Equine MSK ICVA Diseases
1/105
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
106 Terms
Angular Limb Deformity:C.S
Valgus (Outward)
Varus (Inward)
Altered Gait
Joint Laxity
Lameness
Angular Limb Deformity:D.X
Exam
Rads: To asses severity
Check Physeal Status
Measure metaphyseal-diaphyseal angle
Joint Orientation
Dynamic Evaluation
U/S
Angular Limb Deformity:Conservative T.X
Hoof trimming + Shoeing
Rest + Controlled excercise
Dietary Management
Angular Limb Deformity: Surgical T.X
Periosteal Stripping
Minimally invasive
Most effective on foals younger than four months for the carpals and 6 months for the tarsus
Transphyseal bridging
For more severe/refractory cases
Screws or Pins
Osteotomy/Ostectomy
In casses where ALD persist into adulthood
Nonseptic Arthritis:C.S
Chronic Lameness
Stiffness
After rest or cold weather
Joint swelling
Joint Pain
Nonseptic Arthritis:D.X
Exam
Imaging
Rads
Joint narrow
Osteophytes
Subchondral bone sclerosis
Effusion
± U/S
Synovial fluid analysis
Mild inflammatory changes
Clear to yellow fluid
Mild elevated protein
WBC less than 5,000
Arthroscopy
Nonseptic Arthritis:T.X
NSAIDs
Corticosteroids
Polysulfated Glycosaminoglycans
Intra-articular injections
Long term use: cause potential cartilage damage and laminitis
Hyaluronic acid
Intra-articular
Regenerative Therapy
Stem cell or Platelet rich plasma
S.X
Debridement, etc
Septic Arthritis:C.X
Acute, severe, unresponsive to rest or NSAIDs
Joint sweling
± Fever
Draining tracts
in cases of penetrating wounds
Crepitus
Septic Arthritis:D.X
Synovial Fluid analysis*
Turbid fluid
Elevated protein
Neutrophilia
Rads
Early stages: Appear normal
Chronic: Joint erosions or bone lysis
U/S
Identity fluid pockets/abscesses in joints
CBC/CHEM
Leukocytosis, ^ Fibrinogen
Septic Arthritis:T.X
Repeated joint lavage
W/ sterile saline
ABX
NSAIDs
SX
Arthroscopy or arthrotomy
Debride necrotic tisue
Rest + Supportive care
What is Bowed Tendon
Tendonitis of the SDFT—> Thickened/Bowed
What is Tendonitis
Inflammation of tendon
What is Desmitis
Inflammation of suspensory or other ligaments
Bowed Tendon/Tendonitis/Desmitis: C.S
Acute Phase
Swelling + Heat on tendon or ligament
Pain on palpation
Lameness+bowed appearance (Bowed tendon)
Chronic Phase
Persistent swelling/Thickening of tendon/ligament (Fibrosis)
Reduced range of motion + stiffness
Mild intermittent lameness thats worse after exercise
Visible bow in SDFTedinitis

Bowed Tendon/Tendonitis/Desmitis: D.X
U/S:Gold standard
Palpation
MRI
DDFT
Nuclear Scintigraphy
Lameness evaluation
Bowed Tendon/Tendonitis/Desmitis: T.X
Treatment depended on severity
Rest + Controlled Exercise
1-3 months complete rest
6-12 months rehabilitation
Cold Therapy, NSAIDs, Physical Therapy
Intralesional Therapy
PRP, Stem cell therapy, Hyaluronic Acid
Surgery
Tenoscopy or Desmotomy
For severe injuries

Bucked Shins (Dorsal metacarpal periostitis): Pathophy
Young horses in training—> continuous strain on MC3–> ^bone remodel—>Fail to keep up—> Stress fractures
Bucked Shins:C.S
Forelimb lameness
Worse during training
Heat + Swelling of Dorsal aspect of MC3
Pain on palpation, Reduced performance
Stiff on gallop
Bucked Shins:D.X
C.S
Rads
Periosteal new bone formation along dorsal cortex of MC3
Radiolucent ares ( Stress fractures)
Nuclear Scintigraphy
U/S
Thermography
Bucked Shins:T.X
Rest 30 to 60 days
NSAIDs, cold therapy, shockwave therapy
^Bone Heal, Decreased inflammation
Surgery
Severe or refractory (Osteostixix)
Gradual return to training
What is Osteochondrosis
Disturbance during endochondral ossification, leading to retained areas of cartilage within bone
These areas are weaker thus prone to fractures
Common sites
Tarsocrural (Hock)
