Exam 4 (questions I dont know)
1/96
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
97 Terms
If the dose rate in air at 80.5 cm for a 10 x 10 cm field is 100 rad/min, what is the dose rate in air at 100.5 cm for a 12.5 x 12.5 cm field?
A. 120 rad/min
B. 100 rad/.min
C. 80 rad/min
D. 64 rad/min
D. 64 rad/min
reasoning:
inverse square law
This one might seem like a change in field size with a change in distance, but noticed that the change in field size is already given to you, so that's not it.
A patient is treated with an isocentric Co60 unit at 80 cm SAD with a 10 x 10 field at 80 cm. The treatment depth for parallel opposed fields is 6 cm each. The dose rate in air at 80 cm is 100 rad/min for a 10 x 10 field at the TAR at 6 cm is .870. Assuming no timer error, calculate the time to set in order to deliver 100 rad at isocenter with each field.
A. .87 min
B. 1.00
C. 1.15
D. 1.6
2. For the previous problem, the dose at .5 cm in the patient for a single field is:
A. 172 rad
B. 137 rad
C. 115 rad
D. 100 rad
Question 1
C. 1.15
Reasoning:
“100 rad with each field” means 100 rads per field
Time: dose per field / Factors Affecting Output Multiplied
100/ .870 × 100 = 1.15
Question 2
x/1 = 100/.87
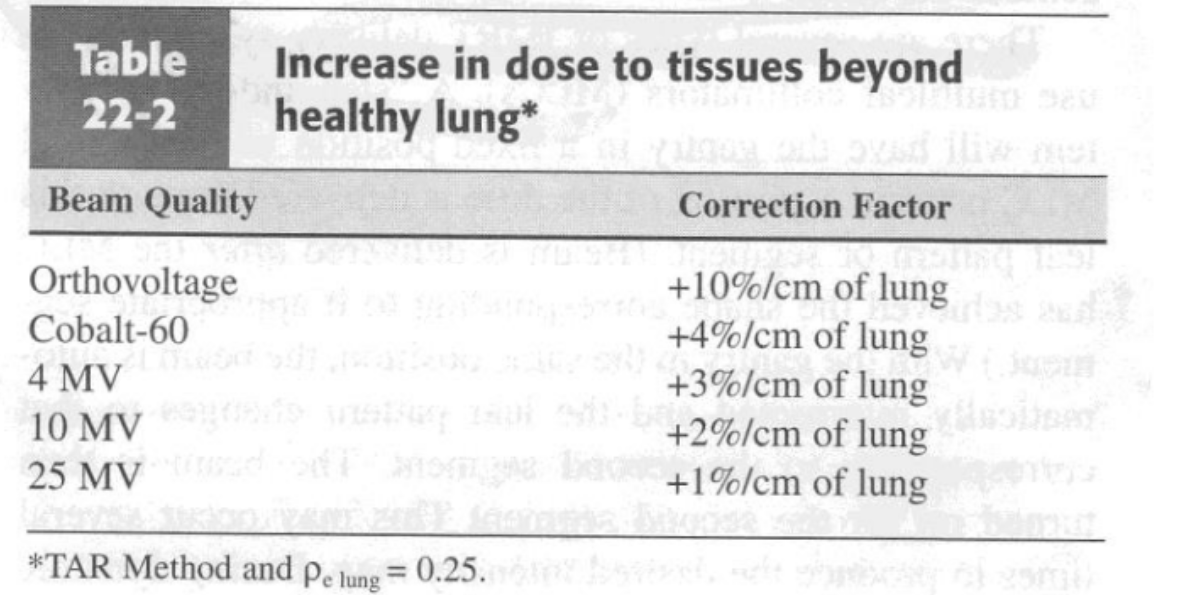
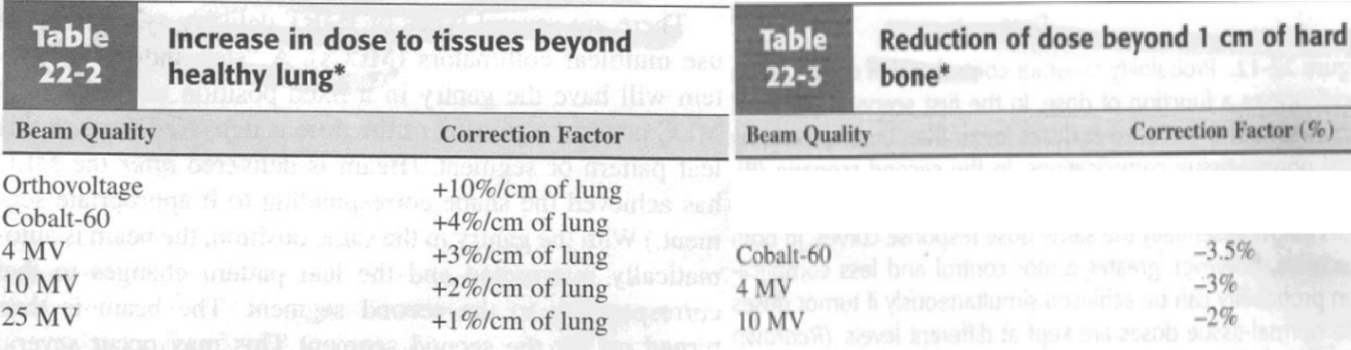
A lateral tracheal port treats through 6cm of lung with Co60 radiation. If calculations are performed with standard tables, the delivered tumor dose is estimated to be:
A. equal to the calculated value
B. about 24% above the calculated value
C. about 6% above the calculated value
D. about 12% below the calculated value
B. about 24% above the calculated value
Reasoning:
Rule of thumb: dose increase of 4%/centimeter of aerated lung. 6 cm of lung described in question. Thus: 6×4 = 24% increase/above the calculated dose value
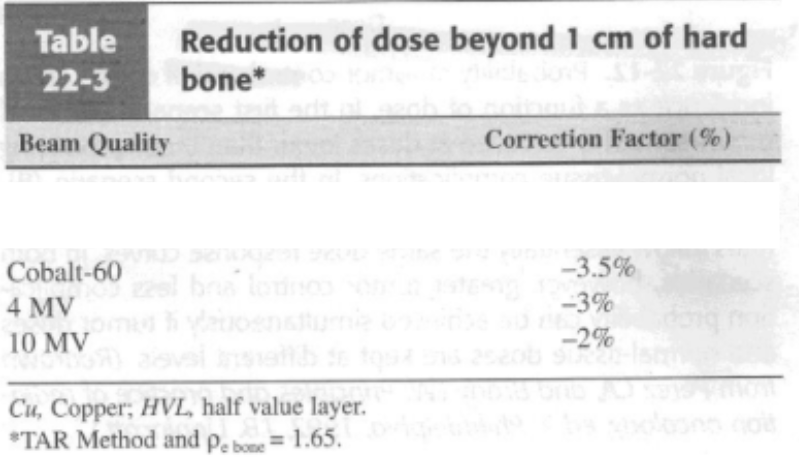
Reduction of dose beyond 1 cm of bone chart
A breast treatment includes an anterior yoke port which is treated to 200 cGy given dose per fraction for 25 fractions. Assume that the midline depth dose for the anterior field is 65% and it is desired to boost the total midline dose to 5000 rad with 10 posterior treatments for which the midline depth dose is 62.5% The given dose for each posterior treatment is:
A. 280 rad
B. 175 rad
C. 109 rad
D. 288 rad
A. 280 rad
Reasoning:
Part 1: Figure out dose given to midline with initial tx
x/200 = 65%/100% → 3250 cGy
Part 2: Figure out how much dose we need to boost midline to 5000
5000-3250 → 1750 cGy left to boost to 5000
Part 3: Figure out dmax from boosted field
1750/10 fractions→ 175 cGy per fraction
x/175 = 100%/62.5% → 280 rad
Equally weighted ,parallel opposed megavoltage x-ray fields are used to deliver a midline dose of 6000 rad. If the surface dose of a single field is 33% and the exit dose is 40%, what is the total skin dose as a result of the treatment if the midline depth dose from each field is 65%?
