Human Physiology Lab Final
1/70
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
71 Terms
Inspiration
diaphragm and external intercostals contract
increase volume in thorax and lungs
volume in lungs increases, the air pressure in the lung decreases below atmospheric pressure, creating a pressure gradient that allows air to rush into the lungs
Expiration
inspiratory muscles relax → abdominals and internal intercostals contract
volume of thorax and lungs decreases
decreased lung volume causes an increase in pressure in the lungs, above atmospheric pressure, forcing air out of the lung and into the atmosphere.
passive expiration = relaxation of inspiratory muscles and elastic recoil → energy is put into stretching (inhalation) and stored energy is used for shrinking (expiration)
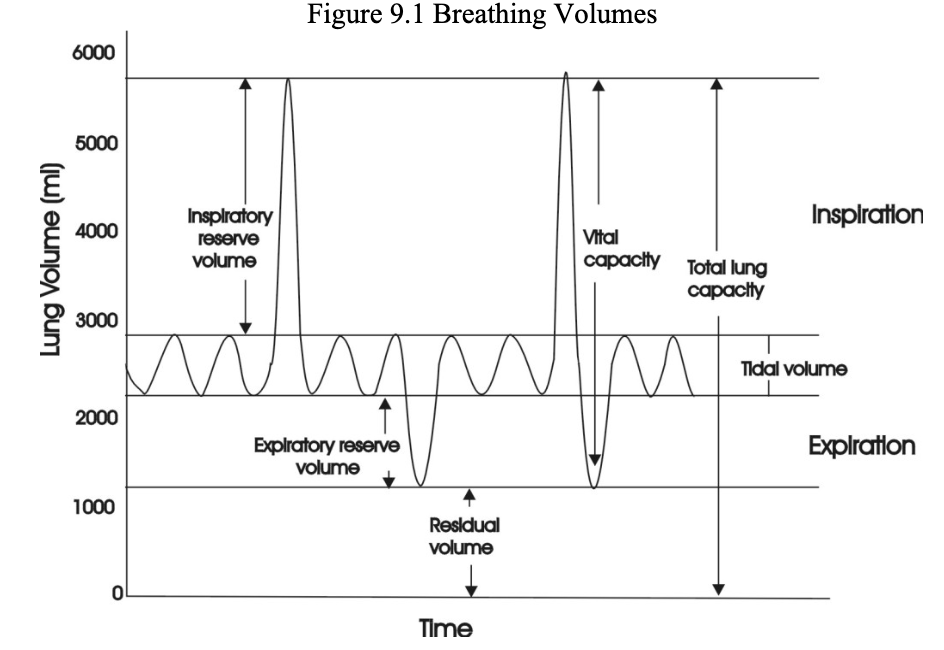
Breathing volumes
Tidal volume is about 500 mLs in males
normal resting respiratory rate is about 12-15 cycles per minute
minute volume = TV x RR
IRV = air inhaled past TV
ERV = air exhaled past TV
Vital Capacity = TV + IRV + ERV
Residual volume = air left in lungs
Total Lung Capacity = RV + VC
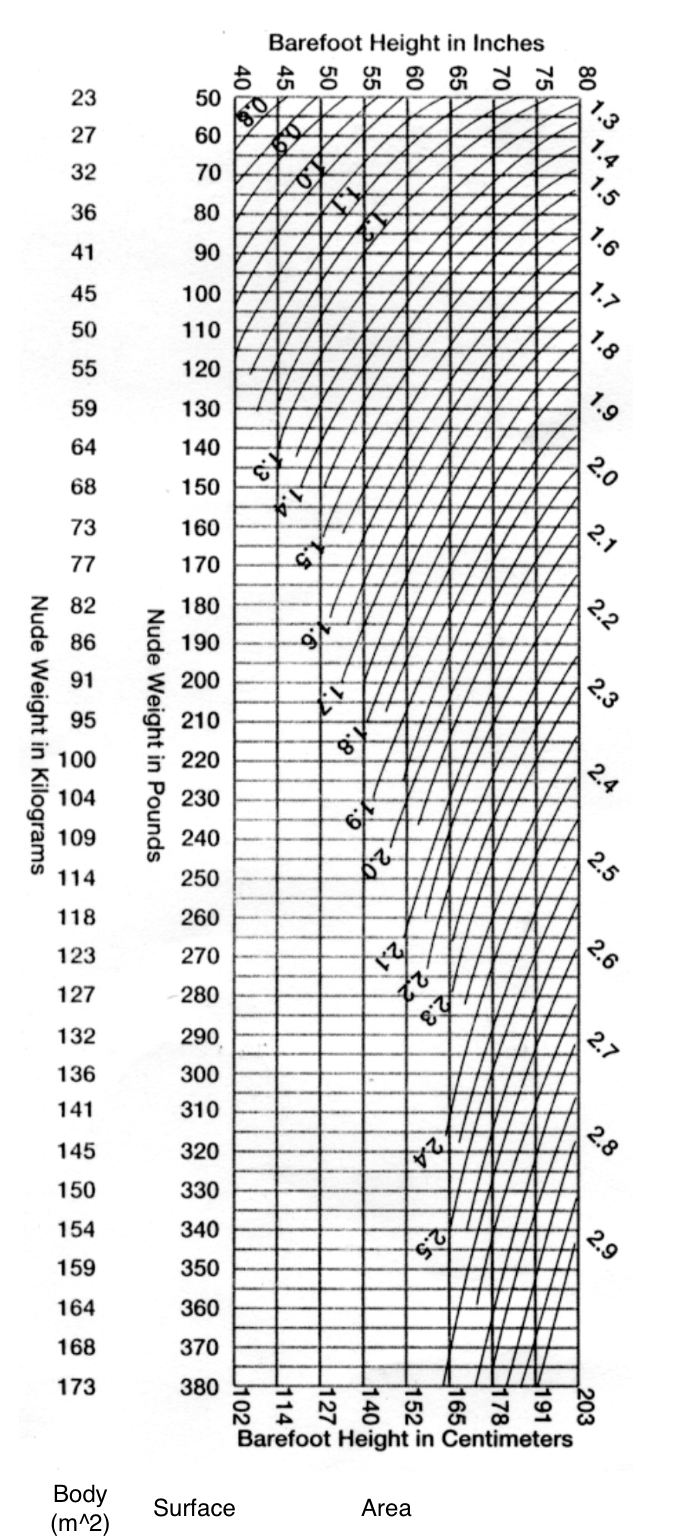
Respiratory volumes
these are usually compared in relation to one’s body surface area (BSA), expressed in meters squared (m2).