Stifle joint
Fetlock joint
What is Physitis
Inflammatory condition of the physes of long bones seen in rapidly growing horses
Mostly self limiting
Common sites
Distal radius
Distal cannon bone
Distal tibia
What is subchondral bone cysts
Fluid filled cavities in the subchondral bone due to focal damage to the articular cartilage
Common sites
Stifle
Fetlock
Phalanges
Osteochondrosis: C.S
Lameness
Joint efusion
Reduced range of motion
Pain upon palpation
Osteochondrosis:D.X
Rads
OCD lesions
Subchondral bone flattening
U/S
MRI
Arthroscopy*
Osteochondrosis:T.X
Rest + controlled exercise
SX(arthroscope)
Nutritional management (balanced miniral intake)
Intra-articular meds
Hyaluronic acid
Corticosteroids
Regen therapy
Physitis:C.S
Lameness in foals
Firm symmetrical swelling around the growth plates
Stiff gait
Angular limb deformities
Physitis:D.X
Exam
Rads
U/S
Physitis: T.X
Dietary management
Reduce caloric intake
NSAIDs
Controlled exercise
Corrective farrowing
Subchondral Bone Cysts:C.S
Intermittent lameness:
Varies in severity and often worsens with exercise.
Joint effusion
May occur if the cyst communicates with the joint space.
Pain on joint flexion:
Particularly noticeable when manipulating the affected joint.
Chronic lameness:
If left untreated, this can lead to persistent joint dysfunction.
Subchondral Bone Cysts: D.X
Radiographs:
Key to identifying cystic lesions within the subchondral bone.
MRI or CT:
Advanced imaging can provide more detail on the extent and depth of the cyst, as well as its communication with the joint.
Arthroscopy:
Useful for visualizing the cyst and assessing the condition of the cartilage.
Subchondral Bone Cysts:T.X
Arthroscopic debridement:
The cyst is surgically cleaned out to remove necrotic tissue and encourage bone healing.
Intra-articular injections:
Corticosteroids or regenerative therapies such as PRP can help manage inflammation and promote healing.
Rest and rehabilitation:
Essential to allow the bone and cartilage to recover.
Orthobiologic treatments:
Stem cells or bone grafts may be used in severe cases to promote healing of the cystic area.
What is Hyperkalemic Periodic Paralysis
Hyperkalemic Periodic Paralysis (HYPP) is a genetic disorder affecting the sodium channels in the muscle cells of horses.
The sodium channels in HYPP-positive horses become defective, allowing for abnormal sodium influx when the membrane depolarizes.
Results in prolonged depolarization of the muscle cell membrane and the inability to restore the resting potential, leading to spontaneous muscle contractions, weakness, and potentially paralysis.
Elevated potassium levels in the blood (hyperkalemia) trigger these episodes because the sodium channel's dysfunction is exacerbated by increased extracellular potassium.
This is a hallmark pathophysiologic feature of HYPP, where potassium plays a direct role in muscle dysfunction.
Hyperkalemic Periodic Paralysis:C.S
Muscle fasciculations
The flanks, neck, and shoulders
Prolapse of the third eyelid during episodes
Generalized muscle weakness,
± Appearing "wobbly" or unstable
Sweating and anxious behavior
Difficulty breathing (stridor) due to pharyngeal muscle involvement
Recumbency and paralysis in severe cases
Cardiac arrhythmias
Bradycardia or tachycardia
Hyperkalemic Periodic Paralysis:D.X
DNA testing: This is the definitive diagnostic tool for HYPP. It can be done using a hair or blood sample.
Since the disorder is caused by a well-defined mutation in the SCN4A gene
Serum potassium levels: Elevated potassium levels during an episode can support the diagnosis, but this is not consistently elevated between episodes, so it is not a reliable sole diagnostic marker.