A. 7300 rad
B. 4380 rad
C. 2190 rad
D. 3369 rad
D. 3369 rad
Reasoning:
Skin receives 33% from the AP and 65% from the PA
33/65 = x/3000 → 1523
40/65 = x /3000 → 1846
1523 + 1846 = 3369
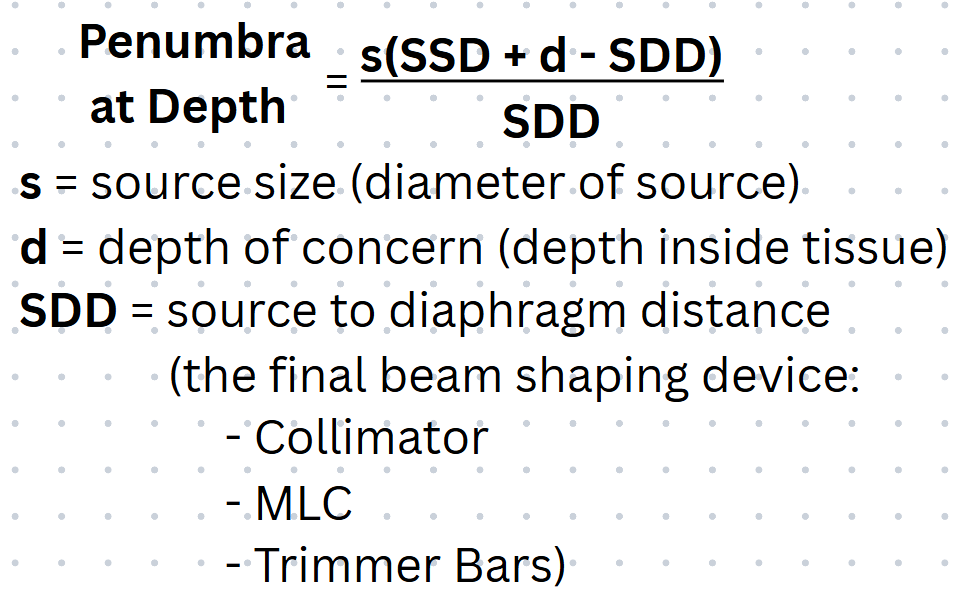
The source in a Co60 unit is 2.5 cm in diameter. The treatment distance is 80 cm and the distance from the source to the final diaphragm is 30 cm. What is the penumbra size 10 cm below the skin?
I'm going to give this one to you since the focus is cobalt math, it's 5 cm. Penumbra is something in our field that is most related to cobalt, so I don't think you'll still need to know this, but be advised that it could come up on the registry exam.
A. 4.2 cm
B. 5 cm
C. 1.2cm
D. 1.5cm
B. 5 cm
Reasoning:
2.5 x (80+10-30)/30 → 5 cm
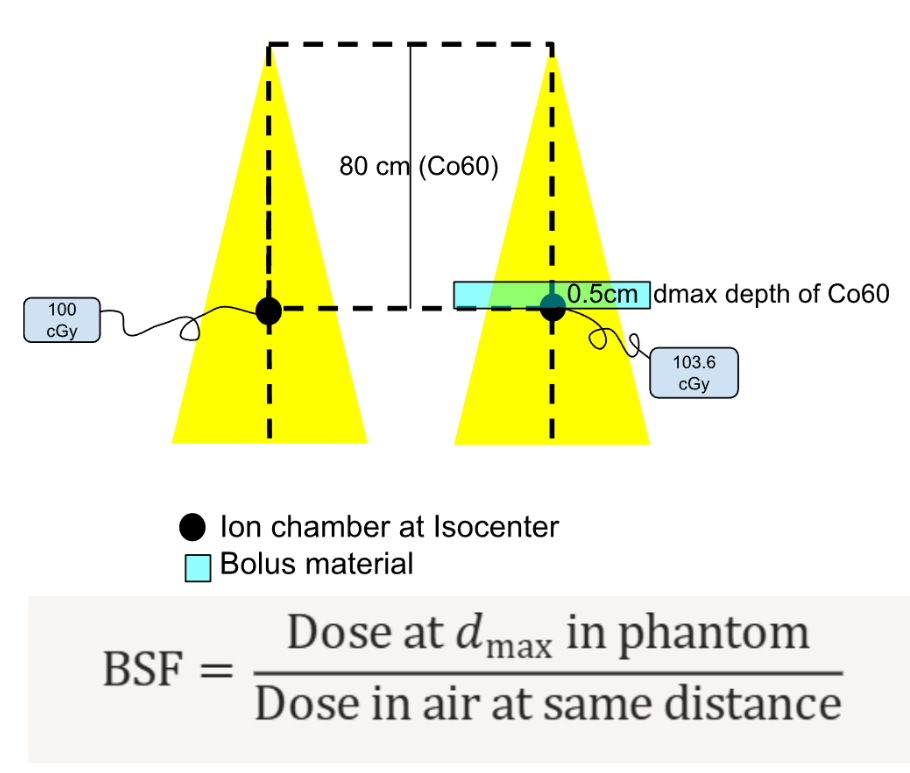
If the measured surface exposure rate is 60/Rminute, and the in air exposure rate is 50 R/minute, the percent backscatter is __________ %
A. 0.2
B. 20
C. 50
D. 500
Reasoning:
BSF always bigger so
BSF = 60/50 = 1.2 → 20% BSF
The maximum depth of a lesion when using an electron beam must not exceed:
A. the 100% %DD curve
B. 10 cm
C. the 80% dose line
D. 20 cm
C. the 80% dose line
Reasoning
1/3 rule useful/ therapeutic beam
If doing a curvature correction on a 6 MV isodose curve, the shift in the curve would be:
A. 2/3
B. 1/2
C. one to one
D. 1/3
B. 1/2
Reasoning:
Old stuff:
For beams 4 MV and lower 2/3 shift
New stuff:
For beams 6MV and higher do ½ shift
For beams 18 MV and higher 1/3 shift

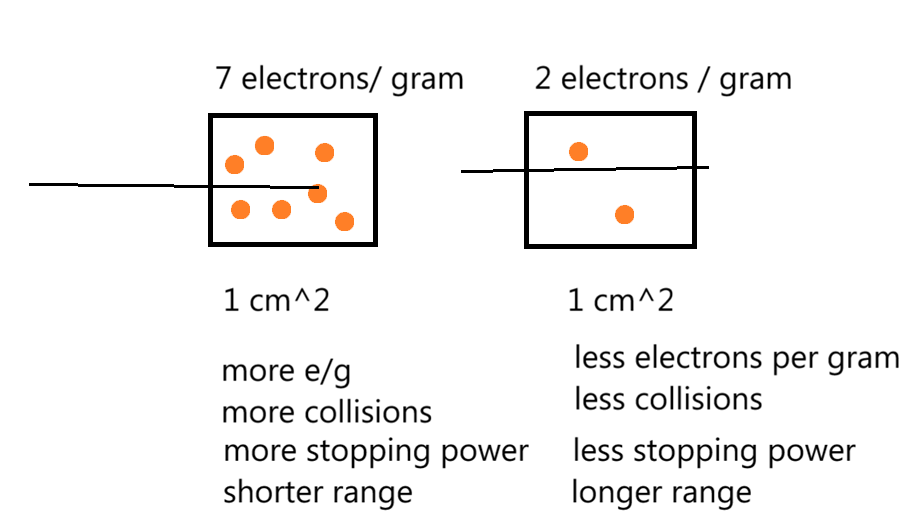
The range of electrons within different materials depends on:
A. output/minute
B. gram-rad
C. electrons/gram/cm2
D. none of these
C. electrons/gram/cm2
Reasoning:
mass stopping power: The rate of energy loss per gram per cm² (rate of E loss/ gram/ cm²)
___
Low z# material = higher Mass Stopping Power
high z# materials = fewer e-/ cm³
e- beams depend mostly on collisions with other e- (as opposed to photon beams)
