Lecture 40-42: Infectious Agents of the Respiratory Tract
1/99
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
100 Terms
Upper Respiratory Tract Infection (URTI)
• Involve nose, sinuses, larynx, pharynx
• Self-limited irritation and swelling of upper airways with associated cough
• No signs of pneumonia
• Patient has no other condition to account for symptoms (COPD, emphysema, chronic bronchitis)
Lower Respiratory Tract Infection (LRTI)
• Involve trachea, bronchi, bronchioles, lungs
• Generally more severe
• Coughing is primary symptom
Pneumnonia
-inflammation fo the lung parenchyma due to infection
-causes alveoli to fill with fluid or pus
-leading cause of death in children <5
Pneumonia
-pts present with productive cough, dyspnea, chest pain, and possibly hemoptysis
-fever, malaise, myalgias, weight loss
-CXR shows parenchymal opacity
Bacterial
the usual cause of lobar pneumonia is _________________
Staphylococcus
-grape like clusters
-beta hemolytic
-catalase positive
-novobiocin sensitive
-coagulase negative
-located on skin
Streptococcus
-short chains
-requires enriched media
-alpha, beta, or gamma hemolysis
-catalase negative
-coagulase negative
-located in nose and throat
S. pyogenes
1

S. agalactiae
2

S. pneumonaie
3

Streptococcus pneumoniae
most common cause of community-acquired pneumonia
Streptococcus pneumoniae
-fastidious, gram positive, alpha hemolytic, catalase negative
-sensitive to optochin and bile salts
-Quellung reaction
-Common inhabitant of respiratory tract
Streptococcus pneumoniae
-assoc with rust-colored sputum
risk factors:
- >65yo
- <2 yo
-smoking and alcohol abuse
-asthma or COPD
-asplenic
Streptococcus pneumoniae
Virulence Factors:
-capulse
-Pneumolysin
-IgA1 protease
-Neuraminidase
Streptococcus pyogenes
-gram positive cocci in chains
-beta hemolytic
catalase negative
-coagulase negative
-facultative anartobe (Group A)
Streptococcus pyogenes
-Colonizes mucosal membranes
-transmitted by droplets, fomites, direct contact, contaminated food
-diagnosed by culture or rapid antigen detection
Streptococcus pyogenes
• Suppurative: pharyngitis, skin infection, abscess, otitis media
• Toxin-mediated: scarlet fever, toxic shock syndrome
• Autoimmune: rheumatic fever, acute glomerulonephritis, PANDAS (controversial)
Streptococcus pyogenes
Virulence Factors:
-hyaluronic acid capsule
-M proteins
-Streptokinase
-Hyaluronidase
-Hemolytic Toxins: Streptolysin S and O
-C5a peptidase
