General Knowledge
1/59
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
60 Terms
Cushing's triad
Irregular respirations
Hypertension with widening pulse pressure
Bradycardia
AEIOUTIPS
Alcohol/Drugs, Acidosis, Arrhythmias
Epilepsy (seizures / post-ictal), Electrolytes
Encephalopathy (brain conditions)
Insulin (diabetic emergency)
Oxygen / Overdose
Underdose (withdrawal), Uremia
Trauma (head), Temperature, Thiamine (B1)
Infection (delirium),
Urinary Odors
Psychiatric, Pain, Poisoning
Stroke, Shock, Syncope, Space Occupying Lesion
7 Seizure types
Generalized Seizures (Affect both hemispheres of the brain)
Tonic-Clonic (Grand Mal) Seizure – Loss of consciousness, muscle rigidity (tonic phase), followed by rhythmic jerking movements (clonic phase).
Absence (Petit Mal) Seizure – Brief loss of awareness (staring spell), often seen in children, with no convulsions.
Myoclonic Seizure – Sudden, brief muscle jerks, usually affecting both sides of the body.
Tonic Seizure – Sudden muscle stiffness or rigidity, often causing falls.
Clonic Seizure – Repetitive jerking movements, usually rhythmic.
Atonic (Drop Attack) Seizure – Sudden loss of muscle tone, causing the person to collapse.
Status, seizure lasts >5 minutes or multiple seizures occur without full recovery between them.
Stroke Mimics
Hypoglycemia
Brain Tumor
Post-ictal state (following a seizure)
Migraine
Electrolyte imbalance
Overdose (toxicity-related neurological impairment)
Head Trauma
Transient Ischemic Attack (TIA)
Stroke Treatment
45 degrees (Positioning the patient with the head elevated)
Antiemetics (To manage nausea and vomiting)
IV fluids (For hydration and circulatory support)
O₂ if hypoxic (Supplemental oxygen if oxygen saturation is low)
NIHSS-8 (National Institutes of Health Stroke Scale score of 8)
Sepsis Signs & Risk factors
HR > 90 (Elevated heart rate)
RR > 22 (Increased respiratory rate)
Temperature > 38°C or < 36°C (Fever or hypothermia)
BGL > 7 (Elevated blood glucose, possible stress response)
SpO₂ < 94% (Low oxygen saturation)
Diabetes (Risk factor for sepsis)
Steroids (Immunosuppression can increase risk)
Chemotherapy (Weakened immune response)
Decreased urination (Possible sign of organ dysfunction)
Syncope (3 classes) + common causes
Orthostatic (Ortho) – Blood pressure drops when standing due to inadequate automimic compensation.
hypovolemia
medications (hypertensives, diuretics)
Autonomic dysfunction (can stem from underlying conditions like diabetes, Parkinson's, infections)
Prolonged bed rest
Neural
vasovagal (stress, pain, fear, sees blood)
situational (defecation, coughing, vomiting, straining)
Carotid sinus hypersensitivity (shaving, turning head, tight collar)
Cardiac
arrythmias
structural heart disease
Ischemia/ACS
Anaphylaxis process
Exposure to Allergen → The immune system mistakenly identifies a harmless substance (e.g., food, insect sting) as a threat and triggers an immune response.
B Cells Produce IgE Antibodies → B cells are immune cells that create IgE antibodies, which are specialized proteins designed to recognize and attach to specific allergens.
IgE Antibodies Bind to Mast Cells → Mast cells are immune cells that store inflammatory chemicals like histamine. IgE antibodies attach to mast cells, making them hypersensitive to the allergen.
Re-exposure to Allergen → When the allergen enters the body again, it binds to the IgE-coated mast cells, causing them to activate.
Mast Cell Degranulation → Activated mast cells release histamine, heparin, and other inflammatory chemicals into the bloodstream, triggering widespread immune effects.
Histamine Causes Blood Vessel Leakage → This leads to swelling (angioedema), redness, hives, and a sudden drop in blood pressure (shock) due to fluid leaking from blood vessels.
Bronchoconstriction & Mucus Production → Airways tighten, and excessive mucus is produced, causing wheezing, difficulty breathing, and potential airway obstruction.
Eosinophils Worsen Inflammation → These white blood cells leave the bloodstream and move to the reaction site, damaging tissues and increasing inflammation, making symptoms worse.
