lab test
1/167
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
168 Terms
non dysjunction
Non disjunction = inability of a pair of homologous chromosome to separate properly
single nucleotide polymorphosim
Single nucleotide substitution of one nucleotide for another (point mutation)
isochromosome
1 long (q) and 2 short arms (p)
non dysjunction examples
XXY = klinfelters = TRISOMY eg: micropthalmia/small eyes
XO. = turners MONOMSOMY eg: myopia/hyperopia/ptosis(droops)
XXX = metafemale syndrome
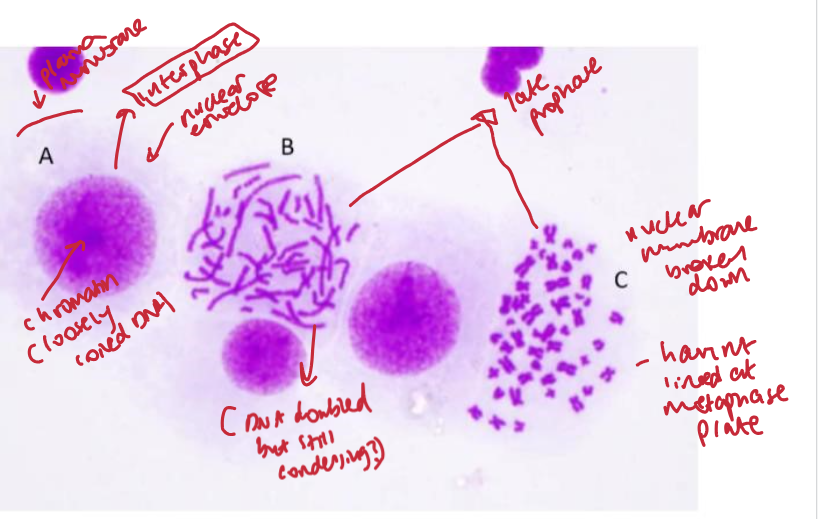
chromosome stucture
2 sister chromatids joined by centromere
one long (q) and one short arm (p)
longer q arm than p arm
DNA supercoiled into double helix around histone proteins from a nucleosome
what stage of mitosis needs arresting to see chromosomes
metaphase
stain to visualise chromsomes
stain with giemsa
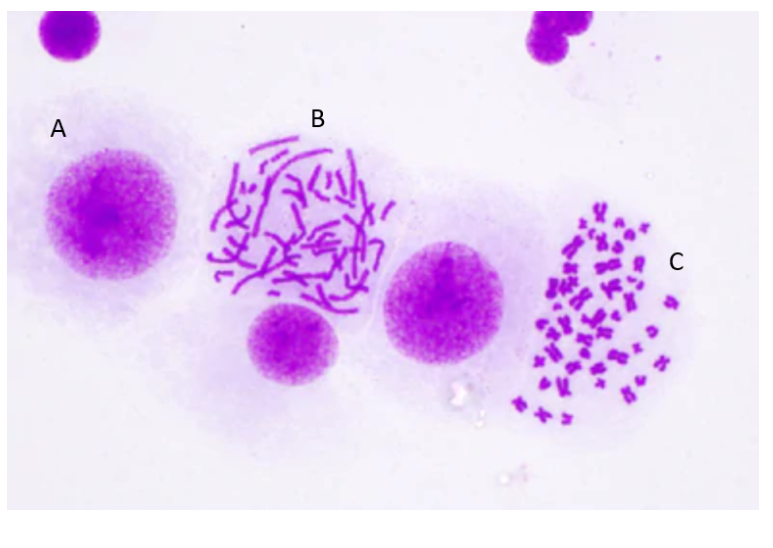
what stages of mitosis are these?
axons vs dendrites
dendrites = point at which info enters neurons from nerve cells/environment
axons = elecrical signals leave cell body
ending in terminal arborizations
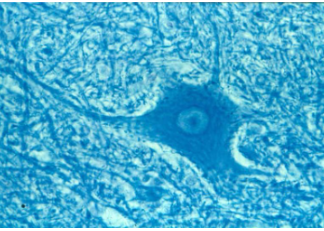
identify the stucture and its features
ventrol horn of spinal cord
stringy bits = neurites (axons/dendrites)
what makes up grey matter vs white matter of CNS
grey = cell bodies, glial cells, dendrites + soma of CNS neurones
axons have little myelination
white = myelinated axons of neurones - few soma
what cells myelinate PNS vs CNS and the differences between the way they myelinate
PNS = schwann cells
CNS = oligodendrocytes
oligodendrocytes create myelin for multiple axons but one schwann cell per axon
what glia maintains blood brain barrier
astrocytes
function of microglia
specialised macrophages maintaining homeostasis via repair
structure of nerves (+ neurones vs nerves )
nerves = collections of neurones
neurones surrounded by endoneurium
many neurones = fasicle wrapped in perineurium
many fasicles = wrapped in epineurium
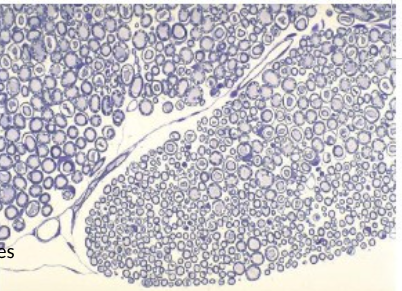
identify the image and its stuctures
cross section of a nerve
axons = pale cicles
myelin sheath = purple ring (thicker if more myelinated)
darker purple cell bodies = schwann cell nuclei producing myelin
range of nerve cell axon diameters and function
1 to 15-20 micrometres
Large diamerer = faster conduction eg motor neurones
Smaller = conduct slower eg: pain
average size of cheek epithelial cell
50 -100 micrometres
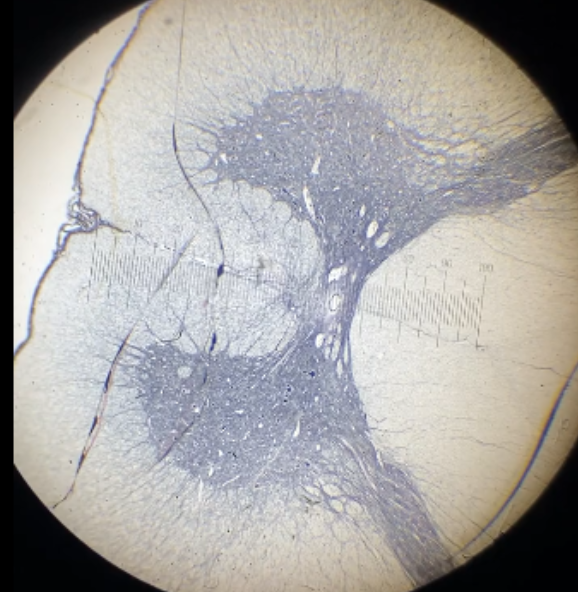
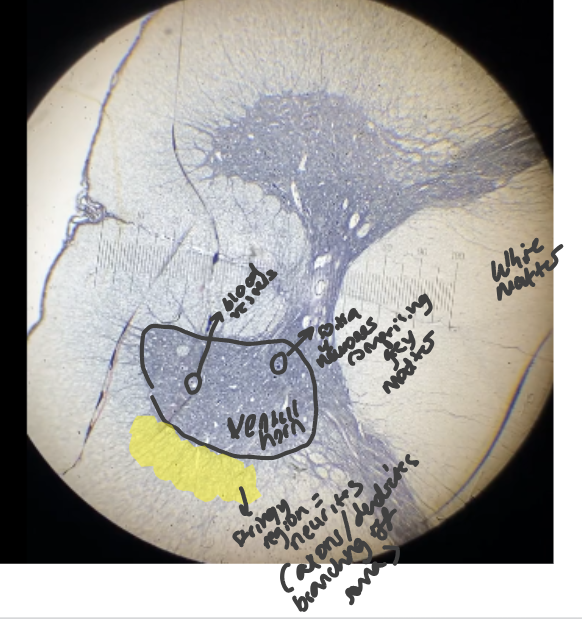
identify structure and its features
