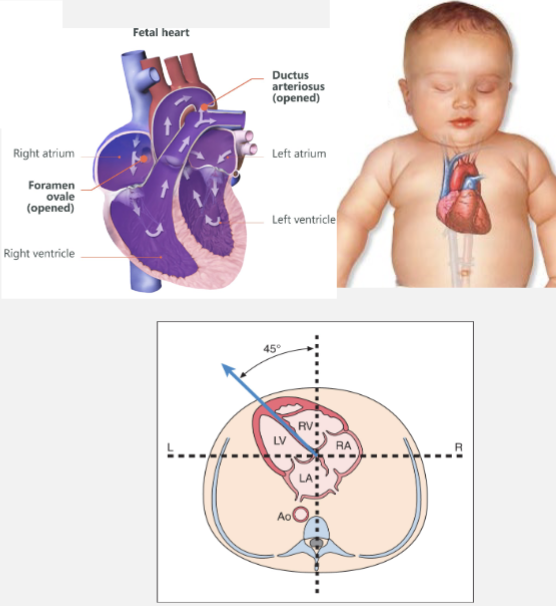
Fetal Heart (Ch. 36)
1/44
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
45 Terms
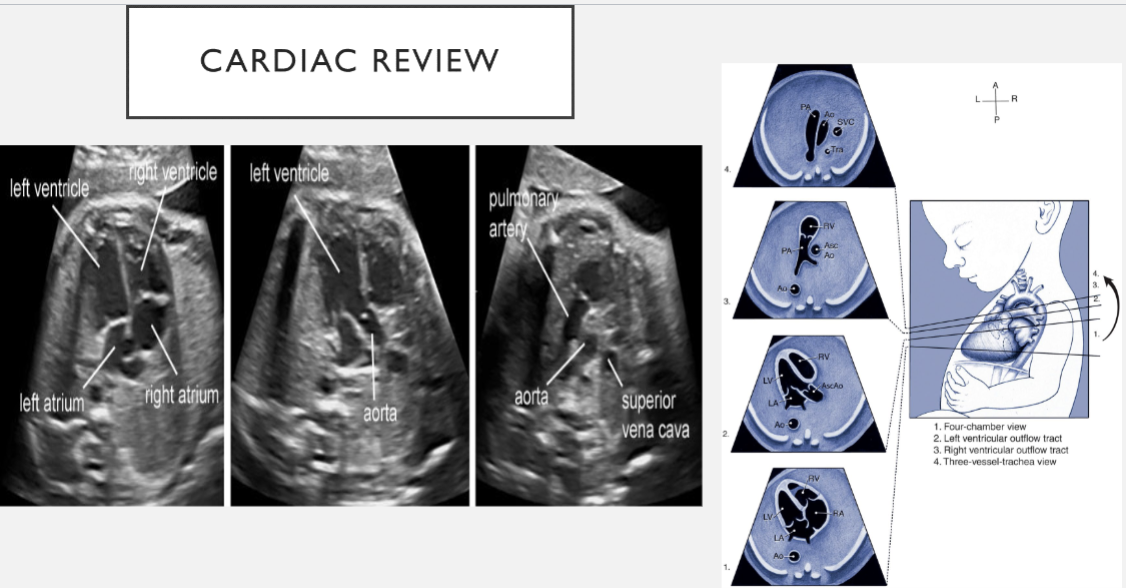
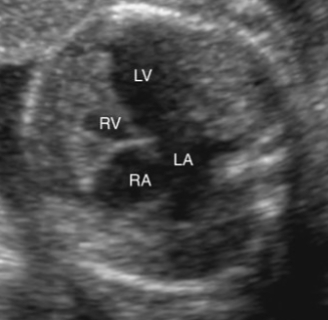
cardiac review
heart lies in mid chest, slightly to left
ventricles (2)
anteriorly to and inferiorly
RV is more anterior than LV
atria (2)
posteriorly and adjacent to spine
LA is closest to spine
apex of heart is tilted toward left
cardiac review: RA and RV
RA
receives deoxygenated blood from IVC and SVC
sends blood to the RV through the tricuspid valve
RV
receives deoxygenated blood RA
sends deoxygenated blood to the lungs via the pulmonary artery (RVOT)
cardiac review: LA and LV
LA
receives oxygenated blood from the pulmonary veins (4)
sends blood to the LV through the mitral valve
LV
receives oxygenated blood from LA
sends oxygenated blood to the body via the aorta
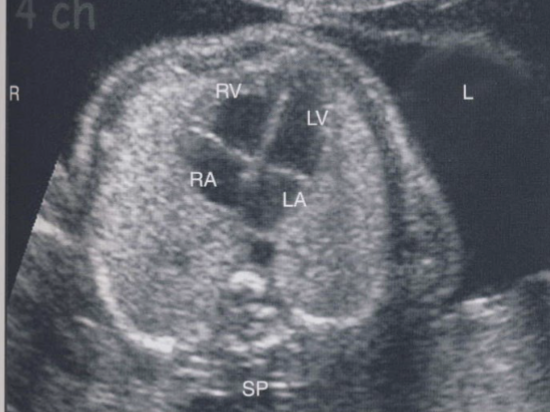
levocardia
normal heart position
apex of heart points to left and bulk of the heart is in the left chest
denotes both normal position of heart in left chest
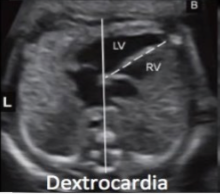
dextrocardia
heart in right chest with apex pointed to right of thorax
can be associated with normal visceral situs, situs inversus, or situs ambiguous
dextroposition
heart is located on right side of chest and cardiac apex points medically or left
usually found when extrinsic factors—space-occupying large diaphragmatic hernia or hypoplasia of right lung are present

levoposition
heart is displaced further toward the left chest, usually in association with space-occupying lesion