COPD Signs and Symptoms
Chronic Obstructive Pulmonary Disease (COPD) ✅ Signs and Symptoms:
Pursed lips breathing (self-PEEP)
Tripod position
Responds to supplemental oxygen
History of COPD or chronic lung disease
Use of CPAP
Use of accessory respiratory muscles
Chronic smoker
Barrel chest (especially in emphysema)
Yellow or green sputum
Peripheral oedema / "blue bloater" (chronic bronchitis)
Thin, wiry frame / "pink puffer" (emphysema)
📈 Common ECG Changes in COPD:
Right Axis Deviation (RAD)
P pulmonale (peaked P waves in lead II from right atrial enlargement)
Right Ventricular Hypertrophy (RVH)
Poor R wave progression (V1–V6)
Low voltage QRS (especially in limb leads due to hyperinflation)
Multifocal atrial tachycardia (MAT) in severe cases
APO Signs and Symptoms
Acute Pulmonary Oedema (APO) ✅ Signs and Symptoms:
Sudden onset of dyspnoea (especially at night)
Orthopnoea (SOB worse when lying flat)
Feeling of suffocation
Severe hypoxia that may not improve with oxygen
Cyanosis (late sign)
Tachycardia
Hypertension early, hypotension late
Crackles on auscultation (usually bilateral)
Pink frothy sputum
Commonly on diuretics
📈 Common ECG Changes in APO:
Left Ventricular Hypertrophy (LVH)
Left Bundle Branch Block (LBBB)
Left Atrial Enlargement (LAE) — broad, notched P waves (P mitrale)
Atrial Fibrillation (AF) — common in CHF-related APO
ST segment depression or T wave inversion in lateral leads if ischemia triggered
Signs of recent or ongoing MI if cardiac cause
what are ACE inhibitors + examples
Suffix: -pril (e.g., enalapril, ramipril, perindopril)
Blocks ACE with creates Angiotensin II with is vasodilator
Lowers BP by vasodilation (↓ afterload)
Protects the kidneys by lowering high blood pressure and reducing pressure within the kidney's tiny filters
Can cause hypotension, Syncope hyperkalaemia, dry cough, or angioedema
They slow kidney disease but can cause kidney impairment & AKI
Used in heart failure and post-MI patients
Cushings/TBI/ICP
Key Clinical Signs:
Wide pulse pressure
Initial hypertension, progressing to bradycardia and irregular respirations as coning (brain herniation) develops
Late-stage hypertension due to brainstem compression
Bradycardia and irregular breathing reflect brainstem dysfunction
ECG Changes Associated with Raised ICP:
Global ST-segment changes
T wave inversions
Prolonged QT interval
ARBs (Angiotensin II Receptor Blockers)
Suffix: -sartan (e.g., losartan, candesartan, irbesartan)
↓ BP via vasodilation,
no cough or angioedema (unlike ACE inhibitor)
Can cause hypotension, hyperkalaemia, renal effects
May be used if ACE inhibitors not tolerated
Beta Blockers
Suffix: -olol (e.g., metoprolol, atenolol, propranolol)
blocks adrenalin & noradrenaline from binding to β-receptors
slows heart rate, reduces force of contraction, relaxes blood vessels
↓ HR, BP, and myocardial oxygen demand
May blunt tachycardia in shock/sepsis
Watch for bradycardia, hypotension, bronchospasm (esp. in asthmatics)
Common in hypertension, post-MI, arrhythmias
makes Anaphylaxis refectory to Adrenaline
Glucagon needed in anaphylaxis with B-Blocker
Alpha & Beta receptors
Alpha-1: (vessel dilation)
Found in most sympathetic organs; causes smooth muscle contraction (e.g., blood vessel constriction, pupil dilation).
Alpha-2:
Located on nerve terminals; inhibits further release of norepinephrine and insulin.
Beta-1: (increases heart rate)
Primarily in the heart and kidneys; increases heart rate, force of contraction, and renin release.
Beta-2: (bronchodilation)
In lungs, blood vessels, and smooth muscles; causes dilation (e.g., bronchioles, arteries to skeletal muscle) and relaxation.
Beta-3:
In fat tissue; stimulates fat breakdown (lipolysis).
Calcium Channel Blockers
Suffix: dipine
Dihydropyridines: -dipine (e.g., amlodipine, nifedipine) ↓ BP (vasodilation) Minal effect on HR
Non-dihydropyridines: verapamil, diltiazem (no consistent suffix) strong cardiac effects, ↓ HR and contractility
Verapamil & Diltiazem particularly toxic, overdose can cause bradycardia and cardiogenic shock
Watch for hypotension, bradycardia, peripheral oedema, heart block
Used in **hypertension, angina, arrhythmias (especially SVT AF and Atrial flutter (Non-dihydropyridines))
Calcium Gluconate for verapamil or diltiazem overdose
CCB overdose can cause Bradycardia, Heart block, Hypotension, cardiogenic shock, seizures, coma, hyperglycemia, metabolic acidosis.
Consider adrenaline
Consider atropine
Consider pacing
Refractory anaphylaxis (3x IM adrenaline) with persistent wheeze.
What medications will you give?
Hydrocortisone
Adult - (doubel dose 200mg)
Paed - 4mg/kg (max 100mg)
Salbutamol
Adult - 5mg Neb (no max dose)
Paed - (1-5 years) 2.5mg (no max dose).
>6 years = Adult For salbutamol
Refractory anaphylaxis (3x IM adrenaline) with persistent hypotension
what medications will you give?
Glucagon1mg IM/IV
Adult - 1mg single dose
Pead >25kg 1mg
Paed <25kg 0.5mg
Normal Saline
Adult- (titrate as needed)
Paed - 10-20ml/kg (Max 60ml/kg)
Refractory anaphylaxis with stridor
Adrenaline Neb 5mg (5 vials)
Medications Causes of long QT
Medication causes
Common drugs that prolong QT:
Antiarrhythmics
Amiodarone
Sotalol
Procainamide
Flecainide
Psychotropics
SSRIs (citalopram, escitalopram)
Antipsychotics (haloperidol, droperidol, quetiapine, risperidone)
Antibiotics
Macrolides (azithro, erythro)
Fluoroquinolones (ciprofloxacin, moxifloxacin)
Antiemetics
Ondansetron
Domperidone
Others
Methadone
Lithium
Hydroxychloroquine
Some antihistamines (older ones)
Electrolytes & Metabolic/physiological causes of long QT
Electrolyte causes
Anything that reduces myocardial stability:
Hypokalaemia
Hypomagnesaemia
Hypocalcaemia
Metabolic/physiological causes
Bradycardia
Hypothermia
Myocardial ischaemia
Raised ICP
Endocrine disorders (e.g., hypothyroidism)
Anorexia/ prolonged malnutrition
Long QT management
2 lead look for Q-Tc >500ms
Look for triggers & reversible causes:
-Medications known to prolong QT
-History of anorexia/malnutrition, electrolyte disturbances (hypokalaemia, hypomagnesaemia, hypocalcaemia)
-Bradycardia (pause‐dependent rhythms)
-Recent re-feeding or metabolic disturbance
Patient at high risk of TdP (no amiodarone!)
