exam 2 pulm
1/410
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
411 Terms
What class of beta blockers are used in COPD patients?
Selective (BMEAN), lower mortality
What is primarily effected by chronic bronchitis?
goblet cells and the glands, hyperactivity will lead to overproduction of mucus and narrowing of the airways
With emphysema there is destruction of ___
alveoli
What naturally activates the M3s?
acetylcholine (bronchial constrict the airways)
In COPD, ____ are not very effective
SABAs
ACh activation of M3 receptors most likely has what effect?
bronchial constriction
COPD is characterized by what?
chronic inflammation of the small airways
What are the two classes of COPD?
1. emphysema (alveolar wall destruction)
2. chronic bronchitis (airflow and mucus production)
What immunemediators attribute to COPD?
neutrophils
macrophages
cytotoxic T-lymphocytes
T helper 17 cells
Key points of COPD
irreversible and progressive
largely corticosteroid resistant
COPD pts have many comorbidities (IHD, HTN, CHF, Diabetes, depression)
COPD definition
airflow limitation that is not fully reversible, it is progressive and associated with abnormal inflammatory response
COPD patients typically present with what symptoms?
dyspnea
chronic cough
sputum production
COPD precipitating factors
Tobacco smoke (85-90%) --> vaping is also an issue but less evidence as of right now
Occupational
Genetic
Cigarettes inhibit what?
ciliary movement
How does smoking cause COPD?
fibrosis/airway remodeling (makes it harder to breathe/dilate)
alveolar wall destruction (Emphysema)
Mucus overproduction (chronic bronchitis)
What is the main difference between asthma and COPD?
asthma is reversible, COPD is not
Blue bloaters
chronic bronchitis patients (increased mucus production)
Pink puffers
Emphysema (alveolar wall destruction)
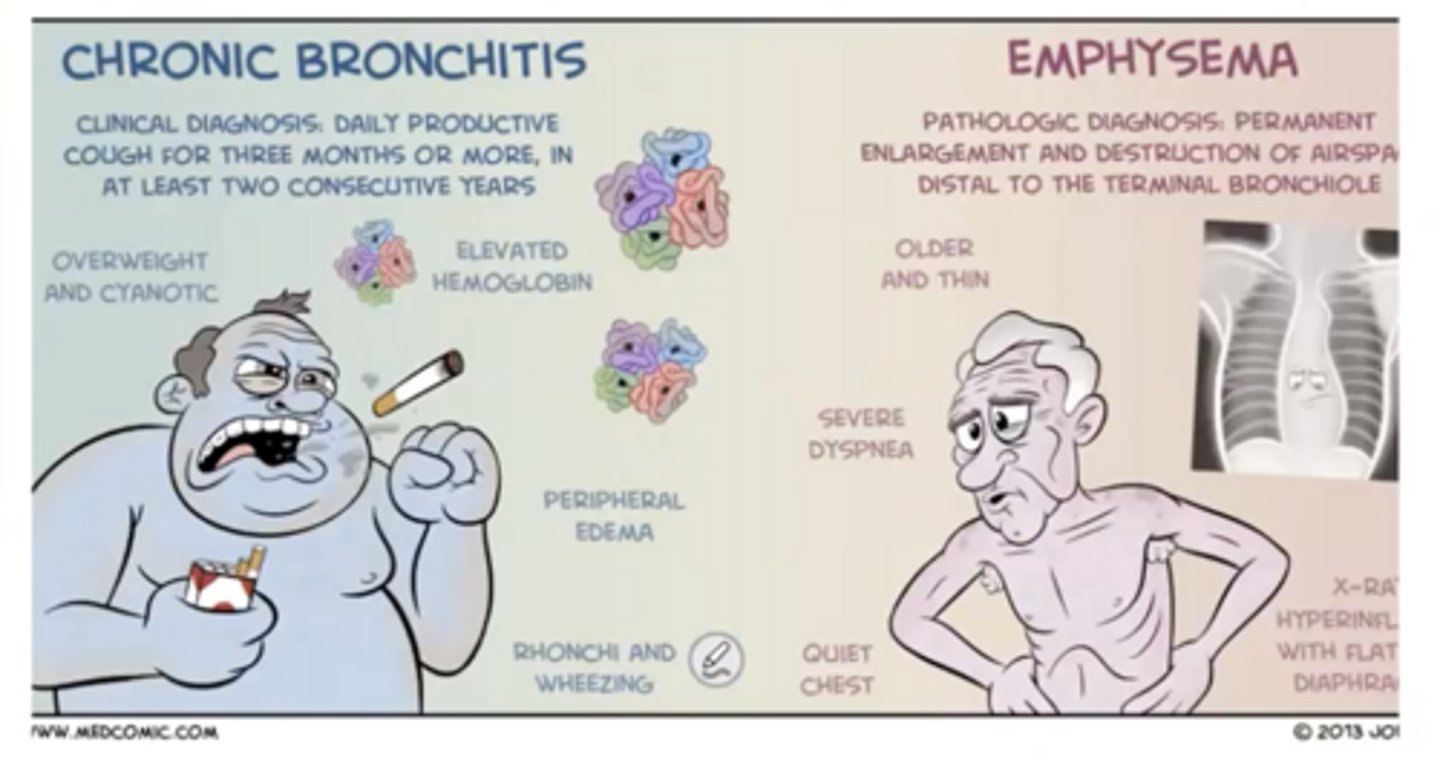
Chronic bronchitis definition
a persistant cough with sputum production for at least 3 months in 2 consecutive years