high z# materials = e- more tightly bound = less available for interactions
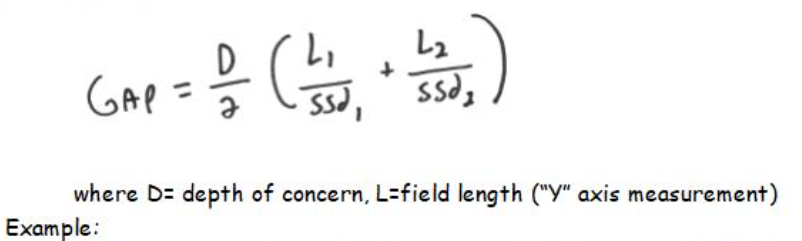
Which is not an accurate way to junction or gap 2 fields? By the way, be sure you know the gap formula for the exit exams and for the registry exam!
A. formula
B. matching isodose curves
C. wedges
D. decrement lines
C. wedges
Reasoning:
Dosimetrically:
Dosimetric Isodose Matching
Gap Calculation
Clinically
Split Beam block Technique
Angling (and mirroring) the tx table
Field Feathering
Gap formula
SAR is NOT useful in which of the following?
A. irregular fields
B. point dose calculations
C. dose received under blocks
B. point dose calculations
Reasoning:
SAR = scatter air ratio,
TAR / TMR / PDD are called:
Classical dose calculation systems (or point dose calculation systems)
When using low energy x-rays (100-250 kv) for radiation therapy, consideration must be given to the absorption in bone. This may be as much as:
C. 3 x z# of bone
Mayneard F factor formula
look up what it gives you

What dose data method can be used to correct isodose curves due to irregular skin surface?
A. sieverts integral
B. TAR method
C. %DD + eut
D. SAR method
B. TAR method
Reasoning:
Correct contour irregularities
Effective SSD method
TAR method
Isodose Shift Method (2/3 shift)
List the 6 Methods for Correcting Inhomogeneities
Isodose Shift Method
TAR method
Power Law TAR method
Equivalent TAR method
Generalized Bartho Correction
Delta Volume Method
I’m ToPEG Danny
For homogenous radiation distribution, the wedge angle should be equal to:
A. 180- 2/3 the hinge angle
B. 180-2/3 the wedge angle
C. 90-1/2 the wedge angle
D. 90-1/2 the hinge angle
D. 90-1/2 the hinge angle
Reasoning
WA = 90- HA/2
HA = 180 -WA2
Dmax is defined as:
A. Skin to isocenter distance
B. Depth in which 20% of dose is absorbed
C. Point of peak dose in an irradiated medium
D. Depth where electronic equilibrium occurs
E. More than one but not all of these is correct
E.