TdP = Magnesium Sulfate (consult)
Hospital will treat with Magnesium Sulfate
Hs & Ts (Hs Causes, Signs and Treatment)
Hypoxia = choking, drowning, overdose CPR, ventilations, O2
Hypovolemia = bleeding, trauma, vomiting/diarrhoea, dehydration, shock, flat neck veins, Saline
H+ Acidosis = DKA, Sepsis, Pt may have been hyperventilating (Hx Kussmaul resps) QRS wide, arrest will likely be PEA > Asystole ETCO2 will likely be low <10mmHg CPR, ventilations, Sodium bicarbonate, saline, calcium gluconate
Hyper/Hypokalemia
Hyperkalemia
Hx renal disease, missed dialysis, Crush Syndrome/Rabo (red urine/ strenuous exercise/ long lies),
Overdose (∧Hx) CKD, renal impairment., dehydration, sepsis, dose escalation, multi therapies,
ACE inhibitors, & ARBs, (pril, sartan)
K+ sparing diuretics, Spironolactone (offender), Amiloride, Eplerenone
NSAID
Trimethoprim-sulfamethoxazole (TMP/SMX, Bactrim and Septra) combination antibiotic for bacterial, fungal, and protozoal infections.
Heparin (∧H x) diabetic
Flattened P waves > Peaked T waves > wide QRS > sinusoidal waves.
Calcium gluconate, salbutamol 20mg neb adult, 5mg child, sodium bicarbonate.
Hypokalemia
Hx of diuretic use(loop/thiazide), vomiting, diarrhoea, muscle cramps, weakness, seizure, poor intake, magnesium deficiency.
Overdose
β2-Agonists (bronchodilators)
insulin
palpitations prior to arrest
Potassium chloride IV
magnesium sulfide if TDP or prolonged QT
Flatted T waves, ST depression, prominent U waves, prolonged QT, PVC, TdP risk
K+ replacement and Mg+ if Mg+ is low (K+ won’t stay if Mg+ is out)
Hypoglycemia
150 mL of 10% (15 g of glucose), paediatric 0.25 g/kg (2.5 mL/kg) of 10%
Hypothermia (not dead till your warm and dead)
active rewarming during CPR is critical, 3 shocks then wait till >30°, no adrenaline, amiodarone till >30°, remove wet clothing, warm torso, insulate from ground, heat packs groin, neck, axillae.
Gentle handling movement can cause VF/VT,
Hs & Ts (Ts Causes, Signs and Treatment)
Tension Pneumothorax
Trauma, absent breath sounds on one side, distended neck veins, difficult ventilation, tracheal deviation, subcutaneous emphysema, chest pain sudden and pleuritic, increased work of breathing
Decompress chest, high flow O2
Tamponade (Cardiac)
Penetrating chest trauma, JVD, hypotension unresponsive to fluids, low voltage alternating QRS, pulsus, paradoxus (>10mmhg fall in systolic during inspiration) arrect likely PEA
Rapid transport, continue CPR
Toxins (Overdose/Poisoning) examples, suffixes
Drug paraphernalia, medication packets, pinpoint or dilated pupils, known history, ventilate, consider naloxone early
Poor ventilation, cherry red skin engines running, could indicate CO
Opioids, bradycardia, Pinpoint pupils, Naloxone, Vent, one, ine
Benzos, Vent, aspiration risk from sedation, pam, lam
TCAs, wide QRS, long Q-T Sodium bicarbonate, triptyline, paramine
Paracetamol, N-acetylcysteine in hospital
β-blockers, bradycardia, Glucagon IV, olol
Ca+ channel blockers, +ACE or β-blockers = high risk, bradycardic, Calcium gluconate, adrenaline, atropine, pacing, amil, tiaz, zem, Verapamil & Diltiazem(worst)
SSRI, antipsychotics, methadone, Long Q-T, MgSO₂
Thrombosis – Cardiac (MI)
History of chest pain, known cardiac disease, ECG pre-arrest (if available)
pre-alert hospital, pPCI referral OR thrombolysis
S-T elevation in 2 continual leads (.2mm limb, >1mm chest), QRS<0.12ms,
Thrombolysis
Tenecteplase IV,50mg in 10ml saline,1ml solution per 10kg, max 50mg
Enoxaparin IV 30mg
Clopidogrel Oral 300mg (4 tablets)
Enoxaparin sub-cut 1mg/kg, max 100mg, after 15 min
pPCI
Heparin IV,5000 IU single dose
Ticagrelor IV 30mg OR Clopidogrel Oral 600mg (8 tablets)
Thrombosis – Pulmonary (PE)
Hx dyspnea beforehand, pleuritic chest pain, swollen leg, long immobilisation (e.g., post-op, long haul flight) tachy & hypotensive.
Hypoxic and refectory to O2,
Right heart strain, RBBB, S1Q1T3, poor R>S progression, Right axis (I=neg, aVF=pos)
Supportive care only prehospital – good CPR, consider PE in handover
Risk factors. (DVT), Recent surgery (especially pelvic, abdominal, or orthopaedic), Cancer (especially metastatic or on chemotherapy), Trauma or fractures (especially to lower limbs or pelvis), Prolonged immobility (e.g. bed rest, long travel, hospitalisation), pregnancy/post-partum, hormone therapy.