How is chronic bronchitis characterized?
inflammation of airways
hypertrophy of large airway mucous glands
increase mucous secretion
mucus obstruction of airways
ventilation/perfusion mismatching (decreased O2 and increased PC) that can lead to respiratory acidosis and polycythemia --> cyanosis
Emphysema
destruction of septa (decreased elastic recoil) --> work to breathe in and breathe out
less mucus production
smooth muscle hypertrophy
red and pink
What two SABAs are used in COPD?
albuterol (Ventolin) and levalbuterol (Xopenex)
B2 agonists are the most potent what?
bronchodilators
What is the most effective drug in COPD patients?
LAMAs, anticholinergic drugs may be as effective as or even superior to B2 agonists by inhibiting PNS
LAMAs have what effect?
Improve lung function
Reduce exacerbations
Reduce mortality
LAMAs decrease ___ and increase ___
mucus production and dilation
Anoro Ellipta
vilanterol + umeclidinium (LABA + LAMA)
Stiolto Respimat
olodaterol + tiotropium (LABA + LAMA)
Duaklir Pressair
formoterol + aclidinium (LABA + LAMA)
Bevespi Aerosphere
formoterol + glycopyrrolate (LABA + LAMA)
Trelegy Ellipta
fluticasone furoate/umeclidinium/vilanterol (LABA/LAMA/ICS)
Breztri Aerosphere
budesonide + formoterol + glycopyrrolate (LABA + LAMA + ICS)
Atrovent
Ipratropium (SAMA)
Spiriva
Tiotropium (LAMA)
Tudorza
Aclidinium (LAMA)
Incurse Ellipta
Umeclidinium (LAMA)
Glycopyrrolate
LAMA
Revefenacin
LAMA (nebulizer)
Major complaint of antimuscarinics
dry mouth
Combivent
ipratropium/albuterol (LABA/SABA)
ICS are ____ in the treatment of COPD than asthma
far less effective, resistant to therapy
When are ICSs effective in COPD?
reducing exacerbations in severe patients, increased blood eosinophils (over 300)
ICSs are more effective as __
triple therapy (ICS + LABA + LAMA)
Corticosteroids decrease __ and indirectly decrease __
inflammation and hyper-responsiveness, airway flow
In COPD, ICSs do not what?
address the underlying cause of the disease
Which steroids are systemic?
