Wrist and Hand Conditions
0.0(0)
Studied by 1 personCard Sorting
1/44
Last updated 1:45 PM on 10/24/22
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
45 Terms
1
New cards
general considerations
multiple articulations provide for wide range of movement
dexterity and precision-of-movement demands
integrity and balance of structures is key
dexterity and precision-of-movement demands
integrity and balance of structures is key
2
New cards
work-related musculoskeletal disorders (WRMD)
injuries or disorders of the muscles, nerves, tendons, joints, cartilage associated with exposure to risk factors in the workplace
account for 1/3 of all lost work days
WRMD of wrist and hand are associated with greater lost productivity than any other body region
account for 1/3 of all lost work days
WRMD of wrist and hand are associated with greater lost productivity than any other body region
3
New cards
conditions
ligament injuries: wrist sprain, dislocation, UCL injury to thumb
tendon injuries: DeQuervain's disease, intersection syndrome
trigger finger
rheumatoid arthritis
Dupuytren's disease
TFCC tear
Kienbock's disease
fractures
tendon lacerations
CTS
nerve injuries
complex regional pain syndrome (CRPS)
tendon injuries: DeQuervain's disease, intersection syndrome
trigger finger
rheumatoid arthritis
Dupuytren's disease
TFCC tear
Kienbock's disease
fractures
tendon lacerations
CTS
nerve injuries
complex regional pain syndrome (CRPS)
4
New cards
wrist sprain
hx of trauma (FOOSH), negative ulnar variance
scapho-lunate dissociation most common and significant wrist sprain
pain well localized
active/passive physiologic movements may be normal, palpatory tenderness common (end range mvmt, particularly ext -> pain)
scapho-lunate dissociation most common and significant wrist sprain
pain well localized
active/passive physiologic movements may be normal, palpatory tenderness common (end range mvmt, particularly ext -> pain)
5
New cards
scapholunate dissociation
traumatic injury -> fall
disruption of scapholunate ligament
radiographic fractures: widened SL interval (>4 mm)
clinical signs and sx: minimal swelling/pain localized over dorsal scapholunate region, pain with active wrist extension
disruption of scapholunate ligament
radiographic fractures: widened SL interval (>4 mm)
clinical signs and sx: minimal swelling/pain localized over dorsal scapholunate region, pain with active wrist extension
6
New cards
Terry Thomas sign
scapholunate dislocation/dissociation

7
New cards
MCP and IP joint dislocation
MOI: MCP - dorsally directed force
IP - axial loading during hyperextension
S&sx: pain, swelling, and stiffness (Grade I, II, III)
imaging may be indicated to r/o fx
Grade I - pain, swelling, no instability
Grade II - partial macro tear, increased joint play
Grade III - complete disruption, instability from basketball, volleyball
IP - axial loading during hyperextension
S&sx: pain, swelling, and stiffness (Grade I, II, III)
imaging may be indicated to r/o fx
Grade I - pain, swelling, no instability
Grade II - partial macro tear, increased joint play
Grade III - complete disruption, instability from basketball, volleyball
8
New cards
UCL of thumb
common hand injury in sports
can rupture from proximal phalange most common secondary to hyperabduction, hyperextension, or overuse
local pain and swelling in thenar web space, radial instability, dec pinch strength
radiograph should be requested
can rupture from proximal phalange most common secondary to hyperabduction, hyperextension, or overuse
local pain and swelling in thenar web space, radial instability, dec pinch strength
radiograph should be requested
9
New cards
tenosynovitis
involves synovial-lined tendon
inflammation of tendon sleeves
stenosing - sheaths become thickened and fibroses (tendon doesn't slide like it normally should)
inflammation of tendon sleeves
stenosing - sheaths become thickened and fibroses (tendon doesn't slide like it normally should)