O2,
cautions fluids (to support RV preload) too much fluid > RV dilation > septal shift > reduced LV preload, targes MAP 65 or sys 90.
noradrenaline to main same BP targets
tPA tissue plasminogen activator, (PE is fibrin rich clot, instead of platelet rich, tPA is used for fibrin rich clots)
tPA, 50mg IV during CPR, repeat @ 15 min, continue CPR for 90 min.
Trauma
Blunt or penetrating injury, visible wounds, obvious signs of major trauma
Control bleeding, decompress chest if indicated, rapid extrication and transport, keep warm, consider pelvic binder if significant mechanism. Traction long bones, pack junctional bleeds, tourniquets, proactive warming.
normal Q-Tc
Men <440 (Borderline441-460) (prolonged >460) (TdP risk >500)
Women <460 (Borderline461-480) (prolonged >480) (TdP risk >500)
Pathological Q waves
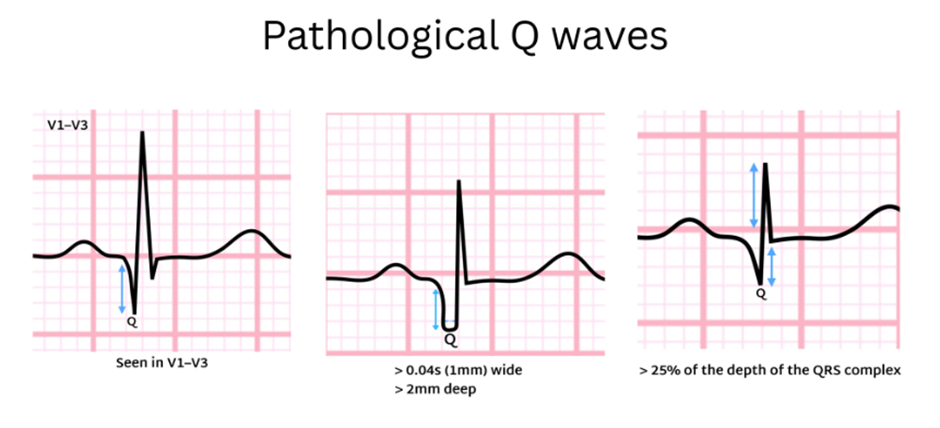
A Q wave is pathological if any of the following apply in ≥2 contiguous leads (same anatomical territory):
1. Duration
≥ 0.04 seconds (≥ 40 ms)
(one small ECG box wide)
2. Depth
≥ 2 mm deep, or
≥ 25% of the height of the following R wave
3. Lead-specific rules
Any Q wave in V1–V3 is pathological
(Q waves are normally absent here)
📍 Contiguous lead groupings
To count, Q waves must appear in anatomically related leads:
Inferior: II, III, aVF
Lateral: I, aVL, V5–V6
Anterior: V1–V4
Septal: V1–V2
Cardiac Tamponade S&S
· Hypotension
· Raised JVP (distended neck veins)
· Muffled heart sounds
· Narrow Pulse pressure
· Pulsus paradoxus (>10 mmHg SBP drop on inspiration, if measurable)
· Chest trauma + unexplained hypotension
· Low voltage QRS
· Electrical alternans (swinging heart)
DVT > PE factors and S&S
Venous stasis
· Immobility, long travel, paralysis, heart failure
Endothelial injury
· Trauma, surgery, IV lines, inflammation
Hypercoagulability
· Cancer, pregnancy/post-partum, OCP/HRT, thrombophilias, dehydration
PE S&S
· Sudden dyspnoea
· Pleuritic chest pain
· Unexplained tachycardia
· Syncope or near-syncope
· Hypoxia with clear lungs
1. Vertigo – sudden, severe, episodic (minutes–hours)
2. Fluctuating unilateral sensorineural hearing loss
3. Tinnitus ± aural fullness (pressure in the ear)
What’s likely condition
Ménière’s disease
excess inner-ear fluid → vestibular + cochlear dysfunction
History clues
Recurrent attacks with full recovery between episodes
Unilateral ear symptoms
Known diagnosis or previous similar episodes
Exam clues
Horizontal/rotatory nystagmus during attack
Normal limb power/sensation
No focal neurological deficit
🚨 Red flags — think NOT Ménière’s
If any of the following are present, prioritise stroke work-up:
First-ever vertigo in older patient
Persistent vertigo >24 h without improvement
Focal neuro signs (ataxia, dysarthria, weakness)
New severe headache
Vertical or direction-changing nystagmus
➡ Posterior circulation stroke can mimic Ménière’s.
These are the symptoms you see:
Confusion / altered mental state
Unsteady gait (ataxia), frequent falls
Nystagmus or other abnormal eye movements
May appear “intoxicated” without clear intoxication
This is the patient history:
Chronic alcohol use or poor nutrition
Prolonged vomiting / not eating
Homelessness, social neglect, eating disorder, or post-bariatric surgery
Recent illness with reduced intake
Likely condition:
Wernicke encephalopathy (thiamine deficiency) B1
These are the symptoms you see:
Episodic severe headaches
Profuse sweating
Tachycardia / palpitations
PVCs or other catecholamine-driven arrhythmias
May have anxiety, tremor, pallor, or hypertension during episodes
This is the patient history you may find:
Recurrent sudden attacks with complete recovery between episodes
Known or episodic hypertension
Attacks triggered by stress, exertion, surgery, or certain medications
Possible family history of endocrine tumours (MEN syndromes)
Likely condition:
Pheochromocytoma (catecholamine-secreting adrenal tumour)
4 types of Vasopressor
Levophed (Norepinephrine)
This medication gently tightens blood vessels and helps the heart pump more effectively. It raises blood pressure so blood can reach vital organs. It’s often the first choice for severe low blood pressure.