C and D are correct
As beam energy increases, %DD:
A. increases
B. decreases
C. stays the same
D. none of these
A. increases
Reasoning:
Energy (direct)
FS (direct)
SSD (direct)
Depth (inverse)
Which of the following quantities is not needed to calculate monitor units for a single field blocked 10 MeV photon beam at 100 TSD?
A. %DD
B. tray factor
C. treatment depth
D. exit dose
E. tumor dose
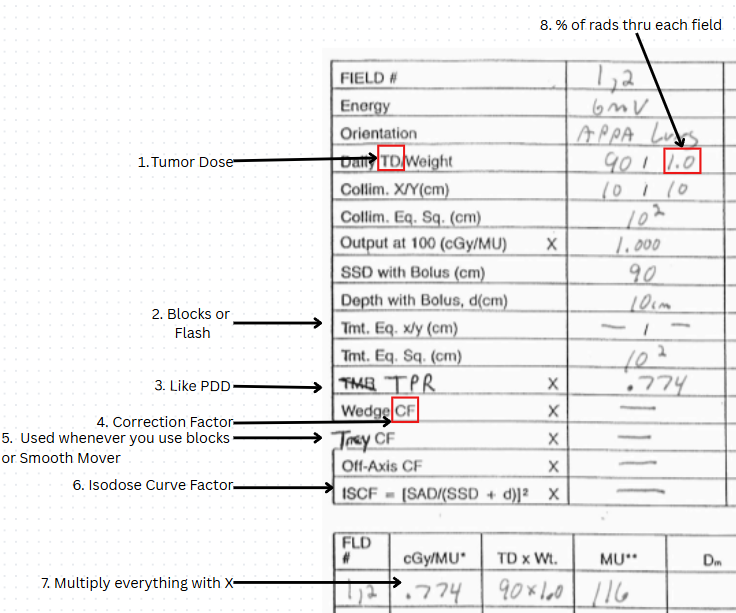
also include an MU calculation chart (what 8 things do you need)
D. exit dose
Reasoning:
B. you do need a tray factor cuz there is a block
D. no need to calculate exit dose cuz it is a single field
FYI: (things)
Energy
Field Orientation x Weight: 2AP: 1PA
Collimator equivalent square to calculate-> Output Factor (Sc)
Treatment equivalent square (EFS)+ Depth to calculate-> TMR (Sp)
Tray CF (if blocks)
Wedge CF (if wedges)
Off-axis CF (for off axis points)
Prescribed isodose line %
TAR tables can be used to determine the monitor units for a given tumor dose when planning a treatment utilizing:
A. SAD parallel opposed ports
B. rotational therapy
C. SSD single port
D. SAD parallel opposed ports AND rotational therapy
D. SAD parallel opposed ports AND rotational therapy
PDD depends on SSD so we cannot use it for SAD treatments or Rotational Txs
15 degree wedge on a 4 MV accelerator:
A. causes an increased skin dose
B. has 2 opposite surfaces at 15 degrees to each other
C. causes a 15 degree tilt of the 100% isodose curve
D. requires no correction factor
E. causes the 50% isodose curve to tilt 15 degrees
E. causes the 50% isodose curve to tilt 15 degrees
Reasoning:
d. you would need a correction factor for the wedge
An isodose curve is created by joining points which have the same:
A. TAR
B. SSD
C. depth
D. dose
D. dose
Isodose curve” points of equal dose
The angle that the 50% isodose curve makes with a line parallel to the surface is the:
A. hinge angle
B. wedge angle
C. heel angle
D. toe angle
B. wedge angle
For superficial or orthovoltage therapy, the BSF:
A. effects air exposure at or just above the skin surface
B. determines the skin dose
C. means back stop factor
D. can be ignored if no lead cutouts are used
E. a and b
E. a and b
Which of the following does not effect TAR?
A. field size
B. quality of the beam
C. depth of overlying tissue
D. TSD
D. TSD
Reasoning:
same things that affect PDD except SSD `
Equivalent square is:
A. necessary for SAR determination
B. a square with the same area as a rectangular field
C. (length x width )2 / length x width
D. 2(length X width) / length x width
B. a square with the same area as a rectangular field
Reasoning:
Equivalent square of irregular fields
2LW / L+ W
or Area/ Perimeter
True/False: Standard wedges can have a beam hardening effect when the radiation is true monoenergetic.
T/F:
If the beam is monoenergenic it cant filter out lower energy beams cuz all beams are the same energy
only when beam is polyenergenic
BSF formula
BSF= Dmax Dose / Dfs
Dsf- dose in free space (air)
FYI:
or if on KV Dmax at the surface
BSF = Dose at the surface/ dfs
Which formula is an expression of the BSF?
A. surface exposure rate / air exposure rate
B. SER + AER / AER
C. SER x AER / 2
D. I1/I2 = D2/D1
A. surface exposure rate / air exposure rate
Reasoning:
BSF = Dose at dmax/ dfs
BUT for KV (where backscatter matters most), the dmax is at the surface
Electron arc therapy has what effect on the Dmax position, as compared with a stationary electron field of the same energy?
A. Moves Dmax towards the surface
B. Does not move Dmax position
C. Moves Dmax away from the surface
C. Moves Dmax away from the surface
Placing blocks into the treatment field affects which of the following parameters?
A. SSD
B. equivalent square
C. STD
D. TTD
B. equivalent square
Reasoning:
Irregular fields must be converted to:
collimator equivalent square (Ceqsq) =
coll. jaw opening
determines: Sc (collimator scatter) / air-output factor
Treatment Equivalent Square/ Effective Field Size (EFS)
blocks/MLC/ flash
Used for irregular or blocked fields
Used to determine Sp (phantom scatter)
FYI
FSOF/ Scp / output factor
Which of the following is not an advantage of SSD setup techniques?
A. more clearance between the gantry and the patient
B. larger field sizes can be achieved
C. less collimator scatter to the patient
D. All of these are advantages of SSD setup techniques
E. More than one but not all of these are advantages of SSD setup techniques
D. All of these are advantages of SSD setup techniques
What is the average TAR for arc setup on Co60/80cm SAD unit if you have the SSD readings every 10 degrees for a 120 degree arc using a 7 x 7 port. 64cm, 65cm,66cm, 67cm, 68cm, 69cm, 69cm, 70cm, 70cm, 70cm, 70cm, 69cm, 68cm. TAR's at these SSd’s are: .64=64cm, .68=68cm, .70=70cm, etc.
