Myopia and Anisometropia - Diagnosis and Management of Common Ocular Conditions Spring 2026
1/64
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
65 Terms
Why may PRA be reduced in an uncorrected myope?
They have been lazy recently and not accommodating fully. When full RX is placed in front of them, they will not like to fully accommodate.
Can accommodation be reduced because of disease?
Yes
After correction, accommodation will usually return to normal within ____ wks
1-2
In a myopic patient, the phoria will be less (eso/exo) when corrected vs uncorrected
Less exo when corrected with (-) lenses
Do we want an uncorrected myope to be ORTHO at near?
No -- we may drive them into ESO posture once corrected at near
An ORTHO posture in an uncorrected myope will be highly suggestive of what?
convergence excess
Does correcting myopia alter accommodation at distance?
No
Does correcting myopia alter accommodation at near? Increase or decrease?
yes -- it will INCREASE the accommodative demand at near
Do we want to overminus our myopic patients? Why?
No - this will increase accommodative demand at distance and near
What is a situation in which we MAY consider overminusing a patient?
to treat significant BV issue -- exotropia in the presence of a high AC/A (divergence excess)
Should myopes wear their RX full time once they get it? Why is this important?
Yes -- wear full time in order to get used to accommodating fully again
Should myopes remove their glasses for near during the initial adaptation period?
No
What is a possible plan for myopes that is not offered for hyperopes?
myopia management
You can consider a _______ for near vision in a myope if BV conditions are present (ESO)
near add/remove the RX for near
Over Minus Patients Key Features
Will a patient who is over-minused have blurry vision?
No -- distance and near vision will be clear
Over Minus Patients Key Features
What are the key complaints of a patient who is over-minused?
HA & asthenopia d/t fatigue of accommodation, esophoria, or no symptoms at all
Over Minus Patients Key Features
Blur on (BI/BO) vergences at distances
BI
**There is accommodation to drop at distance when there is usually not any accommodation present. Increase divergence ability
Over Minus Patients Key Features
NRA ??
> +2.75
**they have more accommodation to drop
Over Minus Patients Exam Findings
Common findings of hyperbole myopes during exam?
Ret, monocular subjective, and final RX may be variable (like a hyperope)
Over Minus Patients Exam
What are some useful tools during the examination of a patient who you suspect is over-minused?
-red/green & then going to the 1st green response
-push plus by bluring 20/20 to unreadable and then wait to see if the letters will clear
Only give the LEAST MINUS RX to an over-minused patient if there are ______
symptoms
Do patients like increase of contrast with more minus?
Yes -- you should discuss this loss of contrast with patients
Should you trial frame a patient who you are prescribing LESS minus to?
Yes -- for acceptance
Should you consider SLOWLY DECREASING MINUS over time in a patient who has been over-minused?
yes
Should you ever criticize other clinicians if a patient comes in who is over-minused?
No -- there may be a reason for this
26 YO patient comes in for 1st eye exam. Notes distance blur
DVA: 20/60 OD/OS
NVA: 20/20 OU
D CT sRx: 2EP; N CT sRx: Ortho
MR: -1.00 OU
AC/A: 8 pd/D
How much does this patient accommodate at 40 cm without correction?
-1.00D underminused
-+1.50 accommodative demand at near
26 YO patient comes in for 1st eye exam. Notes distance blur
DVA: 20/60 OD/OS
NVA: 20/20 OU
D CT sRx: 2EP; N CT sRx: Ortho
MR: -1.00 OU
AC/A: 8 pd/D
How much does this patient accommodate at 40 cm with MR correction?
-emmetrope
-+2.50 accommodative demand at near
26 YO patient comes in for 1st eye exam. Notes distance blur
DVA: 20/60 OD/OS
NVA: 20/20 OU
D CT sRx: 2EP; N CT sRx: Ortho
MR: -1.00 OU
AC/A: 8 pd/D
What is the predicted near phoria through the MR?
-Near: 8EP
26 YO patient comes in for 1st eye exam. Notes distance blur
DVA: 20/60 OD/OS
NVA: 20/20 OU
D CT sRx: 2EP; N CT sRx: Ortho
MR: -1.00 OU
AC/A: 8 pd/D
This patient likely has ________
convergence excess
26 YO patient comes in for 1st eye exam. Notes distance blur
DVA: 20/60 OD/OS
NVA: 20/20 OU
D CT sRx: 2EP; N CT sRx: Ortho
MR: -1.00 OU
AC/A: 8 pd/D
Is the built in add d/t being undercorrected actually helping the patient from having near symptoms?