Vasopressin
Vasopressin helps the body hold onto fluid and narrows blood vessels. It works differently than other medications and is often used alongside Levophed to improve blood pressure.
Epinephrine (Adrenaline)
Epinephrine helps increase heart rate, blood pressure, and heart strength. It’s commonly used in emergencies like cardiac arrest, severe allergic reactions, or shock.
Phenylephrine
This medication raises blood pressure by tightening blood vessels without increasing heart rate as much. It’s helpful when blood pressure is low but heart rate is already high.
AAA
Pain
Signs
Exam Clues
Risk factors
Pain — what does the pain feel like?
Sudden onset abdominal, back, flank, or groin pain
Severe, deep, tearing, ripping, or “worst ever” pain
May start mild or intermittent before rapid deterioration
Can radiate to the back, flank, or legs
Signs — what might I observe?
Syncope or near-syncope
Hypotension (often late)
Tachycardia
Pale, clammy, diaphoretic
Shock or reduced level of consciousness
Exam clues — what might I find (or not find)?
Minimal abdominal tenderness
Soft abdomen despite severe pain
Pulsatile abdominal mass often absent
Rapid haemodynamic deterioration
Risk factors — who is high risk?
Age >65
Male
Smoking history
Known AAA
Hypertension
Atherosclerotic or vascular disease
Family history of AAA
Ectopic Pregnancy
Pain
Signs
Exam Clues
Risk factors
Pain — what does the pain feel like?
Lower abdominal or pelvic pain
Often unilateral initially
Sudden worsening if rupture occurs
Signs — what might I observe?
PV bleeding or spotting
Shoulder tip pain (referred diaphragmatic irritation)
Dizziness, syncope
Hypotension and shock if ruptured
Exam clues — what might I find (or not find)?
Lower abdominal tenderness
Signs of shock disproportionate to visible bleeding
Abdominal exam may appear relatively benign early
Risk factors — who is high risk?
Female of reproductive age
Missed or abnormal period
Previous ectopic pregnancy
IUD in situ
Fertility treatment or assisted reproduction
Mesenteric Ischaemia
Pain
Signs
Exam Clues
Risk factors
Pain — what does the pain feel like?
Sudden, severe, diffuse abdominal pain
Constant, non-colicky
Pain out of proportion to exam
Signs — what might I observe?
Nausea and vomiting
Diarrhoea (may become bloody late)
Tachycardia
Hypotension (late finding)
Exam clues — what might I find (or not find)?
Early: soft abdomen with minimal tenderness
Late: peritonism, guarding, rigidity
Shock once bowel necrosis occurs
Risk factors — who is high risk?
Atrial fibrillation
Recent myocardial infarction
Known atherosclerotic disease
Elderly patients
Embolic or thrombotic disease
Bowel Obstruction / Perforation
Pain
Signs
Exam Clues
Risk factors
Pain — what does the pain feel like?
Colicky, cramping pain initially
Becomes constant with strangulation or perforation
Signs — what might I observe?
Vomiting (bilious or faeculent)
Abdominal distension
Absolute constipation (no stool or flatus)
Fever (late), tachycardia
Exam clues — what might I find (or not find)?
Distended, tympanic abdomen
Localised or generalised tenderness
Guarding or rigidity if perforated
Peritonism indicates late disease
Risk factors — who is high risk?
Previous abdominal surgery (adhesions)
Hernias
Malignancy
Elderly
Chronic constipation
Acute Pancreatitis
Pain
Signs
Exam Clues
Risk factors
Pain — what does the pain feel like?
Severe epigastric pain
Radiates through to the back
Worse lying supine
Relieved by leaning forward
Signs — what might I observe?
Persistent nausea and vomiting
Tachycardia
Hypotension in severe cases
Low-grade fever
Exam clues — what might I find (or not find)?
Epigastric tenderness
Abdominal distension in severe pancreatitis
Signs of systemic inflammatory response if severe
Risk factors — who is high risk?
Heavy alcohol use
Gallstones
Recent binge drinking
Previous episodes of pancreatitis
Inferior Myocardial Infarction (abdominal pain mimic)
Pain
Signs
Exam Clues
Risk factors
Pain — what does the pain feel like?
Epigastric discomfort or indigestion-like pain
Pressure, burning, or vague ache
May radiate to chest, jaw, neck, or back
Signs — what might I observe?
Nausea and vomiting
Diaphoresis
Dyspnoea
Bradycardia or hypotension (inferior MI pattern)
Exam clues — what might I find (or not find)?
Normal abdominal exam
Unexplained abnormal vitals
ECG changes on 12-lead
Risk factors — who is high risk?
Older age
Diabetes
Known ischaemic heart disease
Hypertension
Smoking
Dyslipidaemia
PE ECG
S1Q3T3 Pattern: This classic PE sign is where you see an S wave in lead I, a Q wave in lead III, and a T-wave inversion in lead III.
Right Axis Deviation: The heart’s electrical axis shifts to the right, suggesting the right ventricle is working harder.
Right Ventricular Strain: T-wave inversions in the right precordial leads (V1–V3) and possibly V4R, indicating strain on the right side of the heart.
Right Ventricular Hypertrophy: A larger R wave in V1, right axis deviation, and sometimes a strain pattern with ST depression in the right-sided leads.
Right Bundle Branch Block: A new RBBB can appear, showing that the right ventricle is under stress.
Second Degree SA block, Type II
Intermittent P waves “drop out” of the rhythm, while subsequent P waves arrive “on time”.
distance from one p wave to the other is the same


Second Degree SA block, Type I
The distance between P waves shortens until a P wave is dropped.