A. 0.68
B. .663
C. .607
D. .639
A. 0.68
Reasoning:
ALL TAR added / 13
If an error of greater than 2% is found in a patients treatment, who must be notified immediately?
A. the state
B. the patient
C. the chief therapist or dept. director
D. the physicist or radiation oncologist
D. the physicist or radiation oncologist
The factors which determine the effect of radiation include---1. dose of radiation; 2. physical and psychological status of the patient; 3. volume of tissue treated; 4. frequency of the exposure to radiation
A. 1,2,3
B. 1.2.4
C. 2.3.4
D. 1.2.3.4
D. 1.2.3.4
Reasoning:
higher dose = higher RBE
if patient is doing bad, we might have to discontinue tx
more of the tumor we can irradiate while less normal tissues = more effective tx
frequency of the exposure to radiation = TDF
Question 66
Scatter air ratio was originally described by:
A. Cunningham
B. Gupta
C. Clarkson
D. Hendee
C. Clarkson (came up with it)
FYY:
Cunningham further developed it
For a sloping skin surface, the isodose curves are not perpendicular to the direction of the beam. The skin sparing effect can be maintained and the situation corrected by using:
A. bolus
B. multi-field technique
C. compensating wedge filter
D. none of these
C. compensating wedge filter
Reasoning:
Bolus will correct the isodose curves but does not spare the skin
The 50% central axis depth dose for a 10 x 10cm cobalt field at 80 cm SSD is approximately:
A. 5 cm
B. 8cm
C. 12cm
D. 15cm
C. 12cm
Answer: C this is the correct answer no longer on the registry exam
A lesion is being treated using an arc angle of 100 degrees. The midpoint of the tumor volume is 5cm. The isocenter should be placed at:
A. .5cm
B. 2.5cm
C. 5 cm
D. 7.5cm
D. 7.3-4
Reasoning:
For partial arcs use past pointing technique place isocenter 3-4 cm past the tumor volume
The depth of maximum ionization is MOST dependent on:
A. SSD
B. field size
C. x-ray energy
D. total dose
C. x-ray energy
This concept is still valid....For 60Co, the BSF:
A. continually increases with field size
B. continually decreases with field size
C. decreases with depth
D. increases with field size up to certain field size and then decreases
A. continually increases with field size
BSF depends on
Bigger FS = Bigger BSF
Higher Energy = Lower BSF
The given dose rate increases as field size increases because of:
A. increased scatter from the collimator and the patient
B. change in source activity
C. variation in depth dose
D. variation in radiation energy
A. increased scatter from the collimator and the patient
Reasoning:
When the fs gets bigger…
Sc- more collimation components get exposed = more scatter
Sp- more of the patient tissue gets exposed= more scatter
___
Sc depends more on scatter created by the collimation components:
flattening filter
primary collimator (40×40)
upper parts of the secondary coll jaws
For orthovoltage radiation, BSF is the same as:
A. %DD at the surface
B. %DD at 5 cm depth
C. SAR value at the surface
D. TAR value at the surface
D. TAR value at the surface
Feedback:
note: (By definition) back scatter factor and TAR are the same thing at the surface
BSF = Dmax dose/ dsf for KV Dmax dose is at the surface, so
BSF = Dose at depth/ dsf (just like TAR)
A high energy x-ray beam is incident on the surface of water in a water tank. Indicate which one of the following statements is correct.
A. Maximum does at a the water surface
B. Maximum dose at a depth dependent on the x-ray energy
C. Maximum dose is always at a fixed depth, independent of x-ray energy
D. Dose increase with depth beyond the depth of maximum dose
B. Maximum dose at a depth dependent on the x-ray energy
Define the following
OAR
What is it
What is it used for
SAR:
What is it
What is it used for
Clarkson Method
What is it
How does it work
What values do you need to figure it out
OAR: off axis ratio: dose to points off the CA
how dose changes side-to-side across the beam (lateral variation / beam profile)
Irregular fields + Clarkson
SAR: Scatter Air Ratio (OLD)
Scatter contribution in tissue
OLDER scatter calculations for irregular field→ useful for Clarckson method
BUT REPLACED BY TPC
Clarckson
method for irregular/blocked field dose calculation
breaks field into sectors and sums scatter
Uses:
OAR (beam shape / off-axis dose)
SAR (scatter contribution)- back in the day
central axis dose/output
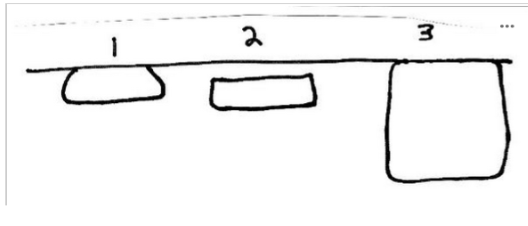
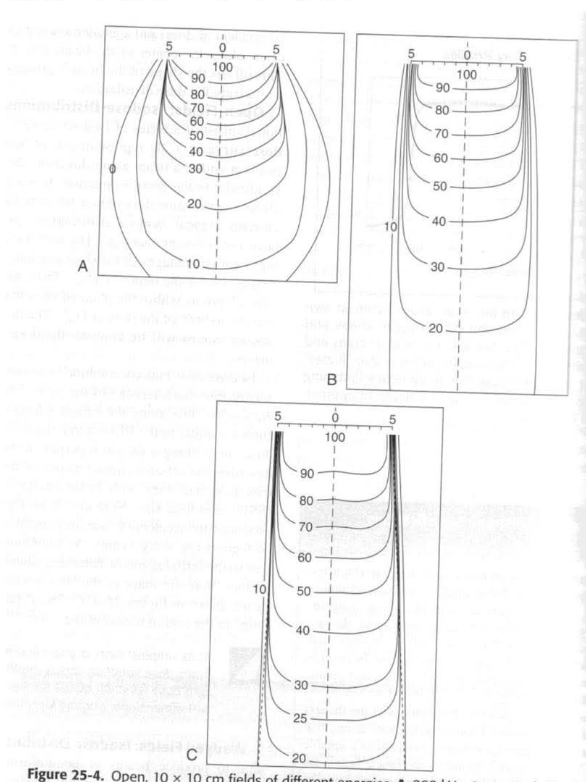
Which of the following electron beam isodose summations best illustrates the useful range of a 9 MeV beam?