Dexmethasone
Prednisone
Prednisolone
Methylprednisolone
QVAR
Beclomethasone (most potent)
Nasonex
Mometasone
Asmanex
Mometasone
Flonase
fluticasone
Beconase
beclomethasone
Rhinocort
budesonide
Pulmicort
budesonide
Alvesco
ciclesonide
Arnuity
fluticasone furoate
Flovent
fluticasone propionate
Airsupra
budesonide/albuterol
Dulera
mometasone/formoterol
Major steroid side effects
hoarseness and dysphonia
thrush
Theophylline
Xanthine derivative
Narrow TI
Substrate 1A2, 2E1, and 3A4
Weak PDE antagonist
Causes some bronchial dilation and anti-inflammatory response
What affect does blocking the PDE4 have?
increases levels of cAMP and decreases degranulation
Roflumilast. brand name
Daliresp
Roflumilast (Daliresp) MOA
selective PDE4 antagonist --> less degranulation and inflammation but not as potent so cannot be used as monotherapy
Dupilumab brand name
Dupixent
Dupilumab (Dupixent) MOA
monoclonal antibody directed against the IL-4a co-receptor for both IL-4 and IL-13
When is Dupilumab (Dupixent) used?
As adjunct therapy to reduce rate of exacerbation in COPD with high eosinophil levels
Azithromycin MOA
Inhibitor of bacterial protein synthesis by reversibly antagonizing the 50S ribosomal subunits which terminates protein synthesis by interfering with transpeptidation and translocation, also has anti-inflammatory properties
Bacterial infections can ___
precipitate COPD exacerbation
Azithromycin side effects
GI distress (may cause loss of potassium)
QTc prolongation (potassium channel blockade)
COPD is a ___
progressive abnormal inflammatory response to airborne chemicals
What problem is associate with COPD?
chronic inflammation with lung damage
What is the long term management of COPD?
LABAs/LAMAs/ICS combos, antibiotics, and PDE-4 inhibitors
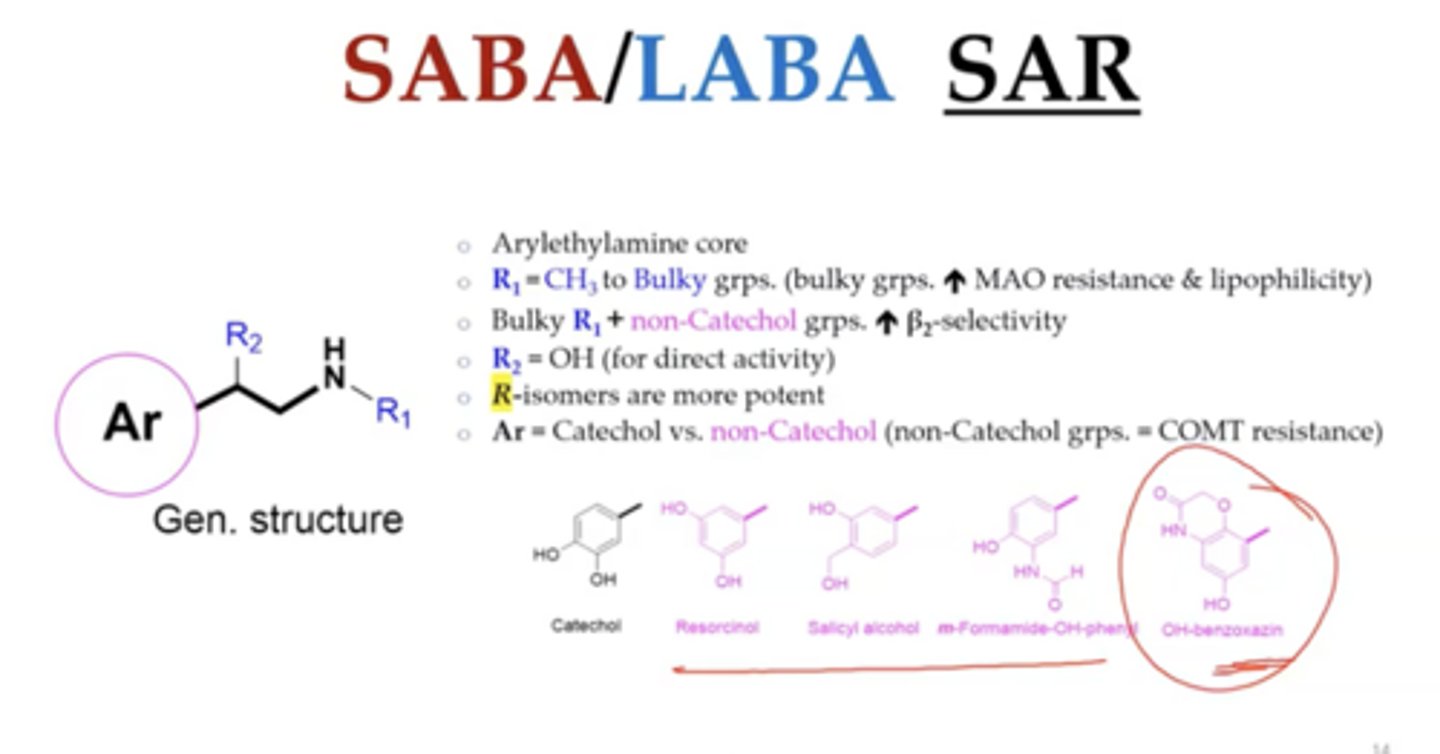
B2 selectivity is driven by what?