You have a wide complex tachycardia is it VT or SVT with Aberrancy
what ECG findings indicate VT
AV dissociation
p waves seen in amongst the QRS,s occurring out of sync
Fusion and capture beats
normal QRS or strange narrow looking QRS in the wide QRS,s
Lack of RBBB or LBBB morphology
wide QRS but no BBB morphologies
V1,V2 are positive (RBBB) but monophasic no rSR, RSR patterns (no M shape) and V6 is all Negative (QS patters)
V1,V2 are negative (LBBB) but there is a q wave in V6, or in V1,V2
r onset to S nadir > 60ms (1.5 small boxes)
notched downstroke
initial r > 30 ms
Chest Lead concordance
all chest leads pointing same way
slower initial ventricular activation velocity and faster later velocity
forward shark fin = VT
Backwards shark fun = SVT with aberrancy
list as many ACS red flags or risk factors as you can
· Age >45M, >55F (Males more likely but females’ worse outcomes)
· Family Hx Cardiovascular Disease 1st Degree relative <45M, <55F
· CAD
· Pervious MI / ACS / OCI / CABG
· Smoker
· Hypertension
· Diabetes
· Dyslipidaemia LDL, HDL
· Obesity / Central Adiposity
· Sedentary lifestyle
· Poor diet
· Excess alcohol
· Psychosocial Stress
· Kidney Disease
· Cocaine / Stimulant use
· Pressure, Tight, Heavy, Crushing
· Radiation Arms, Jaw, Neck, Back
· Ongoing 10+ min
· Provinciated Positional, Palpation, Breathing
· Diaphoresis
· Nausea / Vomiting
· Dyspnoea
· Pallor
· Anxiety
· Syncope / near syncope
· Elderly, Female, Diabetic
Dyspnoea, Indigestion, Fatigue, Syncope
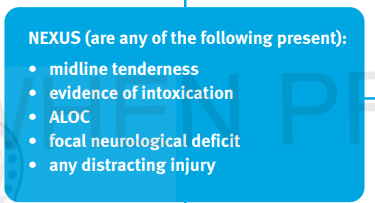
NEXUS criteria
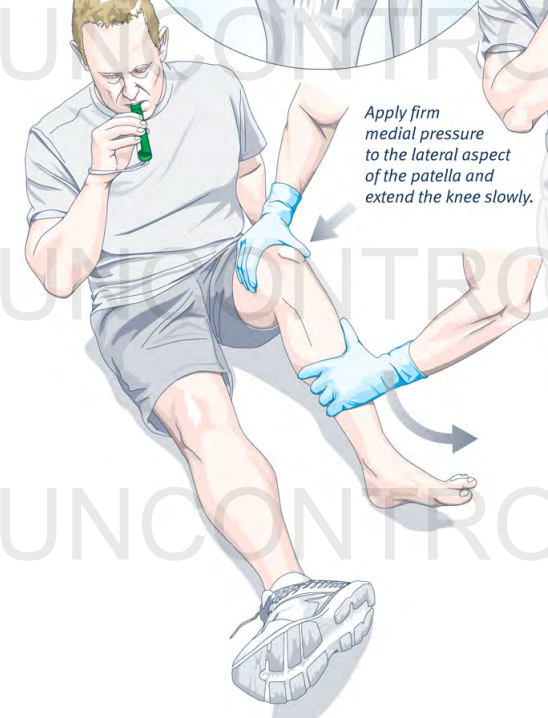
Patella relocation
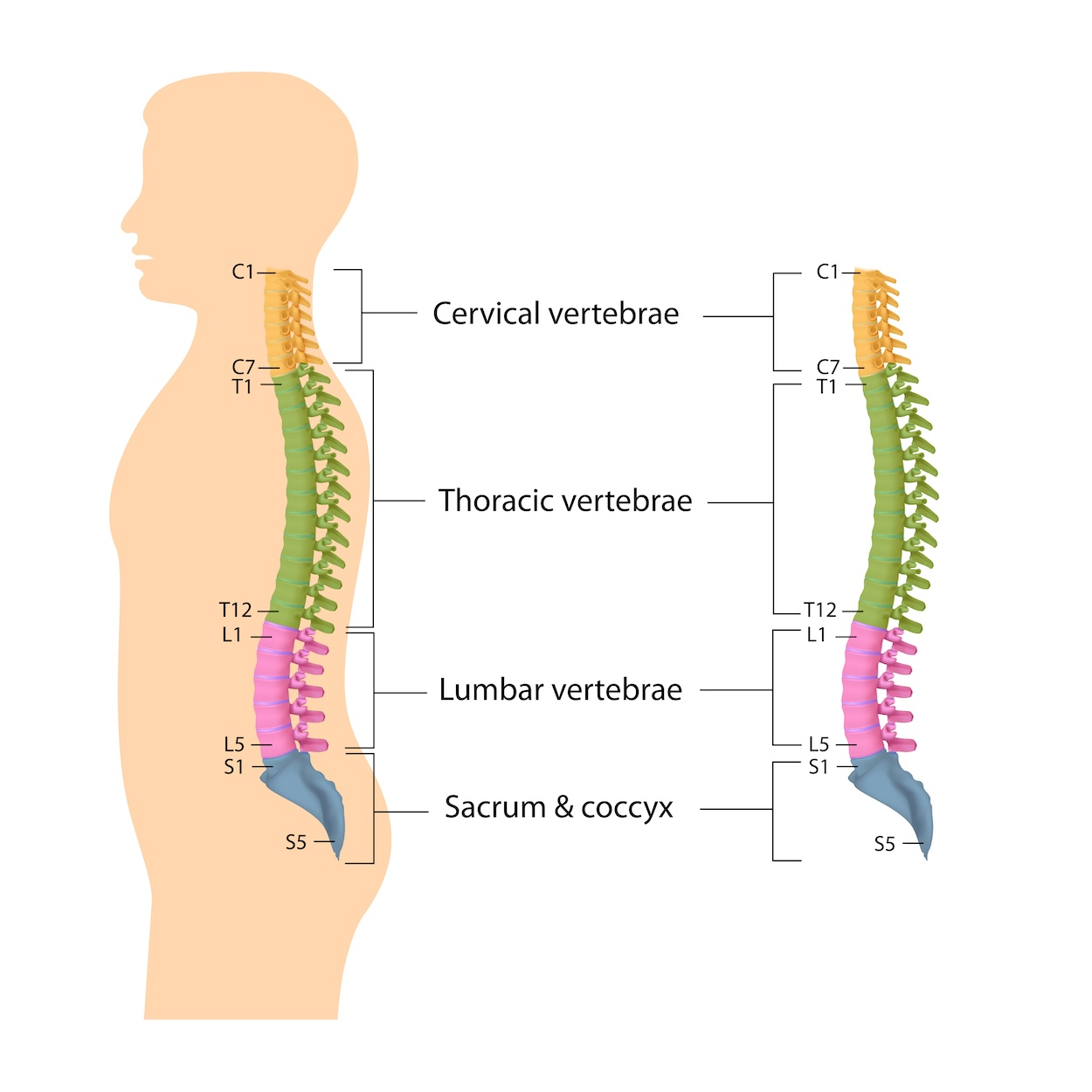
cervical thoracic and lumbar
Suicide Risk questions
Means - is method available
Method - is method lethal? level of detail?
Plans - Rehearsals? time/date? place?
Intent - Plans to carry through? plans to actually die?
Thoughts - Anxious, turmoil? worthlessness? Hopelessness?
Supports - Friends? Family? Case worker? Social network?
History - Personal/family Hx? Pervious attempts? Other illness?
Autonomic dysreflexia symptoms
Above the level of injury (parasympathetic response):
Severe headache (very common)
Flushing/redness
Sweating
Nasal congestion
Blurred vision
Anxiety / feeling of doom
Pupils may dilate
Seizure, pathophysiology and causes
uncontrolled excessive electrical activity in the brain, imbalance between GABA and Glutamate
GABA = inhibitory
Glutamate = excitatory
Reduced GABA (EHOT/Benzo withdrawal)
Excessive glutamate activity (inflammation)
structural abnormalities
Metabolic imbalance
Hypoxia
Toxins/drugs
Fever
Infection
Head injury
chronic seizures normally happen due to excessive excitatory/glutamate pathways, normally diagnosed in happens in people over 60 and children