-Protein F
-Pyrogenic exotoxins
Streptococcus agalactiae
-Gram positive cocci in chains
-catalase negative
-beta hemolytic
-colonizes genital and GI tracts
Streptococcus agalactiae
Important cause of infection in 3 groups:
• Neonates – sepsis, pneumonia, meningitis
• Pregnant women – UTI, chorioamnionitis, postpartum endometriosis, bacteremia
• Nonpregnant adults – sepsis, soft tissue infection, other focal infections
Neonates present with:
• Fever, difficulty feeding, irritability, lethargy
• Respiratory symptoms (tachypnea, grunting, hypoxia, increased work of breathing)
Streptococcus agalactiae
Virulence Factors:
-capsule polysaccharides
-C5a peptidase, beta-hemolysin, superoxide dismutase
-lipoteichoic acid, hyaluronin, pili
Haemophilus influenzae
-Pleomorphic Gram-negative rods, facultative anaerobes, oxidase positive
-Colonizes respiratory tract; humans only known reservoir
• Grows on chocolate agar
-6 typeable strains (a-f) have capsules; nontypeable strains do not
Haemophilus influenzae
• In areas with routine vaccination
• More common to see nontypeable strains; respiratory tract
infections
•causes meningitis and epiglottitis in kids, pneumonia in adults
• Epiglottitis can lead to potentially fatal airway obstruction
• While incidence has decreased since vaccinations, median age at presentation has increased from 3 years to 6-12 years old
Mycoplasma pneumoniae
• Very small, short rod with no cell wall, fastidious; atypical pathogen
• Doesn't Gram stain, difficult to culture
• Lack of cell wall makes bacteria highly pleomorphic
Mycoplasma pneumoniae
• Causes atypical (walking) pneumonia, more commonly in young
children
• Also causes upper respiratory infections and bronchitis
• Transmitted via respiratory droplets; rates rise in the summer
• Associated with autoimmune hemolytic anemia due to cold agglutinins
• M. pneumoniae changes antigen on RBC, leads to IgM autoantibody production
Mycoplasma pneumoniae
Virulence factors:
• Produces hydrogen peroxide and superoxide which injure epithelial cells
• Adherence proteins (P1, P30)
• TLR2 activation leads to inflammatory cytokine production
• CARDS toxin damages epithelial cells
M. tuberculosis
• Human pathogen, no known reservoir
• Latent infection in immunocompetent patients; controlled by cell mediated immune response
• Diagnosed by +PPD skin test
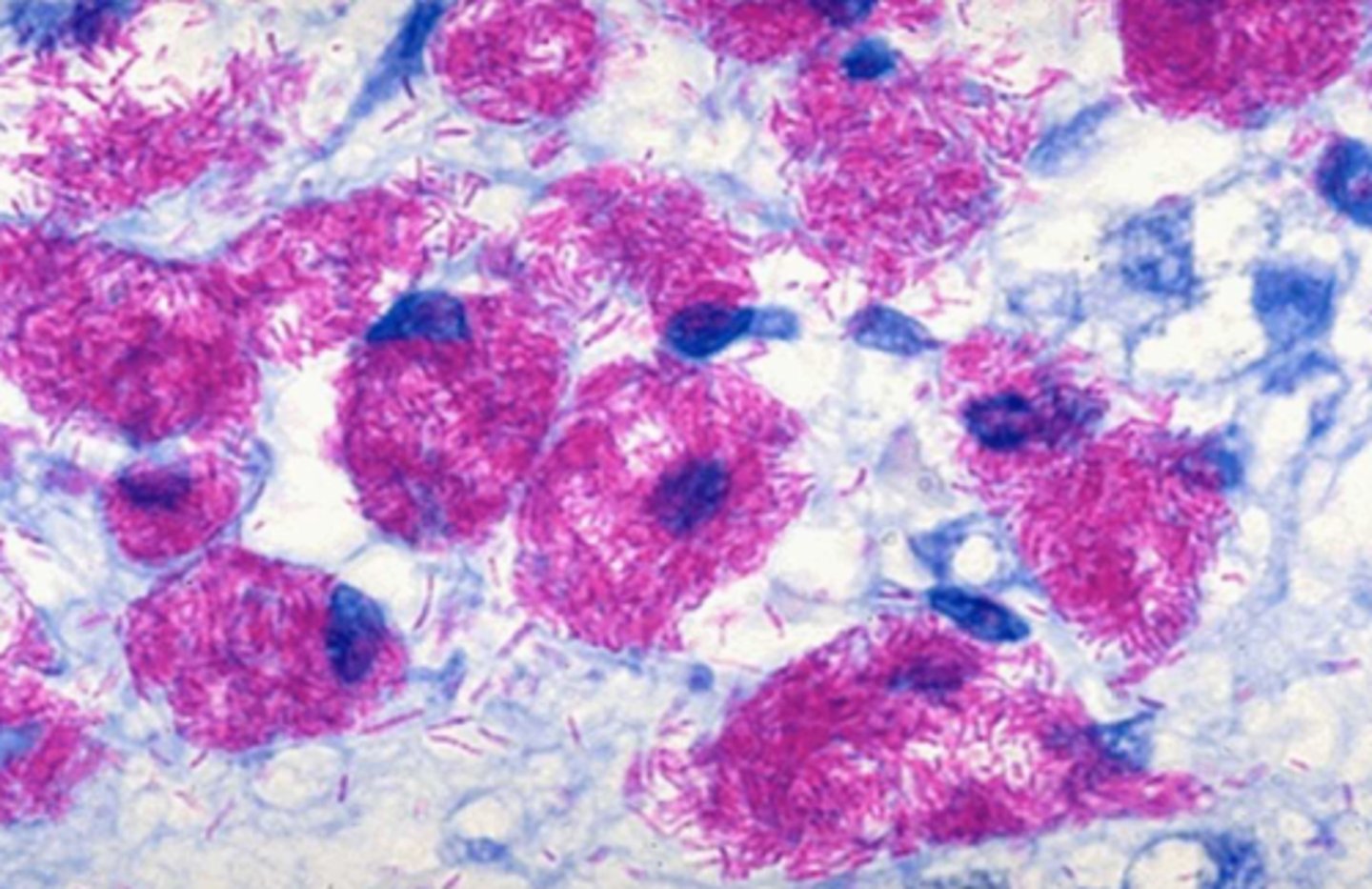
Mycobacterium spp.
• Acid-fast bacilli, slow growing
