UCF Anatomy Block 3 Study Guide: Key Terms & Definitions
1/152
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
153 Terms
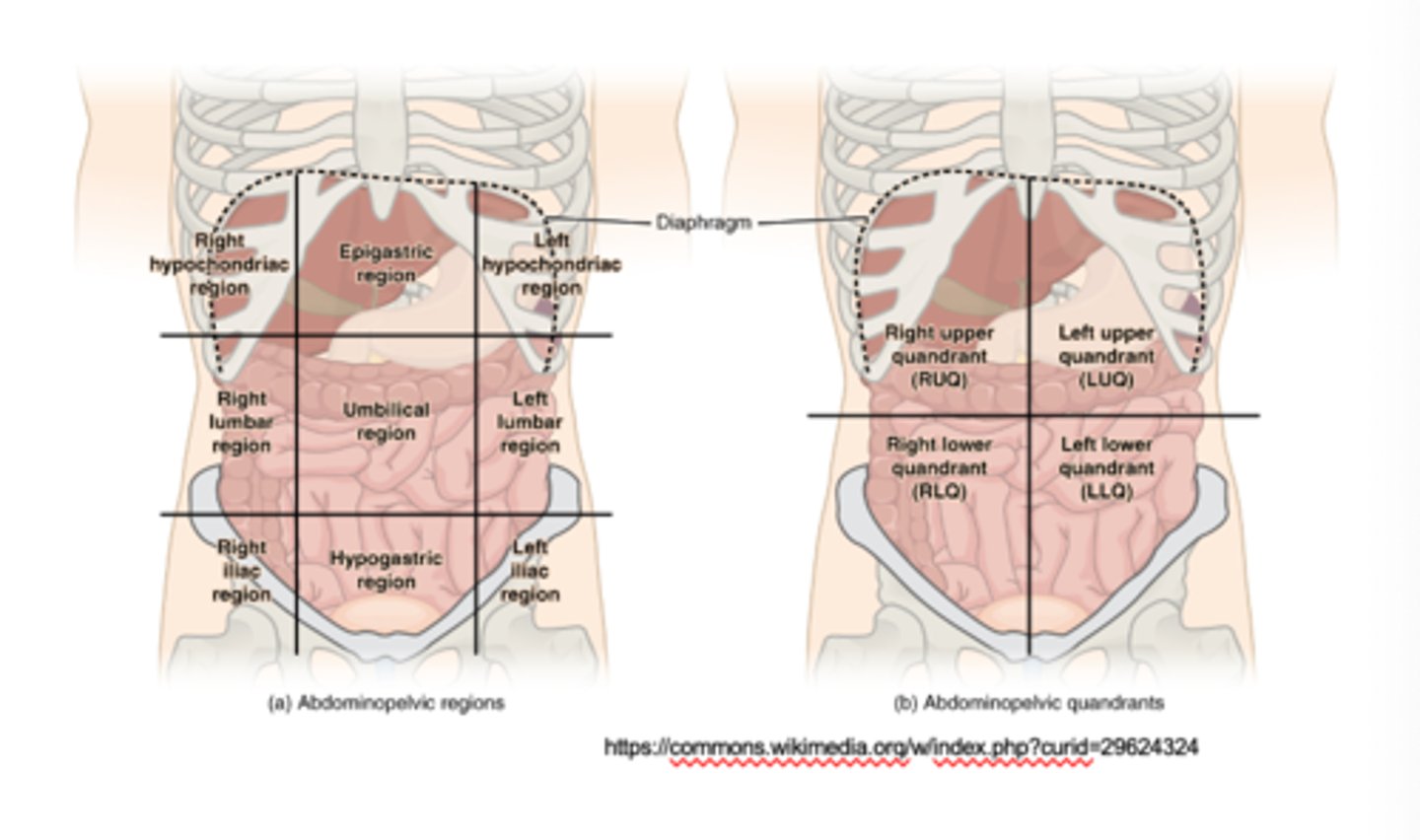
Regarding surface anatomy, what are the nine regions of the abdomen?