Seizure types, ang useful info to capture, and status
Focal
one hemisphere, aware or impaired awareness, can progress to genialized
Generalized
Tonic-Colonic, tonic stiffening + colonic rhythmic jerking
Tonic, sudden stiffening in arms and legs/ pelvic thrust
Myoclonic, sudden jerking/electric shock, irregular, single muscle or group
Colonic, repetitive rhythmic jerking contractions
Atonic, sudden loss of tone/drop
Absence, brief staring episodes
Unilateral vs bilateral, type, eye behavior, head turning, automatisms (lip smacking, eye blinking etc.) duration, post-ictal phase, incontinence, tongue biting.
It recommended to film seizures, 20-30% of epileptics are misdiagnosed.
status epileptics = seizure > 5 min or two without full recovery in-between
Seizure treatment escalation and reversable causes, airway and duration concerns
benzodiazepines, Midazolam
anticonvulsants, levetiracetam
anesthetics, Ketamine
Reversable causes
Hypoglycemia - Glucose
Eclampsia - Magnesium Sulfate
Hypoxia - Oxygen and ventilate
CNS infection - Antibiotics, Cefazolin
Hyponatremia - 3% hypertonic saline
Alcohol or Benzo withdraw - Benzos
Hyperthermia - cooling
airway compromise and aspiration = high risk, Laryngospasm mechanism is compromised during seizure and there will by lots of salivation and possibly tongue biting, Recovery position + NPA
The longer a seizure goes on for the less likely patient will respond to treatment, GABA becomes less responsive (moved into cells) and benzos become less effective, NMDA (with glutamate binds to) moves out of cell so 2nd line also loose effectiveness with time because glutamate pathways become intrenched. Treatment must happen quickly
Stroke, types, Risk factors
Ischemic (clot) embolic (clot travels) thromboembolic (atherosclerotic plaque rupture)
Hemorrhagic (bleed)
TIA
Risk factors include
hypertension
AF
Diabetes
Obesity
hyperlipidemia
age
previous stroke
TIA
Stroke symptoms + ischemic stroke management
Facial droop (not including forehead)
Limb weakness
Dysarthria = difficulty producing speech/slurring
Aphasia = language problem (Problem with creating or understanding language)
Expressive (comprehension preserved, can produce language)
Receptive (comprehension in pared)
Global (both)
Dysphagia (difficulty swallowing)
Diplopia (double vision)
Dysmetria (loss of depth perception)
Vertigo
Ataxia (balance)
Vomiting
Visual disturbances
Altered LOC
crossed neurological findings (Face affected on one side + body affected on the other side)
hearing loss/tinnitus
permissive hypertension up to 185 sys (to push around clot)
don’t over oxygenate (causes collateral vasoconstriction in cerebellar and coronary vascular beds) O2 = ROS (reactive oxygen species) with interact with NO to make ONOO-, this stops NO being able to act as a vasodilator.