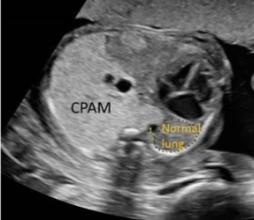
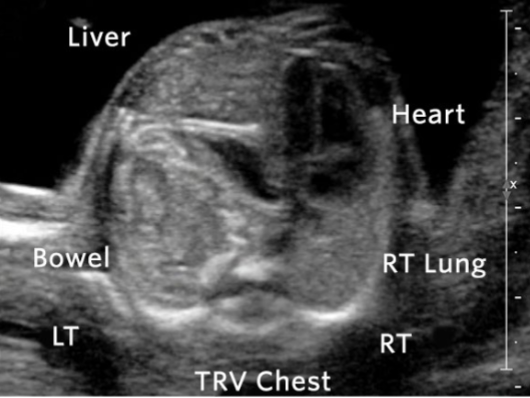
what do you see?
mesocardia
atypical location of heart, with cardiac apex pointing toward midline of the chest
heart is located more toward midline
this may be found with presence of an intracardiac mass or lung abnormality

cardiomyopathy
disease of myocardial tissue in heart
causes:
exposure to virus (coxsackievirus or mumps) or bacteria leading to infection
errors of metabolism
endocardial fibroelastosis
myocarditis
disease of myocardial tissue in heart
necrosis and destruction of myocardial cells and inflammatory infiltrate
thinning of myocardial walls, four chambers dilated
pericardial effusion
abnormal collection of fluid surrounding epicardial layer of heart
normal amount of pericardial fluid is 2mm or less
separation of 2mm or more is considered abnormal
pericardial effusion may be associated with hydrops fetalis
atrial septal defects
defect in atrial wall that allows for communication b/w two atria
oxygen rich blood can flow directly from LA to RA and mix with oxygen poor blood
3 types:
ostium secundum
ostium primum
sinus venosus
ostium secundum
MC type
occurs in area of foramen ovale
absence of foramen ovale flap is noted, with fossa ovalis opening larger than normal
central septum
ostium primum
cleft of mitral valve causing mitral regurge into left atrial cavity
defect is located low in atrial septum, near the AV valves
associated with T21
sinus venosus
defect is in superior portion of septum
adjacent to superior vena cava
less common

which atrial septal defect is this?
ostium primum ASD

which atrial septal defect is this?
