N112 - Periop and Lab Values
1/57
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
58 Terms
What is blood composition?
Plasma (55%): Consists of water and proteins, such as albumin and clotting factors
RBCs (41%): Consists of red blood cells
WBCs or Buffy Coat (4%): Consists of WBCs and platelets
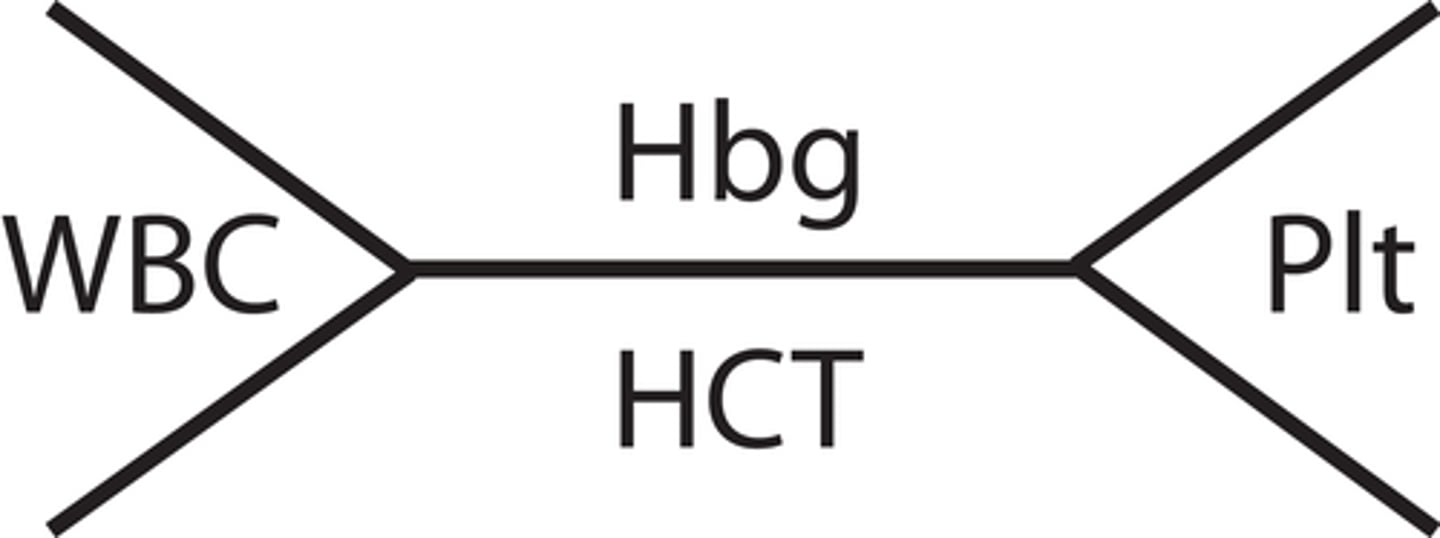
What does CBC consist of?
1) WBC count
2) WBC differential
3) Platelet count
4) Hemoglobin
5) Hematocrit
6) RBC indices
Take note of the CBC fishbone
White Blood Count
Normal range: 5,000 - 10,000
Critical values: <2,500 or >30,000
SIRS criteria: <4,000 and >12,000 since these are indicative of infection in particular.
Increased values can be due to:
1) Infection/inflammation
2) Trauma
3) Stress
4) Wounds and necrosis
5) Cancer, with leukemia causing the highest possible increase
Decreased values can be due to:
1) Overwhelming infection
2) Bone marrow suppression
3) Dietary insufficiency
4) Chemotherapy and cancer
What are expected assessment findings and associated risks with high WBC?
Assessment findings:
1) Enlarged lymph nodes
2) Fever and signs of infection
3) Malaise and weakness
Associated risks:
1) Organ dysfunction from leukemic infiltration
2) Complications including organ swelling, such as hepatomegaly and splenomegaly
What are expected assessment findings and associated risks with low WBC?
Assessment findings:
1) Enlarged lymph nodes
2) Fever and signs of infection
3) Malaise and weakness
Expected risks:
1) Increased risk of infection
2) Increased risk of sepsis if its due to an infection
Nursing interventions related to abnormal WBC count
1) Monitor for infection/inflammation and investigate causes
2) Administer antibiotics or anti-inflammatory as ordered
3) Implement infection controls
4) Consider neutropenic precautions for the patient if WBC low
5) Perform frequent CBC monitoring
6) Coordinate with IDT for potential transfusions/other treatments
WBC Differential
Absolutes are usually not used unless neutrophil count is very low due to cancer.