A. 1
B. 2
C. 3
D. impossible to tell
B. 2
1 20 MeV
3 A KV beam
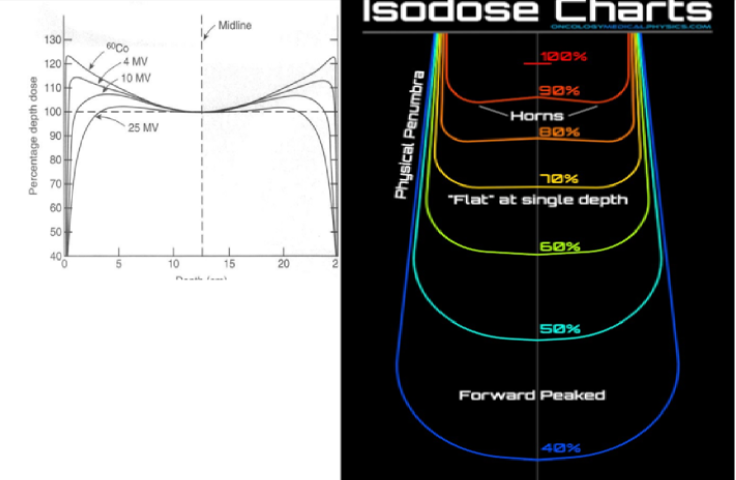
At a given depth in a Co60 field and 4MV linac, how is the average intensity of the photons near the field edge related to the intensity near the center of the field?
A. they are the same for Co60
B. average intensity is lower near the edge
C. average intensity is constant near the center
D. average intensity is higher near the edge
D. average intensity is higher near the edge
Feedback
energy is higher near central axis, but intensity/dose is a bit higher near the edge (e.g. horns
Horns: Areas of high dose near the surface in the periphery of the beam due the flattening filter, which is designed to overcompensate near the surface to get flat isodose curves at depth
Typically, 4 MV and lower have bigger horns- HINT: we dont need to worry about this much cuz nowadays lowest setting is 6MV
near the center of the beam:
the dose is lower cuz the flattening filter attenuates the xrays
the Avg. E is higher cuz the flattening filter hardens the beam
A compensating filter is used to completely compensate for the sloping skin surface of a treatment port. In order that calculations may be done with standard isodose curves, which of the following is correct?
A. the SSD should be set to the center of the field
B. the SSD should be set to the highest point on the patient
C. the SSD should be set to the lowest point on the patient
D. the SSD must be changed each day to move across the field
B. the SSD should be set to the highest point on the patient
feedback:
see #131 in practice test
You always set SSD to the closest surface point in the treatment field
Of the following statements concerning isodose curves, which is correct?---1. a specific set of curves should be obtained for each combination of treatment factors; 2. the curved lines connect all points receiving identical dosage; 3. they serve to ensure uniformity of irradiation and avoid under of over exposure
A. 1
B. 1,2
C. 1,2 and 3
D. 2,3
C. 1,2 and 3
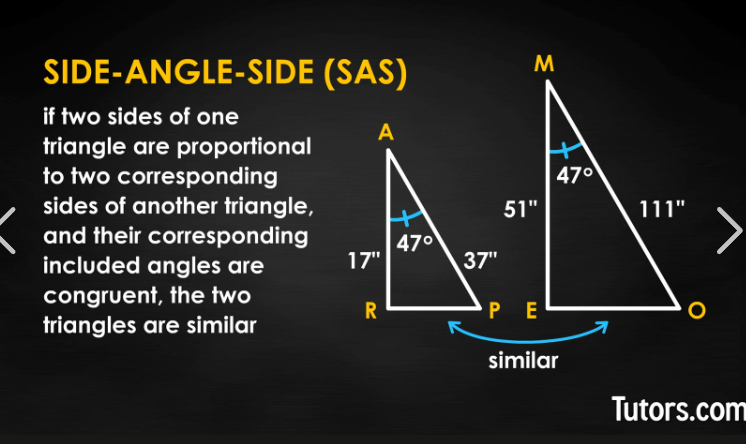
In similar triangles---1. the corresponding sides are directly proportional; 2. the corresponding angles are equal; 3. size is a constant
A. 1
B. 1,2
C. 1,2 and 3
D. 2,3
B. 1,2
Wedge filters designed for use in high voltage beams that are not custom made for each patient vary in angle from _______ degrees.
A. 15-60
B. 15-75
C. 30-60
D. 45-75
A. 15-60
Wedges:
15
30
45
60
In radiation therapy, ________ are used to determine exposure at various points to ensure uniformity of irradiation.
A. depth dose guides
B. isodose curves
C. treatment charts
D. technique guides
B. isodose curves
VARIOUS points
When more than two planes of sources are used, it would be called a:
A. Stereo implant
B. Single-plane implant
C. Orthogonal
D. Volume implant
D. Volume implant
Answer: D; this is the right answer, but this kind of brachytherapy question is no longer on the registry exam
0-1 cm single plane
1-2.5 cm
2.5- up cm volume inplant
Which type of radiation source will show the greatest amount of discontinuity at the edge of the beam on an isodose summation chart?
A. a 200 kv x-ray source
B. a Co60 source
C. a 22 MeV betatron source
D. discontinuity would be identical for these sources
A. a 200 kv x-ray source
Reasoning:
They are NOT asking about penumbra which is from 80%-20%,
“Discontinuity at the edge of the beam” when measuring dose distribution, where the intensity drops sharply rather than gradually.
A (200 kVp)
Very “distorted” isodose shapes
Bulging, uneven lines
Poor penetration + heavy scatter influence
👉 MOST irregular / least smooth transition
✔ This is what they mean by maximum discontinuity
Total exposure= in-air exposure rate x _____________.