Yes
26 YO patient comes in for 1st eye exam. Notes distance blur
DVA: 20/60 OD/OS
NVA: 20/20 OU
D CT sRx: 2EP; N CT sRx: Ortho
MR: -1.00 OU
AC/A: 8 pd/D
What would you prescribe for this patient?
--1.00 OU w/ +1.00 ADD OR
-1.00 for distance only & then take off the glasses for near work
26 YO patient comes in for 1st eye exam. Notes distance blur
DVA: 20/60 OD/OS
NVA: 20/20 OU
D CT sRx: ORTHO; N CT sRx: 8XP
MR: -1.00 OU
AC/A: 4 pd/D
What is the predicted phobia through the RX?
4XP
26 YO patient comes in for 1st eye exam. Notes distance blur
DVA: 20/60 OD/OS
NVA: 20/20 OU
D CT sRx: ORTHO; N CT sRx: 8XP
MR: -1.00 OU
AC/A: 4 pd/D
What would you prescribe for this patient?
-1.00 OU for full time wear
26 YO patient. No complaints
DVA: 20/20 OD/OS
NVA: 20/20 OU
D CT sRx: 2 ESO; N CT sRx: 2 ESO
MR: -4.75 OU
Lensometry: -5.50
How much is the patient accommodating at near in the current RX?
-Patient is overminused by -0.75
-Patient is accommodating +3.25D at near
26 YO patient. No complaints
DVA: 20/20 OD/OS
NVA: 20/20 OU
D CT sRx: 2 ESO; N CT sRx: 2 ESO
MR: -4.75 OU
Lensometry: -5.50
How much is the patient accommodating at near in the MR?
+2.50 (emmetrope)
26 YO patient. No complaints
DVA: 20/20 OD/OS
NVA: 20/20 OU
D CT sRx: 2 ESO; N CT sRx: 2 ESO
MR: -4.75 OU
Lensometry: -5.50
How much is the patient accommodating at distance in the current RX?
Currently accommodating +0.75 at distance
26 YO patient. No complaints
DVA: 20/20 OD/OS
NVA: 20/20 OU
D CT sRx: 2 ESO; N CT sRx: 2 ESO
MR: -4.75 OU
Lensometry: -5.50
How much is the patient accommodating at distance in the MR?
0
26 YO patient. No complaints
DVA: 20/20 OD/OS
NVA: 20/20 OU
D CT sRx: 2 ESO; N CT sRx: 2 ESO
MR: -4.75 OU
Lensometry: -5.50
What will happen to the phoria in this patient when we RX the MR?
Less Eso, more EXO posture at both distance and near
26 YO patient. No complaints
DVA: 20/20 OD/OS
NVA: 20/20 OU
D CT sRx: 2 ESO; N CT sRx: 2 ESO
MR: -4.75 OU
Lensometry: -5.50
What would you prescribe for this patient?
-5.00 or -5.25 OU for full time wear
What is anisometropia?
different amounts of refractive error between the eyes
What is clinically significant anisometropia?
1.00D of SE difference
Is anisometropia of >1.00D an amblyogenic risk factor in hyperopic kids/adults?
yes
If there is uncorrected anisometropia present, can a patient be asymptomatic?
Yes
What are the possible symptoms of uncorrected anisometropia?
HA, strain, blur, poor depth perception
What are the effects of corrected anisometropia, esp in glasses?
issues with prismatic effects when looking away from the optical center
What is refractive aniseikonia?
-equal axial lengths
-image sizes are different
What is Prentice's Rule?
Prismatic Effect = d*P
d = distance from the optical center in cm
P = power of the lens
What is the predicted phoria through 5PD of BO prism in an ORTHO patient?