avg VC for a woman is ~2 L/m2 and for men it’s ~2.5 L/m2
BSA accounts for both height and weight and is a more reliable measure.
Pulmonary Volumes and Capacities
FEV and MVV
clinically measured and used to diagnose and assess pulmonary function → these tests alone don’t provide enough info.
two additional tests are usually performed.
These tests are referred to as the Forced Expiratory Volume (FEV) and the Maximum Voluntary Ventilation (MVV).
The FEV is measured when a subject is asked to expel his or her vital capacity as quickly as possible. After this maneuver is performed, one determines how much (in % of VC) air was expelled in a given amount of time (i.e. one second).
In normal adults, ~75% of the VC is expelled in the first second (referred to as the FEV1.0). After 2 seconds, 88% of the vital capacity should be expelled, and after 3 seconds, 94% of the V.C.
What two categories can respiratory diseases be placed into?
chronic restrictive pulmonary disease
chronic obstructive pulmonary disease
Chronic Restrictive Diseases
restrictive = restricts inhalation
In restrictive diseases the effective surface area available for gas exchange is reduced.
This is seen as a loss in lung volumes. These patients struggle to expand the lung and get air in.
The VC is greatly reduced in these patients as is the FEV1.0, although not to the same extent.
Thus, the ratio of FEV1.0/VC may not change. Pulmonary edema and pulmonary fibrosis are examples of restrictive diseases
Chronic Obstructive Diseases
trapping air → the obstruction of exhalation
patients with obstructive diseases (COPD) like asthmatics or those suffering from bronchitis or emphysema, have a difficult time moving air out of the respiratory airways.
These patients may have normal lung volumes and capacities. But, when asked to forcefully expire, the increase in airway resistance hinders the movement of air and thus all FEV values are reduced.
These patients may have FEV1.0/VC ratios less than 40%.
You will simulate this in lab by placing various resistances to air flow on the spirometers used in lab to measure the respiratory volumes

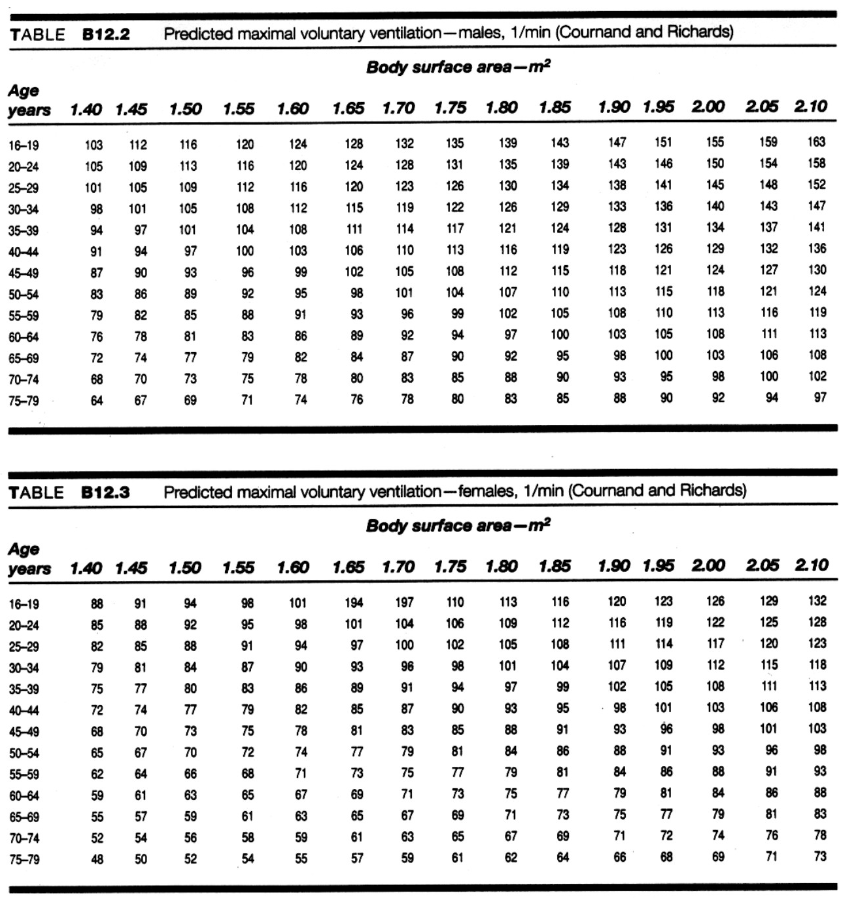
MVV Test
It is used to measure overall function with respect to ventilation. To
perform this test, the patient inspires and expires as deeply and/or rapidly as possible while the Tidal Volume and Respiratory Rate are measured.The product of the average volume per respiratory cycle (Liters) times the # of cycles per minute equals MVV (L/min)
Like VC, MVV values vary with BSA (body surface area).