A. exposure time
B. backscatter factor
C. entrance-R
D. HVL
A. exposure time
Feedback
This is like the principle of mAS= mA x time
The total energy absorbed from a beam of radiation by the patient is called the:
A. linear energy transfer
B. dose
C. integral dose
D. exposure
C. integral dose
Reasoning:
def. a measure of the Total Energy absorbed in the treated volume
Kgram/ Gray or simply Joule
Dose & Mass (i.e. tissue being irradiated)
Key words:
energy absorbed→ dose
TOTAL→ integral
Which of the following parameters would effect the shape of an isodose curve?---1. penumbra; 2. SSD; 3. energy of radiation
A. 1
B. 1,2
C. 2 and 3
D. 1,2,3
D. 1,2,3
Feedback
penumbra described in Khan yes; SSD affects PDD---which impacts shape; energy = like KV vs linac, where there is a big difference in iso curve shape
The shape of isodose curves/%DD curves are affected by the---1. quality of the radiation beam; 2. field size and shape; 3. source diameter
A. 1
B. 1,2
C. 1,2 and 3
D. 2,3
C. 1,2 and 3
Reasoning:
Energy and fs affect PDD
source diameter affects penumbra
The tissue air ratio is:
A. totally dependent on the distance from the source
B. independent from the source distance between 50 and 100 cm
C. defined in terms of a ratio of output to exposure
D. none of these
B. independent from the source distance between 50 and 100 cm
Reasoning;:
TAR, TPR, TMR, are independent of SSD/ distance (including from 50-100cm but it is independent of distance no matter the distance)
Which of the following substances have approximately the same density?
A. fat and water
B. muscle and water
C. bone and water
D. bone and muscle
B. muscle and water
muscle has more water than fat
The backscatter factor becomes negligible at a voltage range of:
A. 20-50 KV
B. 50-150 KV
C. 250-300 KV
D. above 1 MV
D. above 1 MV
reasoning: it matters for cobalt so…1.036
As the area of an irradiated field is increased, the backscatter radiation will ___________ the dose.
A. increase
B. decrease
C. maintain
D. have no effect on
A. increase
Reasoning:
bigger field size = bigger phantom scatter
The summation of absorbed doses in layers of tissue in the irradiated mass is known as the ________dose.
A. depth
B. skin
C. integral
D. total
C. integral
Integral dose is the total dose by the tissue
Checking, as the last step before the treatment plan is put into action, is aimed at---1. ensuring that the treatment volume is in fact the tumor-bearing volume; 2. ensuring the applicability of the plan to the treatment volume; 3. determining the most efficient treatment plan
A. 1
B. 1,2
C. 1,3
D. 2,3
B. 1,2
Reasoning:
Option #3 is done in the middle of treatment planning, before doctor approves, not as a last step (which occurs after the Dr. has approved).
Reasons for using wedge/compensating filters include---1. skin compensation; 2. to avoid hot spots; 3. to improve homogeneity
A. 1
B. 1,2
C. 1, 3
D. 2,3
C. 1, 3
Reasoning:
All are true BUT if you’re forced to choose 2 options only
duh
improving inhomogeneity also reduces hot spots
Factors that dictate the number of treatment fields include the---1. tumor depth; 2. beam quality; 3. age of the patient
A. 1
B. 1,2
C. 1,3
D. 2,3
B. 1,2
reasoning:
Age could be very elderly or infant ,so that is a possibility, but that is not routinely (commonly) a factor. Options 1 and 2 are routinely (commonly—which means “Best response”) correct. Tumor depth and beam energy that is available (quality) always are factors in field arrangement.
Factors that affect the %DD include the---1. depth of the lesion; 2. intensity of the beam; 3. area of the treatment port; 4. distance
A. 1,2
B. 1,3
C. 2,4
D. 1,2,3,4
B. 1,3
reasoning:
#2 is incorrect, so anything with number two can't be correct--which gives you teh answer right there, as only one D. oesn't contain #2 .So even though this doesnt' list ALL of teh factors that affect PDD, it is incomplete, but 1,3 is the most correct answer
FYI: area of tx port → ie field size
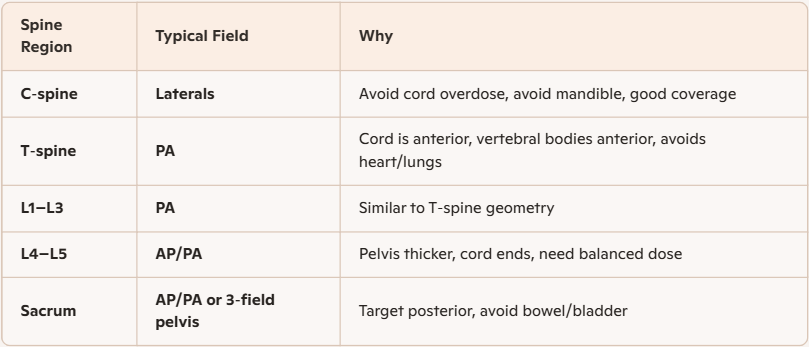
A spinal cord compression at the level of T5-T6 is being treated emergently. The most likely field arrangement would be:
A. Two parallel opposed lateral fields
B. Two parallel opposed AP/PA fields
C. A single posterior electron field
D. A single posterior low energy photon field
D. A single posterior low energy photon field
If two 45 degree wedges are positioned perpendicularly to each other, the resultant isodose curves form a :
A. rhombus
B. triangle
C. regular diamond
D. perfect rectangle
C. regular diamond
Which of the following terms is NOT related to dose distribution?
A. dose time
B. skin opposition
C. sublethal dose
D. erythema dose
B. skin opposition
Reasoning:
???
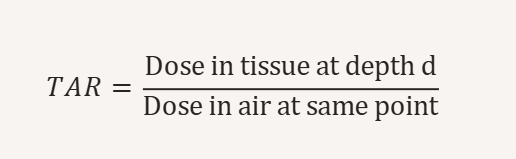
Tissue air ratios are based on:
A. depth dose data
B. treatment port size
C. scattering
D. surface doses
A. depth dose data
reasoning:
Old school way of looking at things
TAR was constructed from depth‑dose measurements, even though the reason TAR changes with depth is scatter.
General problems encountered in the planning of composite fields for radiation therapy include---1. body inhomogeneity; 2. curvature of the body surface; 3. loss of the skin sparing effect when a bolus is used
A. 1
B. 1,2
C. 1,2 and 3
D. 2,3
C. 1,2 and 3
reasoning:
"composite" fields means using more than 1 field, these issues matter with single fields but they compound with composite fields so its worse
body inhomogeneities (lung vs bone density chart)
Contour irregularities CFs
yeah
The area on the surface of a patient or phantom on which a radiation beam is incident is the:
A. treatment volume
B. entrance port
C. distributive radiation coefficient
D. field size
B. entrance port
Reasoning:
Field size is defined at isocenter
tx volume = amount that receives like 90% of the tumor dose /prescribed
The exit dose of a 6 MeV photon beam applied laterally to the neck of an adult can be as high as ____________ percent.