10
New cards
tendonitis
acute, inflammation
11
New cards
tendinosis
longer term, fibrotic, less inflammation
12
New cards
tendinopathy
chronic tendon pathology, weakening of the tendon
13
New cards
tendonitis/tendinosis/tenosynovitis
any extrinsic tendon can be involved
most common: (1) 1st, 2nd, and 6th extensor compartments
(2) digital flexor tendons beneath A1 pulley (volar side of MCP, usually see trigger finger)
most common: (1) 1st, 2nd, and 6th extensor compartments
(2) digital flexor tendons beneath A1 pulley (volar side of MCP, usually see trigger finger)
14
New cards
flexor apparatus
5 annular and 3 cruciate pulleys
hold underlying tendons at fixed distance from joint (AOR)
allows for large ROM at fingers
*without pulleys, contraction of extrinsic finger flexors would pull tendons away from joint AOR*
paratenon - loose areolar connective tissue around tendon in areas of low mechanical stress
hold underlying tendons at fixed distance from joint (AOR)
allows for large ROM at fingers
*without pulleys, contraction of extrinsic finger flexors would pull tendons away from joint AOR*
paratenon - loose areolar connective tissue around tendon in areas of low mechanical stress
15
New cards
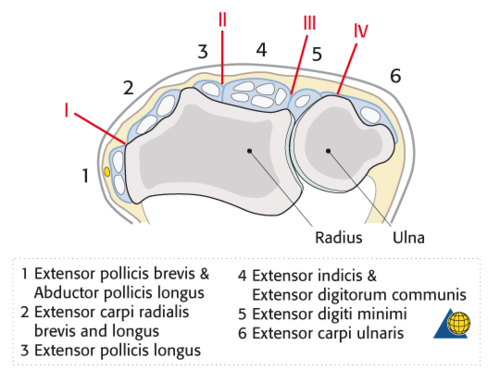
extensor compartments
1 - APL, EPB
2 - ECRL, ECRB
3 - EPL
4 - ED, EI
5 - EDM
6 - ECU
2 - ECRL, ECRB
3 - EPL
4 - ED, EI
5 - EDM
6 - ECU
16
New cards
DeQuervain's Disease
tenosynovitis 1st dorsal compartment
EPB and APL tendons
mechanism: repetitive movement (gamers, factory workers, musicians)
clinical signs incl swelling, decreased ROM, weakness of grip and pinch (tip to tip/chuck)
primary sx: pain radiating to forearm (point tender)
+Finkelstein's test
cluster of signs and sx
EPB and APL tendons
mechanism: repetitive movement (gamers, factory workers, musicians)
clinical signs incl swelling, decreased ROM, weakness of grip and pinch (tip to tip/chuck)
primary sx: pain radiating to forearm (point tender)
+Finkelstein's test
cluster of signs and sx
17
New cards
intersection syndrome
involves tendons of EPB, APL "intersecting" with ECRB and ECRL
MOI: repetitive movements - esp raking, shoveling, canoeing, kayaking
signs and sx: local pain, radiating pain to thumb or radial forearm
swelling
redness
crepitus
palpatory tenderness
MOI: repetitive movements - esp raking, shoveling, canoeing, kayaking
signs and sx: local pain, radiating pain to thumb or radial forearm
swelling
redness
crepitus
palpatory tenderness
18
New cards
trigger finger
signs and sx: morning stiffness, pain with gripping, palpable nodule palmar aspect of digit, inability to extend digit or popping sensation followed by release during extension
19
New cards
rheumatoid arthritis
begins with synovitis of distal RU joint
hand joints most commonly affected: MCP, IP of thumb (interferes w hand function - painful, weak, dec grip strength)
signs and sx: joint pain and swelling, tenderness to palpation rheumatoid nodules, constitutional sx (fever, fatigue, weight loss)
surgical mgmt: synovectomy, arthrodesis, arthroplasty
hand joints most commonly affected: MCP, IP of thumb (interferes w hand function - painful, weak, dec grip strength)
signs and sx: joint pain and swelling, tenderness to palpation rheumatoid nodules, constitutional sx (fever, fatigue, weight loss)
surgical mgmt: synovectomy, arthrodesis, arthroplasty
20
New cards
ulnar drift
common with rheumatoid arthritis
formation of inflammatory pannus, vascular tissue laid down inside synovium - causes distruction/erosion under bone and hyaline cartilage
doesn't tolerate standard loading, susceptible to micro fractures
try to interrupt inflammation with meds but meds --> immunocompromised
formation of inflammatory pannus, vascular tissue laid down inside synovium - causes distruction/erosion under bone and hyaline cartilage
doesn't tolerate standard loading, susceptible to micro fractures