HINTS + exam
Only relevant for continuous vertigo/dizziness
Head impulse L & R | Corrective saccade | Normal/no corrective saccade |
Nystagmus (loo L & R into paper) | Horizontal unidirectional, increases when looking towards nystagmus direction | Horizontal but direction changing with gaze, vertical, torsional/rotational |
Test of Skew, paper in front of eye | No skew/deviation | Vertical skew/correction |
Rub fingers next to ears Anterior Inferior Cerebellar Artery stroke | No new hearing loss | New hearing loss |
Hemorrhagic stroke symptoms & Hx & management
Sudden thunderclap headache
sever hypertension
seizures
vomiting/nausea
unequal pupils/unreactive pupils
decreased GCS
Cushing’s triad
bradycardia
hypertension with widening pulse pressure
irregular respirations
reversal of anticoagulants (if anticoagulated)
BP control (try to get <140) Beat blockers
ICP management, head 30°, neutral neck (avoid veinous obstruction), manage pain, Hypertonic fluids (3% saline)
Neurosurgery
Stroke mimics
Hypoglycemia
Migraines
Seizure post ictal
Bells palsy (affects facial nerves, forehead effected, dry eyes, altered sense off taste)
Intoxication
Inner ear causes of vertigo
BPPV
Brief spinning episodes triggered by head movement
Caused by displaced calcium crystals in inner ear
Dix-Hallpike test (sitting > turn head 45° > lay on back quickly with head off end of bed > wait 30-60 seconds > sit back up repeat on other side (after a few seconds pt should experience a transient vertigo attack, with Nystagmus) whichever side produces more symptom id offendig side
Epley maneuver (sitting > turn head 45° to offending side > lay on back quickly with head off end of bed > wait 30-60 seconds > rotate head 90° to other side > wait 30-60 seconds > roll body to lateral of the direction pt is facing and with face downwards into bed > wait 30-60 seconds > back to sitting position)
Vestibular neuritis (highest risk posterior stroke mimic)
sudden severe vertigo lasting days, worsened by movement
Usually viral inflammation of vestibular nerve
HINTS, head impulse = catch up saccade, Nystagmus = unidirectional horizontal, no skew deviation, no hearing loss.
Prochlorperazine (Stemetil)
Labyrinthitis
similar to vestibular neuritis but also causes hearing loss or ringing, worsened by movement
inflammation of labyrinths (inner ear), usually viral
HINTS
Prochlorperazine (Stemetil)
Meniere’s disease
Episodes of vertigo (20 min to hours) with hearing loss, tinnitus and ear fullness, worsened by movement
build up of inner ear fluid
HINTS
Prochlorperazine (Stemetil)
Stroke assessments, questions etc.
NIHSS-8 1/24 |
Modified Rankin Score 0-5 |
BSL BP |
Exact Time of onset? |
Last known well? |
Wake-up stroke? |
Sudden or gradual onset? Hrs? |
Fluctuation? |
Trouble understanding me? |
Anomia, Difficulty finding words? |
Paraphasia, Using incorrect words? |
Vision Changes? |
Seizure at onset? Todd’s paresis |
Syncope? |
Blood thinners? |
Previous stroke/TIA? |
Atrial fibrillation? |
Smoker? |
Hypertension? |
Diabetes? |
Family history stroke/TIA? |
Recent Head Strike/fall? |
Headache? |
Neck pain? |
New hearing loss? rub hands next to ears |
STROKE ( ATYPICAL) |
Sudden severe vertigo |
Diplopia (double vision) |
Dysarthria (slurred speech) |
Ataxia (loss of coordination) |
Dysmetria (over/undershooting target) |
Dysphonia (hoarseness, rasp, strain) |
Dysphagia (swallowing) |
|
|
Occipital headache (back of head) |
Positional vertigo Inner ear |
Continuous vertigo Central |
Constant Central |
Episodic Inner ear |
Ability to walk |
Other Nuro signs |
Nystagmus |
Head Impulse L and R normal = central |
Test of skew |
New hearing loss? rub hands next to ears |
types of syncope
Type | Simple mechanism | Common causes | Risk level | Key things to assess |
|---|---|---|---|---|
Vasovagal | Nervous system overreacts → BP and HR drop → brain gets less blood | Pain, stress, blood, standing, heat | 🟢 Usually low | Trigger? Prodrome (nausea, warmth, tunnel vision)? Recovery quick? |
Orthostatic | Standing → blood pools in legs → BP drops | Dehydration, bleeding, sepsis, medications | 🟡 Moderate | Orthostatic vitals, hydration, meds, bleeding, Postural BP change |
Cardiac | Heart suddenly doesn’t pump enough blood | Arrhythmia, valve disease, PE, structural disease | 🔴 Highest concern | ECG, palpitations, exertion, chest pain, FHx sudden death |
Neurologic | Brain problem (not usually true syncope) | Stroke, seizure, TIA, autonomic dysfunction | 🔴 High if suspected | Neuro exam, FAST/NIHSS-8 confusion, headache, focal signs |
Subarachnoid haemorrhage (SAH) — Symptoms
Sudden severe thunderclap headache
“Worst headache of life”
Neck pain / neck stiffness
Nausea
Vomiting
Photophobia
Collapse
Loss of consciousness
Reduced GCS
Confusion
Seizure
Visual disturbance
Diplopia
Focal neurological deficits
Dizziness / vertigo
Weakness
Speech changes
Meningism
Hypertension (sometimes)