• Stain with Ziehl-Neelsen or carbol-fuchsin
• Acid-fast bacilli, slow growing
• Stain with Ziehl-Neelsen or carbol-fuchsin
Virulence factors:
• High mycolic acid content makes phagocytosis difficult;
bacteria live inside macrophages
• Cord factor elicits granuloma formation, promotes survival in
macrophages by preventing phagolysosome fusion
• Catalase peroxidase protects from ROS
• Lipoarabinomannan (LAM) is a TLR2 ligand, induces
cytokine production
M. avium complex (MAC)
-M. avium and M. intracellulare
-causes progressive pulmonary disease associated with bronchiectasis or COPD in older patients
-Disseminated infections in AIDS patients
M. avium complex (MAC)
-n opportunistic pathogen, but results from
recent acquisition
• No latent infections
• Can also cause GI and skin/soft tissue infections
-• Biofilm formation, inhibition of cytokine production promote colonization/invasion
M. avium complex (MAC)
Pseudomonas aeruginosa
• Motile, aerobic Gram-negative rod, nonfermenting, ubiquitous in the environment
• Characteristic grape-like odor
• Polar flagellum
• Blue-green pigment (pyocyanin)
Pseudomonas aeruginosa
mportant cause of nosocomial infections:
• Colonization of CF patients
• Wound infections in burn patients
• Ventilator associated pneumonia
• UTI due to indwelling catheters
Pseudomonas aeruginosa
Virulence factors - there are a ton:
• Lives everywhere and forms biofilms (hard to get rid of)
• Exotoxins S, U, and Y (type III secreted toxins)
Klebsiella pneumoniae
Pseudomonas aeruginosa

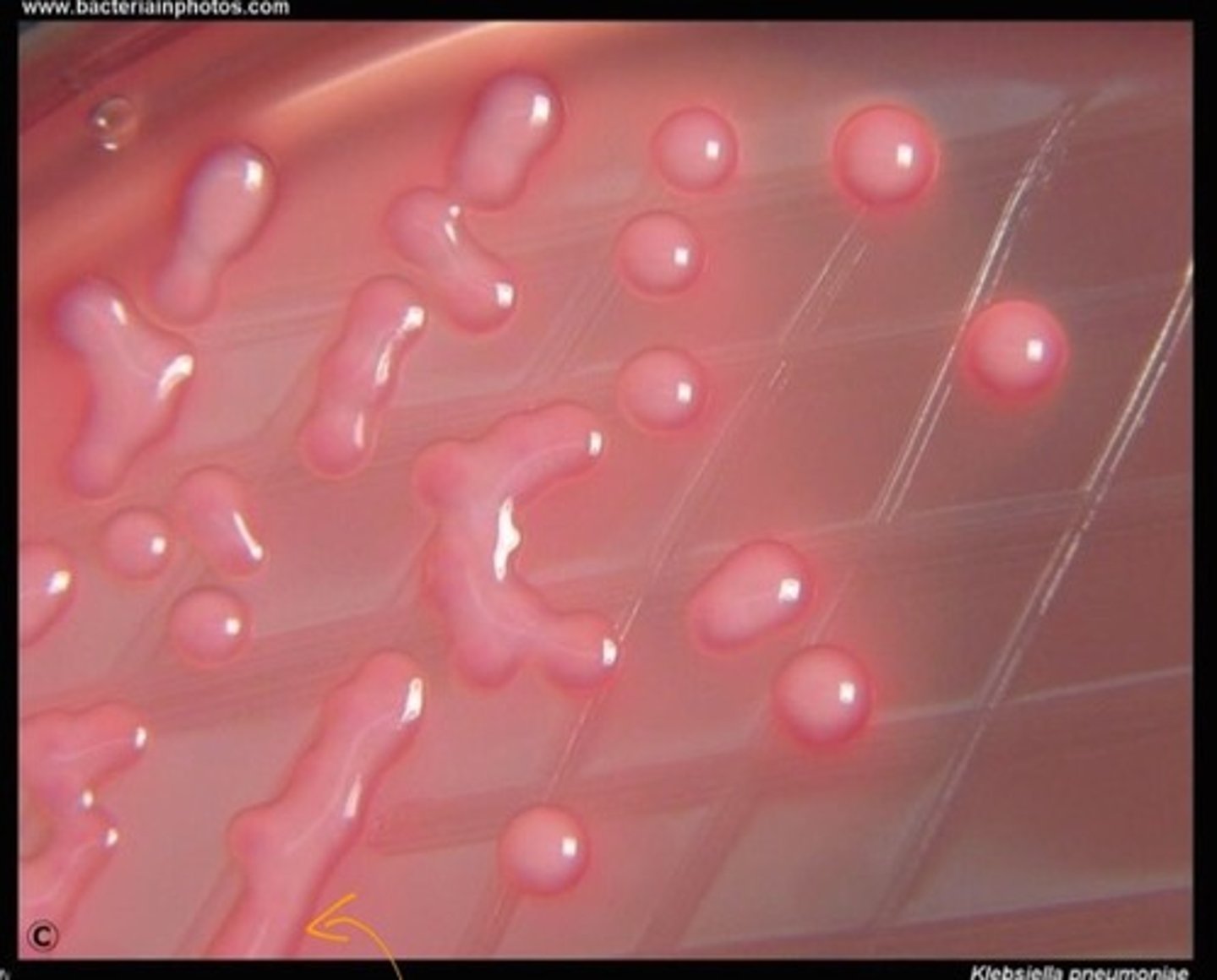
Klebsiella pneumoniae
• Gram-negative rod, encapsulated, lactose fermenting
• Pink mucoid colonies on MacConkey agar
• Positive Voges-Proskauer (VP) reaction
• Member of Enterbacteriaceae family
Klebsiella pneumoniae
• Infections usually hospital-acquired, in immunocompromised patients
• Pneumonia, UTI, bacteremia
• Red currant jelly sputum
Klebsiella pneumoniae
Virulence factors:
• Capsule protects from phagocytosis
• Biofilms
• LPS acts as endotoxin, provides serum resistance
• Siderophores are iron chelators
• Pili/fimbriae mediate adherence
• Some strains produce ESBL
Bordetella pertussis
• Fastidious Gram-negative coccobacilli
• Humans only known reservoir
• Transmitted by respiratory droplets; risk highest during catarrhal stage
Bordetella pertussis
Cause of whooping cough
Legionella pneumophila
• Pleomorphic Gram-negative rods, fastidious, intracellular pathogen