Normal Neutrophil Differential: 55-70%, with absolute within 2500-8000 cells/cubic mm
Normal Lymphocyte Differential: 20-40%, with absolute within 1000-4000 cells/cubic mm
Normal Monocyte Differential: 2-8%, with absolute within 100-700 cells/cubic mm
Normal Eosinophil Differential: 1-4%, with absolute within 50-500 cells/cubic mm
Normal Basophil Differential: 0.5-1%, with absolute within 25-100 cells/cubic mm
What causes changes in different components of WBC Differential?
Neutrophils: Elevated in BACTERIAL infection and trauma. Band differential is also elevated in infection. Low absolute neutrophil count is called NEUTROPENIA and it is indicative of very poor immune function.
Lymphocytes: Elevated in CHRONIC bacterial infections or ACUTE viral infections
Monocytes: Elevations may not necessarily indicate a change in condition since monocytes can live for a long time.
Eosinophils and basophils: Elevated in response to allergies
Platelet counts
Platelets, aka thrombocytes, are cell fragments that aggregate with clotting factor proteins to create clots/scabs. More = more clotting, less = less clotting.
Normal range: 150,000 - 400,000 cells/cubic mm
Critical values: <50,000 or >1,000,000 cells/cubic mm
Increased values (thrombocytosis) can be due to:
1) Infection/Inflammation
2) Certain Cancers
Decreased values (thrombocytopenia) can be due to:
1) Low production
2) All being used to form blood clots, such as during heavy bleeding
3) May result from heparin use
What are expected physical assessment findings for high platelet count? What risks are associated with it?
Assessment findings:
1) Decreased bleeding time
2) Signs of thrombosis
3) Thick blood
Associated risks:
1) Thrombosis and embolisms
2) Ischemia
What are expected physical assessment findings for low platelet count? What risks are associated with it?
Assessment findings:
1) Prolonged bleeding time
2) Increase incidence of bleeding
3) Easy bruising
Associated risks:
1) Spontaneous bleeding
2) Life threatening bleeding
Nursing interventions related to abnormal platelet count
Too low:
1) Monitor for signs of bleeding and implement bleeding precautions, including precautions to prevent skin breakdown
2) Administer platelet transfusions to correct low platelet count
Too high:
1) Monitor for signs of thrombosis
2) Encourage hydration and mobility to prevent blood stasis
3) Administer anticoagulants as prescribed
Hematocrit (HCT)
Hematocrit is the percentage of blood that is RBCs.
Normal values for males: 42-52%
Normal values for females: 37-47%
Critical values regardless of sex: <18-21% or >60%
High values may be due to:
1) Polycythemia, aka too much RBCs
2) Too little water in blood
Low values may be due to:
1) Anemia due to not enough erythropoietin, bone marrow is defective, or if patient is losing blood
2) Too much water in blood
Hemoglobin (HGB)
Hemoglobin is the O2 carrying protein in RBCs. Typically, Hgb should be 1/3 of HCT.
Normal ranges for males: 14-18 g/dL
Normal ranges for females: 12-16 g/dL
Critical values: <6-7 or >20 g/dL
High values may indicate:
1) Abnormal production of Hgb
2) Polycythemia (too much RBCs)
3) Too little water in blood
Low values may indicate:
1) Low levels of RBCs (anemia)
2) Thalassemia (Too little NORMAL Hgb being produced by the body)
3) Too much water in blood
What are expected physical assessment findings for high hemoglobin/hematocrit? What risks are associated with it?
Assessment findings:
1) Warm, flushed skin
2) Manifestations related to ischemia to vital organs
Associated risks:
1) Thrombosis
2) Increased blood viscosity and decreased tissue perfusion (ischemia)
What are expected physical assessment findings for low hemoglobin/hematocrit? What risks are associated with it?
Assessment findings:
1) Pale skin
2) Fatigue and weakness
3) Increased heart rate and shortness of breath
Associated risks:
1) Increased cardiac workload and thus increased risk of cardiac complications
2) Impaired oxygen delivery to tissues and end organ dysfunction
Nursing interventions related to abnormal hematocrit/hemoglobin count
Low:
1) Assess and monitor for signs of tissue hypoxia and fatigue
2) Administer supplements such as iron, erythropoietin, or folic acid as ordered
3) Prepare for and monitor blood transfusions as ordered
4) Monitor for signs of bleeding, which will make the problem worse.
