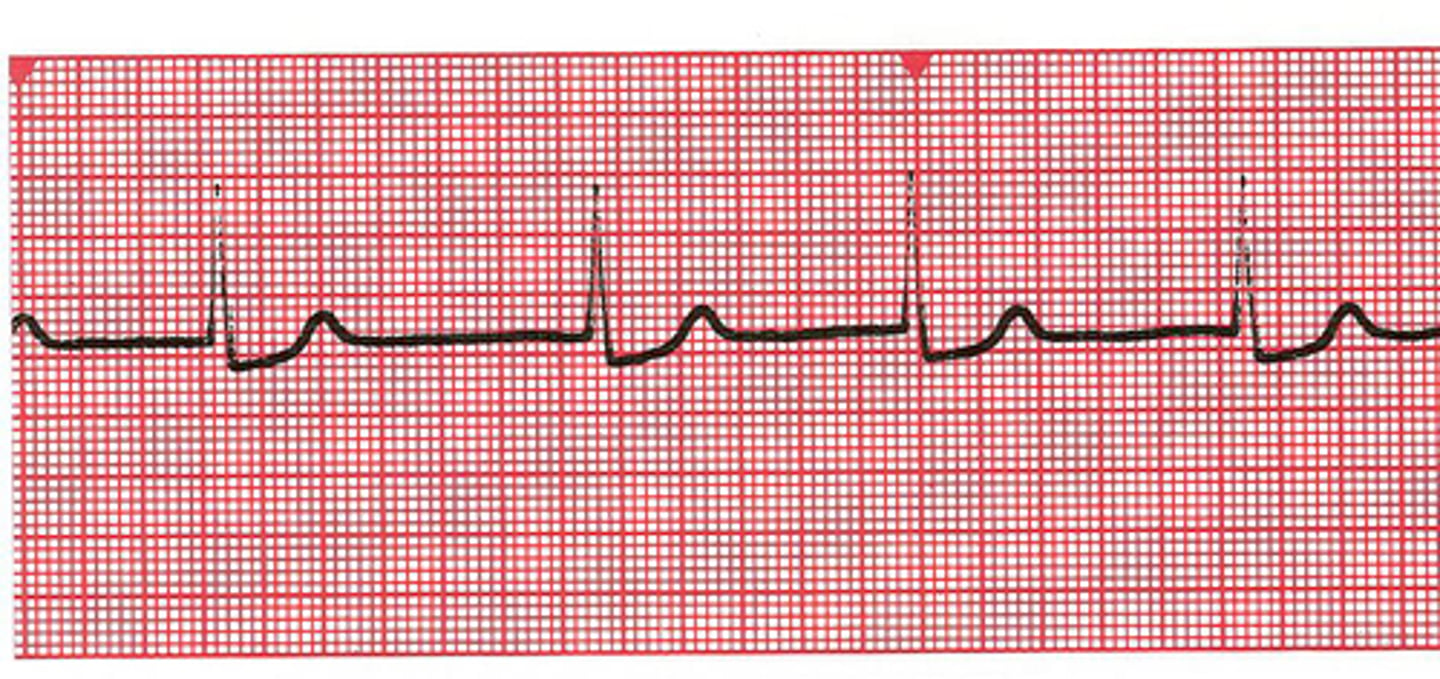
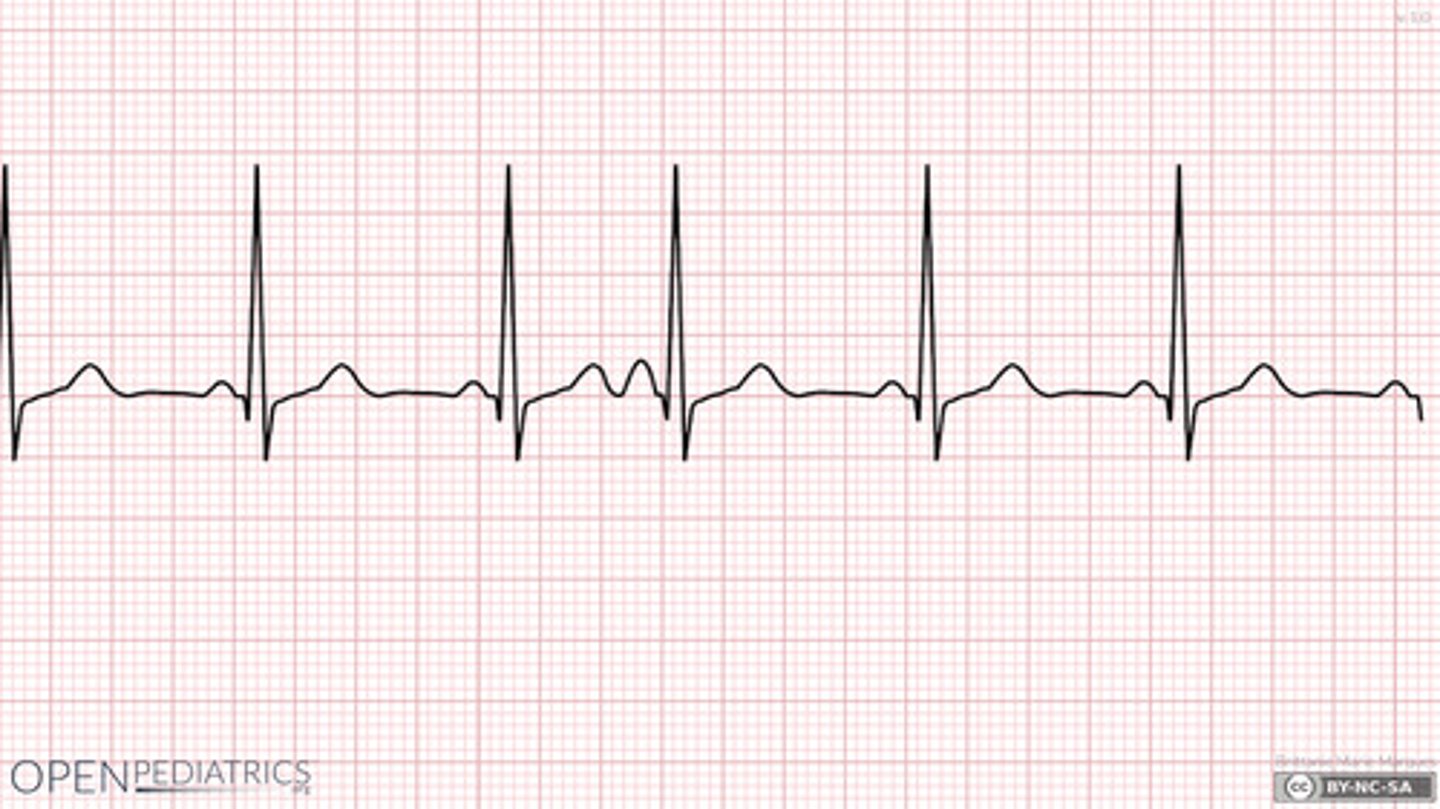
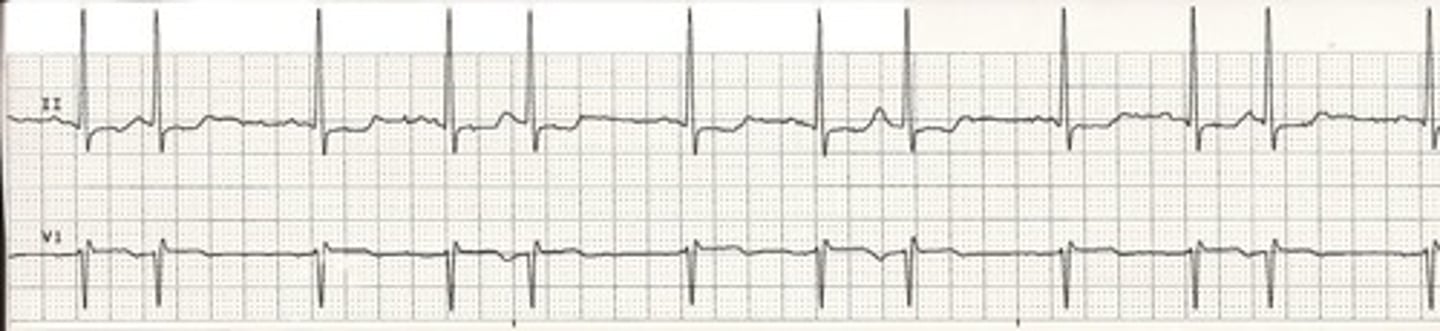
PICTURE ONLY: normal sinus rhythm

What is wandering atrial pacemaker caused by, and what is a characteristic finding?
Pacemaker activity "wanders" from SA node to nearby atrial automaticity foci; irregular rhythm w/ at least 3 different p wave morphologies (& HR < 100 bpm)
What is multifocal atrial tachycardia characterized by? What is this commonly associated with?
Irregular rhythm with a rate > 100 bpm plus at least 3 different p wave morphologies; severe lung disease (COPD)

What is atrial fibrillation characterized by?
Irregularly irregular rhythm due to continuous rapid fire of multiple atrial foci, leading to no real p waves & only an occasional QRS complex

In general, what is the difference between an escape beat and an escape rhythm?
Beat: automaticity focus takes over for one beat due to a brief pause in SA node pacing
Rhythm: automaticity focus takes over & produces its own rate due to the SA node stopping entirely
What is an atrial escape rhythm characterized by?
Originates in an atrial automaticity focus (rate 60-80 bpm); p waves are not identical to the previous p waves (because those were produced by the SA node, these are produced by an automaticity focus)

What is a junctional escape rhythm characterized by?
Originates in an AV junction automaticity focus (rate 40-60 bpm); no p wave or an inverted p wave but a normal QRS
What is a ventricular escape rhythm characterized by?