Electromyography (EMG): EMG may show abnormal muscle electrical activity consistent with myotonia in affected horses, though it is not a routine diagnostic tool for HYPP.
Hyperkalemic Periodic Paralysis: Acute management T.X
Intravenous calcium gluconate: Calcium stabilizes the excitable membranes of muscle cells, reducing the severity of depolarization.
Intravenous dextrose: Dextrose promotes intracellular potassium uptake, lowering serum potassium levels and alleviating symptoms.
Acetazolamide: A carbonic anhydrase inhibitor, acetazolamide increases renal excretion of potassium and promotes mild diuresis. It also causes metabolic acidosis, which helps reduce potassium levels in the blood.
Tracheostomy may be necessary if the horse experiences significant respiratory distress due to pharyngeal paralysis.
Hyperkalemic Periodic Paralysis:Long-Term Management:
Dietary management: Restricting potassium intake is key to managing HYPP. Forage such as alfalfa should be avoided, and grain mixes high in molasses or potassium should be substituted with low-potassium feeds (e.g., grass hay, beet pulp).
Regular exercise: Exercise encourages potassium excretion and helps to maintain normal muscle function.
Potassium binders: Oral potassium-binding agents like sodium polystyrene sulfonate may be used in horses that have difficulty maintaining stable potassium levels.
Acetazolamide: This drug can be administered chronically to reduce serum potassium levels, thereby preventing episodes. It also has a direct effect on reducing muscle excitability.
Commonly Affected Joints in Horses
Coxofemoral Joint (Hip): Hip luxations are rare in horses due to the deep acetabulum, but they can occur due to severe trauma, such as a fall or being cast in a stall.
Stifle Joint: Patellar luxation can be seen in foals with congenital deformities or in adult horses following trauma. Stifle injuries often involve damage to the ligaments or menisci.
Fetlock Joint: The fetlock is a high-motion joint commonly affected by luxation due to its critical role in weight-bearing and movement. Trauma, such as a fall or kick, can result in luxation.
Tarsal (Hock) Joint: Hock luxations often result from severe trauma, such as a fall or collision. They can involve multiple joints within the tarsus, making diagnosis and treatment complex.
Atlantoaxial Joint (Cervical Spine): Less common but significant, cervical luxations typically occur due to trauma and can lead to severe neurological deficits.
Joint Luxations: C.S
Acute Lameness:
The horse often exhibits non-weight-bearing lameness due to pain and joint instability.
Joint Deformity:
Visible or palpable abnormalities in the joint contour, such as shortening of the limb or abnormal bony prominence in hip luxations.
Swelling:
Soft tissue swelling around the joint caused by inflammation, synovial fluid leakage, or hemorrhage.
Pain on Manipulation:
Palpation and manipulation of the joint elicit pain and may reveal abnormal movement (crepitus).
Restricted Range of Motion:
The affected joint may exhibit limited or abnormal motion due to pain, soft tissue swelling, and joint misalignment.
Joint Luxations:D.X
A thorough diagnostic evaluation is crucial to confirm joint luxation, assess its severity, and guide appropriate treatment:
Physical Examination:
Palpation of the affected joint often reveals abnormal positioning, swelling, and crepitus. For instance, hip luxation may present with a limb that appears shortened and an externally rotated femur.
Neurological assessment is necessary to check for nerve damage, particularly in severe luxations involving the limbs.
Radiography (X-rays):
Provide detailed information on the extent of bone displacement, joint capsule damage, and any concurrent fractures.
For hip luxation, a standard dorsoventral view of the pelvis helps confirm the direction of the luxation and assess the acetabulum’s integrity.
Ultrasound: Useful for evaluating soft tissue structures around the joint, including ligaments and tendons, to identify additional injuries.
Advanced Imaging (CT/MRI):
Employed in complex cases to provide a detailed assessment of joint capsules, ligaments, and articular cartilage.
Particularly beneficial for evaluating deep joints like the hip or intricate structures like the stifle.
Joint Luxations: Closed Reduction tx
Indications: Acute luxations without fractures or significant soft tissue damage.
Procedure: Performed under general anesthesia to manually reposition the bones into normal alignment. Post-reduction radiographs confirm successful realignment.
