MS 1
1/61
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
62 Terms
Define a Electromyelogram (EMG) + purpose
Measure electrical charge associated with muscle contraction → Differentiate muscle vs neurological issues
Define Arthroscopy
Insertion of a lens/camera directly into the joint
Abnormal calcium, phosphate & parathyroid hormone labs meaning?
Metabolic changes, possibly secondary to renal disease or parathyroid hormone imbalance
What is Serum CK (creatine kinase)?
Protein that leaks out of damaged muscle cells into body fluids → telling of rhabdo/muscle injury
Healing process of fractures? (4 steps)
Hematoma forms (bleeding)
Inflammation (fibrin mesh + granulation tissue form)
Soft callus → hard callus
Bone remodeling
General healing periods for fractures?
Kids: ~1 month
Adults: 2+ months
Older adults: LONG time
Co-morbidities of impaired bone healing? (5)
Anemia
DM
Nutritional deficits
Glucocorticoids
Nicotine → vasoconstricts
Define osteomyelitis + relevance
Bone infection → common complication of fractures
Define Compartment Syndrome + signs?
Pressure builds (edema turns inward) → cuts off blood flow (compresses nerves + vessels)
Pain + swelling + numbness
Define Fat Emboli
Fatty marrow escapes into vein → goes to lungs → obstruction, inflammation, and
respiratory distress
Define nonunion/malunion
Bone doesn’t heal properly
Define Osteoporosis
Decrease in bone mass and density
Loss of bone matrix and mineralization
2 Types of Osteoporosis?
Primary: postmenopausal, senile, or idiopathic
Secondary: develops as a result of another disorder, like Cushing syndrome
Pathophysiology of Osteoporosis? + Precursor?
Pathophysiology: reabsorption of bone by osteoclasts exceeds bone formation by osteoblasts → thin, fragile bones
○ osteopenia → precursor to full osteoporosis
Risk Factor Pattern for Osteoporosis? (10)
Aging
Female/postmenopausal
Low calcium/vit D
Sedentary
Smoking, caffeine
Steroids/Cushing’s
Key s/s of Osteoporosis? (3)
Back pain
Kyphosis (“hunchback”)
Spontaneous fractures (KEY)
Diagnostic for Osteoporosis?
DEXA scan
T-score:
Normal: ≥ -1
Osteopenia: -1 to -2.5
Osteoporosis: ≤ -2.5
General Treatment for Osteoporosis? (3)
Calcium & Vitamin D + protein
Weight-bearing exercise
Surgery
Prototype Osteoporosis Meds? (2)
Alendronate (Bisphosphonate) & Raloxifene (SERM)
Alendronate MOA?
Inhibits osteoclast-mediated bone reabsorption
Alendronate SE/AE? (3)
SE → dyspepsia
AE → HF, esophageal damage
Nursing considerations for Alendronate? (3)
Must be taken with 8oz water 30 min before other food/fluids
Must remain upright for 30 minutes after taking (esophageal damage)
Also comes with vitamin D for enhanced absorption of calcium
Raloxifene MOA?
Binds to specific estrogen receptors to reduce bone resorption and increase bone mineral density
Raloxifene SE/AE? (3)
SE → Hot flashes, leg cramps
AE → Increased risk for DVT, PE, & CVA (CLOTS!)
Nursing considerations for Raloxifene? (2)
Take with calcium and vitamin D to prevent/treat hypocalcemia while on it
Avoid prolonged periods of sitting, especially first 4 months of therapy (clot risk!)