Originates in a ventricular automaticity focus (rate 20-40 bpm); wide QRS complexes (>0.12 seconds/3 boxes)

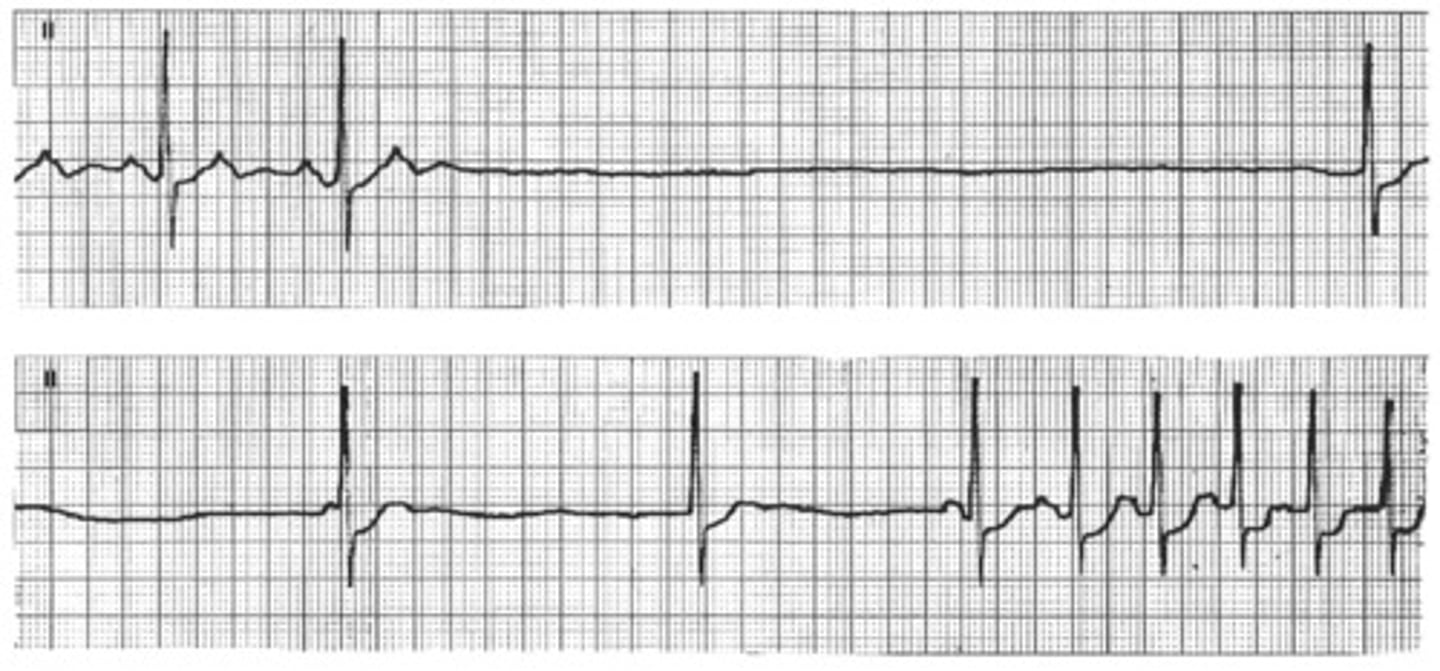
What is sinus arrest, and what is it characterized by?
Pause in SA node pacing, leading to an absence of sinus P waves on the ECG

In general, what is a premature beat? What is the difference between bigeminy & trigeminy?
An irritable focus spontaneously fires a single stimulus leading to an early beat; bigeminy = every other beat is early, trigeminy = every third beat is early
What is a premature atrial contraction (PAC) characterized by?
Early atrial beat where the p wave is of a different morphology than the rest
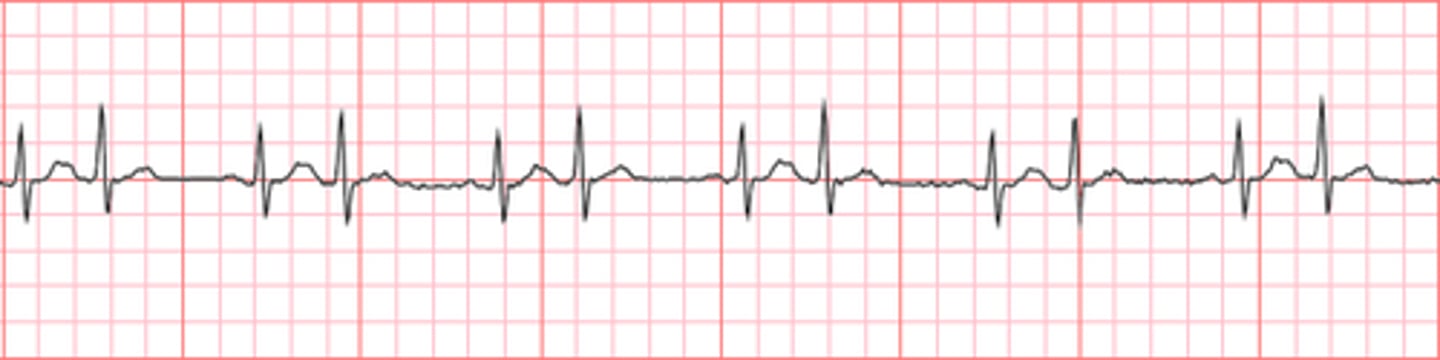
PICTURE ONLY: atrial bigeminy
PICTURE ONLY: atrial trigeminy
What is a premature junctional contraction (PJC) characterized by?
Early junctional beat where the QRS complex is slightly wider than normal & the p wave is absent or inverted

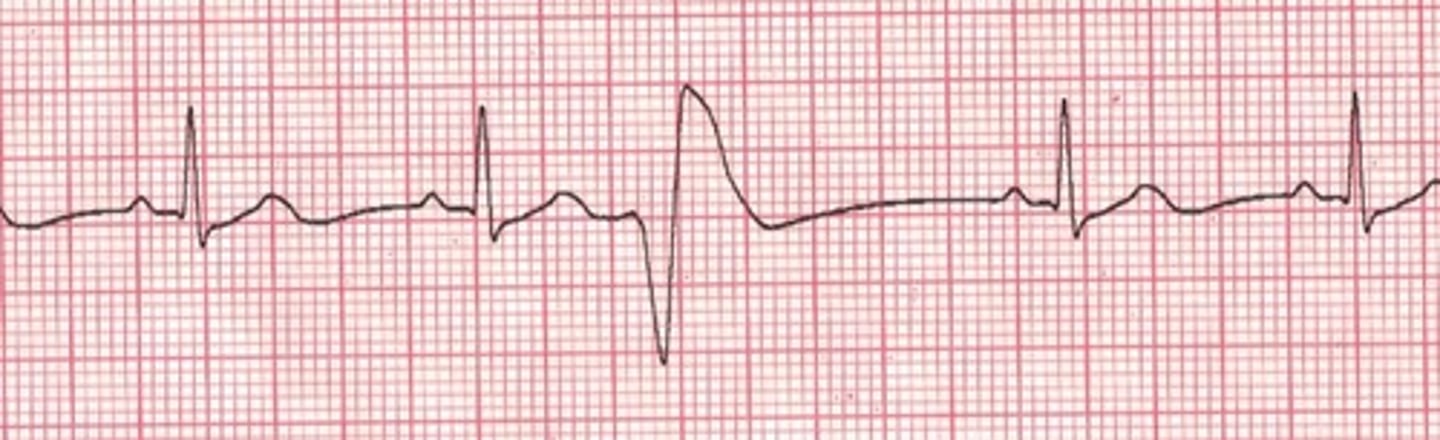
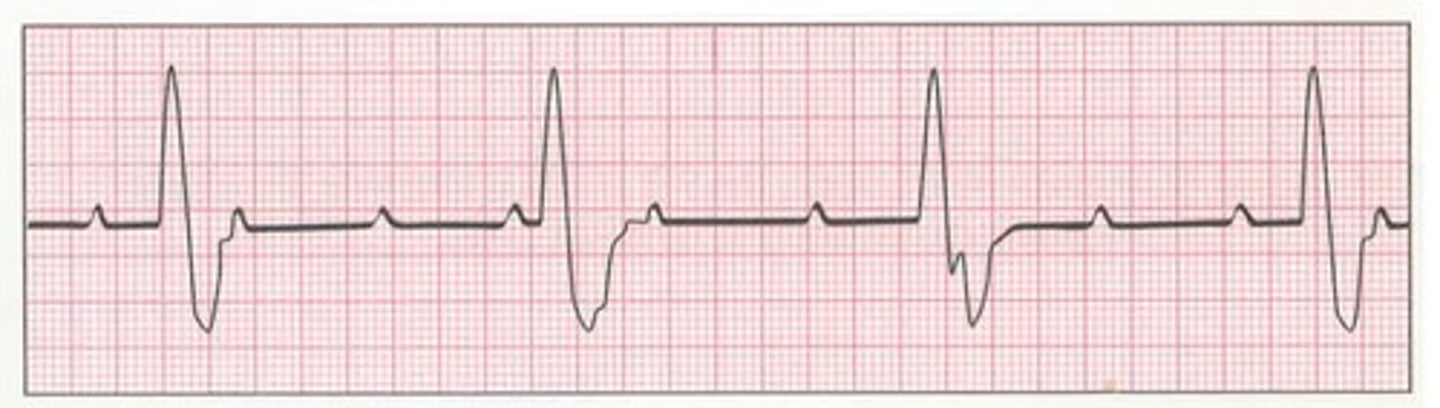
What is a premature ventricular contraction (PVC) characterized by?