The tables below show normal values based on gender, age and BSA.
In terms of pulmonary disease, MVV values will be reduced in both restrictive and COPD (chronic obstructive pulmonary disease) patients.
Control of Respiration
The rate and strength of contraction of respiratory muscles, and hence the rate and depth of respiration, are controlled by primary respiratory centers located in the medulla oblongata at the base of the brainstem.
The primary centers are inherently rhythmic, alternating their activity to produce inspiration and then expiration.
To adjust respiratory rate and depth according to the body's needs, the medullary centers receive inputs from higher neural centers (e.g., pons, cerebellum, cerebral cortex) and from peripheral receptors such as chemoreceptors in the aortic and carotid bodies, stretch receptors in joints, muscles, and tendons, and somatic sensory receptors for pain and thermal stimuli.
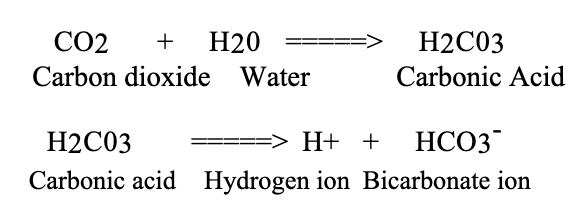
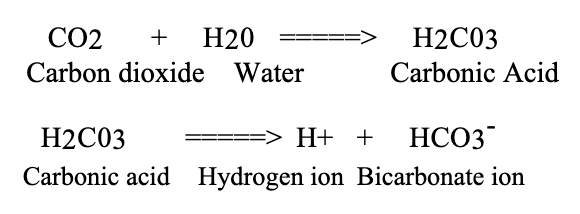
Respiratory System and CO2
Carbon dioxide is being continually produced during cellular metabolism.
As carbon dioxide is formed in body fluids, some of it reacts with body water to form carbonic acid, which releases hydrogen ions.
The hydrogen ions then tend to lower body fluid pH and stimulate respiration.
these reactions are reversible, so hydrogen ions may be removed
from body fluids by combining them with bicarbonate ions to form carbonic acid, breaking down carbonic acid to water and carbon dioxide, and then exhaling the carbon dioxideNormally the lungs eliminate carbon dioxide at the same rate as it is being produced by cells. Under such conditions, the above reaction sequence is at equilibrium, and no net change in hydrogen ion concentration occurs
Increased Respiration
If respiration is increased so that the lungs rid the body of carbon dioxide faster than it is being produced, the above reactions will move to the left; hydrogen ions will be removed from body fluids, and body fluid pH will become elevated (respiratory alkalosis).
This tends to depress respiration until normal carbon dioxide and hydrogen ion levels are restored. The temporary cessation of breathing after voluntary hyperventilation is known as apnea vera.
Hypoventilation
Hypoventilation of the lungs results in a net gain of carbon dioxide in body fluids, since the lungs fail to remove carbon dioxide as rapidly as it is being formed.
As a result, a net gain of hydrogen ions is due to the formation of carbonic acid (respiratory acidosis), and respiration is stimulated.
Elevation of respiratory rate and depth occurs until carbon dioxide and hydrogen ion levels are restored to normal
An increase in the carbon dioxide tension (partial pressure) in the body
fluids results in stimulation of medullary respiratory centers.Stimulation of respiratory rate and depth due to elevated partial pressure of carbon dioxide is caused by the resultant increase of hydrogen ions in cerebrospinal fluid.
Pulmonary ventilation will increase until carbon dioxide levels and extracellular fluid pH return to normal.
Increases in the carbon dioxide content (hypercapnia) and hydrogen ion content of arterial plasma also stimulate respiration by way of the chemoreceptor mechanisms of the aortic and carotid bodies.
FEV = FVC
FEV 1.0 vs FEV 3.0
normal averages: FEV 1.0 = 80% and FEV 3.0 = 95%
If a person was suffering from an obstructive disease like COPD (chronic obstructive pulmonary disease), what would happen to one’s residual volume?