High:
1) Monitor for signs of thrombosis or hyperviscosity syndrome
2) Encourage hydration and mobility to prevent blood thickening
3) Assist with therapeutic phlebotomy if ordered
4) Monitor for CV or neurological complications
What does high levels of reticulocytemia indicate?
Normal range: 0.5-2% of RBCs
High levels of reticulocytes (immature RBCs) in blood indicate that the body is so deficient of Hgb or RBCs that the bone marrow is desperate and pushing immature RBCs into the bloodstream.
Corresponds with
1) Critically low Hgb count
2) Critically low HCT
RBC Indices
This is a collection of tests that look at the size, variation, volume, and Hgb concentration of RBCs. They help determine the CAUSE of anemia or polycythemia.
Symptoms of anemia
1) Fatigue - Due to hypoxia, manifestation of end organ dysfunction.
2) Irregular heartbeats - Due to hypoxia, heart has to increase output to meet tissue O2 demands.
3) Chest pain - Due to hypoxia, blood may not get the O2 it needs (think angina)
4) Weakness - Due to hypoxia, manifestation of end organ dysfunction.
5) SOB - Due to hypoxia, the body increases respiratory effort and rate
6) Cold hands and feet - Due to hypoxia, blood is shunted away from extremities and towards vital organs
7) Pale or yellowish skin - Due to hypoxia, blood is shunted away from skin and towards vital organs.
8) Dizziness - Due to hypoxia, manifestation of end organ dysfunction.
9) Headache - Due to hypoxia, blood vessels in brain vasodilates in response and causes headache
What are the causes of anemia?
1) Decreased RBC production, which can be due to iron deficiency, B12 deficiency (less common), or folic acid deficiency (due to chemotherapy or alcoholism). Can also be due to decreased erythropoietin, which may occur if the body has decreased oxygen demand (such as during periods of immobility).
2) Blood loss, which can be chronic due to cancer, ulcers, or liver disease, or acute due to trauma, ruptured aneurysms, or GI bleed.
3) Increased RBC destruction, which can be due to sickle cell disease, certain medications, infection with hemolytic organisms, transfusion of incompatible blood, or trauma from procedures such as cardiopulmonary bypass.
What medication classes can affect CBC values?
1) Antibiotics - May cause bone marrow suppression, leading to decreased WBCs, RBCs, or platelets
2) Chemotherapy drugs - May cause bone marrow suppression, leading to decreased WBCs, RBCs, or platelets. Also tends to affect folate levels as well.
3) Anticoagulants - Can decrease platelet count and potentially increase bleeding risk
4) NSAIDs - May cause GI bleed, leading to anemia
5) Anticonvulsants - May cause bone marrow suppression or affect folate metabolism, impacting RBC production
6) Diuretics - Can elevate hematocrit due to diuresis (dehydration)
7) Antipsychotics (Clozapine) - Can suppress bone marrow, leading to decreased RBC, WBC, and platelet count
8) Antithyroid medications - Can suppress bone marrow, leading to decreased RBC, WBC, and platelet count
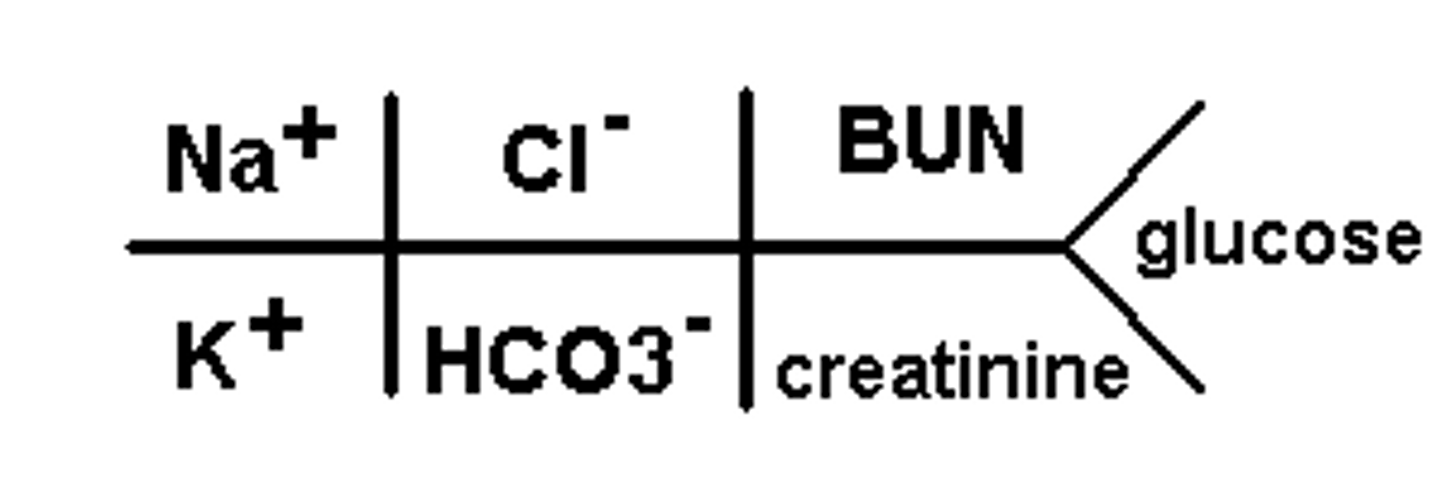
What does basic metabolic panel consist of?