Right hypochondriac region
Right lumbar region
Right iliac region
Epigastric region
Umbilical region
Hypogastric region
Left hypochondriac region
Left lumbar region
Left iliac region
What are the lateral group muscles?
External abdominal oblique, internal abdominal oblique, transverse abdominal
What are the innervations of the lateral group muscles?
6 lower intercostal nerves and L1
What are the medial group muscles?
Rectus abdominis, pyramidalis
What is the origin of the inguinal ligament?
External abdominal oblique muscle
Lowest portion of the aponeurosis
What are the innervations of the medial group muscles?
6 lower intercostal nerves and L1
What is the origin of the cremaster muscle?
The caudal and lowest part of the internal abdominal oblique
What is the innervation of the cremaster muscle?
Genital branch of the genitofemoral nerve (ONLY in genetic males)
What is the clinical significance of the cremasteric reflex?
Is NOT a pathology, it is utilized to our advantage.
If an individual has had a traumatic accident and the testes become twisted (called torsion of the testis), or if there is a mass in the testis and we want to see how invasive that can be, if you palpate the upper portion of the thigh, that will cause a contraction of the cremaster muscle and you can feel that. If you put your hands on the cremaster muscle and palpate the upper thigh, you can feel it contracting. That tells you you've got both sensory and motor innervation from the genitofemoral nerve that is appropriate. If you've had a traumatic event or a mass, you can manipulate the reflex and find out if you have normal innervation.
What is the location of the rectus sheath?
Surrounding the rectus abdominis both anteriorly and posteriorly
External obliques go anterior, internal obliques and transversus abdominis go posterior
What are the contents of the rectus sheath?
Rectus abdominis muscle
Inferior and superior epigastric vessels
Intercostal nerves (5 lower ones), including the subcostal nerve
What is the importance of the rectus sheath?
Holds major abdominal structures
What are the contents of the inguinal canal for the male?
Spermatic cord
What are the contents of the inguinal canal for the female?
Round ligament of the uterus and lymphatics
What is cryptorchidism?
Testis fails to descend
What is the clinical significance of cryptorchidism?
We need to act on this very quickly. In humans, where we have pendulous testes, the testes are very temperature sensitive. They are held 5 to 7° cooler than the rest of the body. If they're inside the body, they don't like to be held at 98.6° or higher. We would need to remove the testes, as long as they are normally developed. If they are left in the abdominal cavity, the tissue can become corrupted and turn into cancer. Typically, we act right when the baby is born.
What is hydrocele of the cord?
Process vaginalis fails to close after testes have descended; fluid forms around the spermatic cord
What is the clinical significance of hydrocele of the cord?
Fluid forms around the spermatic cord
What are the contents of the spermatic cord?
Ductus (vas) defrens
Testicular artery, artery of the ductus deferens, and cremaster artery
Pampiniform plexus
Autonomic nerve fibers
Genital branch of the genitofemoral nerve
Lymphatics
Cremaster muscle
What is the difference between a direct and indirect inguinal hernia?
Direct inguinal hernia:
You can palpate the mass and it is super soft; it is just a loop of intestine. You can even push it back in.
Generally does not require surgery. May put the patient on bed rest or put them into a binding (brace), sometimes it can heal. A doctor might want to do the surgery, depending on the patient they may put a mesh.
Indirect inguinal hernia:
Always requires surgery
Comes through the abdominal wall inside the spermatic cord, so surgery will be required to pull the loop of intestine back out and let it freely into the abdominal cavity.
What are the unique characteristics of an indirect inguinal hernia?
Lateral to epigastric vessels
Passes through the inguinal canal (inside the spermatic cord)
High risk of strangulation/infarct
Congenital and acquired
In younger people
Bigger in size
What are the unique characteristics of a direct inguinal hernia?
Medial to epigastric vessels
Don't pass through the inguinal canal (parallels spermatic cord)
Low risk of strangulation/infarct
Are almost always acquired
Middle age man (over 40 y)
Smaller in size
Occurs within Hesselbach's triangle
Which organs are categorized as intraperitoneal?