ostium secundum ASD
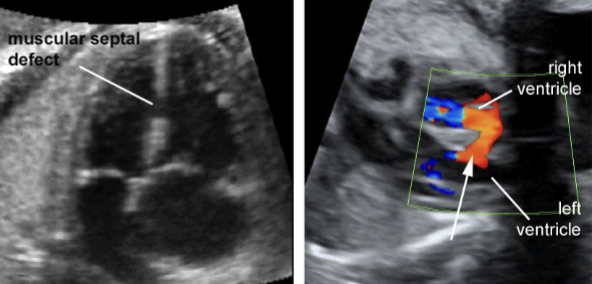
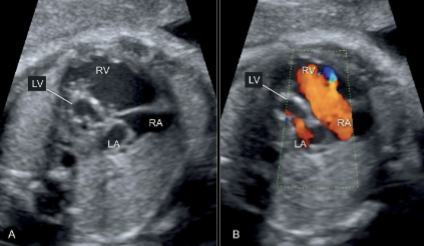
ventricular septal defects (VSD)
MC congenital heart lesion
accounts for 30% of all structural heart defects
accounts for 30% of all structural heart defects
abnormal opening in septum between 2 ventricles of the heart
isolated VSD is MC cardiac defect
appears as an area of discontinuity in interventricular septum
membranous vs muscular
good prognosis
spontaneous closure can occur in utero and within 1st year of life
large defects require surgical treatment
4CH view is best to visualize large defects
color Doppler can show the movements of flow between the ventricles
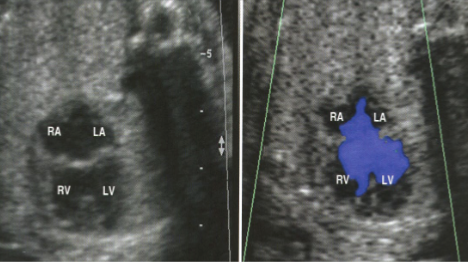
atrioventricular septal defects (AVSD)
previously referred to as endocardial cushion defects of A-V canal defect
defect in the central part of the heart
defect includes: interatrial septum; interventricular septum; mitral valves; tricuspid valves
results from malformation in the development of endocardial cushion
good prognosis with surgery worse when associated abnormalities are present
defect is visualized best in 4CH
color and spectral Doppler are useful in demonstrating flow directions and degree of regurgitation
AVSDs are associated with…
chromosomal abnormalities or extra-cardiac anomalies, such as:
trisomy 21 (40% of cases)
tetralogy of Fallot
subaortic stenosis
ventricular hypoplasia
pulmonary valve stenosis
partial AVSD
part of ventricular septum hsaa filled in with tissue from AV valves or endocardial cushion
tricuspid and mitral valves are divided into 2 distinct valves
complete AVSD
there are defects in all structures formed by the endocardial cushion:
atrial septum
ventricular septa
both AV valves
common valve between mitral and tricuspid valves
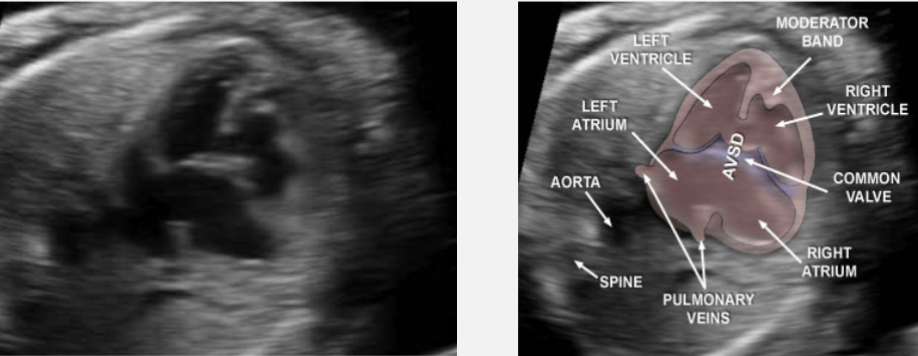
which AVSD is this?
complete AVSD
which AVSD is this?