try to interrupt inflammation with meds but meds --> immunocompromised
21
New cards
RA v OA
RA: thickened synovium --> breakdown of cartilage and surrounding bone, eroded cartilage, bone loss, less white and more dark on radiograph
OA: modest synovial changes, bone spurs, degenerated cartilage
OA: modest synovial changes, bone spurs, degenerated cartilage
22
New cards
Dupuytren's disease/palmer fascial fibromatosis
affects palmar fascia between skin and flexor tendons - begins as inflammatory fibrosis
palmar aponeurosis becomes adaptively shortened
MCP joint most frequently involved, then PIP
can be insidious, occurs in people prone to CT problems
PT mgmt: US, extension splints, stretching, maintain hand function
surgical mgmt: fasciectomy with progressive MCP contracture >30 degrees
palmar aponeurosis becomes adaptively shortened
MCP joint most frequently involved, then PIP
can be insidious, occurs in people prone to CT problems
PT mgmt: US, extension splints, stretching, maintain hand function
surgical mgmt: fasciectomy with progressive MCP contracture >30 degrees
23
New cards
TFCC injury
has poor blood supply (central 1/3rd vascular), capability of healing not good
MOI: axial loading to extended, pronated wrist (sprain or fx), ulnar sided distraction and torsion (golfing) repetitive axial loading
associated with positive ulnar variance, can -> breakdown of this structure
classified based upon traumatic v degenerative (9 diff subtypes based upon structures involved)
signs and sx: deep, ulnar-sided pain with pronation, supination, + gripping, + supination lift test, + TFCC shear, + TFCC grind
MOI: axial loading to extended, pronated wrist (sprain or fx), ulnar sided distraction and torsion (golfing) repetitive axial loading
associated with positive ulnar variance, can -> breakdown of this structure
classified based upon traumatic v degenerative (9 diff subtypes based upon structures involved)
signs and sx: deep, ulnar-sided pain with pronation, supination, + gripping, + supination lift test, + TFCC shear, + TFCC grind
24
New cards
TFCC contents
triangular fibrocartilaginous disc and meniscus homolog
-TFC attaches to hyaline cartilage radially making it vulnerable to injury
extensor carpi ulnaris subsheath
ulnotriquetral and ulnolunate ligaments
dorsal and volar distal radioulnar ligaments
ulnocarpal collateral ligament
*do not need to know exactly what's causing the issue in the TFCC
-TFC attaches to hyaline cartilage radially making it vulnerable to injury
extensor carpi ulnaris subsheath
ulnotriquetral and ulnolunate ligaments
dorsal and volar distal radioulnar ligaments
ulnocarpal collateral ligament
*do not need to know exactly what's causing the issue in the TFCC
25
New cards
Kienbock's disease
necrotic changes in lunate d/t loss of blood supply
associated with negative ulnar variance
most common in men 20-40 y/o
signs and sx: wrist pain and swelling, palpatory tenderness of lunate, impaired wrist ROM and strength
surgical management common (bone graft)
associated with negative ulnar variance
most common in men 20-40 y/o
signs and sx: wrist pain and swelling, palpatory tenderness of lunate, impaired wrist ROM and strength
surgical management common (bone graft)
26
New cards
fractures
Galeazzi
Colles
Smith's
Scaphoid
Bennett's
Boxer's
Barton's
Kienbock's
Colles
Smith's
Scaphoid
Bennett's
Boxer's
Barton's
Kienbock's
27
New cards
distal radial fx
most common fx
75-80% minimally displaced: 6-8 weeks of immobilization
25% are complex and unstable - high impact and require surgical mgmt and rigid fixation (ORIF), longer immobilization, prolonged rehab
75-80% minimally displaced: 6-8 weeks of immobilization
25% are complex and unstable - high impact and require surgical mgmt and rigid fixation (ORIF), longer immobilization, prolonged rehab
28
New cards
Galeazzi fx
distal radius fx with dislocation of the distal RU joint
requires ORIF
potential for compartment syndrome involving anterior interosseous nerve