large horn = ventral horn
circles = blood vessels
stringy region = neurites
white matter = myelinated axons
dots = soma of neurones comprising of grey matter
what type of neurones make up grey matter of CNS
multipolar neurones = single axon and multiple dendrites
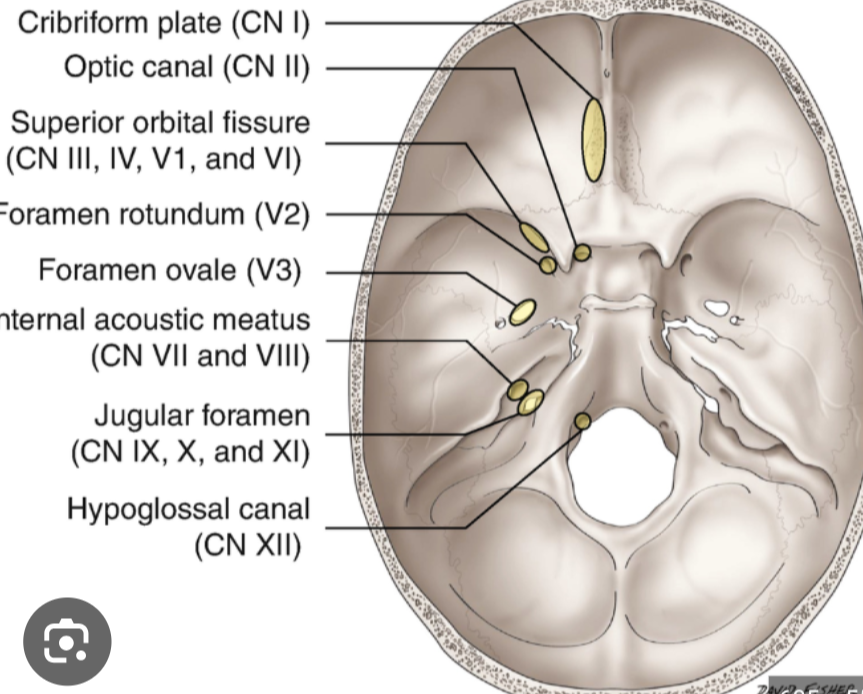
olfactory nerve - role, foramen, damage caused , test
controls sensory sense of smell
via olfactory receptors in nasal mucosa which attach to axons in olfactory filaments
passing through cribriform plate (perforated region) of ethmoid bone to (destination) olfactory bulbs of brain
(found in anterior fossa - opposite side to big hole of skull)
Damage to axons by head injury = cannot regenerate so permanent loss of smell = anosmia
Test = pungent odour
optic nerve 2 - role, foramen, damage caused , test
sensory control of vision
made up of retina ganglion cell axons in retina
optic nerve passes into skull via foramen of optic canal (perfect hole) at back of the orbit
nerve continues to optic chiasm where nerve fibres cross over and continue as the optic tract (opposite side)
to lateral geniculate nucleus of the thalamus
LGN axons pass through to area of brain responsible for conscious visual perception
Pituitary tumour compresses tissue above it
Pressure on axons of optic chiasm at midline so carry info of nasal retina so temporal vision loss = bi temporal hemi anopsia
Test = visual fields
field defect arising from midline compression of optic chiasm
loss of temporal vision = bitemporal hemianopsia
caused by pituitary tumour
direct vs consensual light reflexes
direct = constriction of pupil recieving light
consensual = simultaneous constriction of opposite pupil
oculomotor, trochlear, abducent nerve role, foramen, damage caused , test
control movement of the eye – innervate EOM
Lr6So4R3
Lateral rectus by abducent (6)
Superior oblique by trochlear (4)
Rest = oculomotor (3)
all 3 nerves originate from specific motor nuclei and travel through superior orbital fissure in the back of orbit
supplies specific EOM
Test – ocular motility test – look for symmetry
characteristics of oculomotor nerve palsies
oculomotor innervates LPS so causes ptosis (droppy eyelid) as LPS cant contract to open lid
only SO and LR working as 3rd nerve controls rest
LR over exerts = pulling eye out = exotropia
iris sphincter innervated by 3rd nerve = paralysed so dilated pupil = mydriasis
characteristics of abducent nerve palsies
esotropia = LR cant contract so cant oppose medial rectus so eye pulled inwards
trigeminal nerve -role, foramen, damage caused , test