Electrolytes:
1) Sodium
2) Potassium
3) Chloride
4) Total CO2 (serum bicarbonate)
Other:
1) Blood Urea Nitrogen (BUN)
2) Creatinine
3) Glucose
Take note of the BMP fishbone.
What do the electrolytes do? What are changes in body electrolytes related to?
The electrolytes are responsible for transmission of nervous signals and facilitate muscle contraction. They also contribute to serum osmolality (fluid balance between blood and cells). Changes in values are related to:
1) Dietary intake
2) Urinary excretion
3) Losses from vomiting/diarrhea/sweat
4) Dilution or concentration due to excess/deficient water in body
5) Shifts between cells and blood
6) Binding with H+ ions to alter acid/base balance of blood
Sodium
Sodium is the most prolific cation in the body. Its concentration is dependent on the amount of free water in blood. It also has a huge role in serum osmolality, meaning that water will be drawn out to blood when there is too much sodium. Conversely, water leaves blood and goes in cells when there is too little sodium.
Normal range: 136-145 mEq/L
Critical values: <120 or >160 mEq/L
Hypernatremia is related to:
1) Thirst and dehydration (most common cause)
2) Too much salt intake (not a common cause)
3) Increased thirst decreased urine output due to sodium increasing water demand and retention
Hyponatremia is related to:
1) Excessive fluid intake without replenishing electrolytes (most common cause)
2) Too little salt intake (extremely rare)
3) Sweating and polyuria to eliminate excess water
4) Swelling due to water being retained in cells
Swelling (too little sodium in blood) or crenation (too much sodium in blood) of brain cells can lead to headache, irritability, confusion, and progression to coma.
What are nursing interventions for hypernatremia/hyponatremia?
Hypernatremia:
1) Administer isotonic fluids if due to water deficit
2) Restrict dietary sodium (cardiac diet)
3) Dilute blood with sodium-free fluids and administer diuretics if due to actual sodium excess
4) Be wary of neurological complications such as ALOC or seizures due to crenation
Hyponatremia:
1) Replace sodium using saline if due to actually low sodium
2) Administer loop diuretics and implement fluid restriction if caused by excess fluid intake
3) Restrict free water
4) Be wary of neurologic complications such as ALOC or seizures due to cerebral edema
Potassium
Potassium is the most common intracellular electrolyte. It is important in the electrical function of cardiac cells and skeletal muscle cells.
Normal range: 3.5-5 mEq/L
Critical values: <2.5 or >6.5 mEq/L
Hypokalemia is related to:
1) Increase in duration of the hyperpolarized state, thus leading to difficulty in contracting or conducting electricity. May lead to cardiac arrhythmias.
2) Caused by poor dietary intake or loss of potassium in urine (especially with use of Lasix), vomiting, or diarrhea
Treat hypokalemia using IVPB or PO potassium supplements. Cardiac monitoring is also indicated.
Hyperkalemia is related to:
1) Causes irritability of cells and more frequent but less coordinated contractions (think arrhythmias).
2) Usually caused by inadequate urinary excretion or acute massive cell wall injuries (crush injury).
Hyperkalemia is objectively more dangerous in the acute setting.
What are nursing interventions for hyperkalemia/hypokalemia?
Hyperkalemia:
1) Administer IV calcium to counteract cardiotoxicity.
2) Administer glucose and insulin together to promote cellular K intake since insulin also causes potassium to shift inside cells.
3) Administer bicarbonate, which will cause in influx of sodium in the cells and enhance the activity of the Na+/K+ transporter and result in higher intracellular potassium.