• Gram stain poorly; can use silver or Giemsa stain
• Culture on buffered charcoal yeast extract (BCYE) agar
• Transmitted by aerosols from contaminated water
Legionella pneumophila
• Cause community-acquired and nosocomial pneumonia (Legionnaire’s disease)
• Diagnosed by looking for antigens in urine
• Can be sporadic infections or outbreaks
• Also causes Pontiac fever
• Acute, self-limited febrile illness
• Short incubation period, rapid recovery
• Thought to be toxin mediated
Legionella pneumophila
Virulence and immune escape:
• Bacteria inhibit phagolysosome fusion, multiply inside macrophages
Rececptor mediated endocytosis
how do naked viruses get into the host cell
Membrane fusion
how do enveloped viruses get into the host cell
Rhinovirus
• Small naked viruses, +ssRNA genome
• Part of Enterovirus genus and Picornaviridae family
• >160 rhinoviruses, classified RV-A, B, and C
• Most common cause of URTI across all age groups
• Host cell receptors: ICAM-1 (CD54): RV-A, RV-B
Rhinovirus
Temperature restrictions:
• _________________ replicates most effectively at 33°C; why they prefer
upper respiratory tract
• Host cell response is more efficient at higher temps
Coronavirus
• Medium enveloped viruses, +ssRNA genome
• Spike proteins extend from capsid, looks like a crown
• Spike proteins bind host receptors; major antigen for neutralizing antibodies
Coronarvirus
• Causes colds; cases increase in winter
• Bind to sugars on glycoproteins (low affinity binding)
SARS virus and MERS virus
• Cause pneumonia
• ACE2 is the SARS receptor, CD26 is the MERS receptor
Adenovirus
• Naked dsDNA virus
• Naked viruses survive longer in the environment; can be transmitted without close contact
• Cause wide range of infections (respiratory, ocular, GI)
• Usually self-limited, but can cause serious illness in immunocompromised patients
Adenovirus
3 major capsid antigens:
• Fiber protein binds CAR (host receptor);
• Can hemagglutinate RBC
• Penton base interacts with host integrins and mediates virus
internalization
• Hexon is the major viral surface protein; contains antigenic
determinants and determines tissue tropism
Paramyxovirus
• Enveloped -ssRNA viruses
-measles and mumps
Paramyxovirus
2 viral proteins are key to infection:
• Hemagglutinin mediates attachment to host
receptor (α2,3 sialic acid); varies among
paramyxoviruses
• Fusion protein causes membrane fusion,
releasing virus into host cell and causing
syncytia formation
Measles
• AKA rubeola
