PYSCH EXAM 3 study guide q's
1/25
Earn XP
Description and Tags
kill me now
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
26 Terms
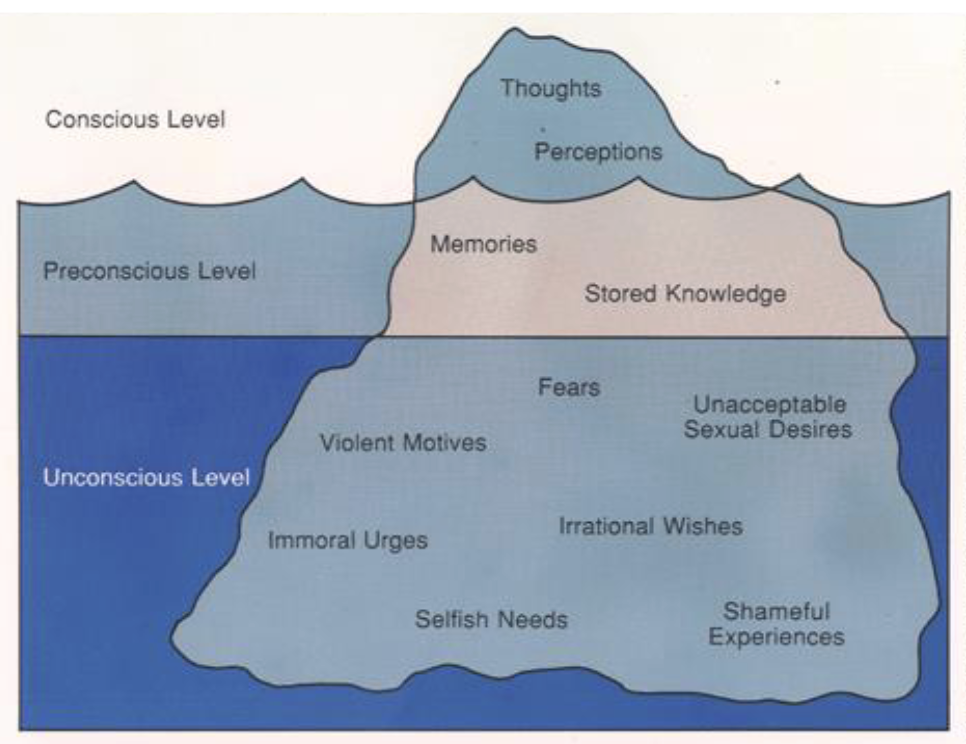
Name and describe the three levels of the mind according to Freud
Conscious: surface thoughts
EX: Thoughts and perceptions
Preconscious: information can be brought
to conscious.
EX: memories and stored knowledge
Unconscious: information of which we are
largely unaware
– Representations exist in preconscious and
conscious
EX: fears, violent motives, irrational wishes, unacceptable sexual desires, selfish needs, shameful experiences, immoral urges
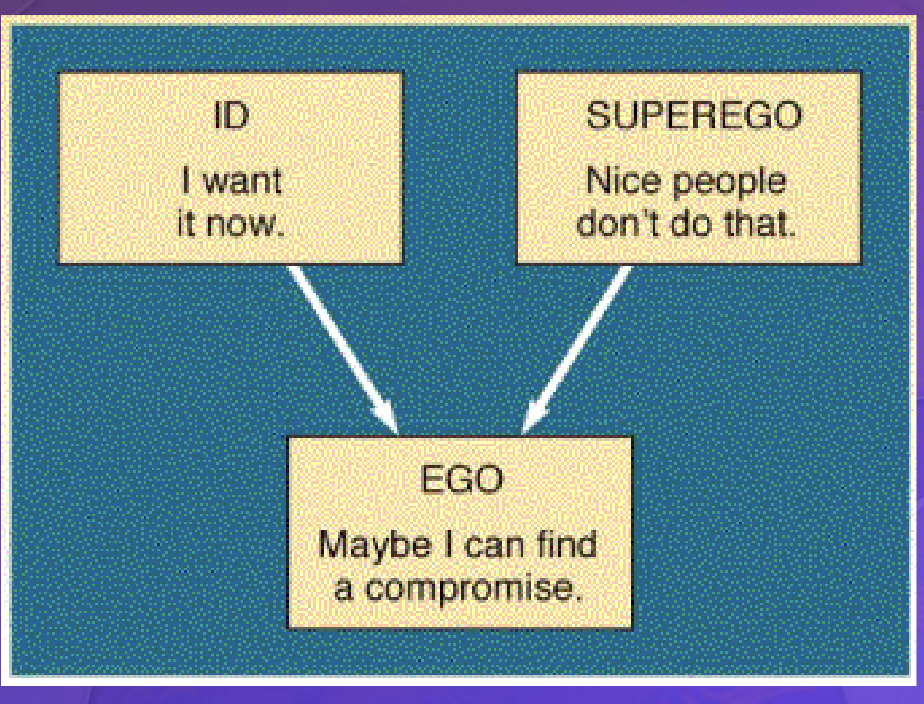
What were the three components of personality, according to Freud?