Trigeminal:
Opthalmic = eyes/cornea (superior orbital fissure)
maxillary = cheekbone (foramen rotundum)
mandibular = bottom jaw branches (foramen ovale)
mainly sensory and some motor nerves
controls somatic sensory feelings (touch/pain/pressure) for face and head
and controls muscles for mastication/chewing (mandibular)
where in the eye are the most sensory receptors
fovea
facial nerve - role, foramen, damage caused , test
Facial:
internal acoustic meatus foramen + stylomastoid foramen?
located in posterior fossa
Innervates Orbicularis oculi
Lacrimal gland and salivary gland controlled by facial nerve
in petrous portion of temporal bone
(2 lines on edge of hole)
zygomatic branch of Facial nerve enters by internal acoustic meatus in petrous temporal bone and exits by stylomastoid foramen to reach obicularis oculi
Damage = lower lid drooping, dry eye, dry mouth = bells palsy
vestibulocochlear nerve - role, foramen, damage caused , test
sensory - posture + hearing
cochlear nerve carries auditory info
vestibular nerve - carries info about the position/movement of head
foramen = internal auditory meatus
located in posterior fossa
Test = tuning fork behind ear on skull – can hear so problem with outer ear
If cant hear = cochlea or vestibulo cochlear nerve damage
otolithic organs vs semicircular canals for vestibulococlear system
Semicircular Canals (aVOR): Detect rotational (angular) acceleration in three-dimensional space.
Otolith Organs (lVOR): Detect linear acceleration (translational motion) and gravity (tilt)
glossopharyngeal nerve - role, foramen, damage caused , test
Glossopharyngeal:
sensory, motor, autonomic nerves
motor:
nerve from nucleus ambiguous to stylopharyngeal muscles elevating larynx to swallow
sensory:
transmit somatic sensation from pharynx + posterior 1/3 tongue + taste buds to brain
parasympathetic:
otic ganglion supplies the parotid salivary gland
foramen = jugular foramen
vagus nerve -role, foramen, damage caused , test
Vagus:
role:
sensory pathway for feelings from the throat, heart, and gut
motor nerve for swallowing and speech
as parasympathetic system, regulating involuntary functions such as heart rate -“rest and digest”
foramen = jugular foramen
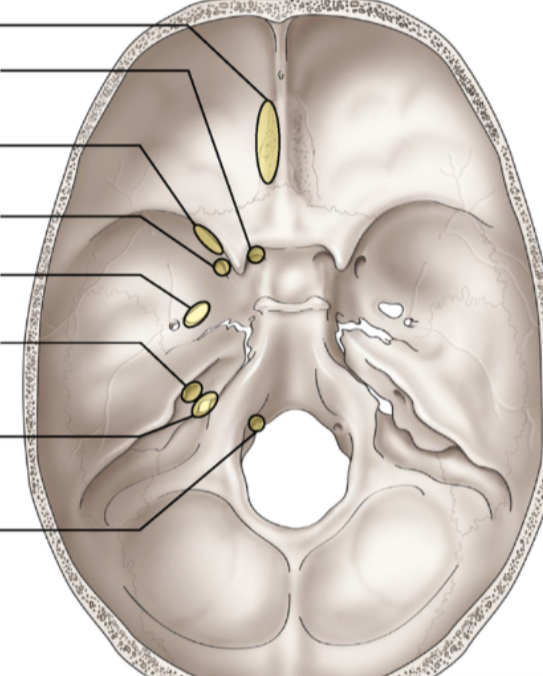
location of cranial nerve foramen

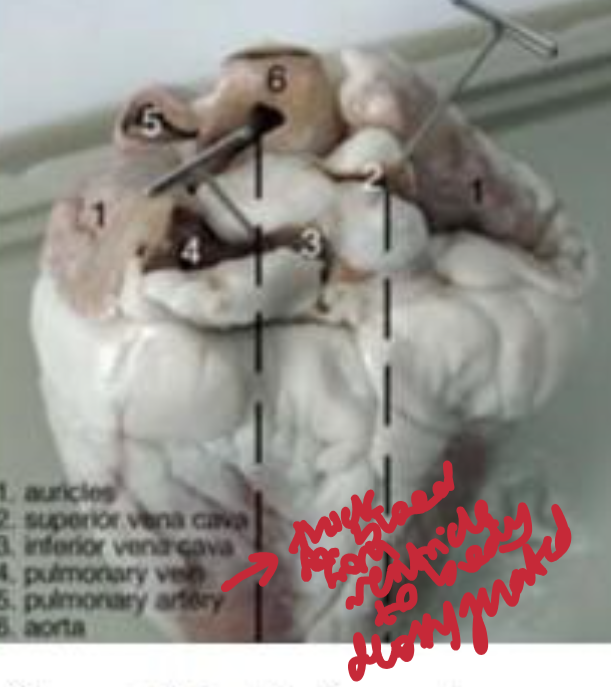
pathway of blood and labels of heart
Deoxygenated blood enters the right atrium via the vena cava, passes to the right ventricle, and is pumped to the lungs via the pulmonary artery. Oxygenated blood returns via the pulmonary veins to the left atrium, moves to the left ventricle, and is pumped to the body through the aorta