Early ventricular beat where the QRS complex is increased in both width & amplitude and the p wave is absent
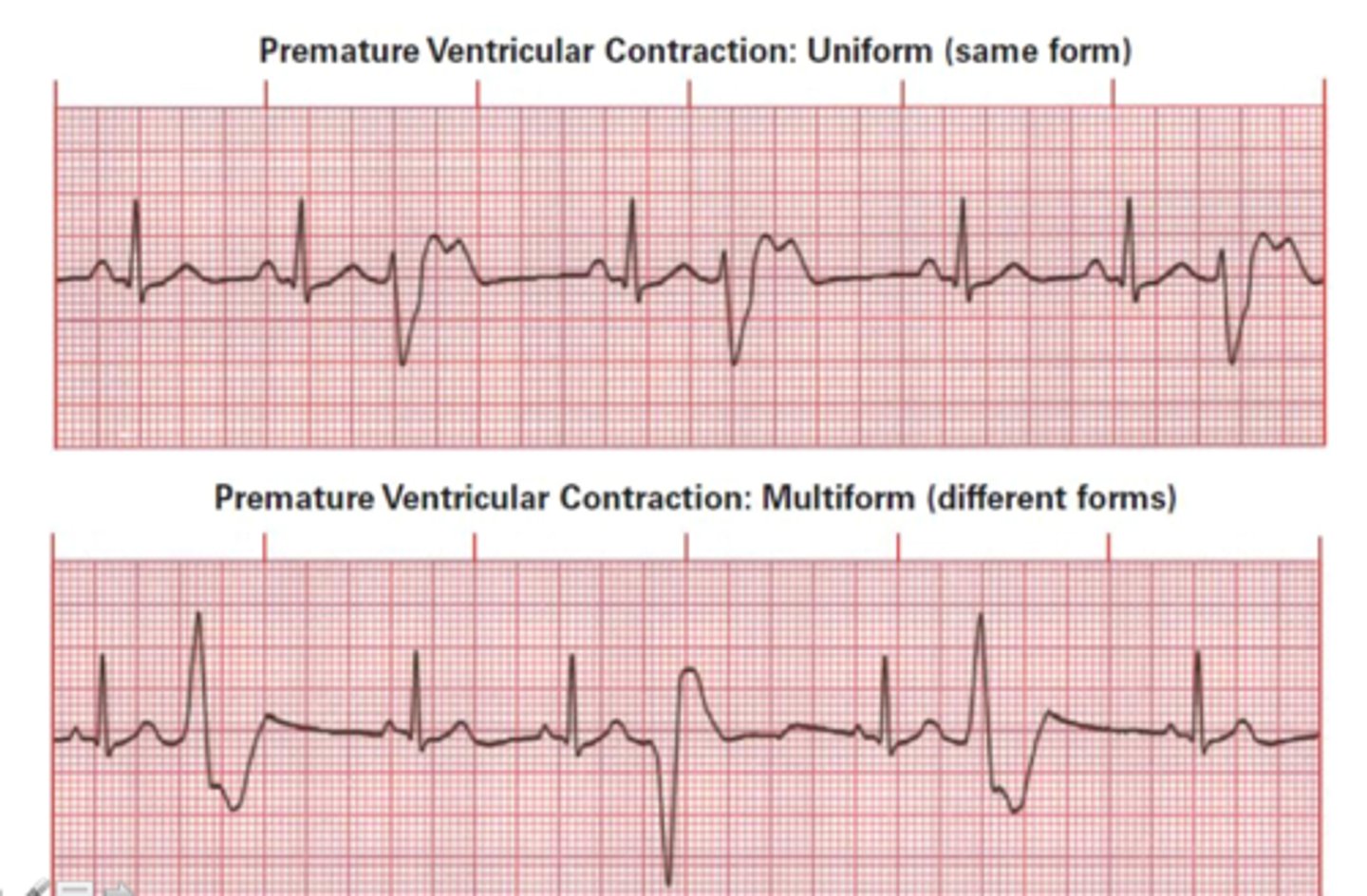
What is the difference between a unifocal and multifocal premature ventricular contraction?
Unifocal: PVC originating from one site, all abnormal QRS complexes will looks the same
Multifocal: PVC originating from multiple sites, abnormal QRS complexes will look different
What heart rates qualify as paroxysmal tachycardia, flutter, & fibrillation, respectively?
Paroxysmal: 150-250 bpm
Flutter: 250-350 bpm
Fibrillation: 350-450 bpm
JUST KNOW: "paroxysmal" means sudden (sometimes tachycardia occurs suddenly)
Although supraventricular tachycardia (SVT) is an umbrella term for any tachycardia originating above the ventricles, what does it tend to be characterized by?
Tachycardia where the p wave is absent or inverted

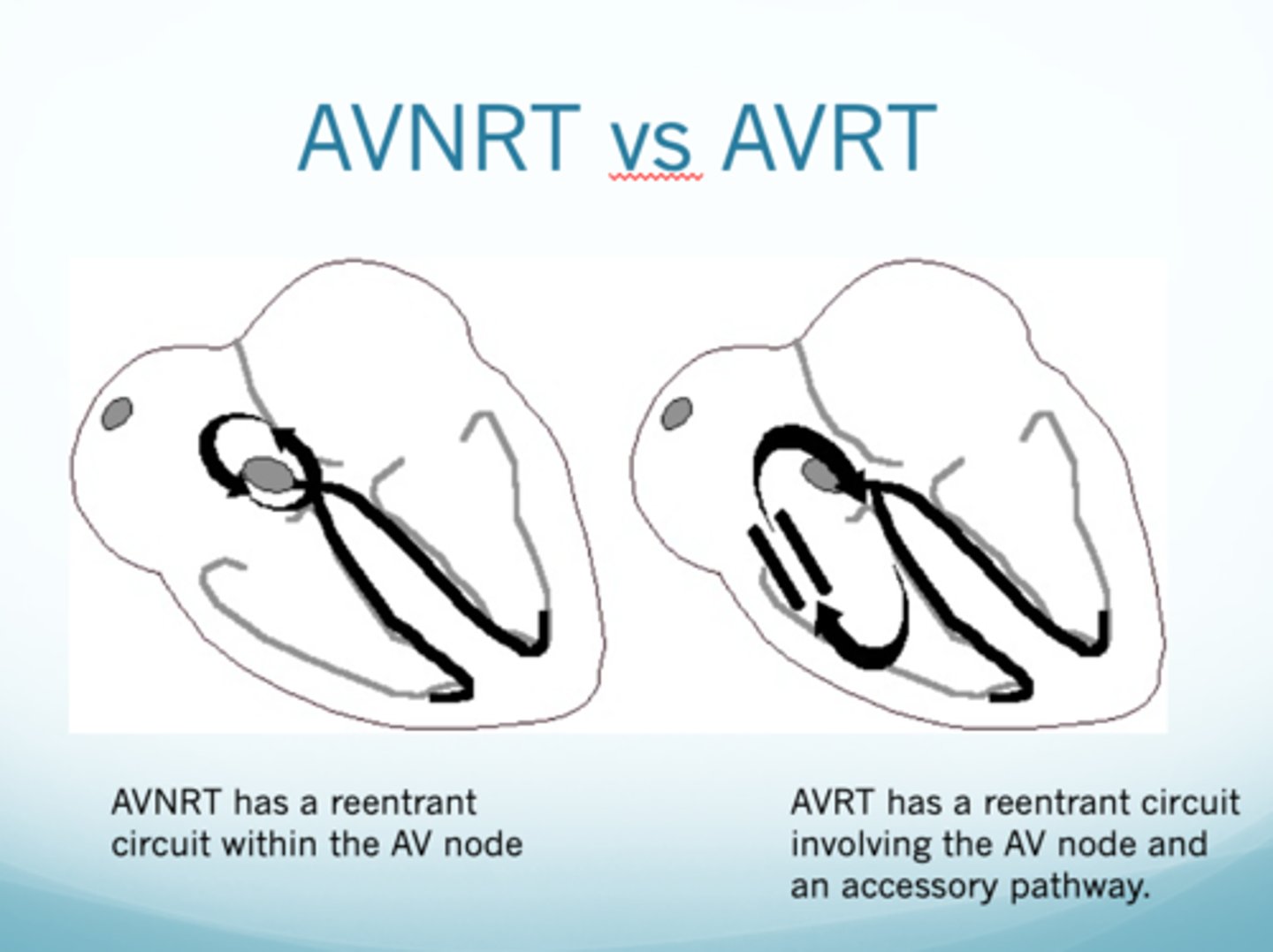
In general, what is AV reentrant tachycardia (AVRT)?
Type of SVT where electrical signals travel through the AV node to the ventricles and then back up to the atria via an accessory pathway, creating a re-entry circuit that causes a rapid heart rate (essentially, the electrical signal travels in the "correct" direction through the AV node and then back up through an abnormal pathway, causing tachycardia)
In general, what is AV nodal reentrant tachycardia (AVNRT)?
Type of SVT where there is a continuous loop circuit within the AV node itself leading to a tachycardic rate
In general, what is orthodromic AVRT?
Most common type of SVT characterized by narrow QRS complexes
What is ventricular tachycardia, and what is it characterized by?
Sudden rapid firing of irritable ventricular focus producing AV dissociation (independent pacing of atria & ventricles) as well as wide QRS complexes

What is Torsades de Pointes, and what is it characterized by?
Variant of ventricular tachycardia characterized by a "twisting of points" (basically same appearances as V tach but it goes up and down as opposed to staying at a consistent level)
What is atrial flutter, and what is it characterized by?
Rapid succession of back-to-back atrial depolarization (QRS complex every 2nd or 3rd wave) producing a sawtooth pattern

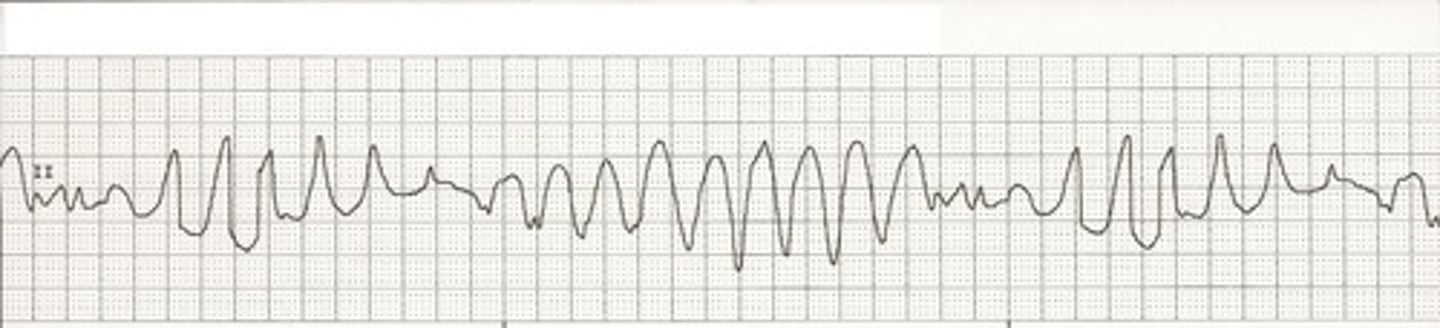
What is ventricular fibrillation, and what is it characterized by?