aryl and bulky R groups
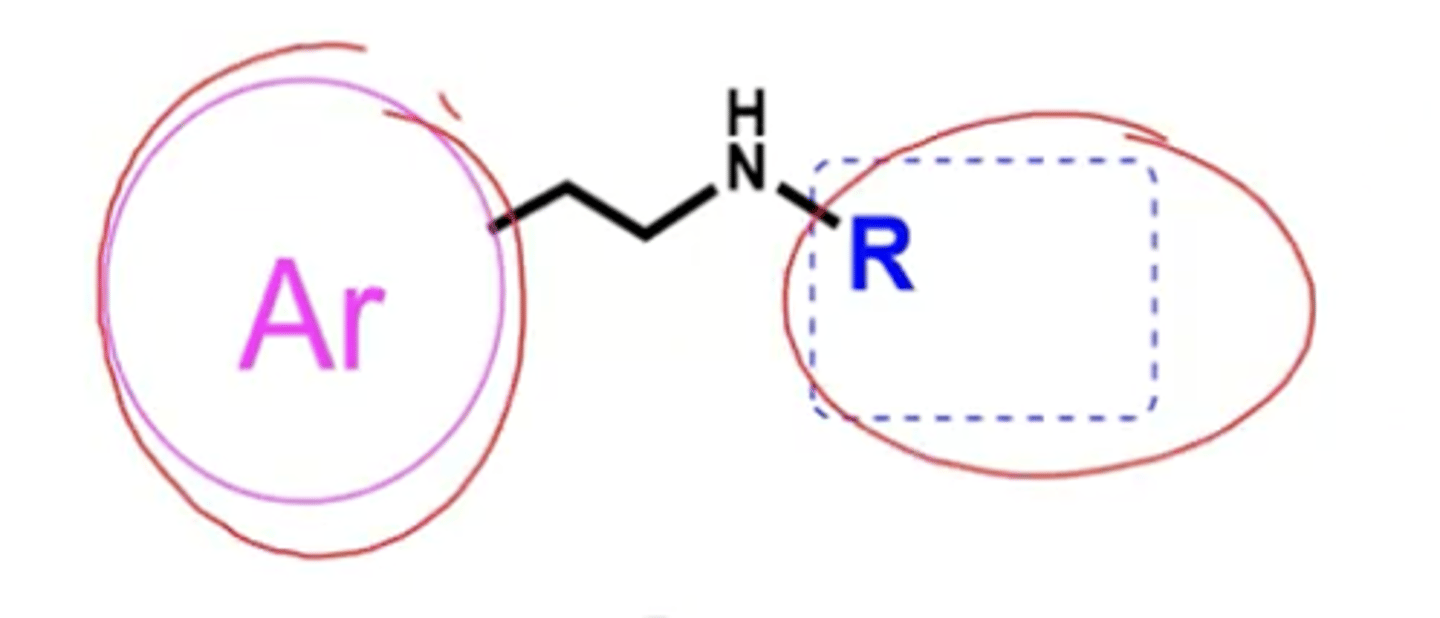
Lipophilicity is driven by what?