3 differences between skeletal and cardiac muscles
cardiac = autonomic but skeletal = somatic/vountary
cardiac = branched + connected by intercollated discs with gap junctions (syncytium) but skeletal = long unbranched
cardiac = myogenic but skeletal = neurogenic
agglutinogens
antigens expressed on erythrocytes determining blood group
blood types and their agglutinogens
type A = blood has agglutinogens binding to antigen B (attack foreign B antigens)
type B = blood has agglutinogens binding to antigen A
type AB = no agglutinogens against A/B so no immune response
type O = have agglutinogen A and B
process of agglutination
plateletes + WBCs (Antibodies bind to B antigen) = cross linked complex activating specific proteins iin plasma membrane causing erythrocytes to rupture leaking haemoglobin into blood plasma = haemolysis = kidney damage
what is serum of the blood
plasma without any clotting proteins containing antibodies
what blood type is a universal donor vs universal recipient
O = universal donor - lacking AB antigens
AB = universal recipient - lacks antibodies to AB so recieved blood from any type
codominance
when more than one allele is expressed in the same phenotype
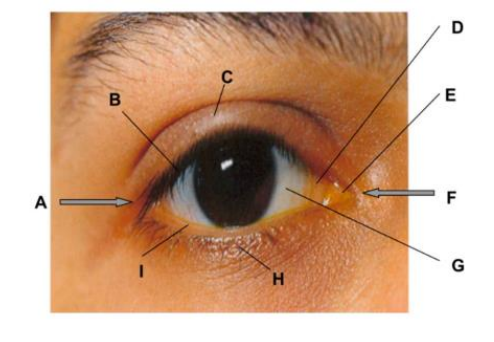
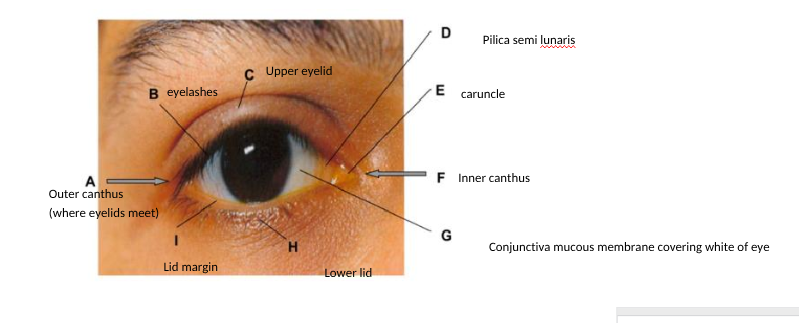
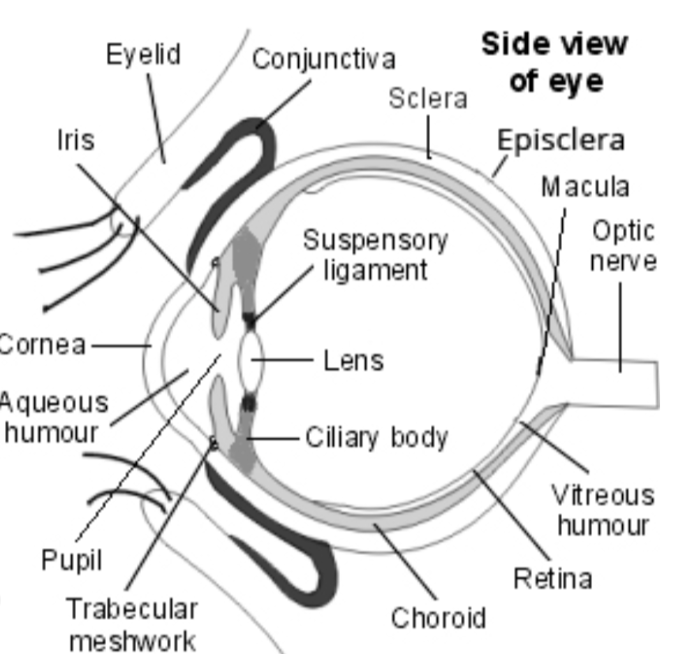
label the outer eye and lid
role of obicularis oculi and cranial nerve innervating it
zygomatic branch of facial nerve innervates sphincter muscle for eyelid closing
role of levator palpebrae superioris
elevates upper lid in blinking
maintains open palpebral aperture
levator originates from lesser wing of sphenoid at apex of orbit
runs over superior rectus and terminates as a broad aponeurosis tendon
levator inserts into the tarsal plate into the skin of the eyelid
innervated by oculomotor nerve
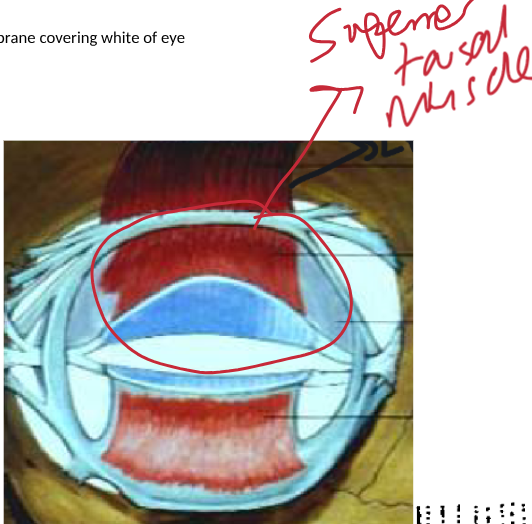
location of the superior tarsal muscle + function
arises from underside of levator and inserts into tarsal plate
smooth muscle with a secondary role in maintaining open palpebral aperture
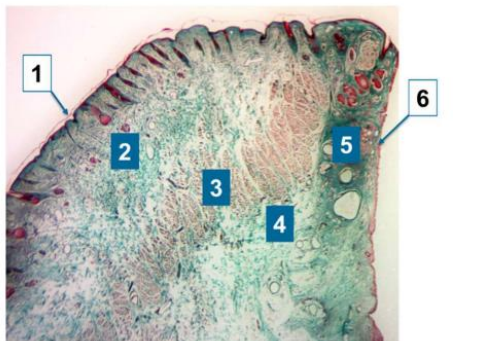
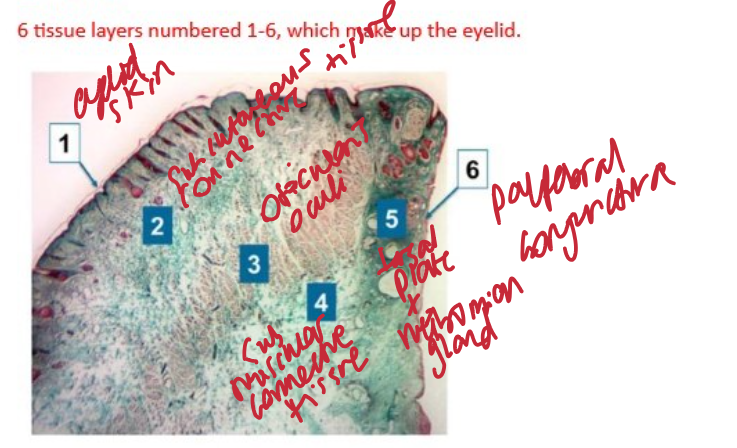
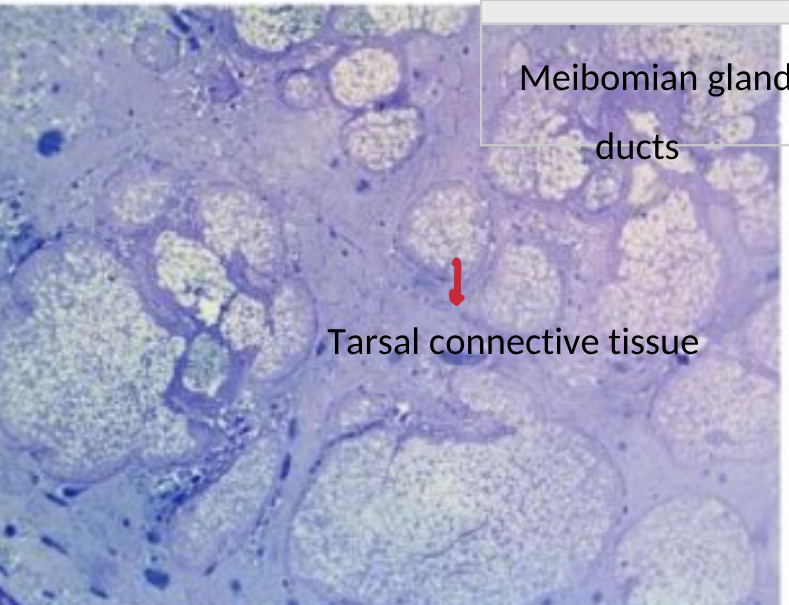
identify the 6 tissue layers of microscopic structure of lower eyeld
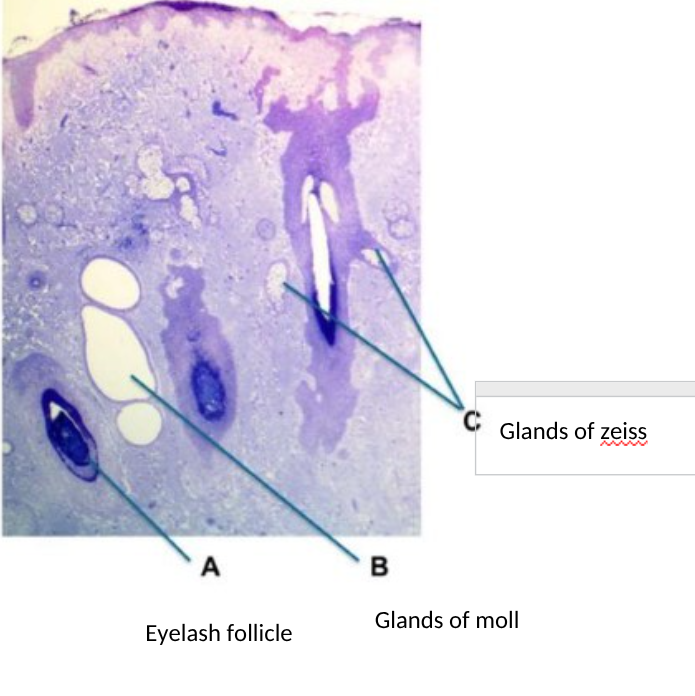
3 principle glands of eyelids + role
meibomian gland (Produces outer lipid layer of tear film preventing ocular surface from drying out)
