Body Sites: Blood and Respiratory
1/105
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
106 Terms
1:10
The traditional blood-to-broth ratio used to reduce the bactericidal effects of serum in adults is what?
collecting the recommended volume of blood in a 24hr period
What variable is crucial in ensuring a high sensitivity of blood cultures?
there has bee a decrease or lapse in proper antiseptic blood culture collection technique
Rates of Staphylococcus epidermidis isolated in blood cultures for the past month on average 4x higher than pervious months. What is the best explanation for increase in isolates?
Granulicatella or Abitrophia (Nutritionally Variant Strep)
A MLS noted tiny white colonies on CHOC and no growth on BAP of a blood culture at 24hrs. The positive blood smear was reported out as gram-positive cocci in chains. What organisms are most consistent with this pattern of growth and gram-stain?
reject the specimen for culture & call the patient care team to request a new specimen
A sputum was received for culture, the direct smear was performed.
Based on the representative field shown, the MLS should do what?
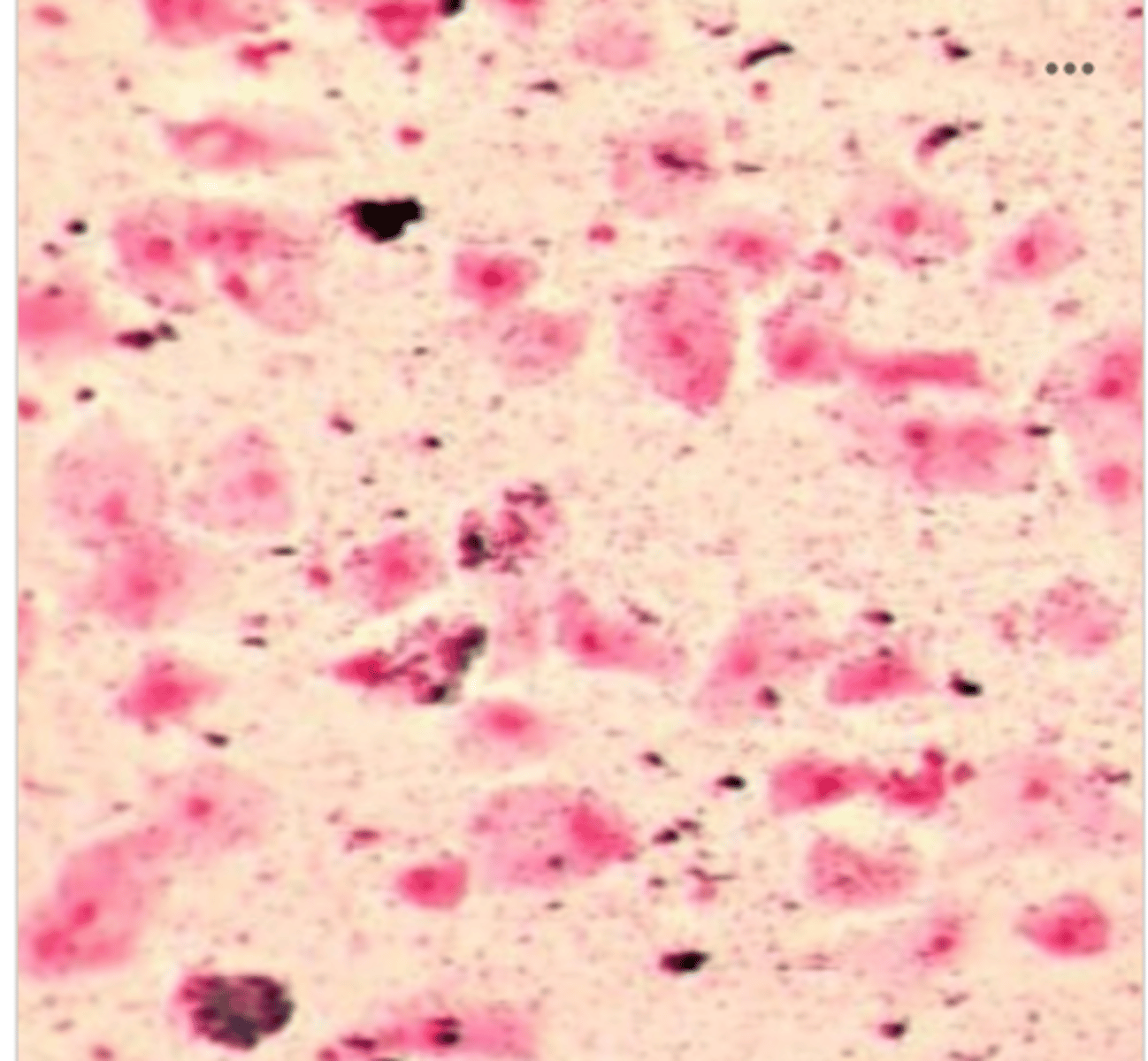
S. pneumoniae and H. influenzae
Which organisms are most frequently isolated form middle ear culture of individual with otitis media?