Numerous ventricular foci pacing rapidly leads to twitching rather than contracting & subsequent lack of heart pumping; disorganized, erratic impulses of varying amplitude

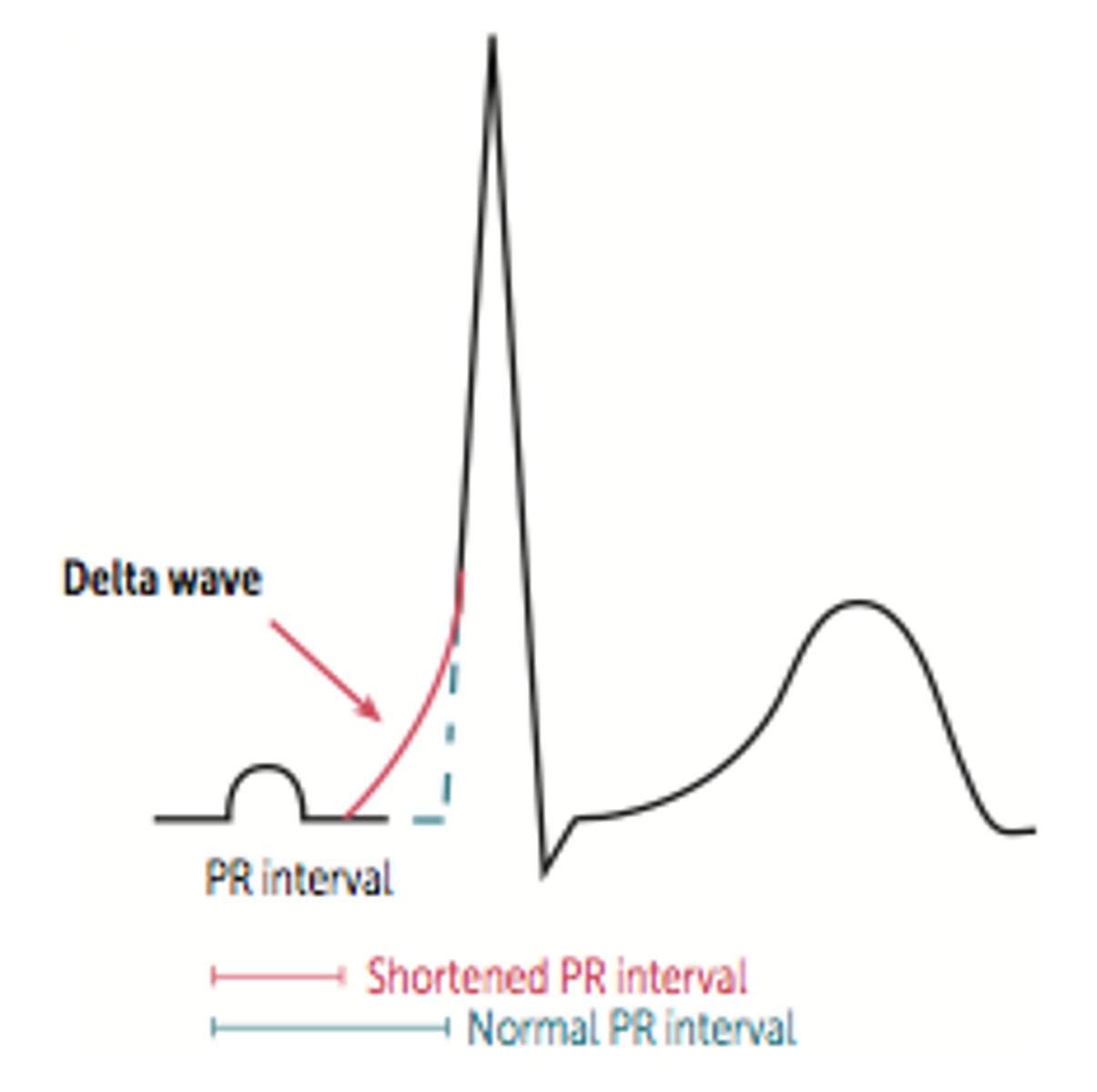
What is Wolff-Parkinson-White syndrome, and what is it characterized by?
Type of ventricular preexcitation syndrome where there is an accessory AV conduction pathway called the bundle of Kent (is a form of AVRT); leads to premature ventricular depolarization resulting in a delta wave (slurred QRS upstroke), short PR interval, & wide QRS complex
In general, what is a heart block?
Slowing or blocking of normal conduction
What is an SA block, & what is it characterized by?
SA node stops firing for at least one cycle, followed by the resumption of normal sinus rhythm or an escape beat

What is sick sinus syndrome, and what is it characterized by?
"Wastebasket" of arrythmias caused by SA node dysfunction (often seen in the elderly due to replacement of sinus tissue with fibrous tissue); tachy-brady syndrome (alternating episodes of bradycardia & tachycardia)
In general, what is an AV block? What is the difference between first, second, & third degree?
Block in or below AV node that delays ventricular contraction
First Degree: block is in AV node
Second Degree: block in (Mobitz type 1) or below (Mobitz type 2) AV node
Third Degree: block below AV node
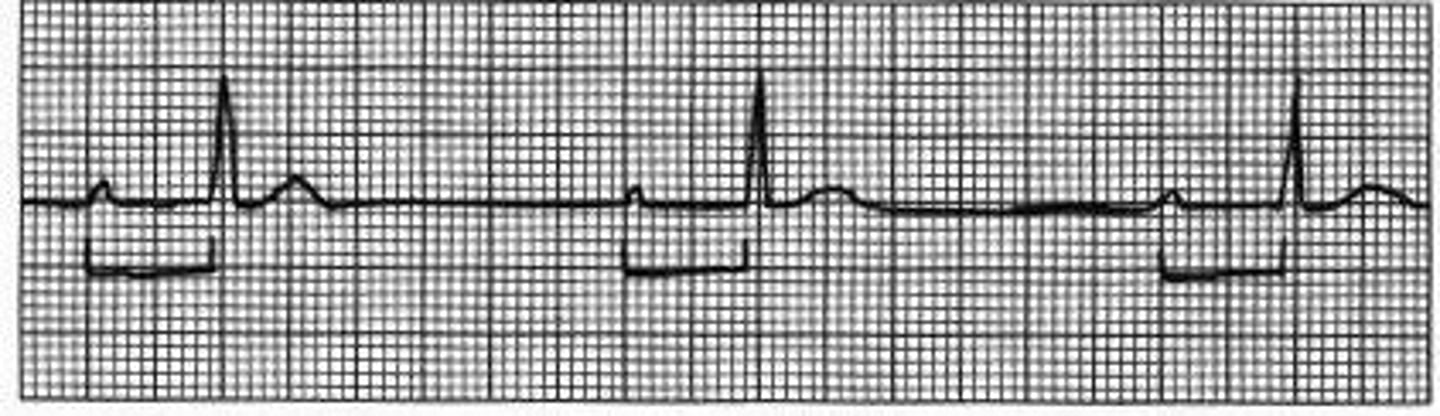
What is a first-degree AV block characterized by?
Prolonged PR interval, always a QRS following the p wave
In general, what are all second-degree AV blocks characterized by?
Dropped QRS complexes (some atrial depolarization but not all)
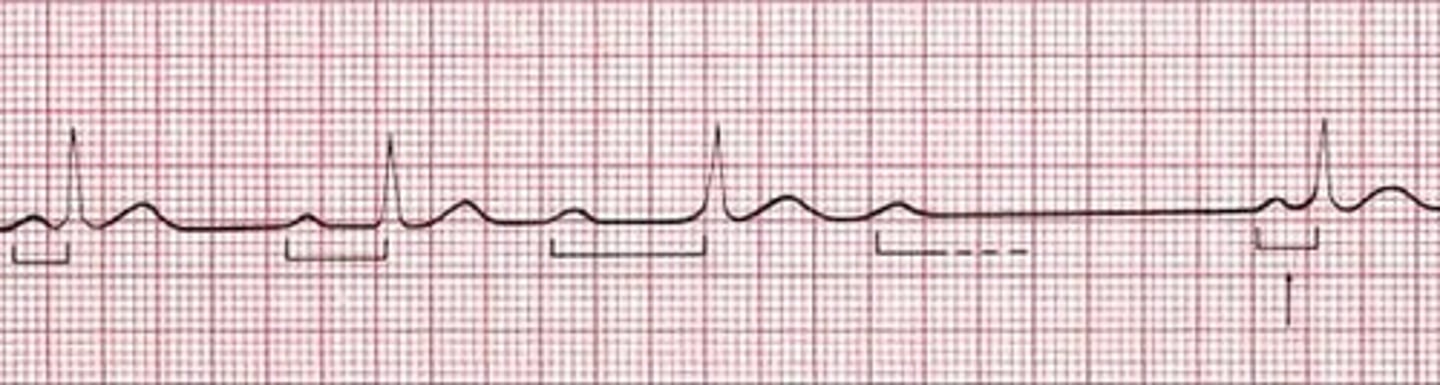
What is a Mobitz Type I second degree AV block characterized by?
Progressive lengthening of PR interval until eventually a QRS is dropped (sort of a "warning" that the block is coming)
What is a Mobitz Type II second degree AV block characterized by?
Dropped QRS complexes with consistent PR intervals (no progressive lengthening as seen in Mobitz Type I)

What is a third-degree AV block characterized by?