glands of zeiss (ciliary sebaceous glands lubricating lashes preventing drying)
glands of moll ( ciliary sweat glands =antimicrobial secreting imminuglobulins for ocular surfaces defence )
identify the meibomian flands of eyelid
in dense connective tissue in tarsal plates in upper eyelid
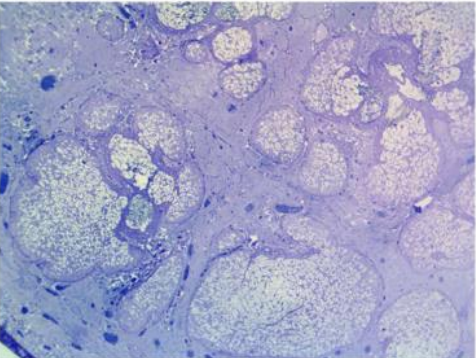
mode of secretion of meibomian glands and identify the stuctures on a microscopic section
Sebaceous glands consisting of multiple secretory acini which open onto a central duct
Discharges contents onto lid margin
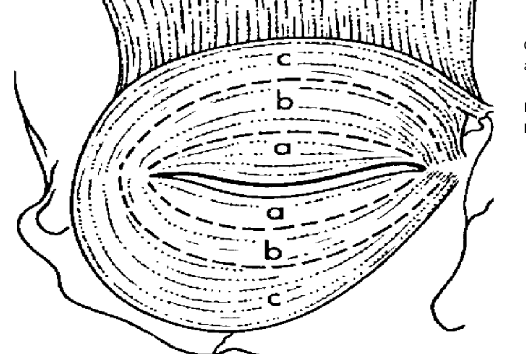
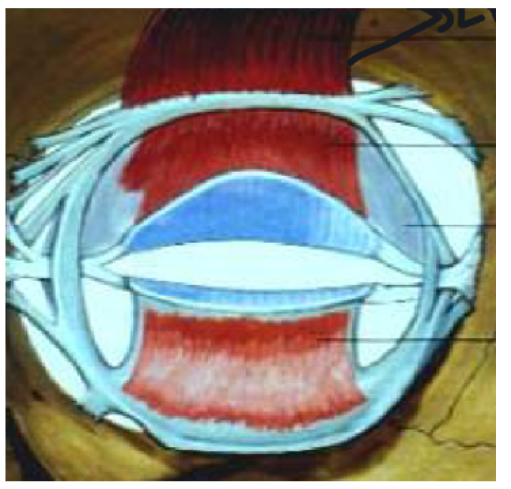
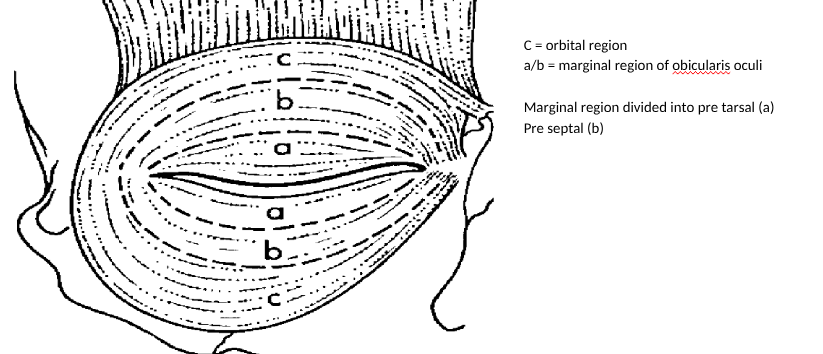
identify the orbital vs palpebral regions of obicularis oculi
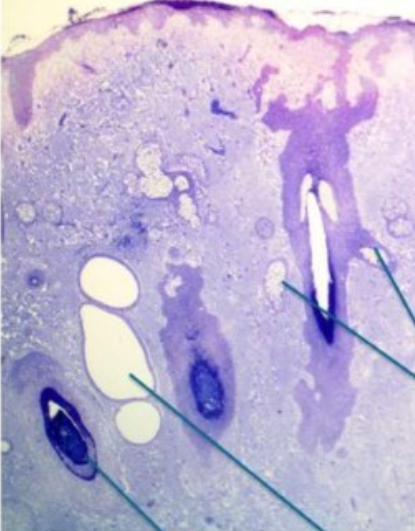
identify gland of zeiss and moll and eyelash follicle on a microscopic image
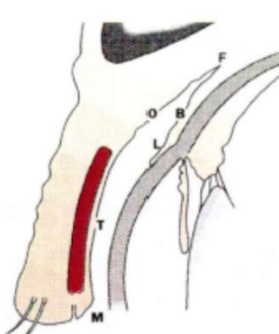
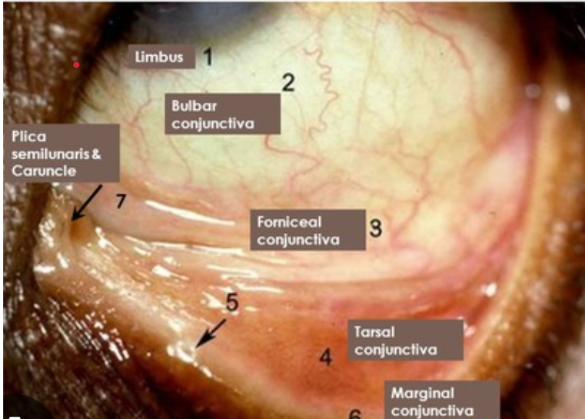
identify the 5 regions of the conjunctiva microscopically
orbital
limbal
bulbar
tarsal
marginal
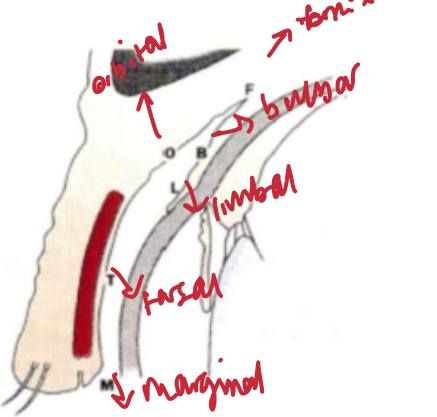
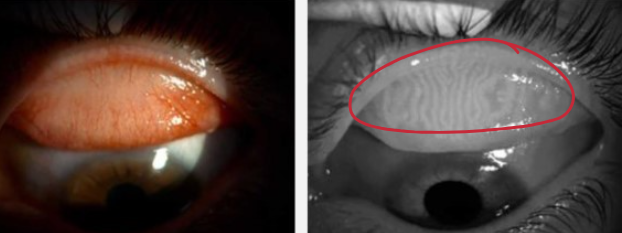
identify the 5 regions of the conjunctiva on the eye
stucture of a goblet cell and function
triangular nucleus due to secretory granules in cytoplasm containing mucin
produce mucousal component of tear film
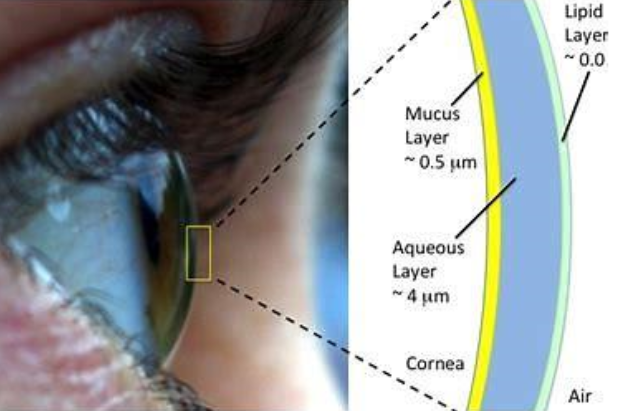
3 layers of tear film and gland responsible
lipid layer outer = meibomian
aqueous layer = lacrimal gland
mucus layer inner = goblet cells
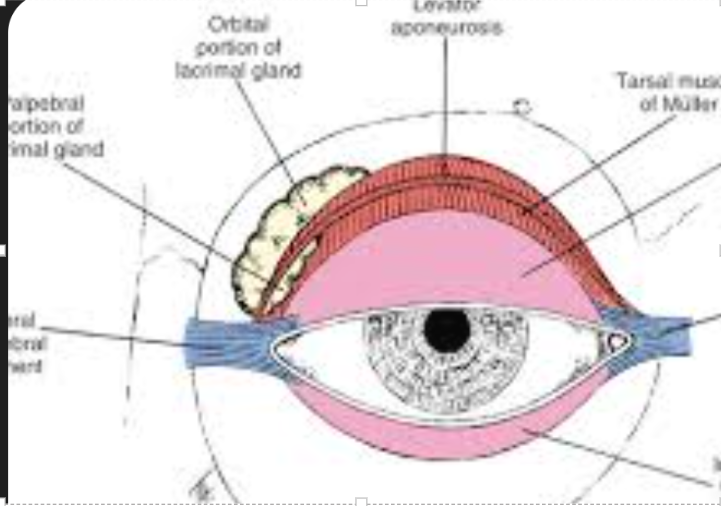
relationship between levator aponeurosis and lacrimal gland
divides lacrimal gland into orbital lobe (upper 2.3rd) and palpebral lobe (lower 1/3rd)
pathway of lacrimal gland secretions
tubuloacinar gland
secretions from acini pass into intercalated ducts and into the main ducts which dischargex onto conjunctival surface

identify features of structure
acini of lacrimal gland
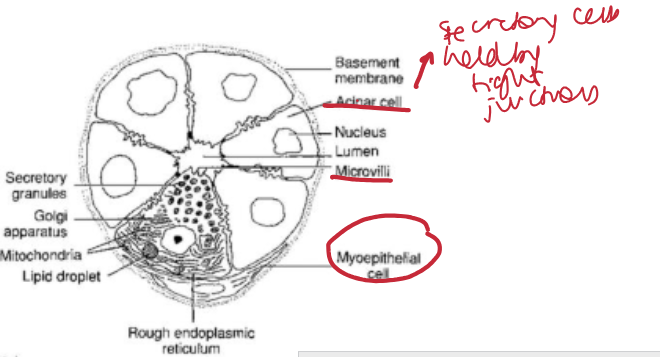
how do acini differ from ducts eg lacrimal gland
ducts lack secretory cells + higher density of myoepithelial cells
ducts modify composition f tear film by secreting electrolytes unlike acini
function of myoepithelial cells in lacrimal gland
Wrap around acini where contractile force squeezes acinus triggering reflex tearing
function of lacrimal stroma lymphocytes
plasma cells secrete IgA in interstices of gland
transported across acini into tears
immunity protection + pathogen defence
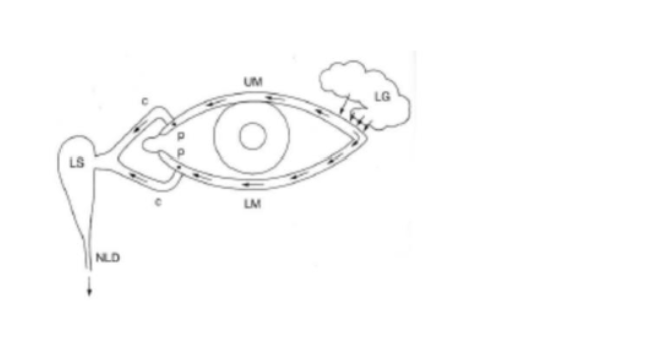
lacrimal drainage system pathway
tears accumulate at inner corner of eye