Id: concerned with immediate
gratification (pleasure)Superego: represents the conscience;
ruled by morality (ideal)Ego: compromises between demands of
the Id and external world (reality)
What were Freud’s stages of personality development? Describe each of them, as well as what
happens when an individual becomes fixated at each stage
Oral Stage: (FIRST 18 MONTHS) mouth as the primary pleasure center
Fixation: -Oral-aggressive personality – Oral-dependent personality
Anal Stage: (18 TO 36 MONTHS) children learn to balance between immediate gratification obtained through defecation and demands of society
Fixation: - Anal-expulsive personality – Anal-retentive personality
Phallic Stage: (3 TO 6 YEARS) children obtain gratification, primarily from the genitals
Fixation: Oedipus complex: a son’s feelings of sexual desire
for his mom & rivalry w/dad Result: Castration Anxiety
Electra complex: a daughter’s hostile feelings towards mom & sexual love toward dad, Result: Penis Envy
Latency Stage: (6 YEARS TO PUBERTY) children develop physically, but sexual urges are inactive
Fixation: Generally, this is a dormant period, but difficulties here may lead to weak social skills.
Genital Stage: (PUBERTY ON) sexuality re-emerges; learn to engage with members of the opposite sex in mature ways
Fixation: If prior stages were not successfully resolved, individuals will carry their neuroses into adulthood, struggling with relationships and balance.
How do psychologists from the behavioral and social cognitive perspective describe personality?
How does the humanistic perspective describe personality?
View people as possessing free will
• Stems from existentialism
the result of an individual's innate drive toward self-actualization and personal growth.
Name and describe the Big Five personality traits
The Big-Five Personality Dimensions | |
Dimension | Defining Descriptors |
Openness to experience | Artistic, curious, imaginative, insightful, original, wide interests, unusual thought processes, intellectual interests |
Conscientiousness | Efficient, organized, planful, reliable, thorough, dependable, ethical, productive |
Extraversion | Active, assertive, energetic, outgoing, talkative, gesturally expressive, gregarious |
Agreeableness | Appreciative, forgiving, generous, kind, trusting, noncritical, warm, compassionate, considerate, straightforward |
Neuroticism | Anxious, self-pitying, tense, emotionally unstable, impulsive, vulnerable, touchy, worrying |
Describe some of the criticisms of Freudian theories.
lacking empirical, scientific testability, being based on subjective, non-representative case studies, and placing an overemphasis on sexuality and childhood experiences.
How was mental illness explained and treated in the past?
Prehistoric views:
Human body was a battleground between good
and evil, Abnormal behavior = victory by evil spirits
Treatments:
rephination: operation in which circular
section of the skull was cut away and Exorcism
Greek & Roman views
Hippocrates: abnormal behavior caused by an
imbalance of humors (bodily chemicals)
Treatment: restore balance of fluids
The Middle Ages
Return to focus on good vs evil, New methods of treatment
Popular = exorcism
The Renaissance
Recognition of a “sick” mind
creation of asylums
19th century
Rise and fall of “moral” treatment
Establishment of state hospitals
Changing view of mentally ill
How to psychologists decide what is abnormal? How does this determination differ between
different perspectives of psychology (cognitive, behavioral, psychodynamic, etc)?
Psychologists decide behavior is “abnormal” when it is unusual, violates social norms, causes distress, or makes it hard to function, often using at least two of these signs to diagnose a disorder.
Different perspectives explain it differently:
cognitive focuses on unhealthy thought patterns
behavioral sees abnormal behavior as learned
psychodynamic looks at unconscious conflicts
biological explains it through genetics or brain/chemical problems.
What is the DSM-5, and what is it used for?
Diagnostic and Statistical Manual of Mental Disorders, the prevalent resource to help psychological professionals diagnose psychological disorders
What are some examples of anxiety disorders, and what are their symptoms?
Social anxiety disorder – fear of social situations, fear of being judged, embarrassment, extreme self-consciousness
Specific phobia – irrational fear of a certain object or situation, avoidance of the feared object
Agoraphobia – fear of places where escape is difficult, avoidance of crowds, public places, or leaving home
Panic disorder – sudden panic attacks, racing heart, sweating, rapid breathing, dizziness, fear of dying
Generalized anxiety disorder – constant excessive worry, tension, irritability, fatigue, trouble concentrating, sleep problems
What are some behavioral and cognitive factors which may lead to anxiety disorders?
chronic avoidance of feared situations, perfectionism, overthinking, and cognitive distortions like catastrophizing
What are the symptoms and causes of different mood disorders?