A. 10
B. 20
C. 40
D. 60
D. 60
Reasoning
given the depth of penetration of six mv. Also remember that MV is just short for MeV, meaning photon beam, not electrons
At just 12 cm 60 Co is 50% 6 MeV penetrates deeper so it has to be higher than 50%
The choice of angles for a wedge filter should produce a distribution of radiation that---1. resembles the tumor shape; 2. avoids excessive irradiation of critical areas; 3. focuses and directs the beam to the desired area
A. 1
B. 1,2
C. 1,2 and 3
D. 2,3
B. 1,2
reasoning:
wedges don't "focus" but beam like a cone or collimator, they are not a beam direction devices so anything with 3 in it is not correct
The entire right breast will be treated in your patient diagnosed with T1 N1 M0 infiltrating ductal carcinoma. The most likely field arrangement would be:
A. Tangential fields with subsequent tumor bed boost
B. Tangential fields with internal mammary and supraclavicular fields
C. Parallel opposed AP/PA fields with spinal cord blocked
D. Single field electron field to the entire breast with bolus
A. Tangential fields with subsequent tumor bed boost
When using a wedge filter, the wedge angle is defined as the angle which makes the:
A. 50% isodose curve perpendicular to the surface
B. 50% isodose curve parallel to the surface
C. 25% isodose curve parallel to the surface
D. none of these
B. 50% isodose curve parallel to the surface
The isodose lines at the periphery of an isodose curve are chiefly influenced by:
A. field shape
B. field size
C. penumbra
D. scatter
C. penumbra
Reasoning:
Penumbra = how quickly the dose drops from ~80% → 20% at the field border.
Penumbra → defines the edge sharpness ✅
When placed approximately 60 degrees from each other, two 60 degree wedges will create a ___________ volume.
A. box-like
B. triangular
C. spherical
D. rectangular
B. triangular
Wedge filters designed for high voltage beams are used in treatment of---1. prostatic carcinoma; 2. lymphoma; 3. breast carcinoma; 4. laryngeal carcinoma; 5. antral carcinoma
A. 1,2,3
B. 4,5
C. 2,3,4
D. 3,4,5
D. 3,4,5
Cancers that use wedges
Irregular surface,
#1 Breast
#2 H&N
Less common
GYN & Rectum pelvis (Not bladder or prostate cuz they are centered & symmetrical)
lung
extremities
2 opposing fields
A. midpoint dose
B. integral dose
C. modal dose
D. tumor dose
A. midpoint dose
The dose rate that can be expected at a certain point from a particular radiation machine is the:
A. output
B. dose distribution
C. absorbed dose rate
D. build-up
A. output
this is literally the definition of output
the others are doses in the patient
A crosstable radiograph is taken to determine the depth of the spinal cord. A 5 cm diameter ring on the patients skin measures 7 cm on the film. If the cord depth below the skin on the film measures 8 cm, what is the cord depth in the patient?
A. 5.7 cm
B. 8 cm
C. 11.2 cm
D. 6.2 cm
A. 5.7 cm
7/5 = 1.4 divided by 8 = 5.71 cm
A primary brain tumor located in the right temporal lobe will likely be treated with:
A. Two parallel opposed equally weighted photon beams
B. A wedged pair consisting of anterior and RPO fields
C. A wedged pair consisting of vertex and right later fields
D. Four field box technique with wedges on the lateral fields
C. A wedged pair consisting of vertex and right later fields
The SSD of a linear accelerator treatment is changed from 80 cm to 100 cm. Which of the following quantities would have to be changed?---1. given dose; 2. monitor setting; 3. collimator setting; 4. field size on skin
A. 1,2
B. 2,3
C. 1,2,3
D. 1,2,3,4
D. 1,2,3,4
Reasoning:
changing the SSD changes the PDD
the TMR or PDD depends on Depth, you use those to calculate MUs so yes
increasing the distance will make fs bigger, so yes
same reasoning, it will make the field size bigger so yes
137 A treatment field is 8 x 15 cm, the equivalent area of the field is:
A. 120 cm
B. 109 cm
C. 436 cm
D. 529 cm
A. 120 cm
Feedback:
LxW
The area of a square equals the:
A. square of the perimeter
B. square of one side
C. product of the four sides
D. sum of two sides
B. square of one side
Question 140
An x-ray tube operating at 200 kv and 10 ma gives an exposure rate of 30 R/min at 50 cm. If the ma is increased to 12.5, the new exposure rate is _________ R/min.
A. 32
B. 33.5
C. 37.5
D. 39
C. 37.5
Feedback
direct proportion 10/12.5 = 30/x
An entire space is treated by matching two fields both treated at 100 cm SSD. Field number 1 measures 8x20 and field number 2 measures 8x25. In order to match these fields at a depth of 5cm, a _________cm skin gap would be required.
A. 1.1 cm
B. 2.0 cm
C. 5.0 cm
D. 3.2 cm
A. 1.1 cm
reasoning: use gap calc
The area of a circle with a diameter of 4 cm is ______ cm.
A. 12.56
B. 15.76
C. 6.76
D. 125.66
A. 12.56
reasoning:
3.14 * r2
3.14 × 22
The length of a circle or a::
A. diameter
B. radius
C. circumference
D. Pi
C. circumference
A strait line through the center to two opposite points on a circle:
A. diameter
B. radius
C. circumference
D. Pi
A. diameter
A parallel pair of treatment fields is used for radiation therapy. The separation between the fields (field thickness/depth) is 20 cm. If each field measures 10 x 15 cm, then the total volume irradiated is ________ cc.
A. 150
B. 1500
C. 3000
D. 9000
C. 3000
Feedback
to calculate volume: LxWxHeight (aka depth) ; 10x15x20 = 3000
lateral tissue damage (LTD)
vs
tissue lateral effect (TLE)
lateral tissue damage (edge effect): with parallel opposed beams, there is a greater normal tissue biologic damage when treating with one field (or one set of fields) per day
Tissue lateral effect: For parallel opposed beams, lower energy MV beams, less than or equal to,4 MV create hot spots in the subcutaneous tissue if the patient separation is greater than 20 cm (cuz of horns)
E for Fat-E
D for Different Day