puncta in eyelid margins connect to lacrimal sac via cannaliculi
lacrimal sac collects tears that travel down nasolacrimal duct into nose for drainage
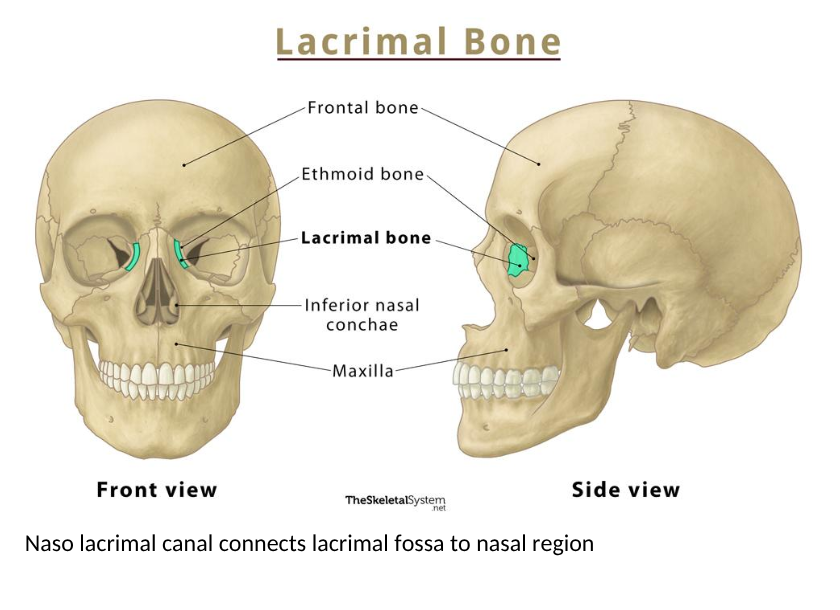
(nasloacrimal canal connects lacrimal fossa to nasal region)
ptosis, proptosis, exopthalmos, enoptlhlamos, epiphora, ectropion, entropion, horedolum
ptosis = drooping of upper eyelid
proptosis + exopthalmos = Abnormal protrusion of eye
enophlamos = Sunken appearance of eye within socket
epiphora = Overflow of tears onto face caused by excessive tear production or blocked drainage ducts
ectropion = Outward turning of lower lid (aging) exposing inner eyelid
entropion = Lower eyelid turns inwards causing lashes/skin to rub against cornea
hordeolum = Stye caused by bacteria
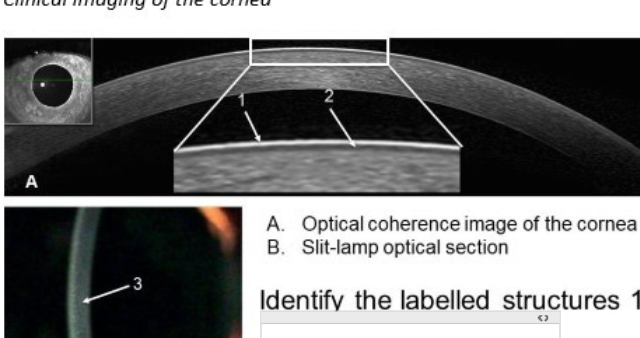
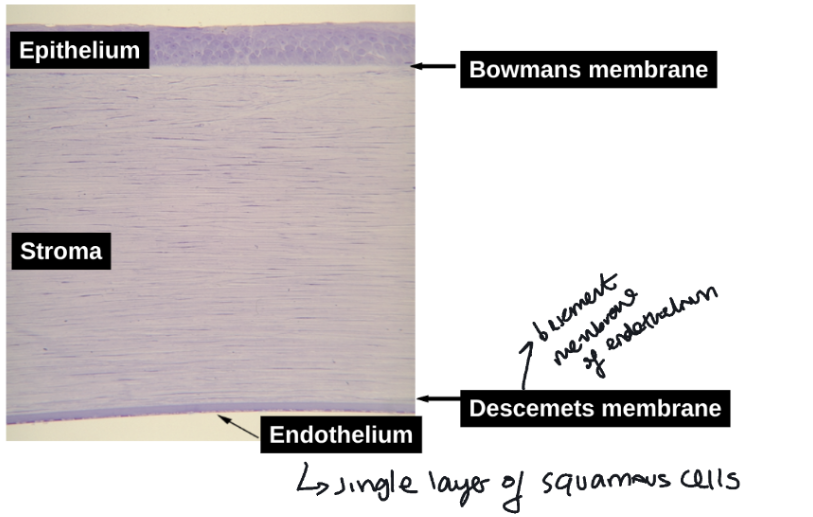
identify stuctures of cornea
1 = pre corneal tear film
2 = corneal epithelium
3 = corneal stroma
typical distance in microns from anterior to posterior surface of central cornea and significance of thickness on intra ocular pressure meaurement
0.52mm
thin cornea = artificially low IOP reading
thick cornea = higher eye pressure reading than it should be
how does the corneal endothelium change with age
Loss of endothelial cells with age
Unable to replicate so increased variability in size and shape
Hexagonal cells expand and flatten to fill gaps
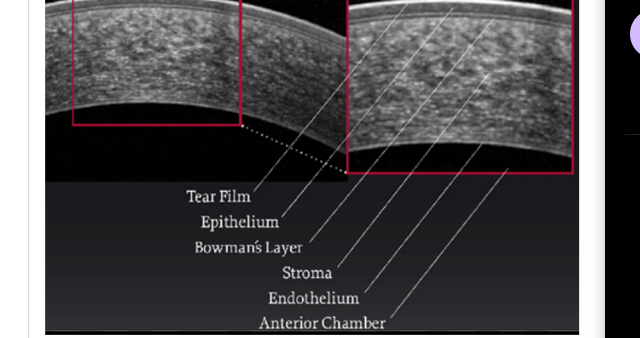
5 layers of cornea
epithelium
bowmans membrane
stroma
descemets membrane
endothelium
adv of having a stratified squamous non keratinised epithelium on anterior corneal surface
non keratinised = no latter scatter = transparant
stratified = renewable barrier from trauma
cell types in corneal epithelium
wing cells, basal cells, squamous cells
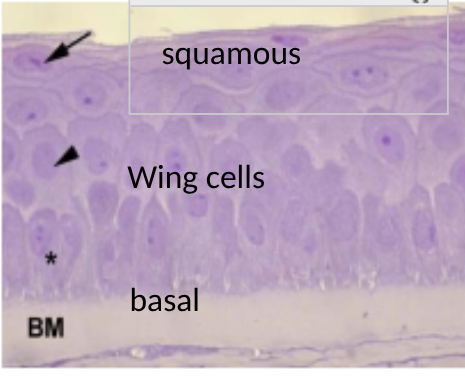
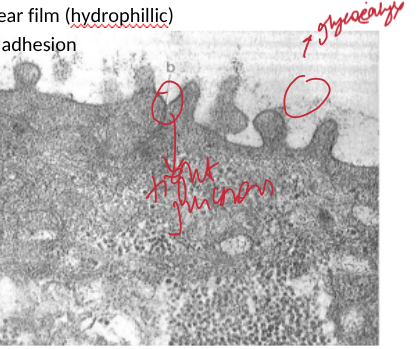
label features of the superficial cells of the cornea
tight junctions between superficial squamous epithelial cells = permeability barrier
glycocalyx facilitates attachment/spreading of tear film (Hydrophillic)
interdigitations and desmosomes between wing cells = intercellular adhesion reistsing force from eye movement
corneal bowmans membrane structure
cell free homogenous layer
lies under epithelium
consists of randomly orientated fine collagen fibrils
corneal stroma structure
regularly arranged lamellae of collagen fibres
paralle fibrils within each lamellae
sucessive lamellae orientate at angles
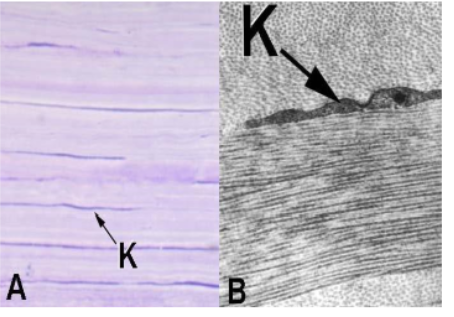
stucture name and label its features
corneal stroma