3) Administer sodium polystyrene sulfonate to remove K from intestines before it can absorbed
4) Administer diuretics
5) Withhold intake of K rich foods and medications
Hypokalemia:
1) Administer KCl supplements and IV KCl as ordered
2) Encourage intake of K rich foods
Cardiac monitoring will be required for both conditions.
Chloride
This ion is not as important as sodium and potassium, but abnormalities can indicate acid/base abnormalities or hydration abnormalities.
Normal range: 98-106 mEq/L
Critical values: <80 or >115 mEq/L
By itself, not much information can be obtained. If chloride is severely out of range, there are probably other more important values that are out of range.
Serum Bicarbonate (CO2)
CO2 is stored mostly as bicarbonate in blood. Bicarbonate is a buffer that balances the pH in blood. The kidneys have a responsibility to retain or excrete bicarbonate as needed to balance pH, but it takes days to fully balance pH.
Normal range: 23-30 mEq/L
Critical values: <6 mEq/L
High levels of bicarbonate is usually due to chronic accumulation of acids in blood (usually due to respiratory acidosis). This is because the kidneys have had time to retain bicarbonate and work to normalize the pH of the blood.
Low levels of bicarbonate indicate ACUTE accumulation of acid in blood. This is because all the available bicarb has been converted to acid, and the kidneys haven't been able to alter its function to retain more bicarbonate. AKI, CKD, or renal failure can also cause low bicarbonate since the ability to excrete acids and retain bicarbonate is impaired.
Relation between respiratory system and bicarbonate in acidosis/alkalosis
CO2 + H2O <-> H2CO3 <-> H+ + HCO3-
Metabolic acidosis: Bicarbonate ions are LOW in metabolic acidosis because most of it has been converted to carbonic acid. Carbonic acid is then converted to CO2, which builds up in excess. This results in KUSSMAUL respirations.
Respiratory acidosis: Occurs when the body is hypoventilating due to sedation, obstruction of airways, or trauma. CO2 accumulates and is converted to carbonic acid, which is then converted into bicarbonate. Bicarbonate levels tend to not change acutely, but they will be high if the issue chronic.
Metabolic alkalosis: Bicarbonate ions are HIGH because carbonic acid is continuously dissociating to release hydrogen ions. This means CO2 is constantly being converted to carbonic acid as well. This results in HYPOVENTILATION.
Respiratory alkalosis: Occurs when the body is hyperventilating, usually due to anxiety or excitation. CO2 is lost excessively, and carbonic acid is converted to CO2. Bicarbonate levels tend to not change change acutely, but they will be LOW if the issue is chronic.
What are nursing interventions for high/low chloride and bicarbonate?
High/low chloride is usually not treated by itself since it is usually linked with issues with other electrolytes, and treating those other issues will usually resolve the chloride abnormality as well.
High/low bicarbonate is related to acidosis/alkalosis, so treating the underlying cause will also resolve the bicarbonate abnormality.
Blood Urea Nitrogen (BUN)
Blood Urea Nitrogen (BUN) is a byproduct of dietary protein breakdown and normal cellular protein breakdown. It is typically removed by the kidneys.
Normal range: 10-20 mg/dL
Critical value: >100 mg/dL
High levels can indicate dehydration, significant cellular breakdown after exercise (rhabdomyolysis), or diet with excessively high protein. More commonly, it is indicative of renal dysfunction and inability to secrete cellular waste products.
Creatinine
Creatinine is a byproduct of skeletal muscle breakdown. It is typically removed by kidneys.
Normal values for males: 0.6-1.2 mg/dL
Normal values for females: 0.5-1.1 mg/dL
Critical values regardless of sex: >4 mg/dL
High levels are related to:
1) Kidney dysfunction and inability to secrete waste products, which can be related to significant dehydration or AKI (may result from nephrotoxic medications).
2) Lower levels (rare) are possible in people with very low muscle mass.
Glucose
Normal range: 75-120 mg/dL
Critical values: <54 mg/dL or >400 mg/dL
Low levels cause:
1) AMS/ALOC
2) Weakness/fatigue
High levels have an unpredictable symptom pattern:
1) Abd pain and N/V
2) Increased thirst and urination
3) AMS/ALOC due to cerebral edema (DKA, which is associated with insulin being insufficient to meet cellular demand)
4) Cellular dehydration due to increased blood osmolality (HHNS, which is associated with insulin being sufficient to meet cellular demand but not enough to lower blood sugar)
Causes of increased glucose other than diabetes include stress, illness, and corticosteroid use.
What are nursing interventions to treat hypoglycemia and hyperglycemia?
Hypoglycemia: Administer glucose orally or via IV.