partial AVSD
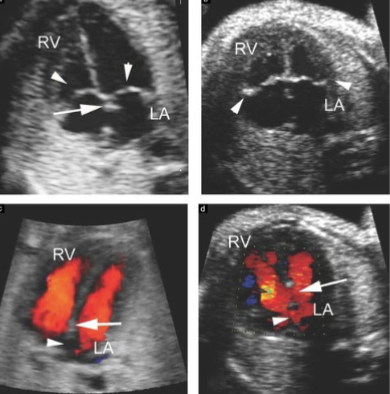
Ebstein’s anomaly
abnormal displacement of tricuspid septal leaflet toward the apex of RV
results in regurgitation or leakage from RV back to RA
RA is large while RV is small
best visualized in 4CH view
enlargement of RA with inferior displacement of tricuspid valve into RV
can be difficult to see if mild
color/spectral Doppler will reveal regurgitation across the tricuspid valve
hypoplastic left heart syndrome
small or hypertrophied LV
decreased blood flow into or out of LV
may have mitral valve dysplasia or atresia
minimal communication between LA and LV
RV ends up supplying both pulmonic and systemic circulations
ascending AO atresia or stenosis is possible
extremely poor prognosis (transplantation is usually required)
SONO: hypoplastic left heart syndrome
small LV
hypertrophied LV walls
mitral valve and AO are hypoplastic or atretic
hypoplastic right heart syndrome
a range of defects secondary to underdevelopment of right side of heart
obstruction of right ventricular outflow tract due to pulmonary stenosis
small tricuspid valve
pulmonary artery stenosis and/or atresia
SONO: hypoplastic right heart syndrome
small RV
small or absent PA
PA stenosis
VSD may or may not be present
tetralogy of fallot
MC form of cyanotic heart
characterized by 4 components:
ventricular septal defect
right ventricular hypertrophy
pulmonary stenosis (RVOT obstruction)
overring AO (aorta overrides both ventricles)
associated with chromosomal abnormalities
4 characteristic of tetralogy of fallot
right ventricular outflow obstruction
right ventricular hypertrophy
AO overrides VSD
ventricular septal defect
truncus arteriosus
only one great artery arises from base of the heart
pulmonary, coronary, and systemic arteries arise from common root
VSD typically present
can mimic ToF with pulmonary atresia
too much blood may be sent to lung
extra fluid may build up in/around lungs
blood vessels to lungs become damaged (pulmonary hypertension)
surgical intervention is required
poor prognosis if left untreated
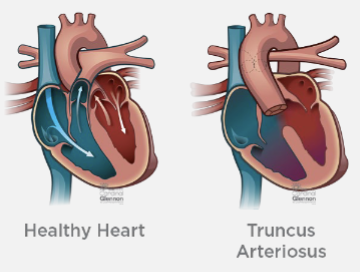
SONO: truncus arteriosus
4CH is usually normal
truncal root overrides ventricular septum
single great artery
transposition of the great arteries
when AO arises from RV and PA arises from LV
AO from RV sends poorly oxygenated blood to the body
PA arising from LV sends well-oxygenated blood back to the lungs
3 main arteries leaving the heart are reversed
leads to shortage of oxygenated blood flowing from heart to rest of body
associated anomalies:
ASD
atrioventricular valve anomalies
underdevelopment of RV and/or LV
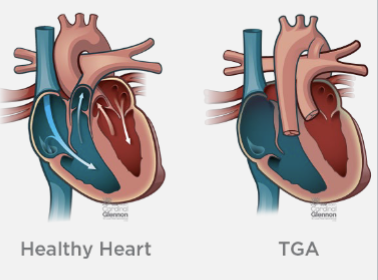
SONO: transposition of the great arteries
2 great vessels fro not cross but arise parallel from base of the heart
4CH is normal
aortic coarctation
congenital defect causing narrowing of aortic lumen
almost 90% are associated with other abnormalities:
aortic stenosis; aortic insufficiency; septal defects; TGA; truncus arteriosus; Turner’s syndrome
narrowing can occur at aortic arch isthmus or left subclavian artery insertion
good prognosis when isolated; worse if other anomalies present
SONO: aortic coarctation
difficult to see
candy can view is best to visualize
echogenic cardiac focus
bright echogenic dot in ventricle
often in LV
associated with T21 and T13
isolated finding is typically a normal finding
3-4% of normal fetuses have ECF

rhabdomyoma
MC fetal intracardiac tumor
tend to be multiple and involve septum
associated with tuberous sclerosis
fetus becomes symptomatic when tumor is large enough to cause outflow tract obstruction
leads to CHF; pericardial effusion; hydrops; death
prognosis depends on size and location
SONO: rhabdomyoma
echogenic, solid mass within fetal heart
fetal echo shows tumor best in 4CH