K = keratocytes = secretes extracellular matrix (collagen and proteoglycans)
stimulate repair
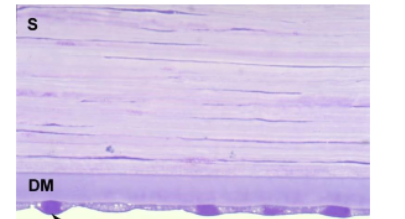
stucture and function
posterior layers of cornea = descemets membrane, stroma and endothelial cell arrowed
corneal endothelium = single layer of squamous cells lining posterior surface of cornea
descemets membrane = basement membrane of endothelium
relationship between organisation of corneal stroma and transparancy
Small diameter collagen fibrils = less light scattered and more light passes through
regular spacing between fibrils= light waves scattered by one fibril interact with others
regular spacing = scattered light waves cancel each other out = destructive interferance
so light passes through = no scatter
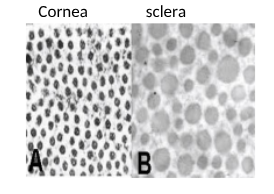
corneal collagen vs scleral collagen structure
Scleral vs corneal collagen:
The cornea has narrow, uniformly packed collagen fibrils allowing transparency, while the sclera has larger, randomly arranged fibrils causing white opacity

how is the corneal endothelium adapted for its role in maintaining physiological hydration and corneal transparancy
Monolayer = facilitates diffusion of nutrients + decreased scatter
Tight junctions = endothelial barrier function so reduce water loss
Numerous mitochondira = ATP for endothelial pump of ions creating osmotic gradient
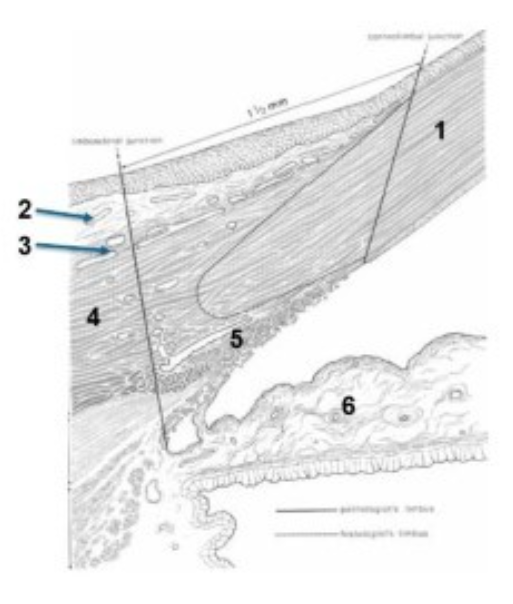
limbus microscopic structure - label structures 1-6
1 cornea
2 conjunctiva
3 episclera
4 sclera
5 trabecular meshwork
6 iris
relationship between limbus and corneal epithelialisation
Sub population of basal cells at limbus (so not only on epithelium) act as stem cells to replenish corneal epithelium
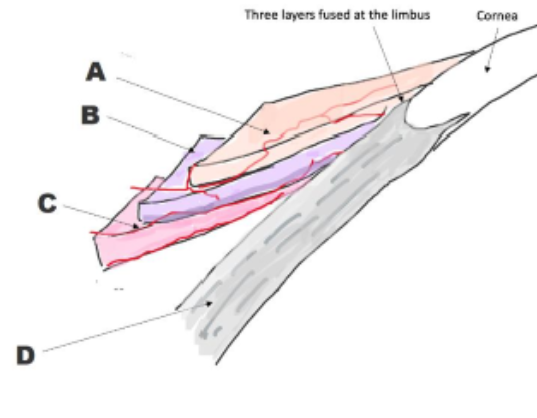
identidy scleral structures
A = conjunctiva
B = tenons capsule
C = episclera
D = sclera
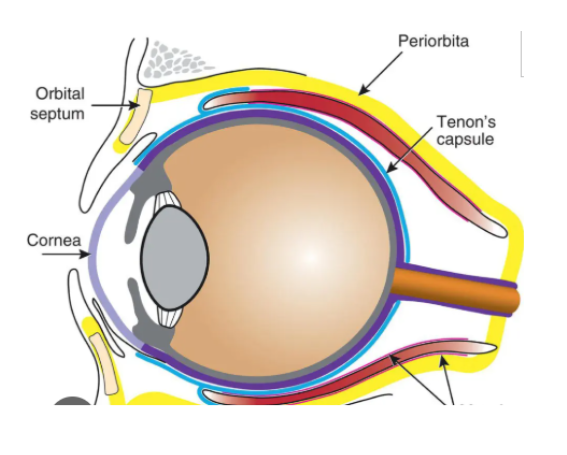
function of tenons capsule
Thin membrane which envelops eyeball from optic nerve to limbus
Found between conjunctiva and episclera
Protects eyeball by forming a socket seperating eyeball from surrounding orbital fat (outside sclera in orbit of eye)
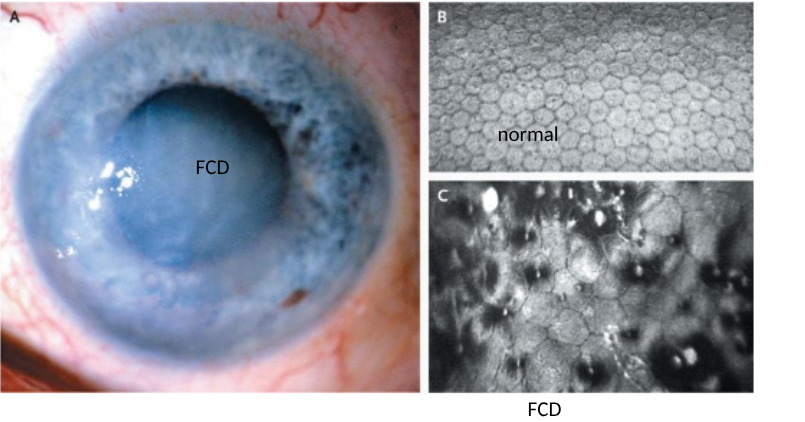
symptoms, causes, treatments of Fuchs corneal dystrophy
glare/blurred vision upon waking (improves over next hours)
causes
corneal endothelial cell loss form guttata (deposits on cornea)
compromised corneal endothelial pump
corneal oedema (inner corneal cells die causing fluid buildup and corneal swelling)
treatment
Eye drops for mild swelling to reduce corneal swelling