AV dissociation (consistent p-p interval & consistent R-R interval, but the two are not related)
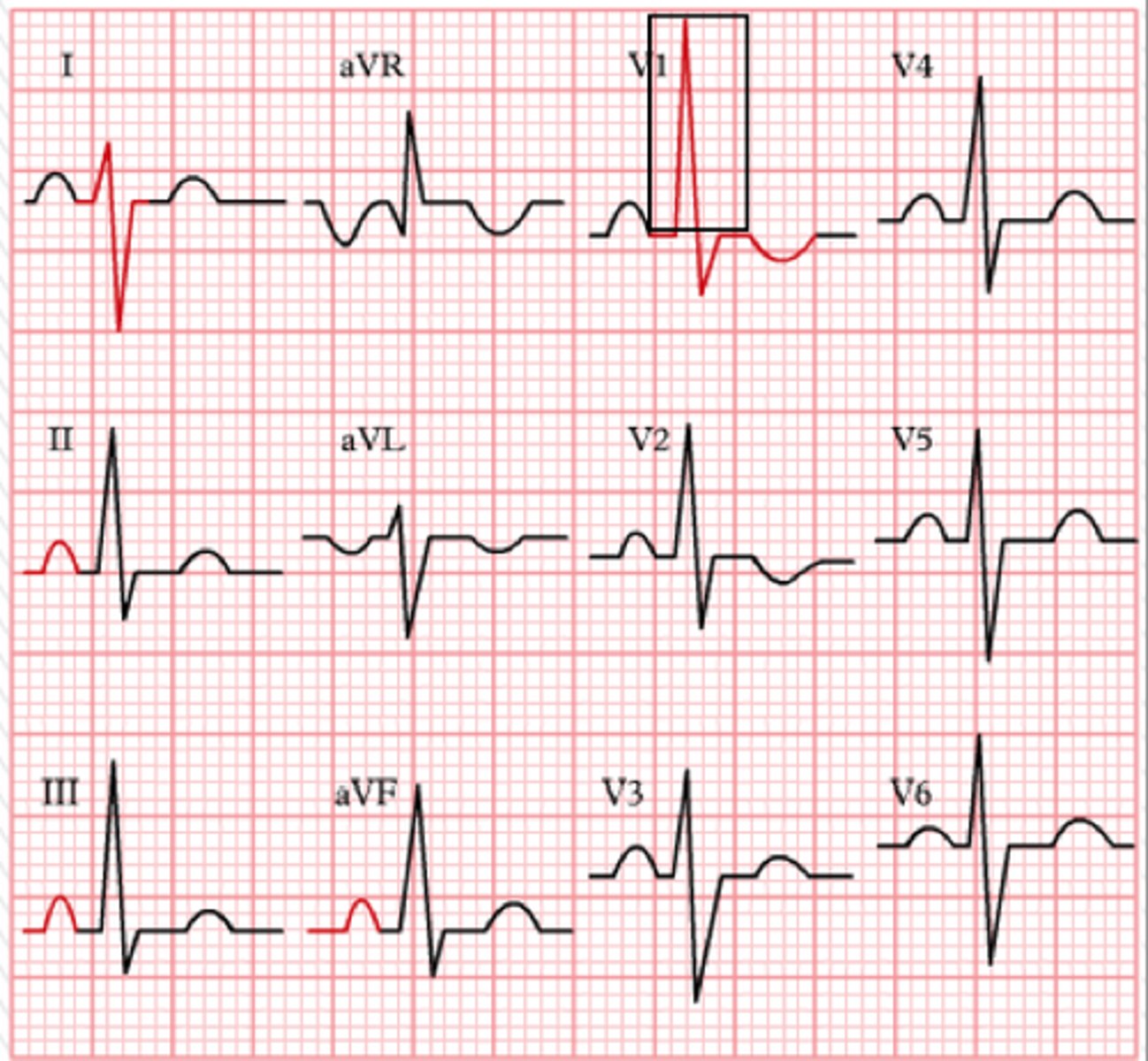
What is the heart axis? Which two leads are most beneficial in determining axis?
Direction of depolarization as it passes through the heart; lead I & lead aVF (since normal conduction goes down & to the left)
In general, what are the 4 ways we categorize axis devation?
1) Normal
2) Left axis deviation (LAD)
3) Right axis deviation
4) Extreme right axis deviation
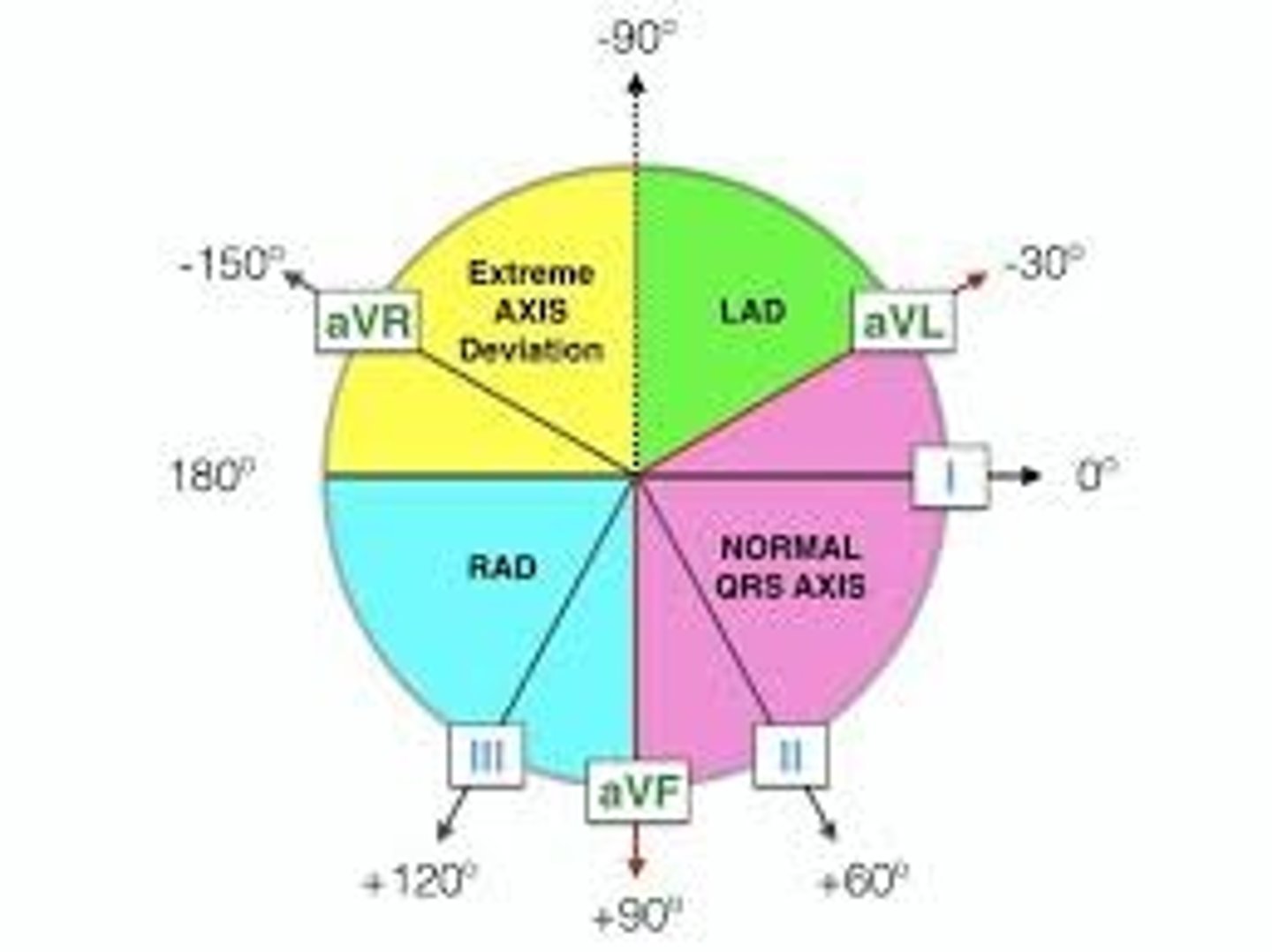
What waveform to we expect to see on lead I & lead aVF in a normal axis?
Lead I: positive
Lead aVF: positive
What waveform to we expect to see on lead I & lead aVF in left axis deviation?
Lead I: positive
Lead aVF: negative
What waveform to we expect to see on lead I & lead aVF in right axis deviation?
Lead I: negative
Lead aVF: positive
What waveform to we expect to see on lead I & lead aVF in extreme right axis deviation?
Lead I: negative
Lead aVF: negative
In general, what do deviation do hypertrophy & infarct produce, respectively?
Hypertrophy: axis deviates towards area
Infarct: axis deviates away from area
What is a handy trick to confirm LAD by using lead II?