1. Increase
2. Decrease
3. No Change
4. Cannot determine
Increase
air gets trapped in the lungs with obstructive diseases, so residual volume increases.
What would happen to their FEV1.0 ratio?
1. Increase
2. Decrease
3. No Change
4. Cannot determine
Decrease
obstructive prevents air from being fully exhaled, so FEV would decrease
What is the major physiological cause for an increase in ventilation during exercise?
b. The partial pressure of carbon dioxide in the lung.
Which of the following experiments in lab today was or were used to Which which of the following demonstrate the affect of the chemoreceptor reflex?
c. A and B
Hyperventilation changes the length of time one can hold their breath because......?
b. It reduces the amount of carbon dioxide in the blood thus the stimulus to breathe is reduced.
If a person’s minute ventilation was 5.2 liters per min and their tidal volume was 400 mLs, how fast are they breathing (i.e. how many breaths per minute are they taking)?
5.2 L x (1000 mL/ 1 L) = 5200 mL
5200 mL / 400 mL = 400 mL x R
13 = R
13 breaths per minute
The respiratory system and the circulatory system are fundamentally different. One is a closed system and the other is an open system. Which is open and which is closed?
Considering the two systems and their function explain how the design of the system (i.e. open or closed) is perfect for that function?
Open System = Respiratory
Closed System = Circulatory
Respiratory
open to exchange with the environment, if closed, no or difficult to exchange with the environment
Circulatory
Has no need to be open to the environment
When you were holding your breath, what was the primary stimulus that caused you to finally take a breath?
b. A high level of carbon dioxide in the blood.
Which of the following would increase pulmonary ventilation?
a. A decrease in blood pH.
b. An increase in blood carbon dioxide levels.
c. An increase in high altitude.
d. An increase in hydrogen ion content of the blood.
e. All of the above.
e. All of the above
When your subject exercised which changed more breathing rate or tidal volume? How do you know it changed the most?
tidal volume
TV = ((1.343 - 0.553) / 0.533) x 100 = 142%
BR = ((29.8 - 13) / 13) x 100 = 129%
TV had higher percent change
Kidney Functions
regulate the osmotic pressure of the blood, its pH, the balance of ions in the plasma, as well as remove nitrogen-containing and other wastes that must be excreted
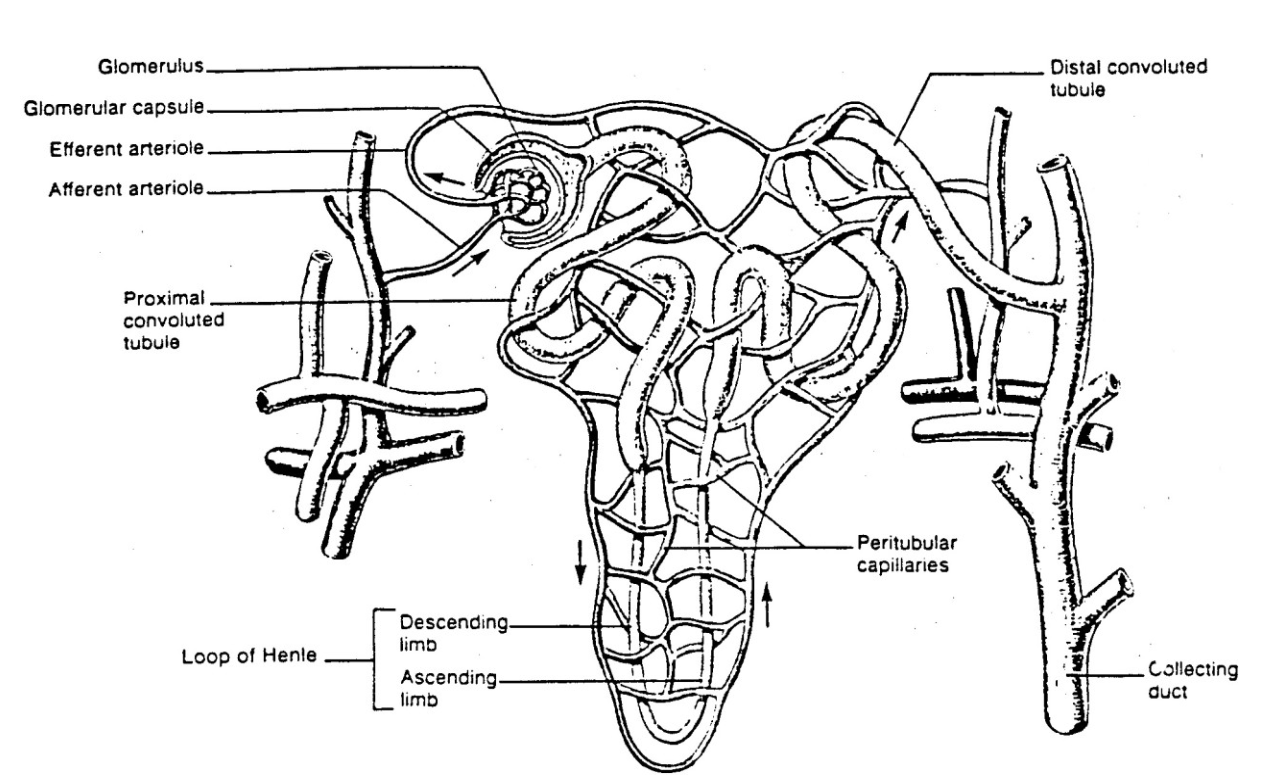
These functions are accomplished by many thousands of kidney units that are essentially similar, containing a kidney tubule or nephron, and surrounding capillaries
Urine Formation - First half of process
The first step in urine formation is filtration, as a portion of the plasma in the capillaries of the glomerulus is forced through the capillary walls into a hollow cup (Bowman's capsule) that is the beginning of the kidney (or renal) tubule.