Have a mesentery and are completely covered by the peritoneum. Includes these organs, found in the abdominal peritoneal cavity:
Stomach, small intestine (jejunum, ileum, some of the superior part of the duodenum), spleen, liver, gallbladder, cecum with vermiform appendix (portions of variable size may be retroperitoneal), large intestine (transverse and sigmoid colons)
Which organs are categorized as retroperitoneal?
Not covered in visceral peritoneum because they're not inside of the peritoneal cavity or sac. Either have no mesentery or lost it during development. Includes these organs:
Primarily: kidneys, suprarenal glands, uterine cervix
Secondarily: Dudodenum (descending, horizontal, ascending), ascending and descending colon, pancreas, rectum (upper 2/3)
What is the lesser sac?
A diverticulum of the peritoneal cavity to the left side and posterior to the stomach
What is the clinical significance of the epiploic foramen?
This is the site of internal herniation and strangulation of part of the intestine into the lesser sac
Surgery should be done from the other side (into the sac), not touching the porta hepatis
The cystic artery of the gall bladder can be reached through this foramen
What is the epiploic foramen?
The opening to the lesser sac, beneath the portal triad
What is the clinical significance of the lesser sac?
This is the site of internal herniation and strangulation of part of the intestine into the lesser sac
Surgery should be done from the other side (into the sac), not touching the porta hepatis
The cystic artery of the gall bladder can be reached through the epiploic foramen
What is the importance of the greater omentum?
Policeman of the abdomen
Has 4 layers
Prevents the visceral peritoneum to adhere to the parietal peritoneum
Has considerable mobility and moves by peristaltic movements of the viscera
Contains fat and lymphocytes and other immune cells to protect against infection or inflammatory conditions in the abdominal cavity; is often called the abdominal policeman
Moves towards the inflamed or infected area (e.g. the appendicitis)
Protects abdominal organs against injury and acts as an insulator against loss of body heat
What is the clinical significance of the peritoneal spaces and compartments?
Can get an increase in fluid in the abdomen, post-operatively, we can see it's just a consequence or a side effect of inhaled anesthetic, we can get an increase in serous fluid production in the abdomen. Not a big deal, but it can sit in the subphrenic space and cause it to be irritated. In a patient in the elderly population, this can lead to development of respiratory problems in a post operative environment from this type of condition. This is why we want you up and moving. Adhesions form, move that fluid around, and it can become an irritant.
Peritonitis, ascites, paracentesis
What is peritonitis?
The inflammation (accompanied by pain) of the peritoneum following an abdominal injury, i.e., from a stab wound or a perforated appendicitis
What is ascites?
Abnormal accumulation of fluid in the abdominal cavity, commonly seen in liver cirrhosis
What is paracentesis?
Puncturing the peritoneal cavity for aspiration of the fluid
What structures/organs belong to the foregut?
Esophagus and stomach down to the 2nd part of the duodenum, including liver, biliary system, gall bladder, and pancreas
What structures/organs belong to the midgut?
Starts from lower half of the 2nd part of the duodenum and jejunum, ileum, colon (cecum, ascending and the right 2/3 of the transverse colon)
What structures/organs belong to the hindgut?
Left 1/3 of the transverse colon, descending colon, sigmoid colon, rectum and upper part of anal canal
What is the innervation of the foregut?
Parasympathetic: Vagus nerve (CN X)
Sympathetic: T5-L2 spinal segments
What is the innervation of the midgut?
Parasympathetic: Vagus nerve (CN X)
Sympathetic: T5-L2 spinal segments
What is the innervation of the hindgut?
Parasympathetic: Pelvic splanchnic nerves (S2, S3, S4)
Sympathetic: T5-L2 spinal segments
What is the blood supply of the foregut?
Celiac trunk
What is the blood supply of the midgut?
Superior mesenteric artery
What is the blood supply of the hindgut?
Inferior mesenteric artery
What is the blood supply of the esophagus?