If you find LAD in either lead I or lead aVF, most of the QRS complexes in lead II will be predominantly negative if it's actually present
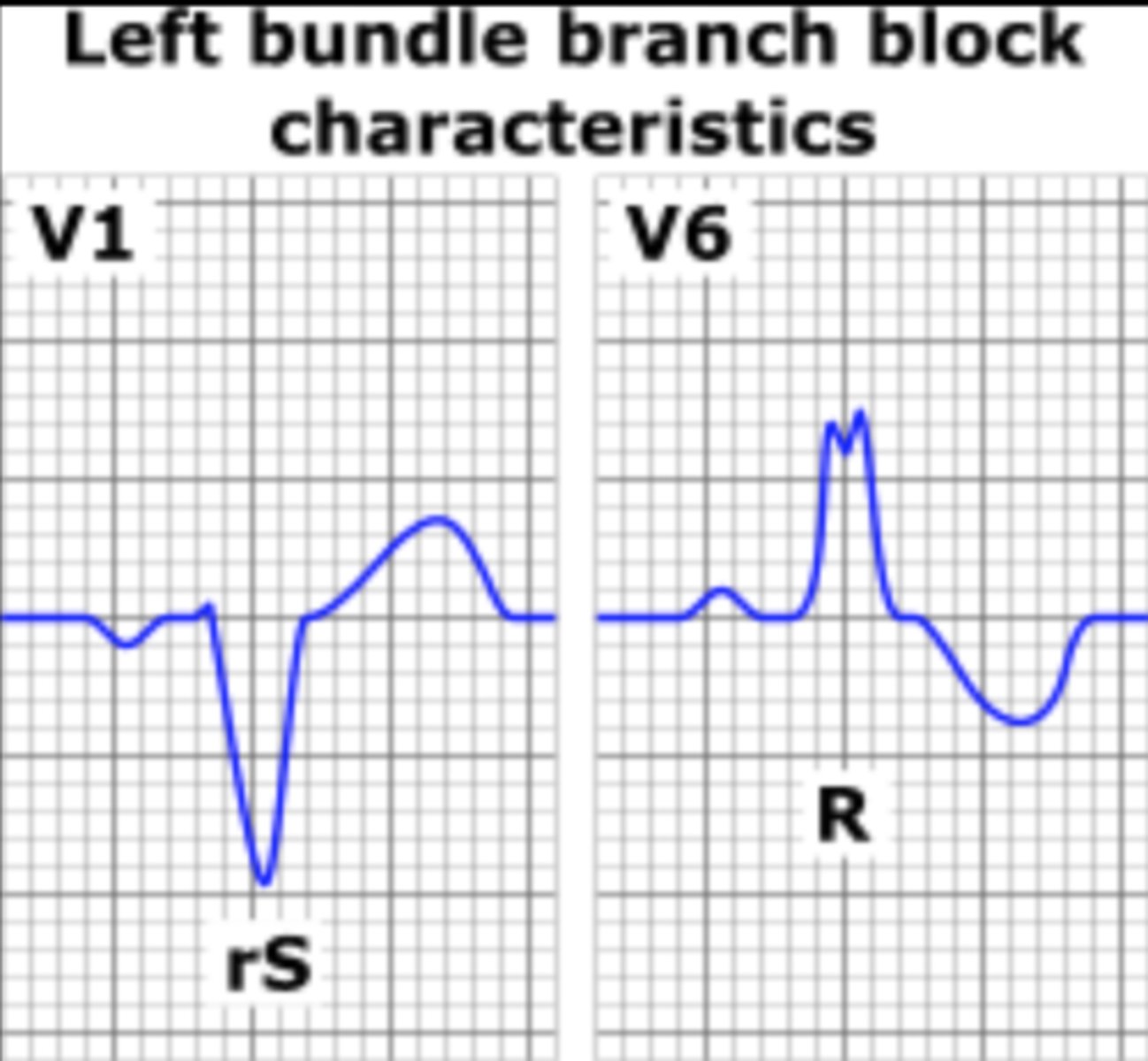
What is a bundle branch block, & what is it characterized by?
Delay in conduction to either bundle branch causes delay in depolarization of the ventricle it supplies (one ventricle will depolarize before the other); two joined QRS complexes
Which leads are best for assessing a suspected left bundle branch block (LBBB)?
Leads V5 & V6
Which leads are best for assessing a suspected right bundle branch block (RBBB)?
Leads V1 & V2
JUST KNOW: it is also possible for incomplete bundle branch blocks to occur
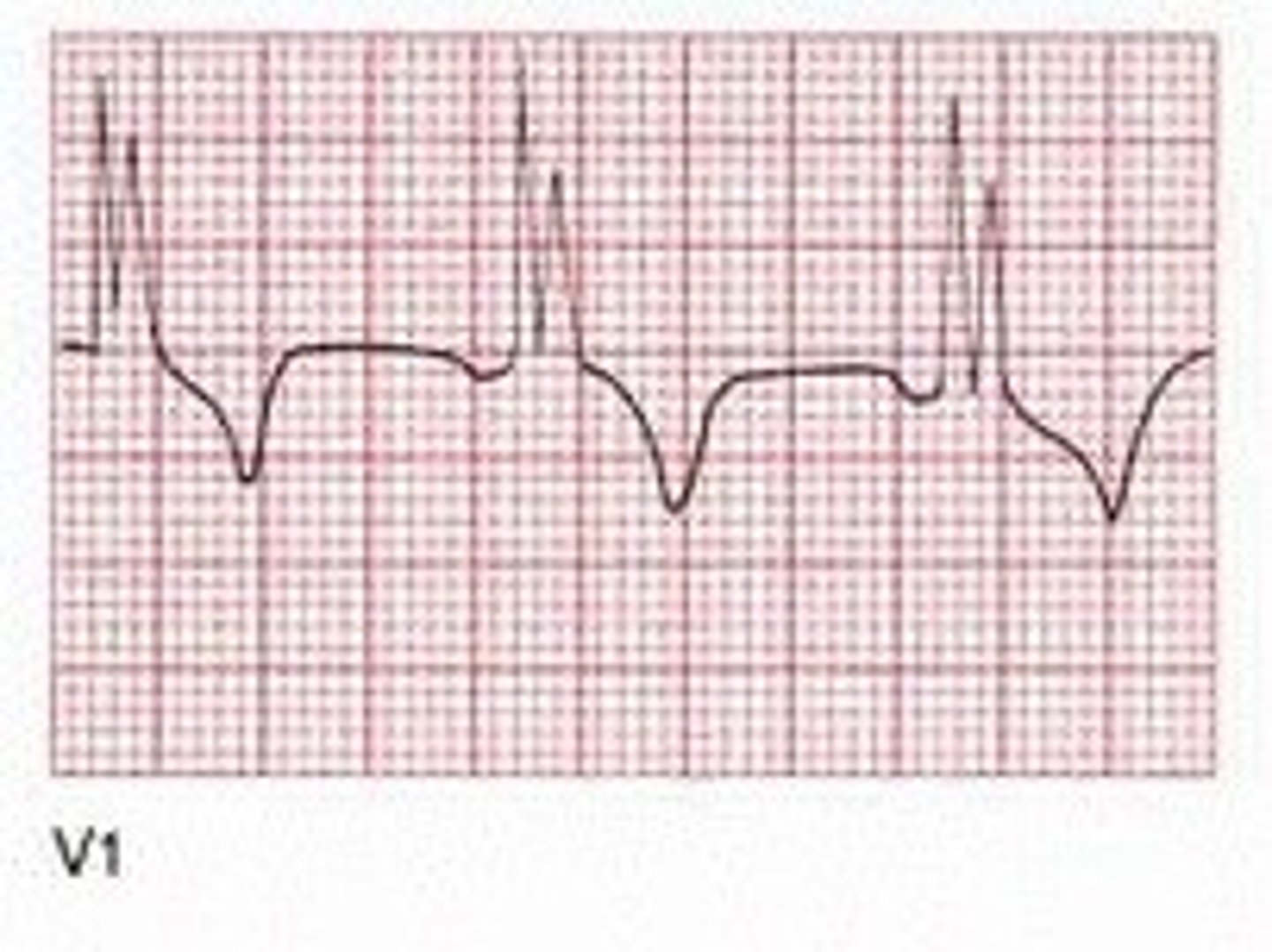
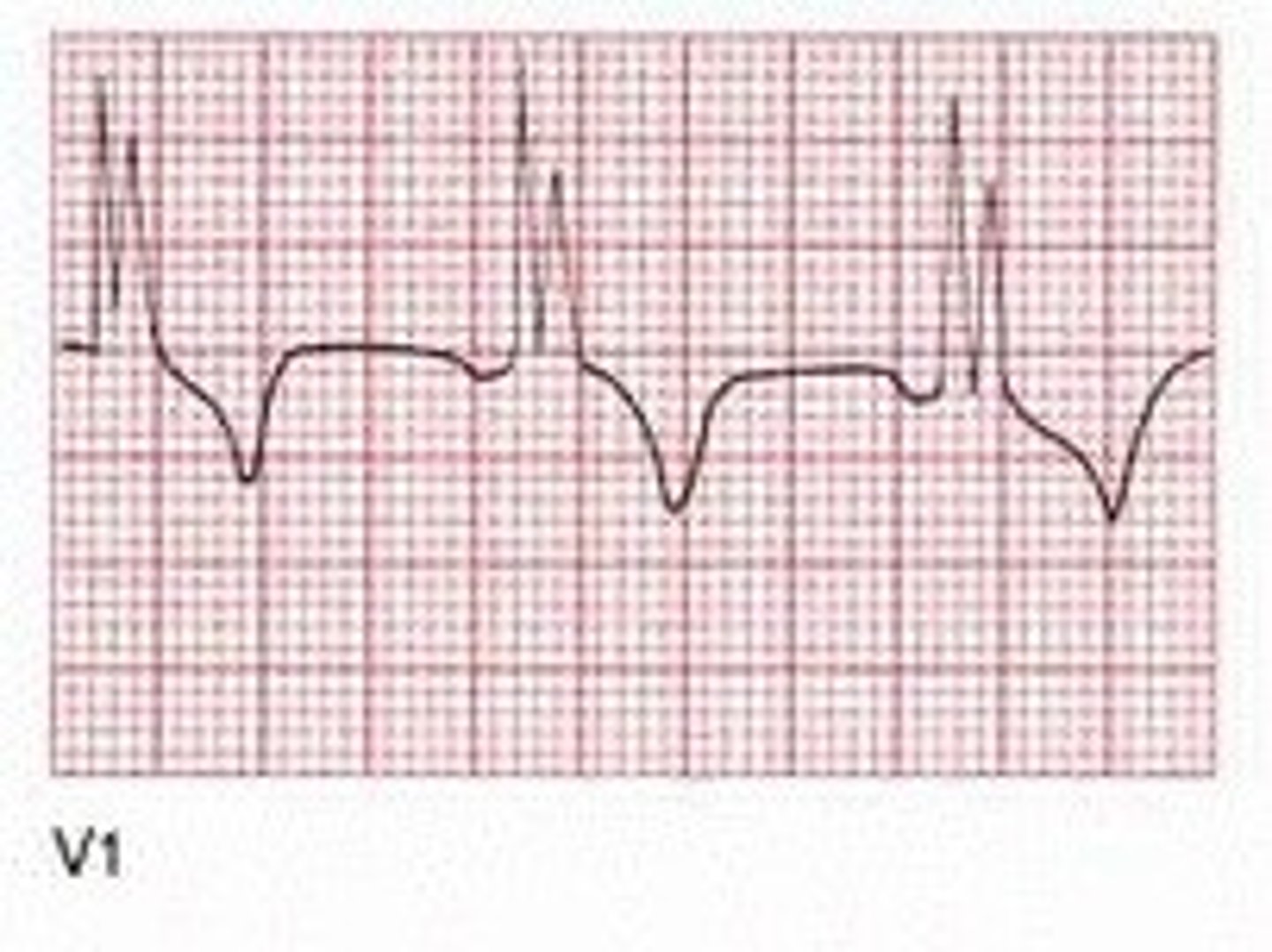
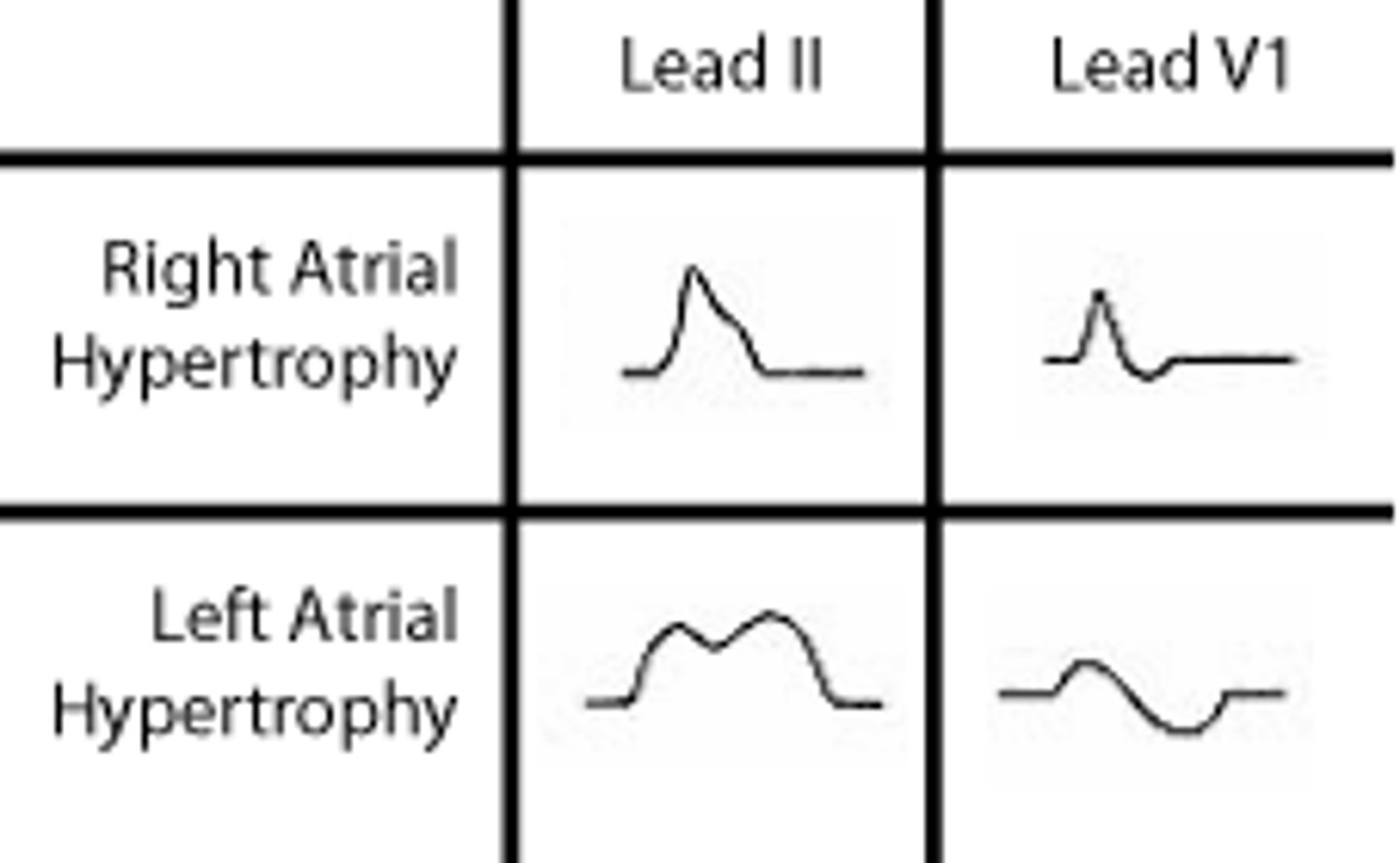
When assessing for atrial hypertrophy, which lead is most helpful to look at? What do we expect to see in right & left atrial hypertrophy, respectively?