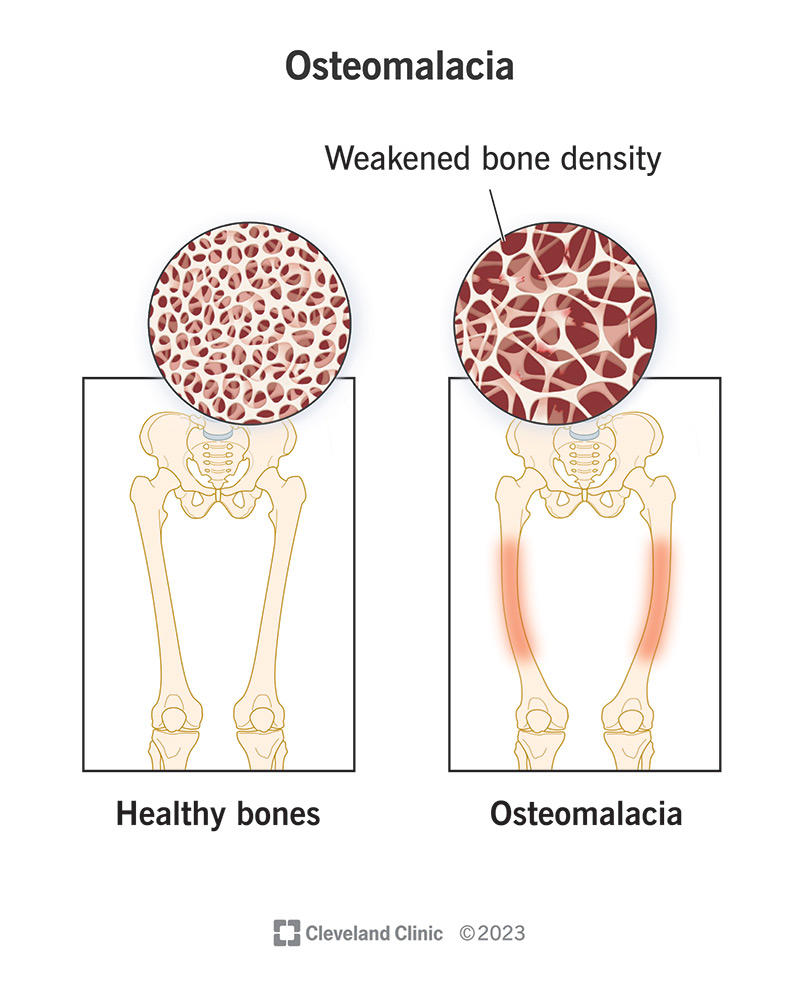
Pathophysiology of Rickets & Osteomalacia?
Deficit of vitamin D and phosphates required for absorption of calcium → lack of
calcification of cartilage formation → weak bones, deformities, compression fractures
Rickets vs. Osteomalacia?
Children → Rickets (“bow legs”)
Adults → Osteomalacia
Key causes of Rickets & Osteomalacia? (3)
Poor diet
No sunlight (lack vitamin D)
Malabsorption
Define Osteosarcoma
Neoplasm in the metaphysis of the femur, tibia, fibula in children and young adults; primarily males
Define Ewing sarcoma
Neoplasm in diaphysis of long bones, commonly in adolescence
Define Muscular Dystrophy (MD)
Group of inherited disorders characterized by degeneration of skeletal muscle
Pathophysiology of MD?
Metabolic deficit of dystrophin (muscle cell membrane protein) → degeneration and necrosis of
the cell → skeletal muscle fibers replaced with fat/fibrous connective tissue & hypertrophic muscle appearance → gradual loss of muscle function
Key s/s of MD? (3)
Weakness (starts in legs)
Gower’s maneuver
Waddling gait
Key MD diagnostic?
Elevated CK levels
Typical outcome of MD?
No cure → focus on PT/OT
Death (usually by age 20) often from respiratory/cardiac failure (possible ventilation to prolong life)
Define Osteoarthritis (OA)
“Wear and tear” damage to weight-bearing joints → can be unilateral
Pathophysiology of Osteoarthritis (OA)?
Weight-bearing joint articular cartilage is damaged from excessive mechanical stress
Key s/s of OA?
Pain with movement
Crepitus
Heberden’s nodes (DIP joints of hands)
Treatment for OA?