Hyperglycemia: Administer fluids to dilute the blood and insulin to promote cell absorption of glucose. May have to manage acidosis as well.
What medication classes can affect BMP values?
1) Diuretics - Can alter electrolyte balance, particularly K+, and affect BUN/creatinine.
2) Angiotensin Converting Enzyme (ACE) inhibitors and Angiotensin II blockers (ARBs) - Can increase K levels and affect BUN/creatinine.
4) K supplements - Obvious effect
5) Corticosteroids - May increase BGL
6) Lithium - Can be nephrotoxic, thus affecting BUN/creatinine. May also affect sodium levels.
7) Aminoglycosides - Can be nephrotoxic, thus affecting BUN/creatinine.
8) Laxatives (chronic use) - Can affect electrolyte balance and hydration status.
9) Beta-blockers - Can mask symptoms of hypoglycemia such as tachycardia, tremors, and perspiration.
10) NSAIDs - Can impair renal function, leading to altered BUN/creatinine. May also affect sodium and water retention.
11) Calcineurin inhibitors - Can be nephrotoxic, thus affecting BUN/creatinine.
Coagulation cascade
The coagulation cascade is a series of coagulation factor reactions that result in the formation of FIBRIN, which is a sticky substance that gathers platelets and RBCs to form clots/scabs.
What influences coagulation factor levels?
1) Coagulation factors are synthesized in the liver. Liver not working -> Not enough factors
2) Some coagulation factors need vitamin K for synthesis
3) Coagulation factors may be depleted if a large amount of clotting is happening, and they take a couple of days to regenerate (assuming normal liver function)
4) Anticoagulants may work on specific factors.
Prothrombin Time and International Normalized Ratio (INR)
PT is measured first, and then it is used to calculate INR. INR is the more standard measurement. For example, if PT is out of range but INR is normal, we just ignore the PT.
Normal PT Range: 11-12.5 seconds
Critical PT value: >20 seconds
Normal INR Range: 0.8-1.1
Critical INR value: >5.5
The primary medication that affects this assay is WARFARIN. Higher levels of INR = Warfarin is working better.
Warfarin's works by inhibiting vitamin K synthesis, and thus, INR will also be affected by vitamin K levels. Thus, patients who need constant INR monitoring also need to have stable vitamin K intake.
Activated Partial Thromboplastin Time (aPTT) and Partial Thromboplastin Time (PTT)
aPTT and PTT are tests for the same clotting factor, but they use different reagents and thus have different reference ranges.
Normal aPTT time: 30-40 seconds
Critical aPTT time: >70 seconds
Normal PTT time: 60-70 seconds
Critical PTT time: >100 seconds
The primary medication that affects these assays is INTRAVENOUS HEPARIN. In addition, the factor that is tested is synthesized using vitamin K, so values will be elevated with vitamin K deficiency. Thus, its also important for patients that need constant aPTT and PTT monitoring to have stable vitamin K intake.
Anti Xa aka Anti Factor Xa
This test directly measures the level of Anti-Xa drugs including heparin, LMWHs such as enoxaparin, and DOACs like apixaban. It is sometimes called a "heparin level." The number obtained from this assay is directly proportional to the amount of anti-Xa drug that is working.
Therapeutic ranges:
Heparin: 0.3-0.7 IU/mL
Lovenox: 0.5-1.2 IU/mL
Prophylactic Ranges:
Heparin: 0.1-0.4 IU/mL
Lovenox: 0.2-0.5 IU/mL
Lovenox in particular is metabolized by the kidneys (it is directly excreted without modification by the liver). Thus, this lab may also be ordered for patients on Lovenox with worsening renal values.
Blood Thinners and Anti-Platelet Drugs
Coumadin/Warfarin are vitamin K antagonists that affect PT/INR. INR is always monitored if a patient is taking this drug, and there are established INR goals.
IV Heparin will affect PTT/aPTT and Anti Xa. These labs are always monitored if patients are on this drug, and there are established goals.
Lovenox will affect Anti Xa and PTT, but these values are not monitored with Lovenox use.
Subcutaneous heparin will affect Anti Xa and slightly prolong PTT/aPTT, but these values are not monitored with Subcut heparin use.
DOACs like Eliquis and Xarelto affect anti Xa, but this value is not monitored with DOAC use.
Anti-Platelets such as Aspirin or Plavix make platelets less likely to adhere to each other, but they DO NOT change the number of platelets.
Heparin has the adverse drug reaction of THROMBOCYTOPENIA. The risk of bleeding with anticoagulant use AND thrombocytopenia is MUCH WORSE than the risk of one or the other.