-symptoms: no sensory innervation, motor n - FPL, PQ, flexor compartment
requires ORIF
potential for compartment syndrome involving anterior interosseous nerve
-symptoms: no sensory innervation, motor n - FPL, PQ, flexor compartment
29
New cards
colle's fx
involves distal radius with dorsal displacement of distal fragment and radial shift of carpus and hand
extra-articular
external or internal fixation
5-8 weeks healing time
may lead to complex regional pain syndrome (CRPS)
"silver fork deformity"
dorsal angulation about 30 degrees
extra-articular
external or internal fixation
5-8 weeks healing time
may lead to complex regional pain syndrome (CRPS)
"silver fork deformity"
dorsal angulation about 30 degrees
30
New cards
smith's fx
involves distal radius with volar displacement of distal fragment (reverse Colle's fx)
MOI fall onto flexed wrist or direct blow
5-9 weeks healing time
usually an extraarticular transverse fx
internal fixation likely
MOI fall onto flexed wrist or direct blow
5-9 weeks healing time
usually an extraarticular transverse fx
internal fixation likely
31
New cards
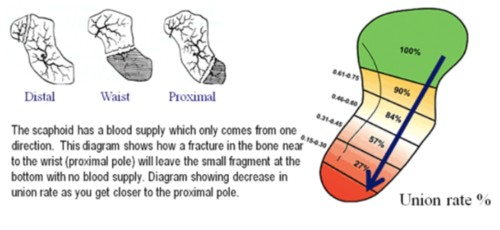
scaphoid fx
represents 60% of all carpal fx; 2-7% of all fxs
FOOSH injury
avascular necrosis is a common complication (~30%) due to poor blood supply (in fx proximal to waist)
-70-80% occur through scaphoid waist (moderate AVN risk)
-20% occur through proximal pole (high incidence of AVN)
-10% occur through distal pole (low incidence of AVN)
capitate and lunate dislocations are commonly associated
FOOSH injury
avascular necrosis is a common complication (~30%) due to poor blood supply (in fx proximal to waist)
-70-80% occur through scaphoid waist (moderate AVN risk)
-20% occur through proximal pole (high incidence of AVN)
-10% occur through distal pole (low incidence of AVN)
capitate and lunate dislocations are commonly associated
32
New cards
scaphoid blood supply
X-ray every week or two
looking for evidence of healing
if not - bone graft
looking for evidence of healing
if not - bone graft
33
New cards
avascular necrosis of scaphoid

34
New cards
Bennet's fx
fracture and displacement of 1st MC from the proximal end
oblique intra-articular fx
tension of AbPL sublimes fragment in dorsal, radial, and proximal direction -> tension from AdP displaces fragment into palm
MOI: trauma (ie football), high impact sports
oblique intra-articular fx
tension of AbPL sublimes fragment in dorsal, radial, and proximal direction -> tension from AdP displaces fragment into palm
MOI: trauma (ie football), high impact sports

35
New cards
Boxer's fx
fx of the neck of the 5th MC
results in acute angulation of the head of the MC into palm
mechanism of injury - typically punching a wall, not a seasoned boxer
results in acute angulation of the head of the MC into palm
mechanism of injury - typically punching a wall, not a seasoned boxer

36
New cards
flexor tendon injuries
second most common injury to hand
tendon disruption: varies from clean cut/tear to untidy injury with blood vessel and nerve damage
delayed repairs involve artificial tendons or graft (palmaris longus)
early mobilization is advantageous to facilitate collagen remodeling (if don't get them moving, risk fibrotic hand tissue)
tendon disruption: varies from clean cut/tear to untidy injury with blood vessel and nerve damage
delayed repairs involve artificial tendons or graft (palmaris longus)
early mobilization is advantageous to facilitate collagen remodeling (if don't get them moving, risk fibrotic hand tissue)
37
New cards
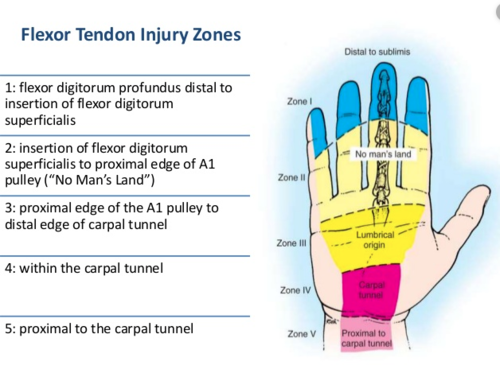
flexor tendon injury zones
1 - flexor digitorum profundus distal to insertion of flexor digitorum superficialis
2 - insertion of flexor digitorum superficialis to proximal edge of A1 pulley ("no man's land")
3 - proximal edge of A1 pulley to distal edge of carpal tunnel
4 - within the carpal tunnel
5 - proximal to the carpal tunnel