Upper part (cervical portion): by inferior thyroid artery
Middle part (thoracic portion): by thoracic aorta (4-5 arteries) and from bronchial arteries
Lower part including the abdominal portion: left gastric artery (from Celiac trunk), and inferior phrenic artery (from abdominal aorta)
What is the venous drainage of the esophagus?
Inferior thyroid vein, azygos, hemiazygos, and gastric veins
Gastric veins drain into the portal vein; therefore, this is a link between portal and the systemic circulation (Porto-Caval anastomosis)
What causes esophageal varices in liver cirrhosis?
Gastric veins drain into the portal vein; therefore, this is a link between portal and the systemic circulation (Porto-Caval anastomosis)
What is the clinical significance of esophageal varices?
When the liver is compromised, the blood is really congested because of these huge fibroids in the liver; it prevents blood from flowing through, so it backs up into the portal vein. When this happens, it causes portal hypertension. The portal vein is really dilated and the walls start to be pushed and gap open. This allows blood plasma and formed elements of blood to be pushed into the abdominal cavity; that is ascites. When that happens, it's not just the portal vein that's dilated, it's all the other veins draining into it that are also dilated. if the stomach drains into the portal vein, the stomach will eventually have blood backing into its veins making it congested. In the areas with the porto-canal anastomosis, if the blood is backing up, the blood will also back up into the lower esophagus because it's backing into the gastral vein. However, you could just flip the switch and have the blood drain into the caval system.
What is the histology of the esophagus?
These four layers/tunics will form the walls of every tubal structure in the body, with slight modifications as form follows function. In addition, all tubes are lined with epithelial cells.
Mucosa: stratified non-keratinized squamous epithelium (in Cardia, transitions simple columnar)
Muscularis mucosa
Submucosa
Tunica muscularis: consist of inner circular and outer longitudinal muscular layers
Adventitia serosa
What is the type of epithelium that lines the Gastrointestinal tract from the mouth to the external anal canal?
Oral cavity to esophagus: stratified non-keratinized squamous epithelium
Stomach to upper anal canal: simple columnar
Below the pectinate line: stratified non-keratinized squamous epithelium
What is a diverticulum of the esophagus?
All 3 wall layers protruding to form little pouches
What is the clinical significance of Zenker's diverticulum?
Upper esophagus, dysphagia, and halitosis
Complications: ulceration, bleeding, and inflammation
Therapy: surgery
Food can get trapped in here. It can cause irritation, ulceration, bleeding, inflammation, and infection. Surgery to remove it can fix it.
What is the clinical significance of achalasia (cardiospasm)?
Retrosternal pain, neuromotor disorder of the lower esophageal sphincter (LES), decreased cells in the myenteric plexus (analogous to Hirschprung's disease), dysphagia for solid and liquid, dilated proximal esophagus and aperistalsis, increased LES pressure
Treated in a case-by-case basis; some patients are completely fine but can have moments of something hurting. They will understand that the lower esophageal sphincter has stayed closed. They will need to go to the hospital and have mechanical assistance. The worst scenario is where the lower esophageal sphincter can't open at all. This will need a feeding tube, liquid diet, or eat something soft like apple sauce/jello, and then wait, take a sip of liquid, and wait. We could try stimulation; if this is because of stroke or trauma, we could work with a physical therapist.
What is the clinical significance of Barrett's esophagus?
Columnar cell metaplasia of the squamous epithelium due to acid injury
This is caused by a chemical burn. Lower esophageal sphincter isn't closing as it should. Can cause damage/erosion to tissue, chronic inflammation, etc.
What is the importance of the stomach rugae?
Expands the stomach
What is the importance of the oblique muscle layer of the stomach?
Allows for churning the stomach
What are gastric pits?
Shallow part of the gastric mucosa; all you'll see is mucus cells, same simple columnar epithelium
What are gastric glands?
Deep part of the gastric mucosa; cells become more specialized
What three types of cells would you find in the gastric glands within the body and fundus of the stomach?