What are nursing responsibilities in pre-operative care?
Supportive care:
1) Provide for the patient caregiver's physical and emotional support. Allow the caregiver to remain with the patient until the OR transfer to reduce anxiety.
2) Provide teaching about peri-operative procedures concerning the impending surgery and instruct on orders such as fluid/food restriction and smoking cessation prior to surgery. Educate on preparation, LOS, anesthesia, devices, and pain management.
3) Provide answers to questions from the patient, or refer to appropriate parties for specific questions about the surgery or anesthesia.
Teamwork:
1) Serve as a witness informed consent of the procedure. The person performing the procedure must obtain the consent.
2) Ensure pre-operative checklist and anesthesia assessment are all completed/available.
3) Assist with transfer to the surgical suite and provide hand-off to the intraoperative nurse.
Nursing Interventions:
1) Place patients NPO 8 hours prior to surgery with clear liquids allowed until 2 hours before surgery.
2) Administer any peri-operative care, such as antimicrobial bathing, or medications, such as prophylactic antibiotics, as ordered. Make sure to remove personal items like jewelry.
3) Perform a thorough basic and physical assessment in preparation for surgery. This includes VS.
4) Ask questions about patient's history and update/review patient's chart. Assess for complications that need to be discussed with the surgery team.
5) Review medications since some medications, such as anti-coagulants, may interact with anesthetics or contribute to post-operative complications.
6) Assess STOP-BANG since sleep apnea contributes to respiratory depression due to anesthesia.
7) Perform diagnostic studies such as ECG, imaging, and indicated lab tests
What is the role of the intraoperative nurse?
1) Assume care from the preoperative nurse and provide emotional support during transfer into the OR
2) Ensure pre-operative checklist is complete.
3) Assist patient to OR table from pre-op area. Secure patient onto OR table in proper position to minimize injury.
4) Apply VS monitoring devices, such as BP cuff, cardiac monitor, and SPO2.
5) Advocate for the patient's safety by monitoring for breaks in sterility and ensuring all patient care standards have been met.
6) Serve as a liaison between the pre-operative nurse, OR team, and post-operative nurse.
How are patients positioned in the OR? What are considerations?
Positioning may depend on the surgical procedure being done. Common positions are prone, supine, lithotomy, side-lying, sitting, Trendelenburg, or reverse Trendelenburg. Supportive devices may be used to help with positioning.
It is important to note that patients will not be able to report pain or injuries during surgery. Common injuries that may occur due to improper positioning include:
1) Damaged joints, strained muscles, and nerve damage
2) Disrupted blood flow to distal body parts
3) Pressure injuries
Why are patients in surgery more prone to hypothermia? What are risks? How do we prevent it?
Patients in the OR are more prone to hypothermia because anesthesia inhibits the body's ability to thermoregulate. The OR is also cold, and the patient's skin is exposed for operation.
Hypothermia during operation can lead to clotting disorders, electrolyte imbalances, and arrhythmias of the heart. Shivering also increases O2 demand by up to 400%. There is also increased risk of post-operative infection or other complications due to hypothermia.
We prevent hypothermia by covering body parts with warm blankets or forced air warming blankets when they are not being operated on.
How do we maintain sterility in the OR?
Extensive time/effort is put towards making a sterile environment. For example:
1) The patient's skin is cleansed the night before the procedure with antiseptic, and once more in the pre-operative area prior to transfer to the OR. The skin is cleansed from the incision site to distal areas (clean to dirty).
2) Sterile gloves (double gloving), gowns, hair coverings, and masks are required in the OR.
3) Avoiding air currents/excessive air movement in the OR decreases incidence of microbes traveling on airborne particles. This includes controlling traffic in/out of the OR and maintaining positive pressure in the OR.
4) Sterile hand asepsis is crucial and requires much more thorough cleaning.
5) Draping the patient and leaving only the surgical incision site exposed.
6) Only using sterile equipment and supplies, and keeping them above the level of the waist/operating table. If there is any doubt about contamination, assume the item is contaminated.
It is the responsibility of the OR nurse to watch for breaks in sterility and to report for these issues when seen.
What are miscellaneous patient safety concerns in the OR?
1) Risk of developing a DVT - address by applying TEDs or SCDs.
2) Retained surgical items - Gauze and equipment can be left in the patient. All gauze and equipment must be counted and accounted for prior to closing up.
3) Blood loss - Blood will inevitably be lost due to surgery, and the amount is monitored. High levels of blood loss may be treated by transfusion during operation, and cell-saver technology that salvages RBCs from lost blood and returns it to the patient's circulation may also be used.