2 - insertion of flexor digitorum superficialis to proximal edge of A1 pulley ("no man's land")
3 - proximal edge of A1 pulley to distal edge of carpal tunnel
4 - within the carpal tunnel
5 - proximal to the carpal tunnel
38
New cards
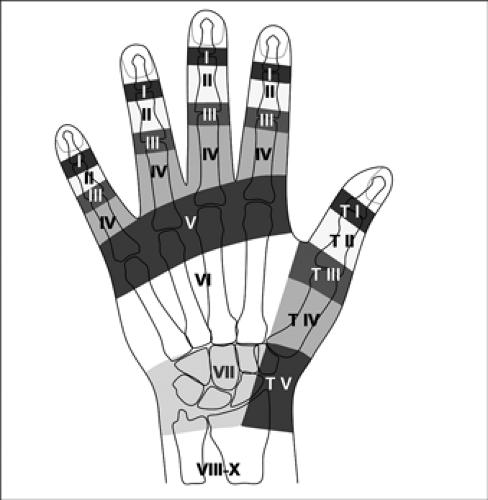
extensor tendon repairs
surgical repairs are much more common for extensor injuries
tx is less complex and healing response is greater as compared to flexor injuries
7 zones identified to classify injury
easier to manage d/t less complex nature of anatomy
tx is less complex and healing response is greater as compared to flexor injuries
7 zones identified to classify injury
easier to manage d/t less complex nature of anatomy
39
New cards
carpal tunnel syndrome
causes include radioulnar, radoiocarpal, and carpal fx; swelling of nerve, swelling of flexor tendon sheaths and anatomic variants
sx include numbness and tingling, pain (night), and weakness
signs incl dec sensation (median n. distribution), atrophy of thenar mms (1/2 FBP, OP, 1st and 2nd lumbricals), + phalen's and tinel's test
NCV testing results (look for latency - takes longer for impulse to travel down axon)
sx include numbness and tingling, pain (night), and weakness
signs incl dec sensation (median n. distribution), atrophy of thenar mms (1/2 FBP, OP, 1st and 2nd lumbricals), + phalen's and tinel's test
NCV testing results (look for latency - takes longer for impulse to travel down axon)
40
New cards
CPR for CTS
shaking hands relieves sx
wrist-ratio index >.67 (AP/ML width)
symptom severity scale (SSS) >1.9
age >45
reduced sensory field of 1st digit (in median n. distribution)
>/= 3 positive: +LR = 2.1
>/= 4 positive: +LR = 4.6
all 5 positive: +LR = 18.3
wrist-ratio index >.67 (AP/ML width)
symptom severity scale (SSS) >1.9
age >45
reduced sensory field of 1st digit (in median n. distribution)
>/= 3 positive: +LR = 2.1
>/= 4 positive: +LR = 4.6
all 5 positive: +LR = 18.3
41
New cards
ulnar n. compression
occurs at guyon's canal - formed by pisiform, volar carpal ligament and transverse carpal ligament
-extends ~4cm to hook of hamate
commonly caused by direct pressure on handlebar with biking
clinical signs: loss of sensation (ulnar distribution) and weakness of the ulnar 2 lumbricals, hupothenar mms, interossei, dep head FPB, AddP
-extends ~4cm to hook of hamate
commonly caused by direct pressure on handlebar with biking
clinical signs: loss of sensation (ulnar distribution) and weakness of the ulnar 2 lumbricals, hupothenar mms, interossei, dep head FPB, AddP
42
New cards
complex regional pain syndrome (CRPS)
AKA: reflex sympathetic dystrophy (RSD) or causalgia
hallmark is vasomotor dysfunction
pain is the primary sx
involves an abnormal sympathetic reflex
three characteristic phases
hallmark is vasomotor dysfunction
pain is the primary sx
involves an abnormal sympathetic reflex
three characteristic phases
43
New cards
CRPS phase I
acute phase of injury
pain and edema primary sx
discoloration of the hand develops
hyperhydrosis also develops
approximately 3 months duration
pain and edema primary sx
discoloration of the hand develops
hyperhydrosis also develops
approximately 3 months duration
44
New cards
CRPS phase II
subacute
pain and edema remain primary sx
pale cyanosis reduces redness (more straightforward vasoconstriction)
dry skin
skin and subcutaneous tissue atrophy
3-12 months
pain and edema remain primary sx
pale cyanosis reduces redness (more straightforward vasoconstriction)
dry skin
skin and subcutaneous tissue atrophy
3-12 months
45
New cards
CRPS phase III
marked joint stiffness
thickening of palmar fascia
osteoporosis
skin and subcutaneous atrophy more severe - hand deformity
skin is dry, pale and shiny
pain may continue or begin to subside
(lacks hair growth)
thickening of palmar fascia
osteoporosis
skin and subcutaneous atrophy more severe - hand deformity
skin is dry, pale and shiny
pain may continue or begin to subside
(lacks hair growth)