The filtrate, now minus blood cells and blood proteins, enters the proximal tubule, where reabsorption begins the removal of substances that need to be saved (glucose, amino acids, salts, etc.), and water osmotically follows.
These reabsorbed substances move into a second set of capillaries that closely surrounds the tubule and are thus returned to circulation.
The proximal tubule leads to the Loop of Henle, which makes a
"hairpin" loop with descending and ascending limbs.Salt is actively pumped out of the ascending limb into the interstitial fluid, where it osmotically draws water out of the descending limb.
Water cannot re-enter the ascending limb, and the end result is that the interstitial fluid has an osmotic pressure at the bend of the loop about 4-5 times that of the tissue around Bowman's capsules.
The osmotic gradient thus established is maintained by blood capillary loops that parallel the loops of the Henle.
The highly reduced volume of filtrate next enters the distal tubule, where the adrenal cortical hormone aldosterone can increase the rate of sodium reabsorbed from the filtrate and thus saved. This action simultaneously lets more potassium go into the filtrate, releasing it in the urine
Urine Formation - second half of process
The final alteration of water content is made as the filtrate moves down the collecting tubule toward the cavity inside the kidney.
As the filtrate moves downward, it passes through increasingly higher osmotic tissue concentrations that tend to remove more water from the tubule.
The rate of water removal is controlled by the posterior pituitary hormone, anti-diuretic hormone or ADH (also called vasopressin).
Increased levels of this hormone make the collecting tubule cells more permeable to water, and thus more water exits the tubule, and urine volume is reduced.
This would save more water for the body if the blood were becoming too "salty" and would bring the osmotic pressure down to normal. If the level of water in the blood is too high, the secretion of ADH is cut back, and this makes the collecting tubule cells more impermeable to water, less leaves the tubule, and thus more water appears in the urine.
Normally only about 1% of the glomerular filtrate appears as urine
Glucose filtration
Usually the reabsorption of glucose is so complete that none appears in the urine.
Sometimes, after a meal rich in carbohydrate, blood glucose rises quickly, and before the kidney tubule cells have a chance to increase their rate of reabsorption, a small amount of glucose appears
in the urine.In normal kidneys, this trace rapidly disappears
Secretion
The process of secretion can also affect kidney function.
By secreting either more hydrogen ions or more bicarbonate ions, the kidney can keep the pH of the blood at a normal value of pH 7.4, in cooperation with the breathing system, which also can affect blood pH.
Since more of the substances to be removed from the body are acids, urine pH usually runs about pH 6.0, although it may be neutral or even slightly alkaline on diets low in protein and high in plant material.
Urine Color
The color of urine is due primarily to the pigment urobilin (or urochrome), which is a breakdown product of hemoglobin.
Since this is thrown away in relatively constant amounts, urine color will vary with the amount of water the kidneys excrete.
Which subject in the renal lab most likely, had the least amount of ADH in their blood?
Excess salt
Excess sugar
Excess Base
Excess Water
Excess water
ADH (antidiuretic hormone, also called vasopressin) is primarily regulated by plasma osmolarity and blood volume.
When you have excess water, plasma osmolarity decreases (blood becomes more dilute).
Osmoreceptors in the hypothalamus detect this and suppress ADH release.
Low ADH → kidneys reabsorb less water → more dilute urine is produced.
The body copes with changes in pH by using which of the following?
Buffers like proteins, and hemoglobin.
Ventilation
Renal excretion or reabsorption of H+ and bicarbonate.
All of the choices are correct.
All of the choices are correct
The body regulates pH through three coordinated systems:
Buffers (immediate response): Proteins and hemoglobin can bind or release H⁺ to resist rapid pH changes.
Ventilation (minutes): Adjusting breathing alters CO₂ levels, which shifts pH via the carbonic acid system.
Renal mechanisms (hours–days): The kidneys excrete or reabsorb H⁺ and bicarbonate (HCO₃⁻) to fine-tune pH.
Under which condition(s) will glucose appear in a normal person's urine?
if a person's brain does not need a lot of sugar.
if the person drinks a 50% sucrose solution like the one in lab this week.
if their kidney's approached but did not exceed their transport maximum.
None of the above.
4) None of the Above
In a normal person, glucose is freely filtered and then completely reabsorbed in the proximal tubule via transporters (SGLT), as long as the transport maximum (Tm) is not exceeded.