Major Depressive Disorder
Symptoms: persistent sadness, loss of interest, fatigue, sleep/appetite changes, guilt, trouble concentrating
Causes: learned helplessness, negative thinking patterns, brain chemical imbalances, geneticsBipolar I Disorder
Symptoms: manic episodes with extreme energy, euphoria, irritability, rapid speech, risky behavior, sometimes depression
Causes: brain chemical imbalances, geneticsBipolar II Disorder
Symptoms: major depressive episodes with hypomania (less severe mania)
Causes: brain chemical imbalances, genetics
What are the symptoms and causes of eating disorders?
Anorexia Nervosa
Symptoms: extreme weight loss, refusal to eat, distorted body image, excessive exercise, weakness, sleep problems
Causes: genetics, fear/anxiety about food, cultural pressure to be thinBulimia Nervosa
Symptoms: binge eating followed by vomiting, laxatives, fasting, excessive exercise, normal weight, tooth decay
Causes: genetics, anxiety/depression, distorted thinking, cultural pressure to be thinBinge-Eating Disorder
Symptoms: repeated binge eating without purging, lack of control overeating
Causes: genetics, sensitivity to food reward, emotional stress
How do dissociative disorders develop?
disorders involving changes in consciousness or self-identity. severe, chronic trauma, particularly during childhood,
What are the positive symptoms of schizophrenia? What are the negative symptoms? How do
they differ from one another
Positive Symptoms: an added element that is
not normally present
Delusions: false, but unshakable beliefs
Hallucinations: Perceptual experiences that occur
without any actual physical stimulus
Negative Symptoms: a deficit of normal
performance
Disorganized speech
Disorganized or catatonic behavior
What are the symptoms and causes of personality disorders?
Histrionic Personality Disorder:
Overly dramatic and emotional
Excessive need to be the center of attention
Constant demands for reassurance, praise, and
approval
Narcissistic Personality Disorder:
Inflated or grandiose self-image
Extreme needs for admiration (from
others)
Antisocial Personality Disorder:
A pattern of antisocial and irresponsible behavior
Flagrant disregard for the interests & feelings of
others
A lack of remorse
Paranoid PD
Symptoms: distrust, suspects harm, holds grudges
Antisocial PD
Symptoms: breaks rules, lies, uses others, no remorse
Borderline PD
Symptoms: unstable relationships, fear of abandonment, impulsive, mood swings
Dependent PD
Symptoms: needy, passive, can’t decide alone, fears abandonment
How did Freud conduct psychoanalysis? What are the differences between the latent and
manifest content within dreams, according to Freud?
Couch therapy with writing notes behind head of couch so as the patient cant see him. A;sp with dream interoperation and free association (his patients to freely say whatever came into their minds)
Dream analysis:
◼ Manifest content: reported, actual content
of dreams
◼ Latent content: symbolized or underlying
content of dreams
How does psychodynamic therapy today differ from Freud’s original methods of
psychoanalysis?
Freud’s original psychoanalysis was long-term, often several sessions per week for years, and used techniques like free association, dream analysis, and a passive therapist interpretation of unconscious conflicts.
Today’s psychodynamic therapy is:
Shorter-term and more focused (not years-long)
Less intensive (usually 1 session per week)
More collaborative (therapist is more active, not just interpreting)
Focuses on current problems and relationships, not only deep unconscious conflicts
Uses less emphasis on techniques like dream analysis
What are the similarities and differences between Person-centered therapy and Gestalt therapy?
Similarities:
Both are based in humanistic ideas
Both focus on feelings, awareness, and client experience
Both use the therapist–client relationship
Differences:
Person-centered therapy: nondirective; client talks freely, therapist gives minimal guidance and empathy
Gestalt therapy: very directive; therapist uses confrontation and planned experiences (role-play, empty chair) to increase awareness and responsibility
Motivational interviewing (MI): “client-centered with a twist”; has specific goals (reduce ambivalence, increase motivation to change) and includes structured processes like engaging, focusing, evoking motivation, and planning change
What are some examples of applied behavior analysis, and how do they alter an individual’s
behavior?
What are the differences between flooding and gradual exposure and systematic desensitization? How effective are each of these therapies?
Systematic desensitization and gradual (graded) exposure both use a step-by-step approach to face fears, while flooding involves immediate, maximum-intensity exposure
Gradual Exposure & Systematic
Desensitization:
▪ Clients learn relaxation techniques
▪ Construct fear hierarchy
▪ Slowly master each step of fear hierarchy
flooding: echnique for treating phobias and other stress disorders in which the person is rapidly and intensely exposed to the fear-provoking situation or object and prevented from making the usual avoidance or escape response.
gradual exposure:
systematic desensitization: behavior technique used to treat phobias, in which a client is asked to make a list of ordered fears and taught to relax while concentrating on those fears.
What are the three basic goals of cognitive-behavioral therapy?

What factors influence the effectiveness of psychotherapies, and how effective are they?
What types of drugs are used to treat psychological disorders? How do they work?
What are some examples of psychosurgeries, and how can they treat psychological disorders?