Pneumocysis jirovecii
Which organism most commonly causes an opportunistic infection in patients with HIV/AIDS?
culture on buffered charcoal yeast extract agar
A bronchoscopy sample with request for culture Legionella is sent to the lab. What is the correct plating protocol?
Butyrate esterase
An elderly patient presents to the ER with difficulty breathing
Blood count: shows an elevated WBC count with increased segmented neutrophils
Sputum gram stain: reported to contain a large amount of WBCs and a large amount of gram-negative diplocci
Plate: white, shiny colony that scoots across the agar like a hockey puck
What test could be utilized to obtain an identity for the organism?
Microdase
A positive blood culture shows a very yellow colony on the BAP. The gram stain reveals gram-positive cocci in tetrads and clusters. Catalase is positive & Coagulase is negative (slide & tube).
What is the most appropriate next test for this organism?
true
True or False:
Very high WBC counts can lead to false-positive blood cultures
5-7 days
For how long should routine blood culture bottles be incubated on an automated blood culture instrument?
false
True or False:
Acute bronchitis is most commonly bacterial in origin
NAAT
What is the most common method of testing for Mycoplasma pneumonia, Bordetella pertussis and Chlamydia pneumoniae?
72 hours
How long should we incubate and examine routine lower respiratory cultures?
Streptococcus pyogenes
What is the most common cause of bacterial pharyngitis?
beta-lactam
A PCR respiratory panel was run on a NP specimen from a 17 year old female and was positive for Mycoplasma pneumoniae. Which class of antibiotic would NOT be effective to treat the infection?
**hint: Mycoplasma's do not have cell walls
Bronchoalveolar lavage (BAL)
A quantitative lower respiratory culture can be performed off of what type of specimen?
true
True or False:
Streptococcus pneumoniae is the most common cause of community acquired pneumonia in adults
BAP, CHOC, MAC
Which media would be most appropriate for a lower respiratory culture?
CO2
For lower respiratory cultures, where do we incubate BAP and CHOC?
ambient air
For lower respiratory cultures, where do we incubate MAC?
small, round, tan-brown colonies
Which is the best description of the colony morphology of Haemophilus influenzae on CHOC agar?
Optochin & Bile Solubility
What are the best 2 tests to differentiate Streptococcus pneumoniae and Viridans Streptococci?
improper antiseptic technique during collection led to contamination of the aerobic bottle from 1629
A patient arrived in the ER 4/20/26 and 2 blood cultures were collected: one set at 1629 & another set at 1632
Only the aerobic bottle from the set at 1629 flagged as positive by day 5 of incubation
The blood smear from the aerobic bottle showed diphtheroids.
What is the best interpretation of this result?
Staphylococcus aureus, Pseudomonas aeruginosa, Klebsiella pneumoniae
What are 3 common causes of Ventilator Associated Pneumonia?
gram-negative coccobacilli
What is the gram stain of Haemophilus influenzae?
Intravascular
Begins in the blood, continuous -- Primary Source
- Acute infective endocarditis
- Subacute endocarditis
- Intravenous catheters
Acute infective endocarditis
Subacute endocarditis
Intravenous cartheters
What are the 3 intravascular infections seen in Bacteremia?
Staph aureus, Strep pyogenes, Step pneumoniae
Intravascular Bacteremia
What organisms are responsible for Acute Infective Endocarditis?
- Rapid on set of disease with severe symptoms
viridans group Strep, HACEK group, CNS
Intravascular Bacteremia
What organisms are responsible for Subacute endocarditis?
- Slower progressing infection
Staph spp (attach well to catheters)
Enterococcus & Yeast
Intravascular Bacteremia
What organisms are responsible for Intravenous catheters?
- Directly entry into bloodstream
Extravascular
Enter blood from another source (typically lymphatic system) -- Secondary Source
- Pneumonia
- Urogenital tract (Kidneys)
- Intraabdominal
- Skin (agents that cause cellulitis, decubitus ulcers, burns)
Strep pneumo, Staph aureus, Pseudomonas, Klebsiella, Enterobacter
Extravascular Bacteremia
What organisms are responsible for Pneumonia?