Lead V1
Right hypertrophy: initial portion of diphasic p wave is larger
Left hypertrophy: terminal portion of diphasic p wave is larger
Which lead is most helpful to assess for right ventricular hypertrophy? What do we expect to see there?
Lead V1; large R wave > 7 small boxes (right ventricle wall is thicker so more depolarization energy towards this lead)
Which leads are most helpful for assessing left ventricular hypertrophy? What do we expect to see here?
Lead V1 & V5; deeper S wave in V1, large R wave in V5 (depth of S wave in V1 + height of R wave in V5 is > 35 mm (7 large boxes))
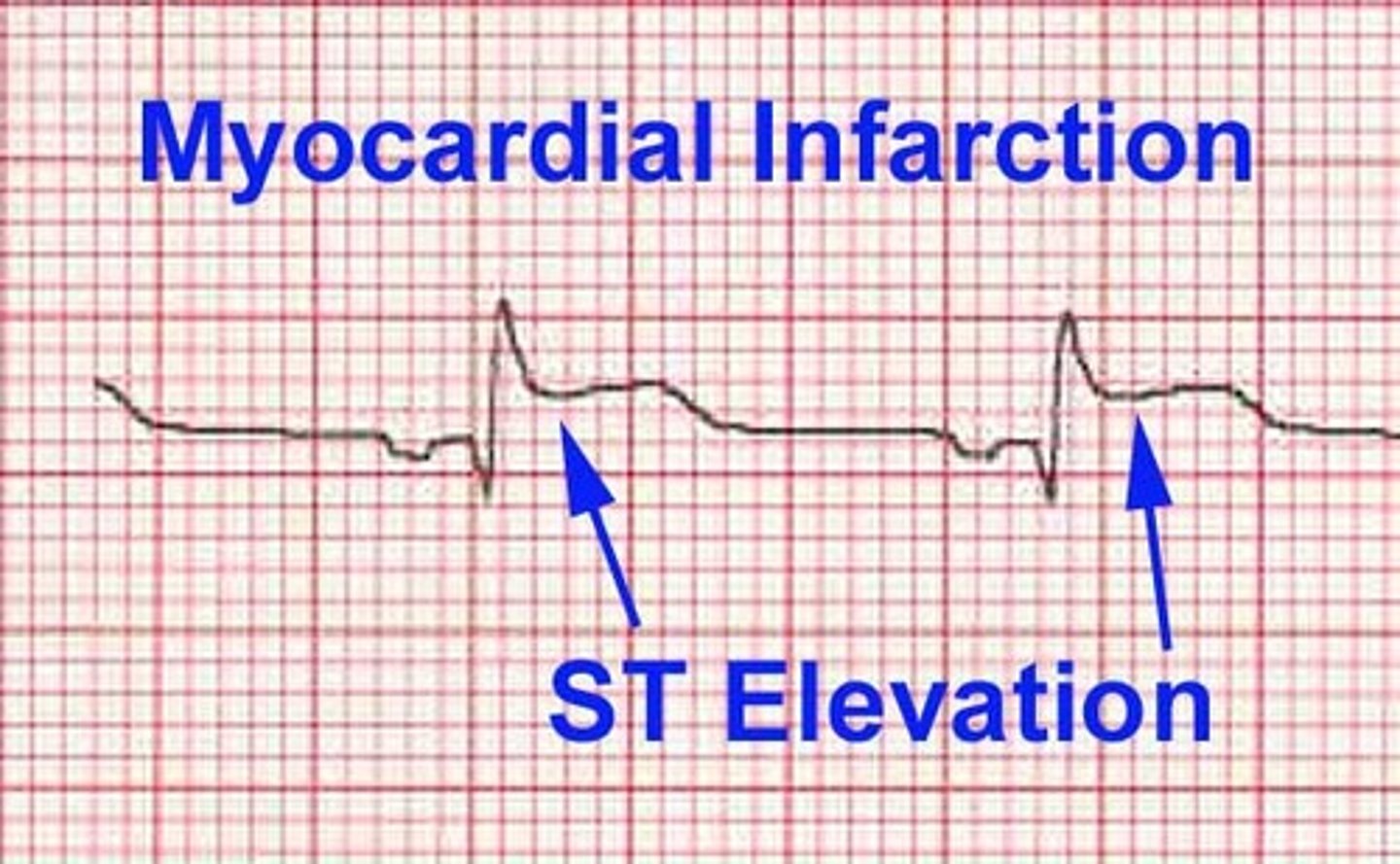
In general, what is a myocardial infarction (MI)?
Occlusion of a coronary artery producing a triad of ischemia, injury, & necrosis
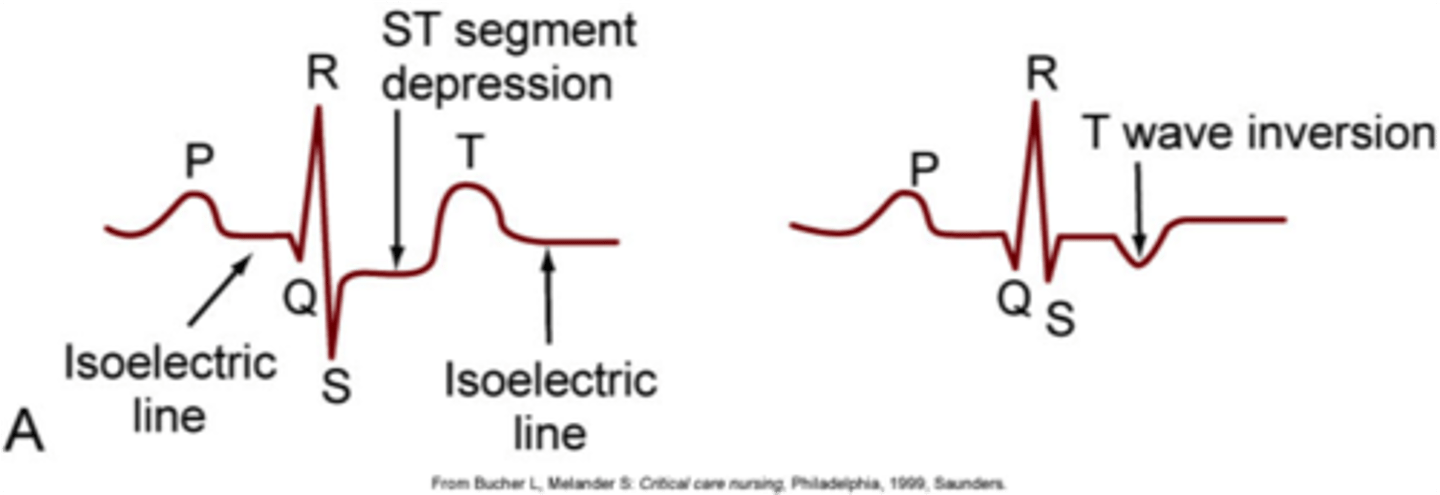
What are some characteristic signs of ischemia on ECG? Which leads are these seen best in?