• Fever, malaise, cough, coryza, conjunctivitis, then rash
• Koplik spots are pathognomonic for measles
Measles
• Diarrhea is most common complication
• Pneumonia is most common cause of ________________ assoc death in children
• Encephalitis, acute disseminated encephalomyelitis, subacute sclerosing panencephalitis
• Can lead to immune suppression and secondary infections (bacteremia, pneumonia,
gastroenteritis)
-depletes T and B cells
Mumps
-Presents with fever, headache, myalgia, fatigue, anorexia, then parotitis
• Complications include orchitis, meningitis, encephalitis, and deafness
• Most commonly in school age children and college aged young adults
Mumps
-virus prefers glandular epithelium
-viral replication in parotid gland leads to local inflammtion and infilatration of macrophages and lymphocytes, causing swelling
Croup
• Presents with inspiratory stridor, cough, and hoarseness (laryngotracheitis)
• Infants and young children: barking cough
• Older children and adults: hoarseness
Croup
• URT symptoms first, then LRT symptoms
• Most common in children 6 months-3 years old; usually in fall or winter
• Anatomic hallmark is narrowing of subglottic airway (steeple sign)
Parainfluenza virus type 1
most common cause of croup
Respiratory Syncytial Virus (RSV)
• -ssRNA virus; A and B subtypes
• Can cause severe disease in infants, older and immunocompromised adults
• Risk factors: premature birth, asthma, cardiopulmonary disease, secondhand smoke
• Bronchiolitis in infants
• Pneumonia, bronchitis, asthma/COPD exacerbations in adults
Respiratory Syncytial Virus (RSV)
• Infection doesn't generate immunity to reinfection
• Viral infection can cause inflammatory response that promotes asthma
• Synagis (palivizumab) is a mAb against F protein given monthly during ____________ season
• Only for high-risk infants
• No lasting protection, very expensive
Influenza
• Enveloped virus with segmented, -ssRNA genome; part of Orthomyxoviridae family
• M2 protein is an ion channel that allows intracellular
virus to replicate and exocytose
• Antiviral therapies: Zanamivir, oseltamivir target neuraminidase, Amantidine, rimantadine target M2
Influenza A
-characterized by hemagglutinin (H) and neuraminidase (N) proteins
• H binds to sialic acids on respiratory epithelium
Antigenic drift
• Minor changes in antigens
• Leads to seasonal epidemics
• Occurs as result of error prone replication
• Existing antibodies may be cross-protective