Glucose appears in urine (glucosuria) only when Tm is exceeded (e.g., very high blood glucose levels, like in uncontrolled diabetes).
Which of these listed below will not filter from the blood into the Bowman's capsule of a nephron?
Sodium
Large blood proteins like hemoglobin
Glucose
Potassium
2) large blood proteins like hemoglobin
Filtration at the glomerulus is based on size and charge:
Small solutes like sodium, glucose, and potassium are freely filtered into Bowman’s capsule.
Large proteins (and cells) are normally too big to pass through the filtration barrier.
SO, sodium, glucose, and potassium are all filtered, large proteins are not
Ingesting excess salt like some did in lab does which of the following?
Decreases specific gravity.
Decreases the release of the hormone ANF.
Increases renal bicarbonate reabsorption.
Increases the release of ADH.
4) increases the release of ADH
Excess salt intake raises plasma osmolarity.
Osmoreceptors in the hypothalamus detect this increase and stimulate ADH (antidiuretic hormone) release.
ADH acts on the kidneys to increase water reabsorption, helping dilute the excess salt.
Which of the following is regulated by the kidney?
Osmotic pressure of the blood
Blood pH
Plasma ion balance
All of the answers can be regulated by the kidney.
4) all of the answers can be regulated by the kidney
The kidneys are central to maintaining multiple aspects of internal homeostasis:
Osmotic pressure of the blood: regulated by adjusting water reabsorption and excretion (primarily via ADH influence).
Blood pH: regulated through secretion of H⁺ and reabsorption/generation of bicarbonate (HCO₃⁻).
Plasma ion balance: regulated by controlling levels of Na⁺, K⁺, Ca²⁺, Cl⁻, and others through selective reabsorption and secretion.
Because all listed functions fall under renal regulation, the correct choice is All of the answers can be regulated by the kidney.
Which of the following is true concerning the person who ingested the excess salt?
Blood osmolarity will increase.
Hydrogen ion content of the blood and urine increased.
Aldosterone secretion will increase.
ADH decreases
1) blood osmolarity will increase
Ingesting excess salt (NaCl) increases the concentration of solutes in the blood.
This directly raises blood osmolarity.
High salt → high osmolarity → stimulates ADH, helping retain water to dilute the blood.
Which of the following statements describes what was occurring in the body of the subjects who ingested the sodium bicarbonate?
the pH of the urine increased because there were too many hydrogen ions.
the volume of urine increased in order to dilute the excess base.
the pH of the urine increased because of the excess base in the blood and filtrate.
the volume of urine increased to neutralize the acid.
3) the pH of the urine increased because of the excess base in the blood and filtrate
Sodium bicarbonate (NaHCO₃) is a base, so ingestion increases blood bicarbonate levels → causes a metabolic alkalosis tendency.
The kidneys respond by excreting excess bicarbonate (HCO₃⁻) into the urine.
Because bicarbonate is basic, its presence in urine raises urine pH (makes it more alkaline).
The kidney corrects alkalosis by excreting bicarbonate, which makes urine more basic → urine pH increases.
True or False: The specific gravity of urine will decrease with diuretics like Lasix that act on the loop of Henle.
True
Lasix (furosemide) is a loop diuretic that blocks the Na⁺/K⁺/2Cl⁻ cotransporter in the thick ascending limb of the loop of Henle.
This disrupts the kidney’s ability to create a hyperosmotic medulla, reducing water reabsorption downstream.
As a result, more water is excreted relative to solutes → urine becomes more dilute.
Specific gravity reflects solute concentration in urine.
More dilute urine → lower specific gravity.
True or False: Glucose that is filtered from the blood is always excreted.
False
Glucose is freely filtered at the glomerulus, but in a normal kidney it is almost completely reabsorbed in the proximal tubule via SGLT transporters.
As long as blood glucose is below the renal transport maximum (Tm), no glucose appears in urine.
Only when blood glucose is high enough to exceed Tm (e.g., uncontrolled diabetes mellitus), or if transporters are impaired
True or False: Excess water increases ANP levels in the blood stream.
True
ANP (atrial natriuretic peptide) is released by the atria of the heart when they are stretched.
Excess water intake increases blood volume, which increases venous return and stretches the atria.
This stretch triggers increased ANP release.
ANP function
Promotes sodium excretion (natriuresis) and water loss in the kidneys
Inhibits aldosterone and ADH
Helps reduce blood volume and blood pressure
True or False: An increase in the concentration of ADH would increase the volume of urine output.
False
ADH (antidiuretic hormone) increases water reabsorption in the collecting ducts by inserting aquaporin channels.
More ADH → more water reabsorbed back into the bloodstream.
This results in:
Decreased urine volume
More concentrated urine
True or False: The reason urine output is normally small compared to what is filtered is due to the high concentration of solutes outside the collecting duct.
False
The small urine output relative to filtrate volume is mainly due to selective reabsorption of water and solutes in the nephron (especially the proximal tubule and loop of Henle), not simply because of solute concentration outside the collecting duct.
The key driver of water reabsorption in the collecting duct is the osmotic gradient in the renal medulla, which is established by:
NaCl reabsorption in the loop of Henle
Urea recycling
Regulation by ADH
it’s the combination of nephron reabsorption processes + medullary osmotic gradient + ADH regulation that determines final urine volume.