bulky R groups
Why is albuterol short acting?
direct conjugation metabolism by sulfotransferases (STs)
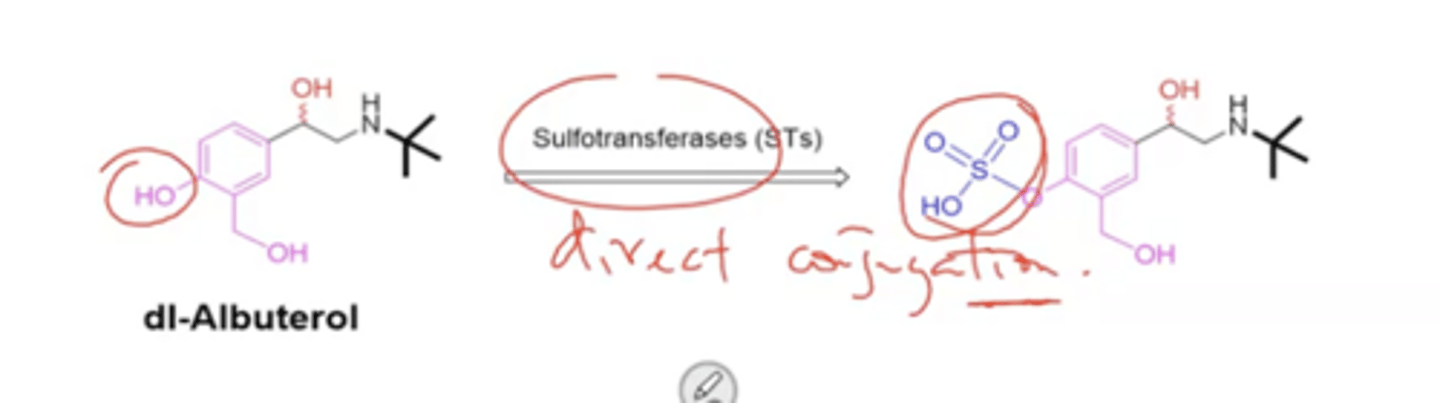
Which isomer of albuterol is metabolized faster?
R isomer is metabolized faster than S-isomer (so the S isomer lingers around longer than the R isomer)
S-isomer has what effects?
inflammatory
COMT =
catechol
Why are LABAs long acting?
non catechol aryl groups resist COMT
bulky N-R groups resist MAO
slower metabolism = longer duration of action
Formoterol is a ___ mixture