E coli
Extravascular Bacteremia
What organisms are responsible for UTIs?
E coli, Klebsiella, Enterococcus
Extravascular Bacteremia
What organisms are responsible for Intraabdominal infections?
Septicemia
Constant & multiplying bacteria in the blood and harmful effect bacteria produce
Systemic Inflammatory Response Syndrome (SIRS)
The systemic response to an infectious or noninfectious trigger
Criteria for SIRS
Must include 2 of the following:
Temperature: >38C or <38C
Heart Rate: >90bpm
Respiratory Rate: >20 breath/min or pCO2 <32mmHg
WBC count: >12,000/uL or <4,000/uL
Sepsis
Infection with SIR
Hypotension
Systolic <90mmHg
Arterial <70mmHg or reduction of >40mmHg from baseline
Severe sepsis
Sepsis with organ dysfunction, hypoperfusion or hypotension
Septic shock
Sepsis with hypotension despite adequate treatment (IV fluids, vasopressors)
Lab Signs of Septicemia
C-reactive protein (CRP)
Procalcitonin
Lactic Acid (Lactate)
Monocyte Distribution Width
C-reactive protein (CRP)
Lab Signs of Septicemia
Synthesized in the liver -- marker of inflammation& tissue damage
Sensitive but not specific
Procalcitonin
Lab Signs of Septicemia
Often produced by cells in response to bacterial infection
Normally, gets converted to calcitonin so our levels are almost undetectable
During serious infection, a different pathway is followed leaving it being released into the blood
Lactic Acid (Lactate)
Lab Signs of Septicemia
Increased levels can indicate lack of O2 causing acid/base imbalance in the body
Increase often seen in sepsis
Fungemia
Nonbacterial Etiologic Agents of BSI
Fungi
- Candida spp
Parasitemia
Nonbacterial Etiologic Agents of BSI
Parasites
- Plasmodium, Trypanosoma, Babesia
Viremia
Nonbacterial Etiologic Agents of BSI
Viruses
- Epstein-Barr virus, cytomegalovirus, HIV
1. Cleanse skin with chlorhexidine & scrub for 1 min
2. Let skin sit for 1 min
3. Draw aerobic bottle, then draw anaerobic bottle
What are the steps for blood culture collections?
Nutrient broth
Anticoagulant (SPS)
Resin Beads
Blood culture bottles used are dependent on automated system being used but all contain what 3 things?
for growth
What is the purpose of the nutrient broth in blood culture bottles?
prevents coagulation & traps bacteria
What is the purpose of the anticoagulant (SPS) in blood culture bottles?
inactivate antimicrobials
What is the purpose of the resin beads in blood culture bottles?
8-10mL
For an adult blood culture, how much blood is collected?
1-5mL
For a pediatric blood culture, how much blood is collected?
automated
Blood culture bottles are most commonly incubated where?
5-7 days at 35-37C
How do we manually incubate blood cultures?
How long & at what temp?
gram-stain
Once growth is detected in a blood culture (positive), what do we do next?
true
True or False
A positive gram-stained smear from a blood bottle is a critical value
BAP, ABAP, CHOC
What media is set up based on gram stain result for a blood culture?
3%
Contamination rates in blood cultures should be kept below what percent?
improper antiseptic technique
Contamination of blood cultures is most commonly due to what?
Bacillus, Corynebacterium, Cutibacterium acnes, Micrococcus
What are 4 likely contaminants seen in 1 out of several blood culture bottles?
Likely Pathogen
Growth of same organisms in multiple blood culture sets
Growth of organisms not considered part of normal skin flora
Growth of blood culture organisms matches organism causing primary infection or is consistent with clinical presentation
Upper and Lower
Respiratory Cultures are separated based on what?