Mucoid cells
Chief cells
Parietal cells
What are the functions of mucoid cells?
Secrete mucus to shield the mucosal membrane
What are the functions of chief cells?
Produce pepsinogen
What are the functions of parietal cells?
Produce HCl and intrinsic factor for B-12 absorption in the ileum
What enteroendocrine cell would you find within the gastric glands in the pyloric antrum?
Endocrine cells of mucosa (1.2% of all) mainly in antrum
Gastrin, produced by G cells mainly in pyloric antrum
What is one of the most important enteroendocrine cells we have in the stomach, found in the glands, in the pylorus and the pyloric antrum?
G cells
What is the function of the endocrine cells of mucosa?
Produce histamine, somatostatin, gastrin, serotonin, and prostaglandins
What is the function of the gastrin?
Stimulate acid secretion and growth of parietal cells
What is the blood supply of the stomach?
Celiac trunk branches
Left gastric artery
Common hepatic artery -> right gastric artery
Common hepatic artery -> gastroduodenal artery -> right gastroepiploic artery
Splenic artery -> short gastric arteries and left gastroepiploic artery
What is the venous drainage of the stomach?
Portal vein directly (left and right gastric veins) or indirectly through the splenic vein (the left gastroepiploic vein and short gastric veins)
The right gastroepiploic vein goes to the superior mesenteric vein
What is the innervation of the stomach?
Parasympathetic: Vagus nerve
Sympathetic: Mostly coming from splanchnic (innervating organs) nerves (also from upper lumbar) which synapse in the Celiac ganglion
Postganglionic fibers innervate the stomach to inhibit peristalsis and gastric secretion, and cause pyloric contraction; they also convey pain
What is the clinical significance of gastric ulcers?
Understanding how gastric juices are secreted is essential for treating an unresponsive ulcer.
A gastric/duodenal ulcer can be incompatible with life if we have a perforation, meaning the ulcer erodes all the layers of the wall of the organs and spills the hydrochloric acid and gastric contents into the abdominal cavity. When I am treating an ulcer, first thing I want to do is say, what's going on in the patient's life? Make changes to their life. Or give medication and see if it helps. If not, get more invasive. The rule of thumb is no acid, no ulcer, or highly regulated acid secretion, no ulcer. One of the ways to do that is a vagotomy.
Will focus on a pylorectomy: removes G cells that secrete Gastrin; controls acid secretion
What is a pylorectomy?
Removes G cells that secrete gastrin; controls acid secretion
What is the clinical significance of a vagotomy?
Used to be popular in the US but not anymore. Performed in other countries, going in and cutting the vagus nerve. Not going to cut all areas, but depending on the patent you could completely cut it on the top of the fundus of the stomach. Still going to have mechanical stimulation; when you eat, food will go into the duodenum but it won't be optimal. The consequences of it outweigh the benefits. Controlling neural stimulation to cut the vagus nerve out, but seeing/smelling food will not cause neural secretion of hydrochloric acid. Eliminates the neural stimulation of gastric secretion. Procedure is known to have complication on gastric emptying.
What is the clinical significance of a hemigastrectomy?
Part of the stomach gets removed
Could potentially perform a pylorectomy: Removes G cells that secrete gastrin; controls acid secretion
How are gastric ulcers, vagotomy, and hemigastrectomy connected?
You could perform a vagotomy or hemigastrectomy to deal with gastric ulcers
What is the clinical significance of a sliding hernia?
When abdominal part of the esophagus and cardia and even part of the fundus slide up through the esophageal hiatus. *Regurgitation and heart burn
The stomach pushes up and everything shifts upwards. The esophagus gets pushed up, the cardia gets pushed up, and sometimes the fundus. Puts pressure on the lower esophageal sphincter and pushes it open.
What is the treatment for a sliding hernia?