Or replacement of damaged endothelial cell layer (corneal transplant)
most common reaons for corneal transplant + alternatives
Corneal dystophies (fuchs. Keratoconus) or corneal scarring
alternative = lamellar grafts and endothelial keratoplasty instead of full thickness graft
why does corneal transplant not need matching donor to host
cornea = immuno privelaged site
no BV so no immune response and no rejection

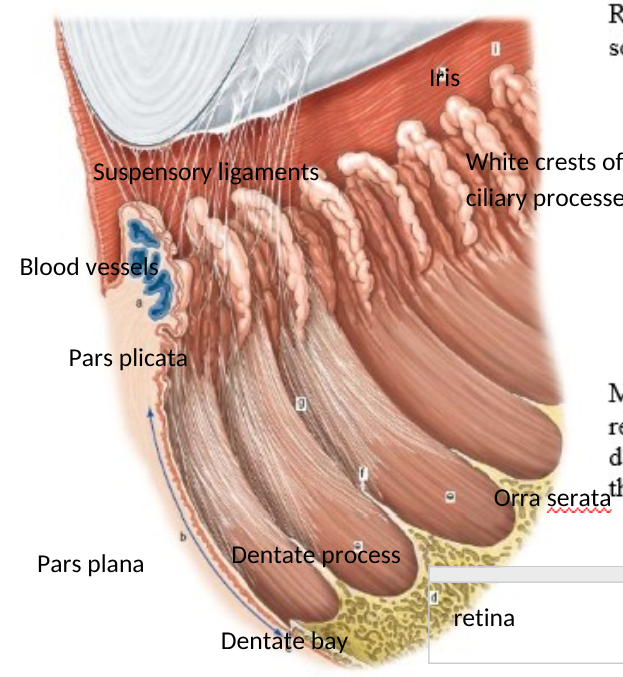
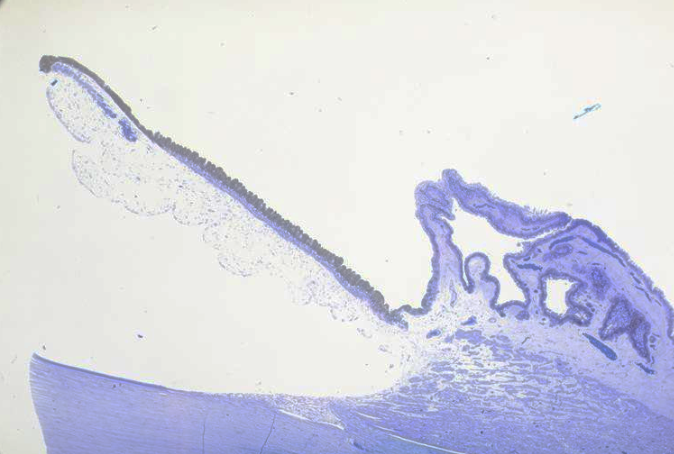
label structures of the anterior eye
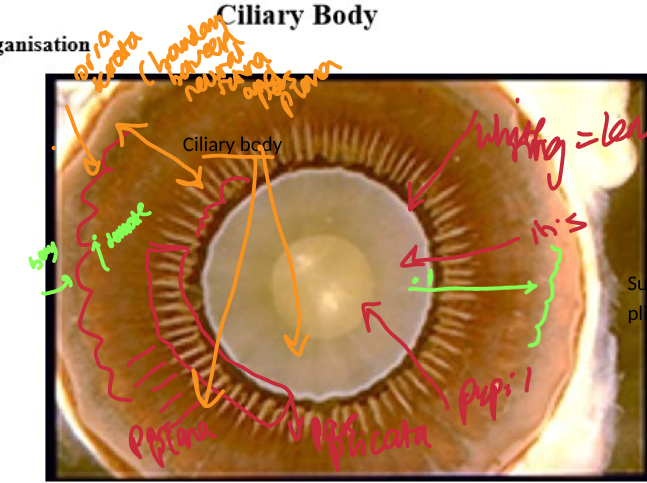
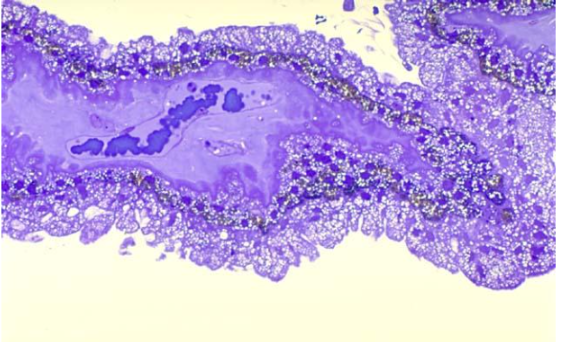
why are the crests of ciliary processes of pars plicata white
pigment lost from outer epithelium
both epithelial = non pigmented
where do suspensory ligaments of zonules attach to ciliary body
begin at lens
run through pars plicata and attach to dentate processes of orra serrata
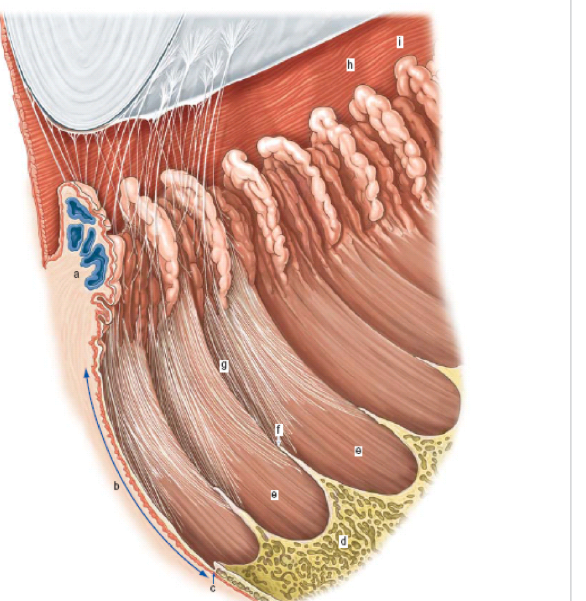
label structures of anterior eye - side profile
a = pars plicata
b = pars plana
h/i = iris
d= retina
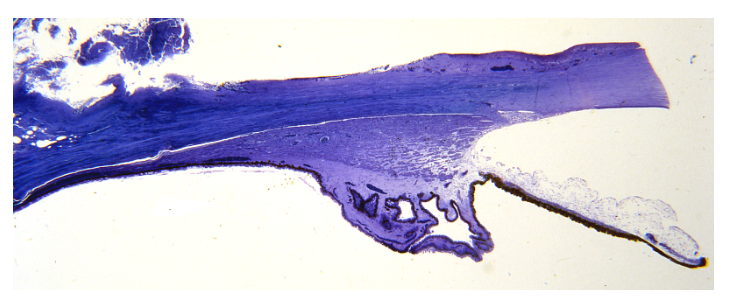
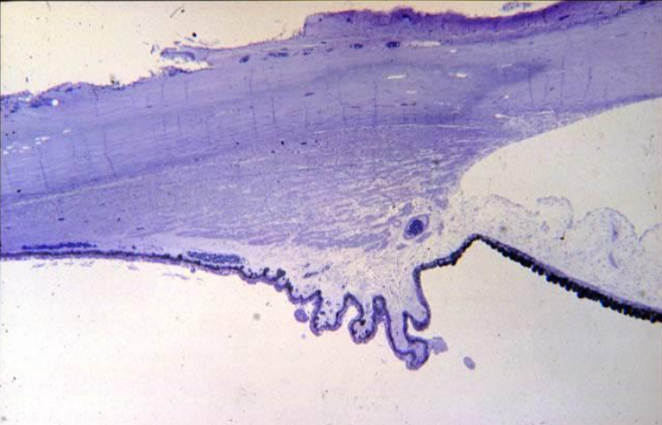
identidy the structures of the microscopic structures of the ciliary body
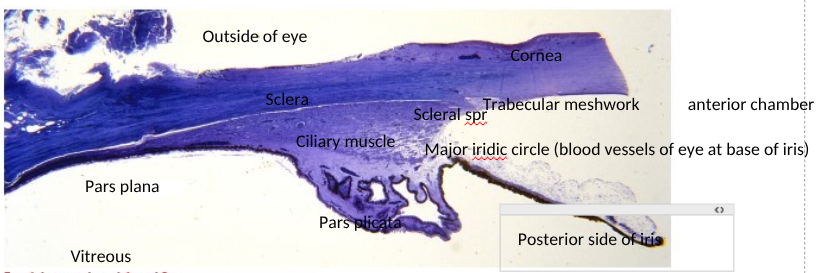
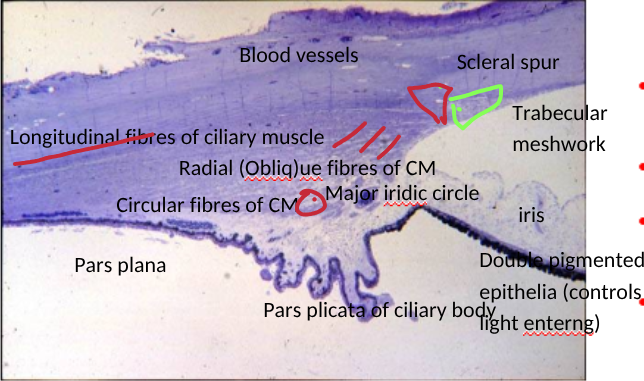
identify the structures of the histology of the filtration angle
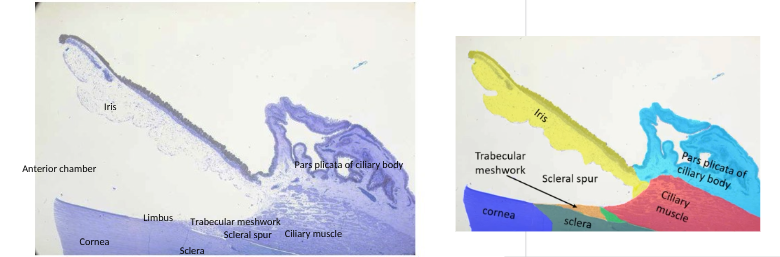
pathway of aqueous at filtration angle
Pars plicata epithelium secretes aqueous
Flows along posterior surface of iris
Through gap between iris and lens into anterior chamber through pupil
Flows around and then leaves via canal of schlemm of trabecular meshwork
scleral spur holds trabecular meshwork in place so aqueous can be fed through and into canal of schlemm for drainage
OR UVEO SCLERAL = leaves between muscle fibres of ciliary muscle

ciliary epithelium structure
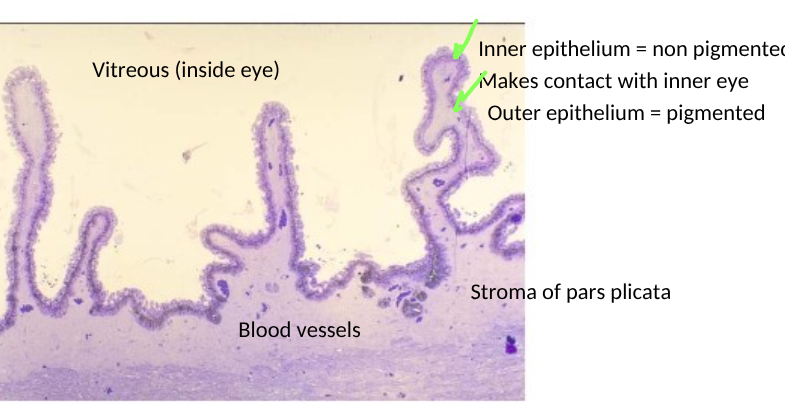
structure of the pars plicata
includes blood vessels (dark blue) and melanocytes
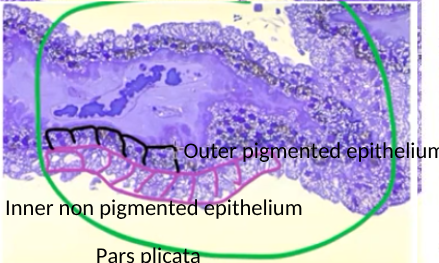
function of the inner vs outer epithelium of the pars plicata of ciliary body
inner = non pigmented = produces aqueous humour
outer = pigmented = absorbs stray light = black box effecr
3 muscles of the ciliary muscle
longitudinal
radial
circular
ciliary muscle structure labels
role of ciliary muscle fibres in accomodation
ciliary muscles contract pulling cilliary body inwards
relieves tension on suspensory ligaments
opens trabecular meshwork increasing aqueous outflor into canal of schlemm
how is ciliary muscle innervated
parasympathetic NS