4) Improper positioning -> Pressure injuries, soft tissue injuries, impaired CSM
Environmental: Cautery equipment present a fire risk, especially in the presence of O2 use. Such equipment must be grounded.
What is sign-in, time-out, and sign-out in the intraoperative setting?
These are all dedicated times for clear communication before the induction of anesthesia (sign-in), before skin incision (time-out), and before closing up (sign-out). Each time has associated tasks/discussion topics that must be completed/addressed.
Such practices improve patient safety and reduce risk of wrong-patient or wrong-site mistakes.
What does OR sign-in include?
1) Verifying patient, site, procedure, and consent
2) Ensuring the surgical site is marked
3) Ensuring anesthesia safety check is completed
4) Ensuring all VS monitoring equipment is applied and functioning
5) Addressing allergies, airway/aspiration risk, and bleeding risk.
What does OR time-out include?
1) Confirm all team members have introduced themselves by name and role
2) Verbally confirm patient, site, and procedure again
3) Review risk/[plan for critical or unexpected events that may occur such as oversedation, extended operative duration, excessive blood loss, and breaks in sterility.
3) Ensure antibiotic prophylaxis has been given within past 60 minutes
4) Ensure essential imaging is displayed
What does OR sign-out include?
Nurse verbally confirms
1) Name of procedure recorded
2) Instrument, sponge, and needle counts are correct
3) How specimen is labeled if a specimen was collected
4) Whether there are any equipment problems to be addressed
The surgeon, anesthesia professional, and nurse review the key concerns for recovery/management of the patient.
What is the purpose of prophylactic antibiotics prior to surgery?
Such antibiotics reduce the risk of postoperative surgical-site infection from intestinal bacteria.
What is true about hydration status in older adults?
Older adults are less adaptive in response to changes in fluid status, so they are prone to overhydration AND dehydration.
What is the role of the post-operative nurse?
1) Obtain handoff from PACU nurse
2) Manage post-operative complications (see other term)
3) Perform assessment of the wound and provide wound care, including dressing changes and device maintenance.
3a) Advise patient to keep surgical site clean/dry. They may take showers, but make sure to cover the surgical site and devices. They should not remove staples, scrub the incision, or submerge the incision.
4) Manage medications, IV solutions, and IV site. Prophylactic anticoagulants may be prescribed.
5) Perform a focused assessment including VS, pain, LOC, mental status, CSM, respiratory status, mobility, CV status, GI status,
6) Educate the patient on splinting (pain relief), changing positions frequently, use of incentive spirometer, use of compression devices, new medications, how to recognize signs of inflammation/infection and when to contact HCP.
6a) Educate the patient on the importance of rest, not lifting >10 lbs., adequate hydration, eating protein-rich foods to promote healing, the importance of mobility/activity, and follow-up appointments.
7) Ensure patient comfort, such as by providing warm blankets and managing pain.
8) I&O monitoring.
What are common post-operative complications?
1) Hypoxia, which is most commonly caused by atelectasis as a side effect of anesthesia. However, such atelectasis is reversible with incentive spirometry.
2) Nausea/Vomiting and lack of appetite due to anesthesia
3) Urinary retention, constipation, or ileus due to opioids and anesthesia
4) Infection of the wound site or internal organs; inflammation without infection
5) Hypotension due to fluid loss during surgery
6) Electrolyte imbalance due to fluid loss during surgery
7) Pain
8) Hemorrhage or wound dehiscence
9) Hypothermia due to effects of general anesthesia
10) Delirium or delayed emergence from anesthesia
Describe the process of consent for a medical procedure, including the nurse's responsibility in the process.
Informed consent involves
1) Adequate DISCLOSURE of diagnosis, nature/purpose of the procedure, risks/consequences of the procedure, probability of successful outcome, availability and benefits/risks of alternative treatments, and prognosis if treatment not given.
2) The patient's UNDERSTANDING of the disclosed information, meaning the patient must be of sound mind and able to make decisions for themself.
3) VOLUNTARY consent, meaning the patient cannot be persuaded by anyone to make the decision.
The person performing the procedure is ultimately responsible for obtaining the consent. Nursing responsibilities concerning consent include:
1) Witnessing consent and signature
2) Advocating for the patient and providing additional education to guide consent, involving the IDT as needed
Note that consent is not needed for emergency situations in which life saving interventions will be rendered. Attempts to reach next of kin will be made, but consent is not necessary to perform such interventions.