Surgery:
Reinforces the barrier to reflux that the lower esophageal valve normally provides
In most cases, the operation performed to correct gastroesophageal reflux is a procedure called "fundoplication"
The upper portion of the stomach (the fundus) is wrapped (plicated) around the lower portion of the esophagus and anchored securely below the diaphragm
Radiofrequency treatment:
Using an endoscope supplied by electrodes
Radiofrequency energy causes tiny burns at G-E junction that heal and form scar tissue that actually tightens the weak valve
Case-by-case basis
What is the clinical significance of a paraesophageal hiatal hernia?
Cardia doesn't move but part of the fundus and peritoneum passes through the esophageal hiatus.
*Usually, no regurgitation
Para = beside, so beside the esophagus. The lower part of the esophagus stays in place; the fundus gets slipped up.
What is the treatment for a paraesophageal hiatal hernia?
Surgery:
Reinforces the barrier to reflux that the lower esophageal valve normally provides
In most cases, the operation performed to correct gastroesophageal reflux is a procedure called "fundoplication"
The upper portion of the stomach (the fundus) is wrapped (plicated) around the lower portion of the esophagus and anchored securely below the diaphragm
Radiofrequency treatment:
Using an endoscope supplied by electrodes
Radiofrequency energy causes tiny burns at G-E junction that heal and form scar tissue that actually tightens the weak valve
Case-by-case basis
What is the clinical significance of hypertrophic pyloric stenosis?
Progressive hypertrophy of circular muscles in pyloric sphincter, causing a narrow pyloric lumen which may obstruct food passage
This may happen in male infants (first child usually) which is associated with projectile, non bilious vomiting after feeding; palpation reveals a small knot (olive-sized mass) at the right costal margin
Treatment: longitudinal pyloromyotomy, leaving the mucosa intact
What are the names of the four parts of the duodenum?
1st or superior part
2nd or descending part
What are the characteristics of the four parts of the duodenum?
1st or superior part:
5 cm long, between T12-L1
Anterior to portal vein and common bile duct
Duodenal cap: site of ulcer
2nd or descending part:
All kinds of things happen
7.5 cm long until lower level of L3
Contains the major duodenal papilla, a common opening for the common bile duct and the main pancreatic duct
Within the wall, the sphincter of Oddi is connected to the common dilated opening known as the hepatopancreatic ampulla of Vater
The minor duodenal papilla, superior to the major opening, is an opening of the accessory pancreatic duct
3rd or horizontal part:
10 cm, at L3 level
Anterior to IVC and abdominal aorta
Crossed by superior mesenteric artery and vein anteriorly
4th or amending part:
2.5 cm long
Travels across the midline to the duodenojejunal flexure at the L1-L2
The beginning of the 1st part and part of the 4th part are covered by the peritoneum (have some mobility), the rest of duodenum is not mobile
Function:
Regulates stomach and gallbladder emptying in response to acidic chyme
Secrete Secretin due to high acid and fatty acids in its lumen; Secretin inhibits the gastric acid secretion
Secretes Cholecystokinin, in response to fatty chyme which induces gallbladder contraction
Secretes the Enterogastrone, that inhibits stomach peristalsis
What is the parasympathetic innervation of the digestive tract?
Submucosal plexus of Meissner and myenteric plexus of Auberach
What is the function of the submucosal plexus of Meissner (digestive tract)?
Parasympathetic innervation
Secretomotor function produces mucus for lubrication and facilitates molecule movement
What is the function of the myenteric plexus of Auberach (digestive tract)?
Parasympathetic innervation
Peristaltic movement of smooth muscle
What is the function of the jejunum?
Absorption of the digested food
What is the blood supply of the small intestine?
Superior mesenteric artery, superior mesenteric vein
What is the function of the ileum?
Absorption of the digested food, vitamin B12, and intrinsic factor
What are the characteristics of the jejunum?
Begins at the duodenojejunal junction and is continuous with ileum
About 2/5 of the total length of the small intestine (6-7 m)
Folate is reabsorbed here
1. Lies mostly in the left upper quadrant
2. More vascular
3. Red color
4. Thick wall
5. Long vasa recta
6. Less Arcades
7. Less fat
8. Window in the mesentery
9. No or very few peyer's patches
10. Large and many circular folds (place circulare)
What are the characteristics of the ileum?