racemic
Arformoterol
R-R isomer and is 1000x more potent than S,S and 2 fold more potent than racemic mixture
What groups impart B2 selectivity in formoterol?
m-Formamide-OH-phenyl and Isopropyl-p-methoxy phenyl group
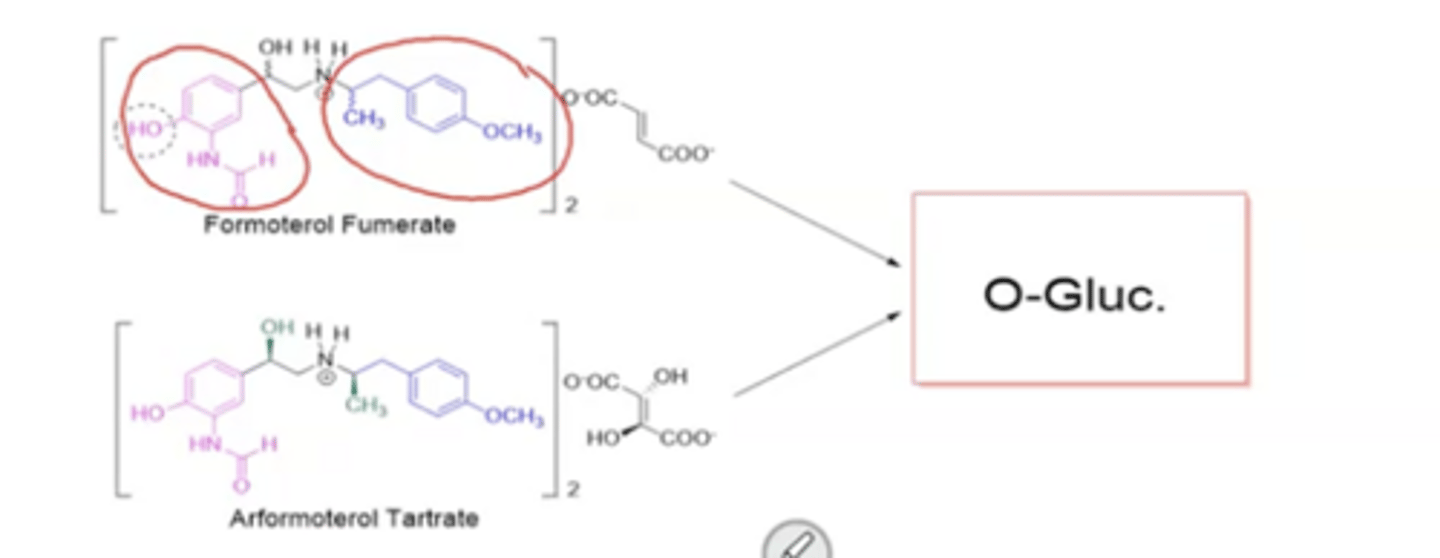
major formoterol metabolism
UGT, O-Glucoronidation
Salmeterol
Serevent Diskus
Athletes can abuse __
salmeterol
Vilanterol is a __
ante-drug --> when it becomes systemic it is deactivated
Olodaterol
Striverdi Respimat
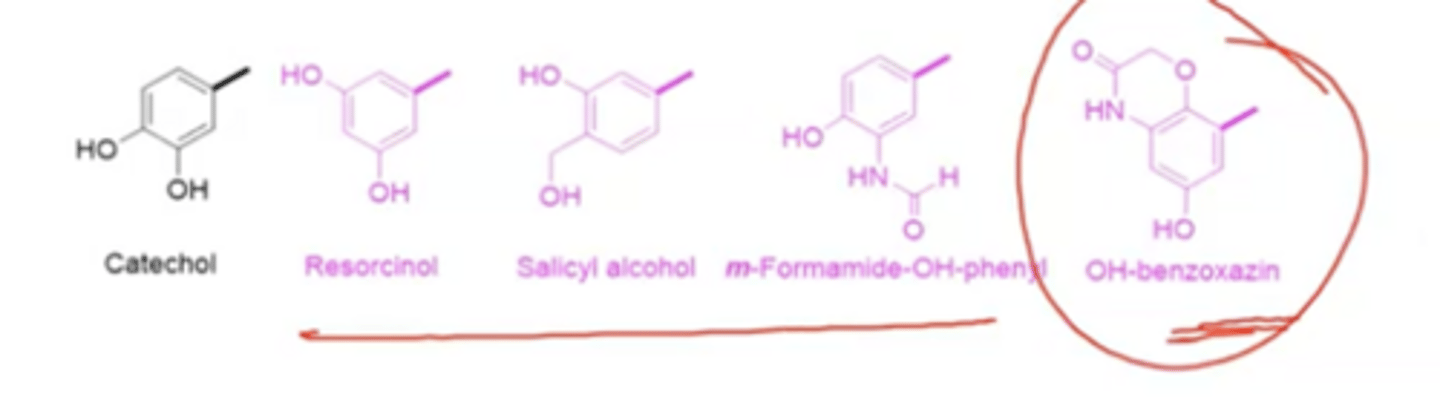