You are working in the ER, patient comes in and an arterial blood gas sample is drawn. The results show that the patient is suffering from a condition known as respiratory acidosis. A urine sample is collected. What do you except the pH of this urine sample to be?
normal
below normal of 7.4.
have a pH of 12.
above normal of 7.4.
below normal, acidic urine.
The kidneys respond by:
Increasing H⁺ secretion into urine
Increasing HCO₃⁻ reabsorption into blood
Result in urine:
More H⁺ excreted → urine becomes more acidic than normal
So urine pH is below normal (~< 6 rather than 7.4)
A decrease in blood osmolarity would cause:
an increase EPO from the Kidney
a decrease in the release of ANP from the heart
inhibition of ADH secretion from the posterior pituitary gland.
a decrease in Aldosterone from the adrenal gland
3) inhibition of ADH secretion from the posterior pituitary gland
Blood osmolarity decreases → blood becomes more dilute (excess water relative to solutes).
Osmoreceptors in the hypothalamus detect this change and respond by reducing ADH release from the posterior pituitary.
Less ADH → decreased water reabsorption in the collecting ducts
More dilute urine → increased water excretion
Helps restore normal osmolarity
The reason for calculating the amount of chloride in our samples was to:
1. see how much potassium was excreted.
be able to calculate the amount of solids in each sample.
figure out the change in pH.
estimate the amount of sodium in each sample.
4) estimate the amount of sodium in each sample
In physiology labs, chloride (Cl⁻) is often measured because it is the major accompanying anion of sodium (Na⁺) in extracellular fluid.
Since sodium and chloride are usually present in a ~1:1 relationship in plasma and many physiological fluids, measuring chloride allows you to indirectly estimate sodium concentration.
True or False: Maintaining blood pH is a function that the respiratory system and the renal system have in common.
True
Both the respiratory system and the renal system play essential roles in maintaining blood pH homeostasis, but they act on different time scales and mechanisms:
Respiratory system (fast, minutes):
Regulates CO₂ levels
CO₂ + H₂O ⇌ H₂CO₃ ⇌ H⁺ + HCO₃⁻
Increasing ventilation lowers CO₂ → raises pH
Decreasing ventilation raises CO₂ → lowers pH
Renal system (slow, hours to days):
Regulates H⁺ secretion and HCO₃⁻ reabsorption/production
Provides long-term correction of acid–base balance
An increase in blood pressure will cause a decrease in the amount of circulating ADH. What is the relationship between a decrease in ADH and high blood pressure?
a decrease in ADH would allow more water to be excreted and thus maintain blood pressure by reducing blood volume
High blood pressure → decreased ADH release
Less ADH means:
Reduced insertion of aquaporins in the collecting ducts
↓ water reabsorption
↑ water excretion in urine
This leads to a decrease in blood volume, which helps lower or stabilize blood pressure
ADH is a water retention hormone—so lowering it promotes water loss, which reduces blood volume and helps correct high blood pressure
What is the relationship between specific gravity and urine formation?
specific gravity and flow rate are inversely related (i.e. as one goes up the other goes down).
specific gravity is equal to flow rate.
specific gravity is directly proportional to the rate of urine formation.
specific gravity and flow rate are not related at all.
1) specific gravity and flow rate are inversely related
Specific gravity measures how concentrated urine is (amount of dissolved solutes).
Urine flow rate reflects how much urine is being produced per unit time.
Relationship:
When urine flow rate is high (e.g., diuretics, low ADH):
Less time for reabsorption
Urine is more dilute
Specific gravity decreases
When urine flow rate is low (e.g., high ADH, dehydration):
More water is reabsorbed
Urine is more concentrated
Specific gravity increases
How to determine specific gravity
last 2 digits of specific gravity x 2.66 = solids g/L
solids/sample: g/L x volume of sample
e.g. Specific gravity = 1.015
solids: 15 × 2.66 = 39.9 g/L
solids/sample: 39.9 g/L x 0.6L/sample = 23.9 g/sample
Determination of Chloride Concentration
Measure 10 drops of urine into a test tube
• 1 drop = 0.05 mLAdd 1 drop of 20% potassium chromate solution
Using the 2.9% silver nitrate solution, add 1 drop at a time
• Shake well after each addition
• Count the number of drops needed to observe a color change
• Yellow to brown-brick red
Why does sugar end up in the urine of a diabetic?
hyperglycemia: high blood sugar, overwhelms the kidney’s ability to reabsorb glucose into the bloodstream
when blood sugar levels exceed a certain level, the renal threshold, the transport proteins become saturated, and the high glucose levels in a diabetic overwhelm the kidney, causing excess to spill into the urine.