Inverted T waves, ST segment depression; precordial leads (V1-V6) due to their position nearest to the ventricles, but any lead can be used
What is a characteristic sign of injury/infarct on ECG?
ST segment elevation (in any lead)
What is a characteristic sign of necrosis on ECG?
Significant Q wave (1 small box wide or 1/3 QRS amplitude)

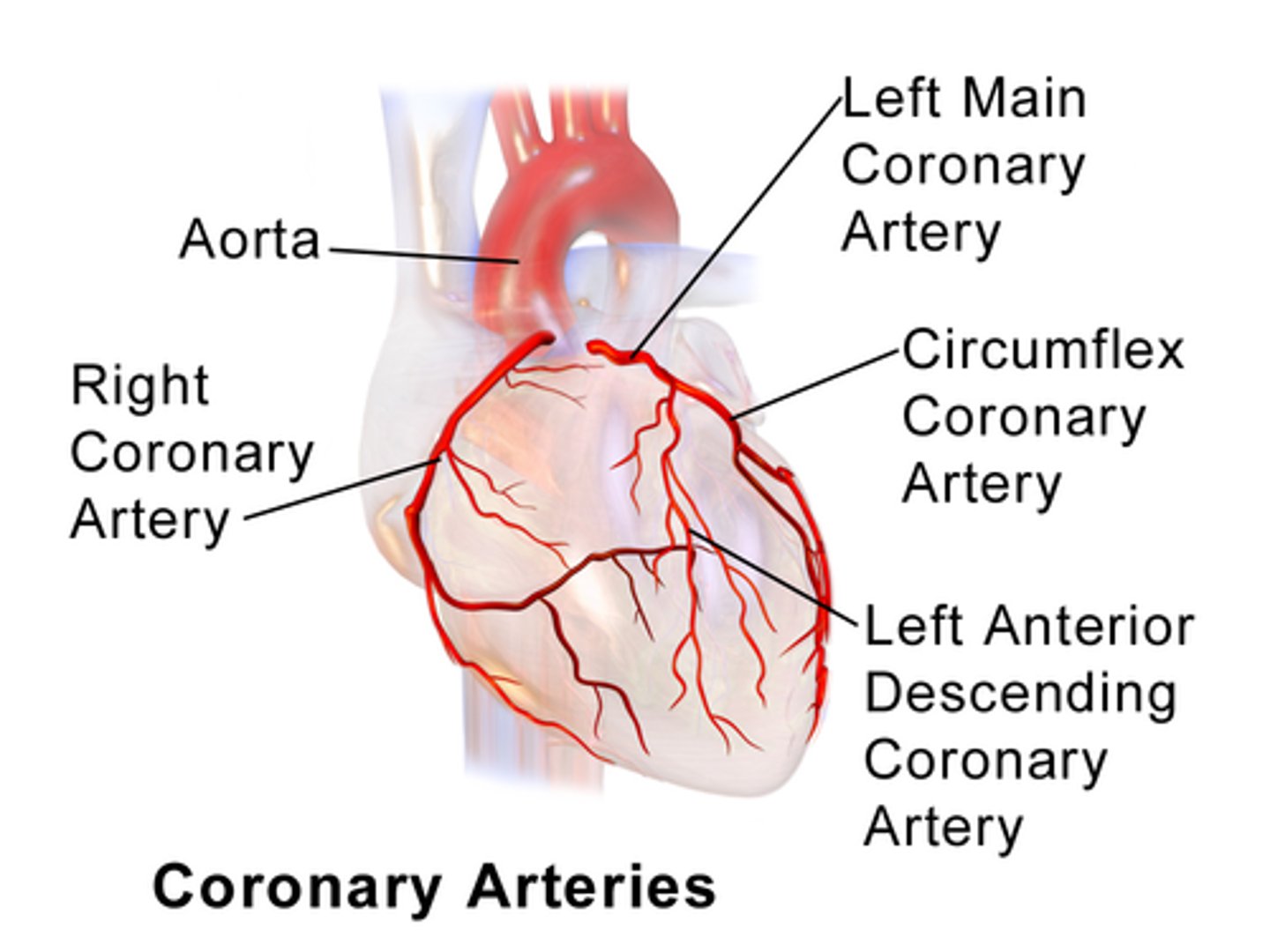
Which leads would we expect to see anterior MI signs in? Which artery/arteries does this likely involve?
V1-V4; LAD
Which leads would we expect to see anteroseptal MI signs in? Which artery/arteries does this likely involve?
V1 & V2; LAD
Which leads would we expect to see anterolateral MI signs in? Which artery/arteries does this likely involve?
I, AVL, V4-V6; LAD, circumflex
Which leads would we expect to see lateral MI signs in? Which artery/arteries does this likely involve?
I, AVL, V5, V6; circumflex
Which leads would we expect to see inferior MI signs in? Which artery/arteries does this likely involve?
II, III, AVF; right coronary (possibly left coronary artery too)
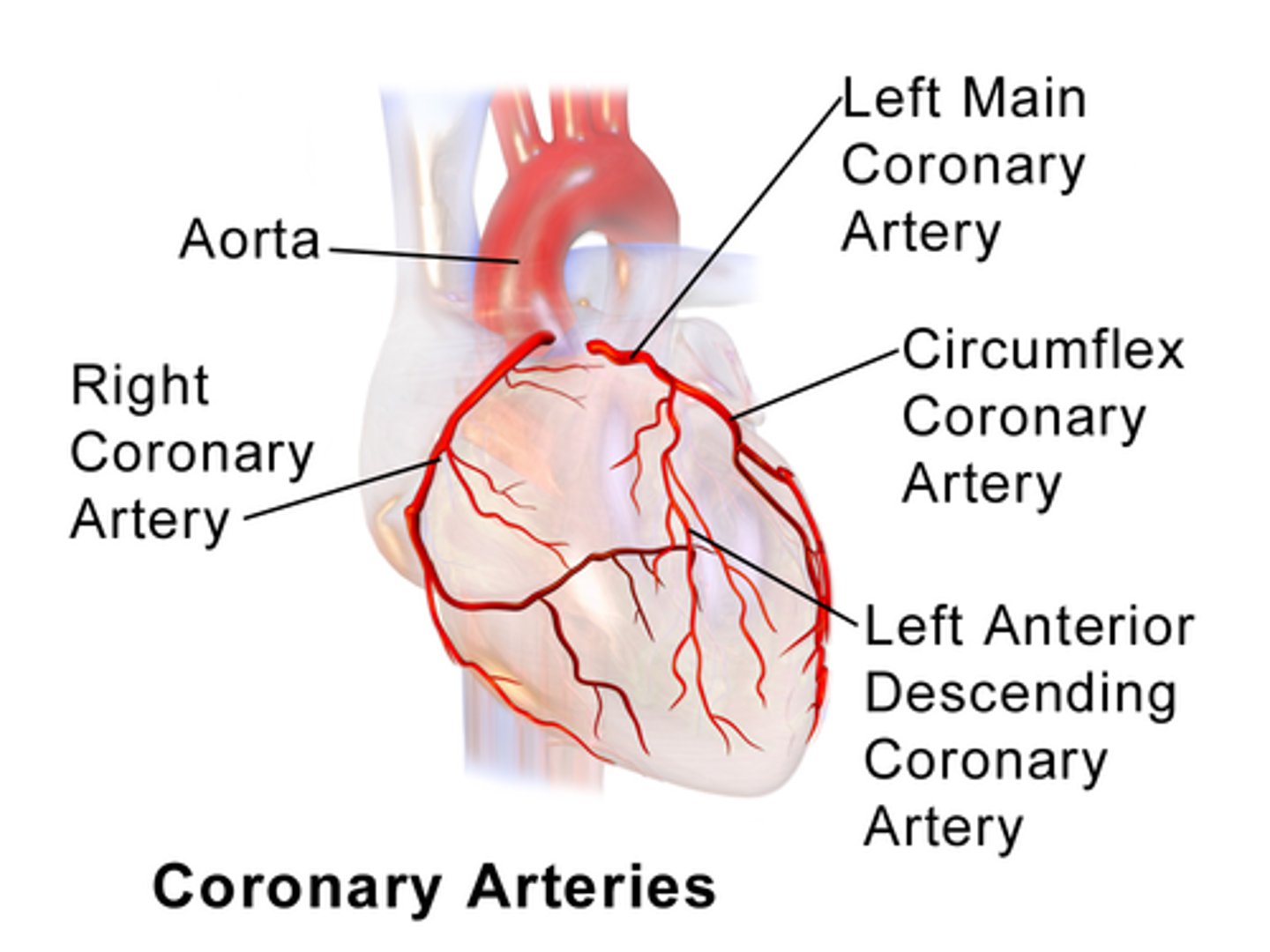
Which leads would we expect to see posterior MI signs in? Which artery/arteries does this likely involve?
Larger R & ST depression in V1 or V2; right coronary artery