Minimize stress on joint, ambulatory aids, PT, OT
Pain relief; 1st line medication → Acetaminophen
Celecoxib (NSAID)
Celecoxib uses? (3)
OA, rheumatoid arthritis, & ankylosing spondylitis
Celecoxib MOA?
Inhibits COX-2, which normally promotes prostaglandin synthesis and inflammatory response (does not inhibit COX-1)
Key Celecoxib AE? (3)
Tinnitus, bronchospasm, blood dyscrasias
Nursing consideration for Celecoxib? (1)
Less risk for peptic ulcer/GI bleed than traditional NSAIDs
Define Rheumatoid Arthritis (RA)
Autoimmune disorder → chronic systemic inflammatory disease with exacerbations and remissions; with each exacerbation more damage & additional joints involved
RA genetic factor?
Rheumatoid factor (RF), antibody against immunoglobulin G, is present in the blood of most persons with RA
Pathophysiology of initial onset RA?
Abnormal immune response → Acute inflammation of synovial membrane → Formation of exudate → Typical red, swollen, painful joint (synovitis) → Appears to recover
Pathophysiology of subsequent exacerbations of RA?
Synovitis (inflammation recurs) → Granulation tissue spreads over joint causing “pannus” formation → Pannus releases enzymes that erodes cartilage → Fibrosis of joint space, limited
movement → Ankylosis (joint fixation and deformity)
Key s/s of RA? (4)
Morning stiffness (improves with movement)
Swollen, warm joints
Fatigue, fever (systemic)
Ulnar deviation
Medications for RA? (4)
Focus = pain control
High-doses of NSAIDs/aspirin
Celecoxib
Corticosteroids (if severe)
Disease-modifying antirheumatic agents (DMARDs)
Immunosuppressant → methotrexate
Immunomodulator → etanercept
Antimalarials → hydrochloroquine
Methotrexate MOA?
For RA exact MOA unknown but decreases joint inflammation and damage
Key SE/AE of Methotrexate? (4)
SE → photosensitivity
AE → hepatotoxicity, bone marrow suppression → increased infection risk, gastric ulcers
Nursing considerations for Methotrexate? (5)
Class 1 hazardous drug → double chemo gloves
Teratogenic
Avoid aspirin, NSAIDs, PPIs, and alcohol
Monitor labs (bone marrow suppression, liver function, GI bleeding)
Take folic acid to decrease toxicity risk
Etanercept MOA?
TNFI → inactivates tumor necrosis factor (TNF) which prevents it from attaching to cells synovial fluid in joints → blocked inflammatory reaction
Key SE/AE of Etanercept? (2)
SE → Increased infection risk (blocks inflammation)
AE → Reactivation of latent TB
Nursing considerations for Etanercept? (3)
Give with methotrexate for enhanced effect
Monitor for infection symptoms & CBC
Test for TB before starting and periodically
Define Gout (Gouty Arthritis)
Uric acid and urate crystal deposits in joints → acute inflammatory response; most commonly effects big toe
Most common underlying cause of Gout?
Inadequate renal excretion → hyperuricemia (uric acid is purine metabolism waste product the kidneys excrete)
Define a tophus
Large hard nodule of urate crystals in soft tissue or bone → local inflammation
Define Ankylosing Spondylitis
Chronic, progressive autoimmune inflammatory condition of sacroiliac (SI) joints, intervertebral spaces, & costovertebral joints
Pathophysiology of Ankylosing Spondylitis?
Vertebral joints (SI) of lower back become inflamed → calcification/fusion of joints → ankylosis → progression up spine → “poker back” → kyphosis
Key s/s of Ankylosing Spondylitis? (3)
Morning body stiffness relieved by walking, rigid spine, & systemic signs (fever/anorexia)
Treatment for Ankylosing Spondylitis?
Pain relief with anti-inflammatory meds & maintain mobility