Olodaterol is a ___
hydroxybenzoxazine
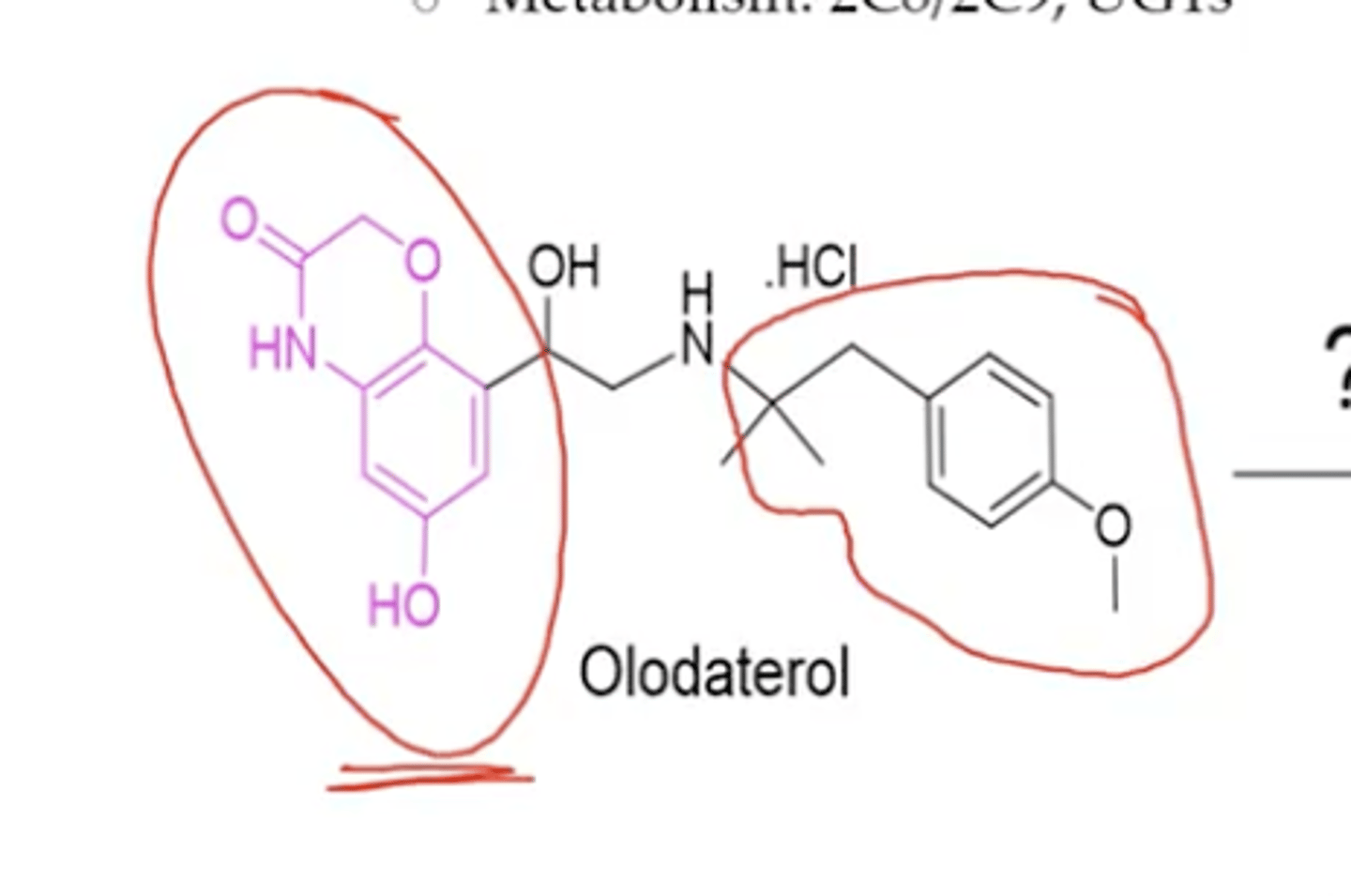
Olodaterol pharmacological category
Ultra long acting beta adrenergic
Why is olodaterol long acting
resistant to COMT and MAO
Accumulates in lung tissue due to lipophilicity
Olodaterol metabolism
2C8/2C9, UGTs
Catechol replacements for COPD
:)
SABA/LABA SAR summary
:)
Muscarinic antagonists are derived from what?
atropine and scopolamine (wears and epoxide hat)
What promotes local activity in anti muscarinics?