Antigenic Shift
• Completely new antigens
• Leads to pandemics
• Occurs as result of combining RNA segments
from 2 different strains in one host cell
• There are no pre-existing antibodies
Hantavirus
• Enveloped virus with segmented -ssRNA genome, Bunyaviridae family
• Transmitted by inhaling dried rodent urine/feces or by rodent bite
• Most common in SW U.S. and South America
Hantavirus
• Causes hemorrhagic fevers, acute respiratory distress syndrome (ARDS), and renal failure
• GI symptoms may help distinguish HCPS or HPS from other illnesses
Mold; yeast
In relation to fungi:
usually ____________ in environement, and ______________ in host
Pneumocystis jiroveci
• Opportunistic pathogen
• Risk factors: AIDS, glucocorticoids, chemotherapy, cancer,
other immunosuppressive meds
• Interstitial pneumonia with plasma cell infiltrates and
foamy alveolar exudate
• Ground glass on X-ray
• Hypoxemia at rest or with exertion; ↑ A-a O2 gradient
Pneumocystis jiroveci
• LDH may be elevated
• Presence of beta-D-glucan
• PCR of bronchoalveolar lavage fluid
• Visualize fungi with Gomori-methenamine silver or other stains
Aspergillus fumigatus
• Filamentous mold, has narrow septate hyaline hyphae with 45° branching
• Galactomannan is major component of cell walls
• Pulmonary aspergillosis presents with fever, pleuritic chest pain, and hemoptysis
• Also causes aspergilloma, hypersensitivity pneumonitis, rhinosinusitis
Aspergillus fumigatus
• Culture + histopathology showing tissue invasion
• Noninvasive methods: serum galactomannan, staining BAL with Gomori silver or PAS
-Risk factors: Neutropenia, glucocorticoids, immunocompromised
Histoplasma capsulatum
• Thermally dimorphic fungus
• Mold in soil, yeast in host
• Ovoid yeast with narrow based budding
• In the U.S.: Mississippi, Ohio, and St. Lawrence River valleys
• Concentrated in soil contaminated with bird/bat droppings
Histoplasma capsulatum
Suspect in patients with:
• Lung granulomas
• Pneumonia with mediastinal or hilar
lymphadenopathy
• Pulmonary nodules or cavitary lung disease
Coccidioides immitis
• Thermally dimorphic fungus
• Mycelia found in deserts in the southwestern U.S.
• In hosts, spherules contain endospores
• Diagnosed via intradermal antigen injection (similar to PPD for tuberculosis) or serology
Coccidioides immitis
• Coccidioidomycosis (AKA San Joaquin Valley fever)
• Caused by inhaling arthroconidia
• 2nd most common fungal infection in U.S.