5PD exophoria
**the eye will follow the image IN and swing IN. Seeing an eye move in looks like an EXO deviation
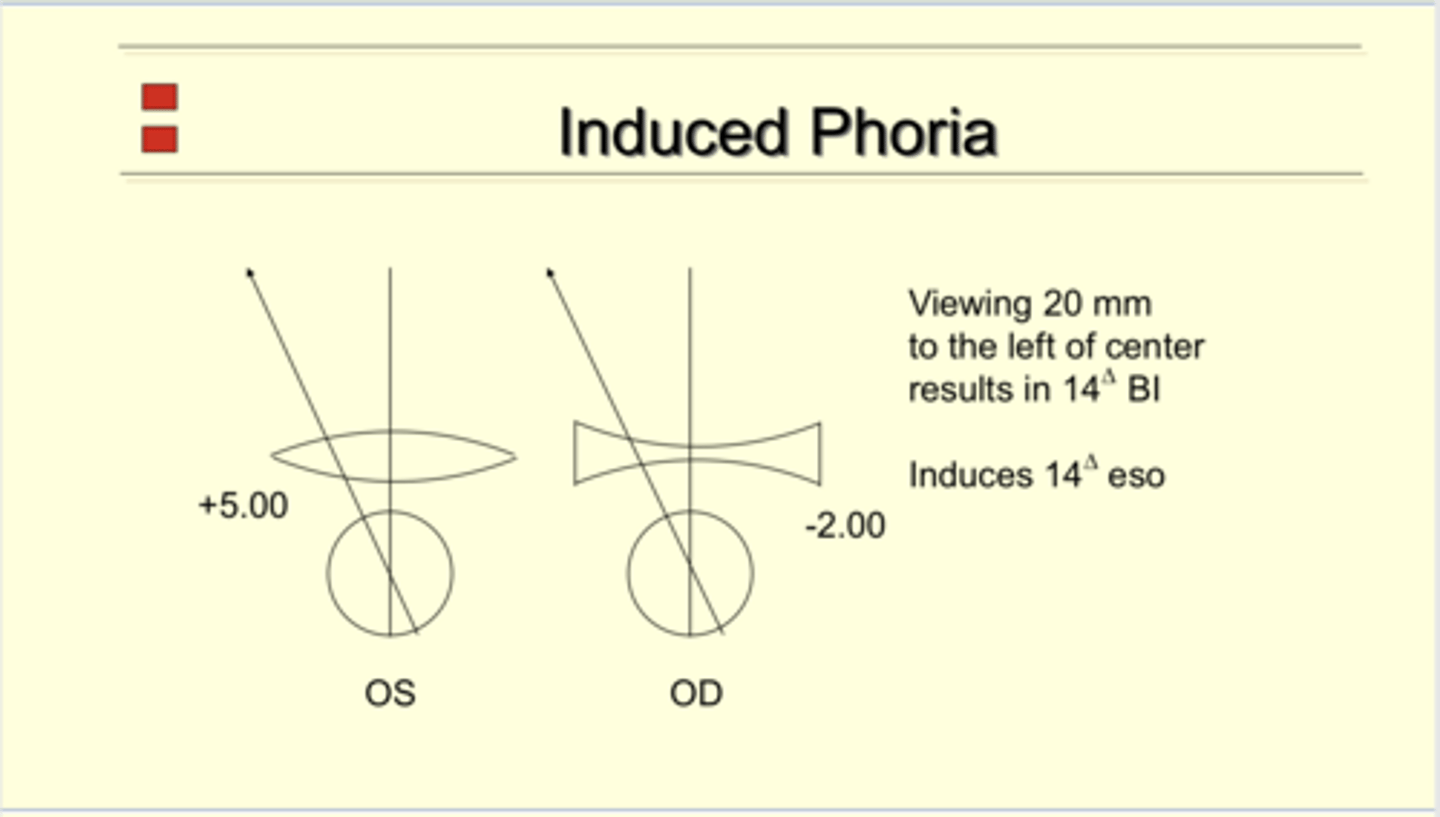
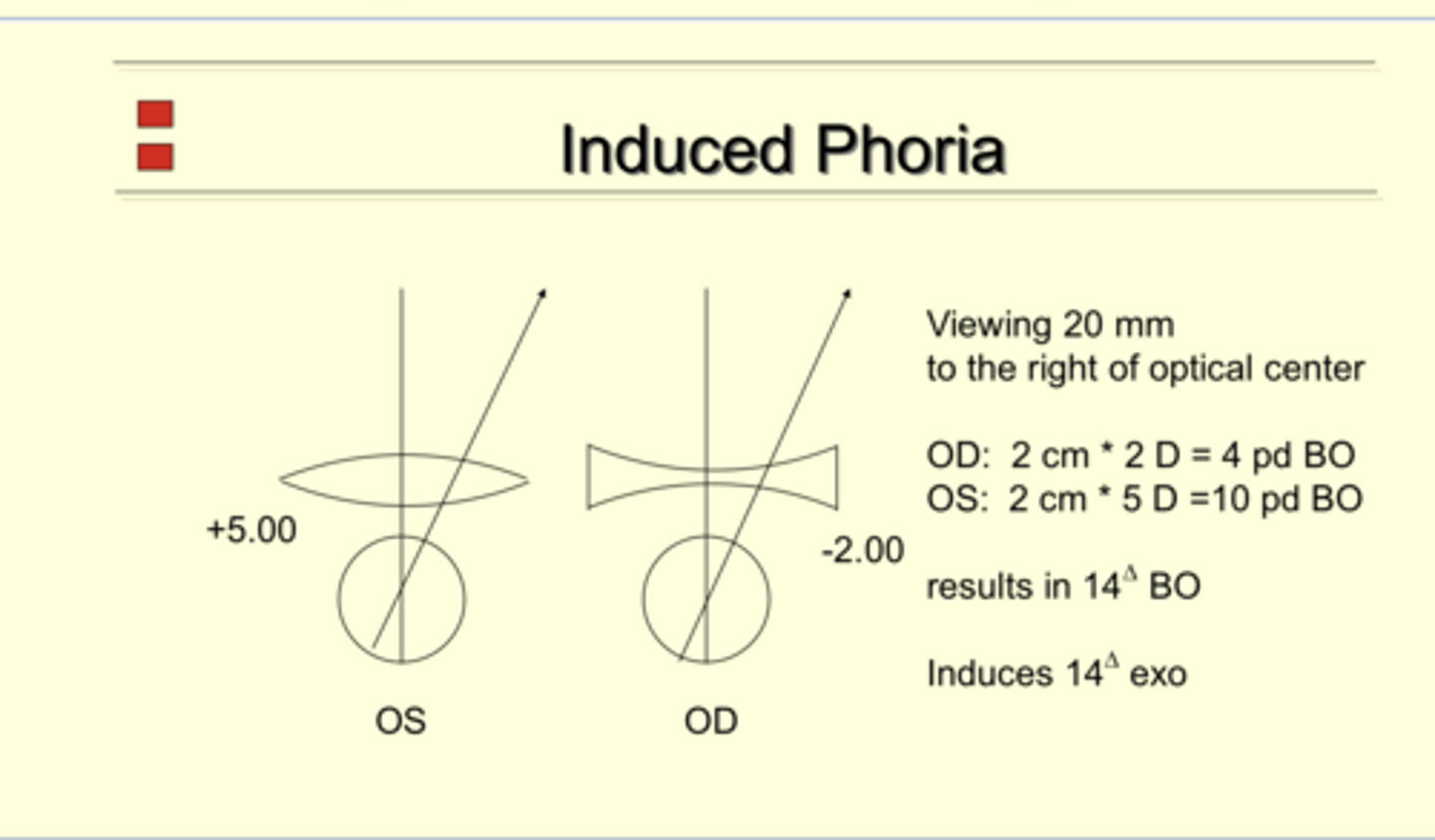
OD: -2.00
OS: +5.00
A patient is viewing 20mm to the right of optical center. What is the induced phoria of each eye?
-Prentice Rule: Prismatic Effect = dP
-OD: 2*2 = 4 BO
-OS: 2*5 = 10 BO
-OU Prismatic Effect= 14BO
-Induced Phoria = 14 exo
OD: -2.00
OS: +5.00
A patient is viewing 20mm to the left of optical center. What is the induced phoria of each eye?
-Prentice Rule: Prismatic Effect = dP
-OD: 2*2 = 4 BI
-OS: 2*5 = 10 BI
-OU Prismatic Effect= 14BI
-Induced Phoria = 14 eso
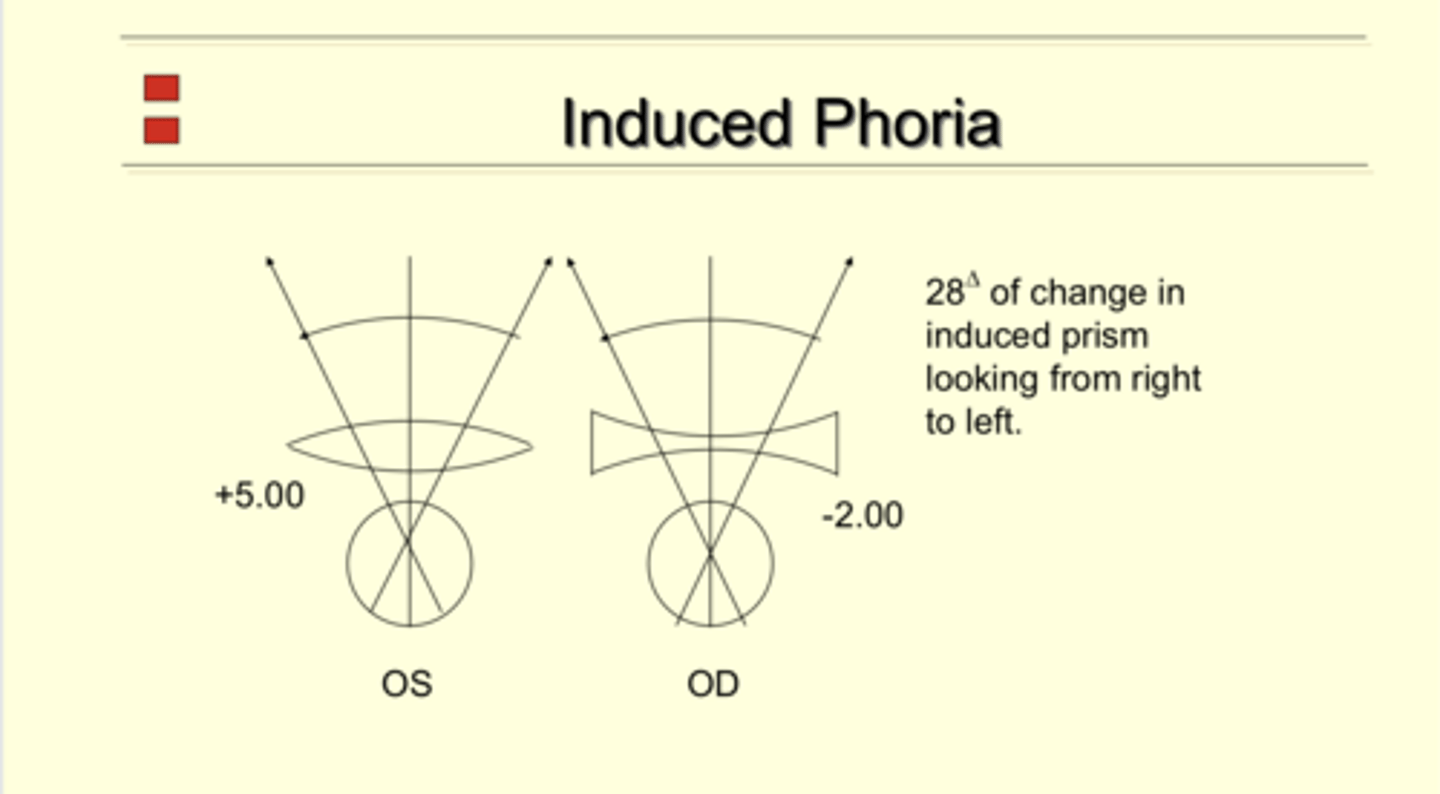
OD: -2.00
OS: +5.00
A patient is viewing 20mm from the right to the left of optical center. What is the change in phoria ?
Δ28 of change
Correcting refractive anisometropia with glasses will cause _____ difference between the eyes