ionized quarternary amine or ionizable N
M3 antagonists block __
cholinergic bronchoconstriction
Ipratropium (Atrovent) can be classified as a ___
amino alcohol ester, SAMA
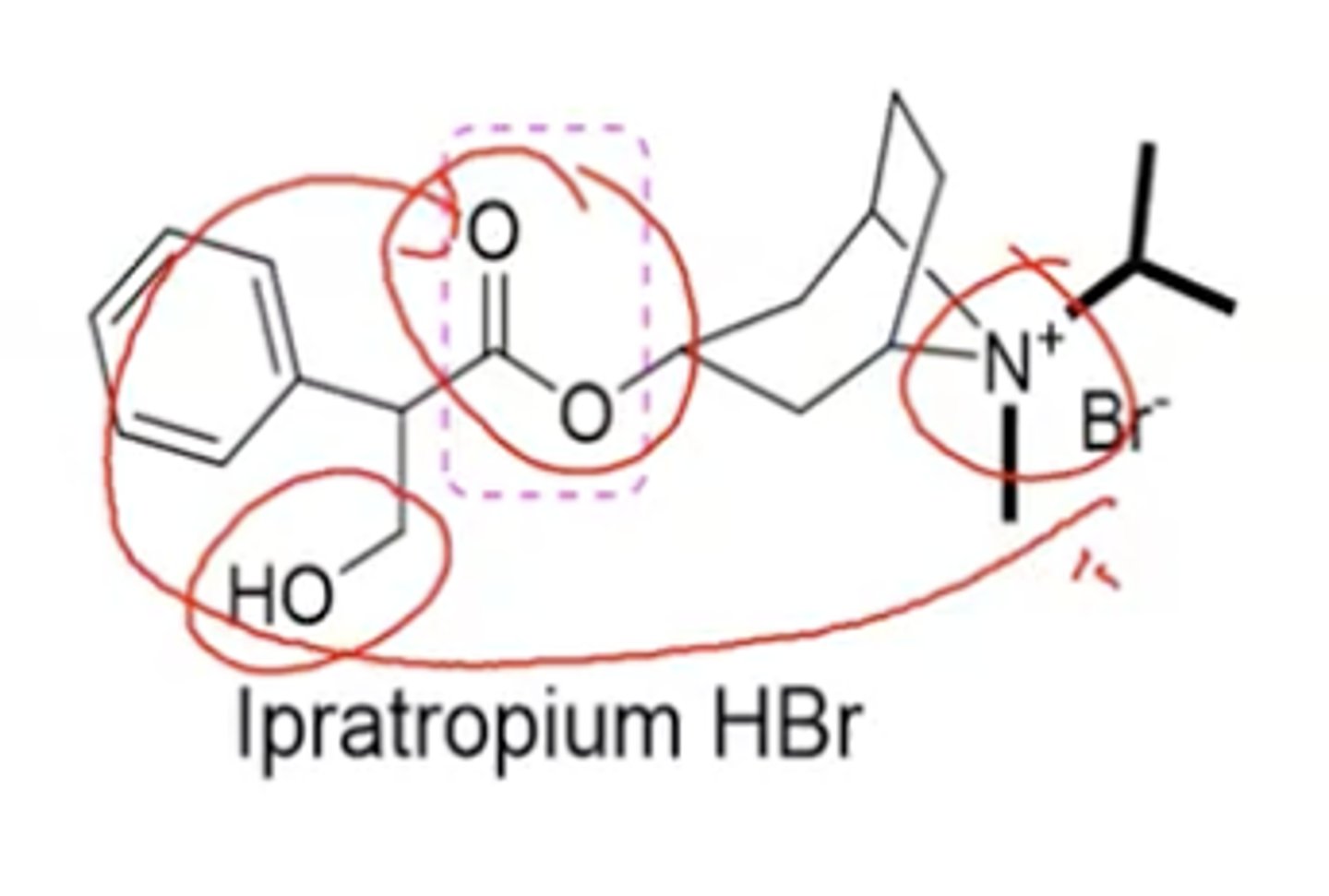
What aspect of metabolism will minimize anticholinergic effects?
esterase hydrolysis
Ipratropium + Albuterol
Combivent
Tiotropium (Spiriva) and Aclidinium (Tudorza) are both ___
LAMAs and amino alcohol esters