Blastomyces dermatitidis
• Thermally dimorphic fungus
• 25°C: fluffy white mold
• 37°C: brown folded yeast with thick refractile cell wall; reproduce with a single broad-based bud
Blastomyces dermatitidis
• Endemic in Ohio and Mississippi River valleys, Great Lakes area, and SE U.S.
• Found in soil in wooded areas with decaying vegetation
• Extrapulmonary disease is common
• Skin, bones, genitourinary tract
• Can cause disease in immunocompetent patients
• Or infections may be asymptomatic
Cryptococcus neoformans
• Encapsulated yeasts
• Found in soil contaminated with bird droppings, decaying wood, and tree hollows
• Diagnosed by CSF analysis, culture, and staining
• Stain with India ink to show capsule; mucicarmine stain shows both yeast and capsule
• CSF usually shows low WBC, low glucose, ↑ protein, but can be normal in ~30% of patients
• Look for antigen in serum and CSF
Cryptococcus neoformans
• Cryptococcosis (cryptococcal meningitis) occurs mostly in immunosuppressed patients
• Focal pneumonitis (with or without symptoms) in immunocompetent patients
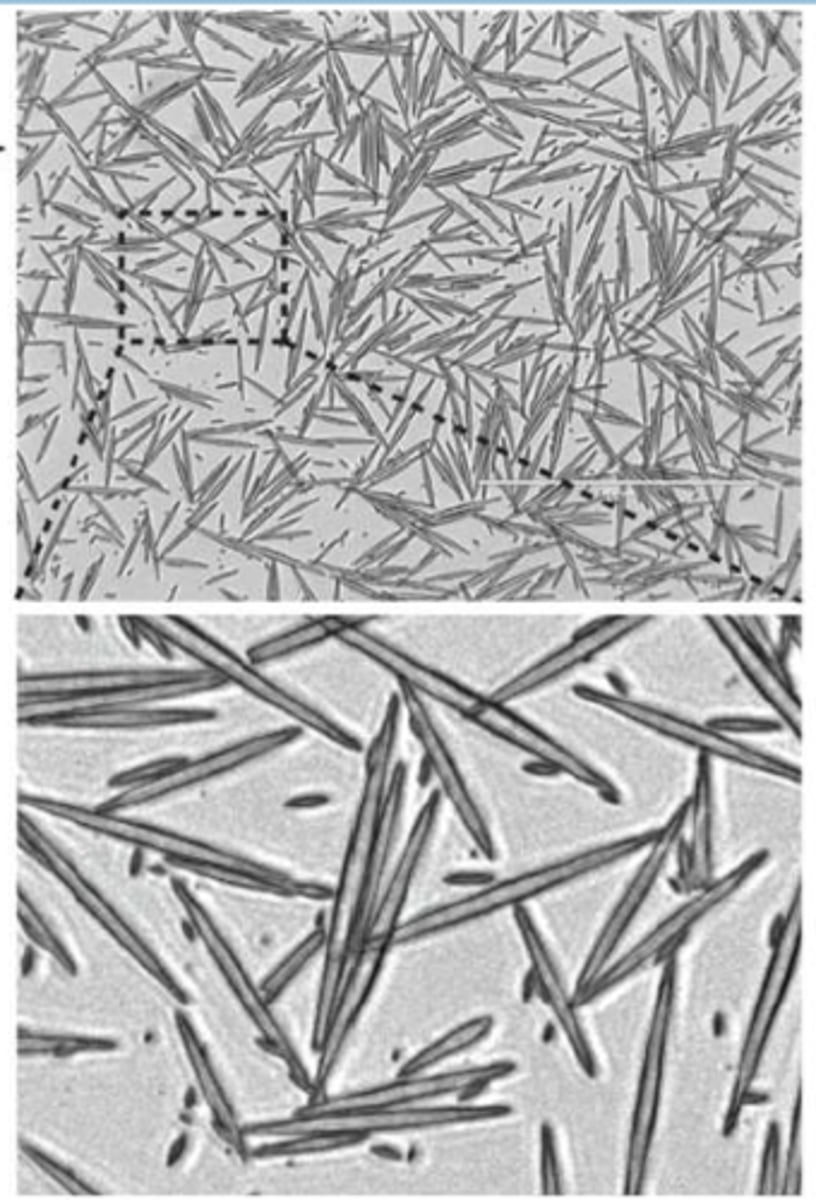
Charcot-Leyden crystals
Ascaris lumbricoides
• Worldwide distribution; most cases in Asia
• Most common in children 2-10 years old
• Highest prevalence in tropics
• Loeffler syndrome (A. pneumonia)
• Nonspecific symptoms (late phase intestinal involvement)
• Abdominal pain, anorexia, nausea/vomiting, diarrhea
• Look for eggs in stool
• Oval with a thick mamillated shell
Ascaris lumbricoides
Life cycle:
• Eggs must embryonate in soil to become infectious
• Humans ingest eggs
• Larvae migrate through intestine into bloodstream and then lungs
• Worms are swallowed and become adults; majority found in the jejunum
Hookworms
• Common in tropics and subtropics
• Risk factors: walking barefoot, poor sanitation
• Ancylostoma duodenale (Mediterranean countries,
Iran, India, Pakistan, Asia)
• Necator americanus (North and South America,
Africa, Indonesia, and South Pacific)
Hookworms
Life cycle
• Filariform larvae penetrate the skin
• Bloodstream carries larvae to the lungs; they migrate
up the bronchial tree and are swallowed