Ends at ileocecal junction
About 3/5 of the total length of the small intestine (6-7 m)
Vitamin B12 is reabsorbed here
1. Lies mostly in the right lower quadrant
2. Less vascular
3. Pale pink
4. Thin wall
5. Short vasa recta
6. More arcades
7. More fat
8. No window in the mesentery
9. Many peers patches
10. Low and fewer circular folds
What is the venous drainage of the small intestine?
Superior mesenteric vein
What is the innervation of the small intestine?
Sympathetic:
Splanchnic nerves
- Inhibition of peristalsis and contraction of the ileocecal sphincter and vasoconstriction of vessels
Parasympathetic:
Vagus nerve
- Causes peristalsis and glandular secretion
What is the clinical significance of Meckel's diverticulum?
An ideal out-pocketing typically located within 50-75 cm (40 cm in newborn) of the ileocecal valve
This is a congenital anomaly resulting from persistence of the vitelline (omphalomesenteric) duct. It might free 74% or attached by a cord to the umbilicus
May mimic pain of appendicitis
About half of them cause ulceration, inflammation, and GI bleeding because of the presence of ectopic acid-secreting gastric epithelium; pancreatic tissue may also be present there
Rule of 2's: Occurs in about 2% of children, 2 feet from the ileocecal valve, contain 2 types of ectopic mucosa (gastric and pancreatic), usually occurs at 2 years of age
What is the location of the vermiform appendix?
The posteromedial aspect of the cecum about 2-3 cm below the ileocecal junction
What is the function of the vermiform appendix?
In younger adults it's a lot larger and as we age it gets smaller in length and diameter. We also know that throughout our lives it contains a very large concentration of e-coli. It's thought that because it houses a lot of e-coli, if I have an insult to the large intestine, i.e. diarrhea, stress, diet, because of an infection of some sort, food poisoning, bacterial infection, viral infection, a lot of the e-coli is eliminated and this can easily be re-colonized due to the storage of the appendix. The gut microbiome is super important, a byproduct of the bacteria is vitamin K, which is important for clotting factors. At the end of the day we really don't know what it's there for or what it does; we can speculate, but we're not sure.
What is the clinical significance of an appendicitis, including treatment?
The appendix may be occluded by a fecalith (fetal material stuck inside) or inflammation and edema of the lymphatic tissue leading to acute (acute abdomen) and chronic appendicitis
Pain is preumbilical at T10 dermatome (sympathetic)
Appendectomy using the McBurney's point between umbilicus and right anterior superior iliac spine (junction between right 1/3 and mid 1/3)
The iliohypogastric nerve should be saved, if not, muscle weakness and direct inguinal hernia may result
The stages:
1. Early appendicitis
2. Appendiceal distention
3. Irritation of the lining of the abdominal and pelvic cavities
4. Perforation
What is the blood supply of the colon?
Branches of the superior and inferior mesenteric arteries
Marginal Artery of Drummond is an anastomosis of the superior and inferior mesenteric arteries. It is an important anastomosis if a portion of the arteries is blocked.
What is the overall function of the duodenum?
Digestion and absorption of food
What is the venous drainage of the colon?
Colic veins -> superior mesenteric veins -> portal vein
What is the clinical significance of the pectinate line of the anal canal?
Separation of the upper and lower anal canal; innervation, drainage, and blood supply change between the upper and lower anal canal
What is the pectinate line of the anal canal?
The inferior comb shaped limit of the anal valves
Separation of the upper and lower anal canal
What is the blood supply of the rectum and anus?
Superior rectal artery: the final branch of the inferior mesenteric artery supplies the superior part of the rectum
Middle rectal artery: from the internal iliac artery supplies the middle
Inferior rectal artery: a branch of the internal pudendal a.
What is the portocaval anastomosis?
Abdominal organs and structures either drain their blood directly into the IVC or indirectly by draining the portal vein and then through the liver for "filtering"