Metabolic Acidosis
Primary cause: dietary and metabolic input of H+ exceeds excretion. (Ex: Diabetes-ketoacids, fruit juice)
high CO2 + H2O <→ high H+ + HCO3-
increase H+(and decrease pH/acidic), causes equation to drive left, and then HCO3- decreases
will cause CO2 to increase
Response: Decrease CO2 (hyperventilation)
Metabolic Alkalosis
Primary cause: HCO3- excess (Ex: drinking sodium bicarbonate water in lab today)
high CO2 + H2O <→ low H+ + high HCO3-
will increase HCO3- (increase pH/basic), causes equation to drive left, and then lower H+
will cause CO2 to increase
Respiratory Acidosis
Primary cause: increased CO2 (hypercapnia ) due to hypoventilation. (ex. COPD)
high CO2 + H2O <→ high H+ + high HCO3-
increase CO2, causes equation to drive to the right
H+ and HCO3- will increase (causing blood pH to decrease/become acidic)
Response: Increased reabsorption of HCO3- and/or excretion of H+
Respiratory Alkalosis
Primary cause: decreased CO2 (hypocapnia) due to hyperventilation. (ex. Anxiety, high altitude)
Low CO2 + H2O <–> low H+ + low HCO3-
decrease CO2, causing equation to drive to the left
H+ and HCO3- will decrease (causing blood pH to increase/become basic)
Response: Must be Renal
decreased reabsorption / increased secretion HCO3 / increased reabsorption of H+
The excess sugar drinker did not exceed the transport maximum for glucose
of the kidney because?
c. The kidney was capable of producing enough transporters to meet the
demand.
What is the relationship between specific gravity and urine flow rate
b. Inversely proportional
Diuretics like alcohol are chemicals that increase the volume of urine
excreted. What would you expect a patient’s urine specific gravity and urine
flow rate to be if they had large amounts of these substances in their bodies?
c. Specific gravity would be low and urine flow rate would be high.
How does your body “know” that it just ingested an excess amount of water? In other words, what are the stimuli that trigger your body to respond to the amount of water you just took in?
an increase in water causes:
increased pressure
decreased osmolarity
How do these signals (high pressure, low osmolarity) lead to an increase in urine flow rate?
high blood pressure is bad for the body, so that will cause an increase in secretion and excretion to remove the extra water/fluid from the body
Sarah P. is 25 weeks pregnant and was in for her routine exam. Her blood
pressure was 160/110. The physician is concerned about preclampia so
orders a urine test. The high blood pressure could be altering filtration by
pushing substances across the glomerulus that should not show up in the
urine.
what will her urinalysis contain?
due to the concern of preeclampsia and the high blood pressure, she will likely have cloudy urine due to filtration issues caused by the high blood pressure
the urine is cloudy due to proteins being present in it from the filtration issues
Riley M. is a 28 year old human physiology student at Washburn. She is so
stressed that she eats TUMS (an antacid) by the handful and takes Prilosec
(over-the-counter proton pump inhibitor, decreases acid in the stomach). She
is afraid she has developed an ulcer and went to see her physician.
The physician ordered a urinalysis.
the urine sample will be basic due to stress-eating TUMS and taking Prilosec.
Mark P. is a 19 year old male student who has noticed that his urine output
and appetite have increased. He complains about being thirsty all the time and has lost weight.
What will the urinalysis contain?
his symptoms align with those of type 1 diabetes: polyuria, polyphagia, and polydipsia.
His urinalysis would be glucose positive due to the kidneys being overwhelmed by the amount of sugar in the blood, thus causing receptor saturation and therefore glucose leaking into the urine.
Mark is an ultra-distance runner. He has come in from a 50 mile training run. He appears disoriented, face is covered in dry salt and is asking for water
what is his urinalysis?
he is dehydrated so his urine will be highly concentrated and dark
the urine will be highly acidic due to high concentration
Marty is a 21 year old male who came in for a routine physical exam and
urinalysis for insurance purposes.
what will his urinalysis look like?
normal values
normal pH, glucose negative, and protein negative
What is the average pH of urine?
6.0
ranges from 4.5 - 8.0
What is a GSR?
Galvanic Skin Response
one of several electrodermal responses (EDRs)
EDRs are changes in the electrical properties of the human skin which occur due to an interaction between environmental events and an individual's psychological state
The human skin is a good conductor of electricity and when a weak electrical current is delivered to the skin, you can measure changes in the skin’s conduction of that signal
What is measured is either skin resistance or its reciprocal, skin conductance
Ohm’s Law and Skin Conductance
According to Ohm's Law, skin resistance ®) equals the voltage (V)
applied between two electrodes on the skin, divided by the current passed through the skin (I).The law can be expressed as R=V/I.
Skin Conductance
The GSR Amp, which is interfaced to your iWorx/204, applies a
constant voltage to the skin electrodes so that current flow through the skin can be measured.The voltage is so small you cannot perceive it, nevertheless the small changes in current flow which occur can be detected and displayed.
The current flow will vary with the skin conductance.
The output of the amplifier will be displayed as skin conductance in units called microsiemens (μS).
Tonic Skin
Tonic skin conductance refers to
the ongoing or baseline level of skin conductance in the absence of any particular discrete
environmental event. Tonic skin conductance is generally referred to as Skin Conductance Level
(SCL). Individuals will differ from one another in the SCL in μS, with typical tonic levels ranging
from 10-50 μS. Also, tonic level of skin conductance will vary over time in individuals depending
on psychological state and autonomic regulation.