• Develop into adults in small intestine; attach to wall
and feed on blood from capillaries
Hookworms
• Major damage due to blood loss at site of attachment
• Reflects 4 phases of infection
• Ground itch, cutaneous larvae migrans
• Pulmonary symptoms (maybe)
• GI symptoms
• Chronic nutritional impairment
Hookworms
• Stool examination is not helpful before established GI disease
• May see eosinophilia, occult blood in stool
Threadworms
• AKA Strongyloides stercoralis (causes strongyloidiasis)
• Endemic in rural areas in tropics and subtropics
• Sporadic in temperate areas
• Highest rates in US in southeastern states and people who have traveled in endemic areas
Threadworms
• Symptoms depend on site of worm
• Watery diarrhea, pneumonitis, ground itch or larva currens
• Chronic infection: intermittent abdominal pain, fluctuating rash, intermittent eosinophilia
• Find larvae in stool
• Use ELISA to look for antibodies
Clonorchis sinensis and Fasciola hepatica
-liver flukes
-ingesting raw/undercooked fish
-contaminated water in sheep-raising areas
Paragonimus westermani
-lung flukes
• Ingesting raw/undercooked crab or crawfish
• Late infection → chocolate-colored sputum
Entamoeba histolytica
-amebic dysentery
• Ingesting contaminated food/water
• Diarrhea with blood and mucus in stools; trophozoites in stools or tissues
Schistosoma spp.
-blood flukes
• Highest prevalence in sub-Saharan Africa
• Contact with contaminated water; snail hosts
Echinococcus granulosus
-Hydatid Cyst
• Dogs (canids) are definitive hosts; domestic animals are intermediate hosts
• Highest rates of disease in areas where sheep are raised
• Usually a single cyst; symptoms depend on size and location
Tuberculosis
• Present globally, but disease burden is higher in developing nations
• Risk factors: Poverty, malnutrition, incarceration, immunosuppression, occupation
Tuberculosis
• Primary infection is usually asymptomatic
• Chronic cough, weight loss, fever, night sweats
• Hemoptysis is late-stage symptom
• Secondary TB has more severe tissue reaction/hypersensitivity
• Kidney, bone growth plates, lymph nodes, meninges, elbows
• Hip joints (avascular necrosis)
• Vertebrae (Pott's disease)