image size
More (plus/minus) eye will have a larger image size
plus
Will anisometropia cause symptoms in some patients who experience different image sizes?
yes
What is the BEST correction option for patients with anisometropia?
CLs
WHY are CLs the best treatment option for patient's with anisometropia?
-no induced prism
-may eliminate aniseikonia
Are backup glasses still needed for patients with anisometropia?
Yes
Will all patients with anisometropia be interested in Cls?
No
If the patient insists on having glasses for full time wear with anisometropia, what should our treatment plan be?
-Demo the RX
-Counsel patient on how to use glasses & be a head pointer... NOT an eye mover
-Avoid the periphery of the glasses to eliminate unwanted prismatic effects
If the patient STILL does not accept their RX with anisometropia & have anisokonia... what can we do?
-Eikonic lens design
-Cut amount of anisometropia corrected
Can we cut the amount of anisometropia in a child RX?
No -- we want they to develop good VA in each eye
How to cut amount of anisometropia in an adult RX?
decrease plus or minus in the higher powered eye & then DEMO to determine how much needs cut off
For a bifocal design in a patient with anisometropia, what may we consider?
Slab off to get more BU in front of the more minus eye to get around the prismatic effects that happens when the patient needs to go into downgaze to get into their bifocals
ADULT PATIENT
MR OD: +6.00; OS: +1.00
You determine that you want to cut the aniso that is prescribed by 2.00D. What should you RX?
You should prescribe +4.00 OD; +1.00 OS
ADULT PATIENT
MR OD: -6.00; OS: -1.00
You determine that you want to cut the aniso that is prescribed by 2.00D. What should you RX?
You should prescribe -4.00 OD; -1.00 OS