Upper Respiratory
Abundant normal flora
Consists of: Throat, Nasopharynx, Mouth, Sinuses/Ear
Lower Resipratory
Sterile Sites
Consists of: Trachea, Bronchi, Lungs
Respiratory Tract Host Defenses
Nasal hairs
Antibacterial substances in respiratory secretions (lysozyme)
Goblet cells & cilia of the columnar epithelial cells
Coughing, sneezing, swallowing
Alveolar machrophages
Upper Respiratory Tract Infection
Pharyngitis
Sinusitis
Otitis media
Laryngitis
Croup (laryngotracheobronchitis)
Epiglottis
Peritonsillar abscess
Stomatitis
Thrush
Periodontal infections
Parotitis
Pharyngitis
Upper Respiratory Tract Infections:
Inflammation of the back of the throat (pharynx)
Strep pyogenes (primary bacterial cause), Arcanobacterium, C. diptheriae
Sinusitis
Upper Respiratory Tract Infections:
Inflammation of the nasal sinus tissues
Strep pneumo, H. influenzae, M. catarrhalis, Staph aureus
Otitis Media
Upper Respiratory Tract Infections:
Inner Ear Infection
Strep pneumo, H. influenzae, M. catarrhalis
Laryngitis
Upper Respiratory Tract Infections:
Inflammation of the voice box (larynx)
Strep pyogenes, H. influenzae, Staph aureus
Croup (Larynogotracheobronchitis)
Upper Respiratory Tract Infections:
"Seal Bark" Cough
Epiglottis
Upper Respiratory Tract Infections:
Inflammation of epiglottis
H. influenzae
Peritonsillar abscess
Upper Respiratory Tract Infections:
A pus-filled infection near the tonsils
Anaerobes
Stomatitis
Upper Respiratory Tract Infections:
Inflammation of the oral mucosa
HSV
Thrush
Upper Respiratory Tract Infection
Fungal infection in the mouth and/or throat
Candida spp
Periodontal infections
Upper Respiratory Tract Infection
Bacterial infection that destroys the gums, ligaments, and bone supporting the teeth, often caused by plaque buildup
Polymicrobial, Anaerobes
Parotitis
Upper Respiratory Tract Infection
Inflammation of the parotid salivary gland
Mumps
Lower Respiratory Tract Infection
Acute bronchitis
Acute pneumonia
Chronic pneumonia
Cystic Fibrosis
Infections in pts with HIV
Lung abscess
Pleural infection
Acute Bronchitis
Lower Respiratory Tract Infection
Inflammation of bronchial tubes
Over 90% of time caused by viruses
If Bacterial: Mycoplasma pneumo, B. pertussis (whooping cough), & Chlamydia pneumo
Acute Pneumonia
Lower Respiratory Tract Infection
Routes of infection: aspiration, inhalation of airborne droplets, seeding of lung via blood from distant site infection, upper airway colonization/infection that extends to the lung
Children Acute Pneumonia
Lower Respiratory Tract Infections
- More than 80% of cases are viral (RSV, Influenza, Parainfluenza, Adenovirus)
Strep agalactiae, E coli, Listera
What 3 organisms cause Acute Pneumonia in NEONATES?
M. pneumo, C. pneumo, H. inflenzae, Step pneumo, Staph aureus
What 5 organisms cause Acute Pneumonia in CHILDREN?
Viruses, M. pneumo, C. pneumo
What 3 organisms cause Acute Pneumonia in YOUNG ADULTS?
Community Acquired Pneumonia (CAP)
Adult Acute Pneumonia
Strep pneumoniae, Viral, M. pneumoniae, C. pneumoniae, H. influenzae, Legionella
Hospital Acquired Pneumonia (HAP)
Adult Acute Pneumonia
Enterobacterales, Pseudomonas, Acinetobacter, Staph aureus (MRSA), Strep pneumoniae, H. influenzae, Legionella
Chronic Pneumonia
Lower Respiratory Tract Infections
Mycobacteria spp, Actinomyces, Nocardia, mixer aerobic & anaerobic bacteria, dimorphic fungi, Cryptococcus
Cystic Fibrosis
Lower Respiratory Tract Infections
Genetic Disorder
Staph aureus, H. influenzae, non-fermenter organisms
Infections in pts with HIV
Lower Respiratory Tract Infections
Thrush, Pneumocysits pneumonia, dimorphic fungi, Cryptococcus neoformans, tuberculosis
Lung abscess
Lower Respiratory Tract Infections
Pus-filled localized cavity
Specimen Collection of Lower Respiratory
Sputum
Suctioning - Lukens trap
Bronchoscopy
Mini-BAL
Thoracentesis
Biopsy
Sputum
Specimen Collection - Lower Respiratory
- May be expectorated or induced
Suctioning - Lukens trap
Specimen Collection - Lower Respiratory
- Endotracheal Tube (intubation) - shorter term airway management
- Tracheostomy Tube - longer term airway management
Bronchoscopy
Specimen Collection - Lower Respiratory
- Bronchial wash - specimen from larger airways
- Bronchoalveolar lavage (BAL) - specimen from smaller airways
- Bronchial brushing
Mini-BAL
Specimen Collection - Lower Respiratory
- Catheter instead of bronchoscope, smaller amount of saline used