Post-Reduction: The joint is immobilized using bandages, splints, or slings (e.g., Robert Jones bandage for limb joints) to allow soft tissue healing. Restricted activity and monitoring for recurrence are necessary.
Joint Luxations: Open Reduction and Internal Fixation (ORIF)T.X
Indications: Chronic luxations, cases with concurrent fractures, or when closed reduction fails.
Procedure: Surgical intervention to realign the joint and stabilize it using fixation methods such as screws, plates, suture anchors, or prosthetic ligaments.
Post-Operative Care: Involves joint immobilization, pain management, and physical therapy to restore joint function.
Joint Luxations: Salvage Procedures T.X
Indications: When joint integrity cannot be restored or in cases of severe degenerative joint disease following luxation.
Options: Procedures include arthrodesis (joint fusion) to eliminate movement in the affected joint or excision arthroplasty (e.g., femoral head ostectomy in hip luxations) to alleviate pain.
Lameness: C.S
Head Nodding or Bobbing:
In forelimb lameness
Raises its head when the affected limb touches the ground and lowers it when the sound limb is loaded.
Hip Hike or Drop:
In hindlimb lameness
Exaggerated motion of the hips
with the affected side appearing to "hike" or rise higher than normal.
Reduced Range of Motion:
Affected joints or limbs exhibit stiffness,
Reduced flexibility,
Shortened strides.
Reluctance to Move:
Swelling and Heat:
Abnormal Limb Placement: Affected horses may place the limb in an abnormal stance to alleviate pain, such as shifting weight onto the opposite limb.
Diagnostics for Lameness in Horses
1. Lameness Examination: A thorough physical examination and dynamic assessment of the horse at walk, trot, and potentially under saddle are the first steps in lameness diagnosis. Specific diagnostic tools include:
Flexion Tests: Performed to isolate and exacerbate pain in specific joints or limbs. Positive flexion tests indicate increased discomfort or lameness after flexion and trotting.
Hoof Tester Examination: Used to detect pain or sensitivity in the hoof, often indicating hoof abscesses, laminitis, or bruises.
2. Diagnostic Imaging:
Radiography (X-rays): Useful in detecting bone fractures, joint abnormalities, and osteoarthritis.
Ultrasound: Primarily employed to evaluate soft tissue injuries, such as tendinitis, desmitis (ligament injuries), and muscle tears.
Nuclear Scintigraphy (Bone Scans): Often used for horses with vague lameness or hard-to-locate pain, detecting areas of increased bone metabolism.
Computed Tomography (CT) and Magnetic Resonance Imaging (MRI): Advanced imaging used to detect subtle lesions in bones, joints, and soft tissues that may not be visible with other techniques.
3. Nerve Blocks: Local anesthesia (nerve or joint blocks) helps isolate the affected region by numbing specific areas sequentially. A reduction in lameness following a block confirms the location of pain, aiding in diagnosis.
4. Arthroscopy: This minimally invasive procedure allows direct visualization and treatment of joint issues. Arthroscopy is often performed in cases of osteochondritis dissecans (OCD), joint debris, or cartilage damage.
Deep dive into diagnosis:1. Flexion Tests
Purpose: Flexion tests are designed to put stress on specific joints or parts of a limb to pinpoint areas of discomfort. By holding the limb in a flexed position and then assessing the horse’s movement immediately after, the test helps identify potential sources of lameness.
Procedure: A veterinarian or technician holds a joint (such as the fetlock, carpus, hock, or stifle) in a flexed position for a specific duration (typically 30 seconds to 1 minute). Immediately after, the horse is trotted in a straight line. The examiner observes for any changes in the horse's gait, including stiffness, shortened stride, limping, or an increase in lameness.
Interpretation:
Positive Flexion Test: If the horse shows increased lameness or an obvious discomfort after the test, it suggests that the joint or region tested may be the source of pain.
False Positives: Note that some degree of discomfort may be normal following flexion, especially in older horses or those with pre-existing conditions, so results must be interpreted carefully and alongside other diagnostics.
2. Hoof Tester Examination
Purpose: Hoof testers are used to apply pressure to various areas of the hoof to identify pain or sensitivity. This method is particularly useful for detecting conditions localized in the hoof, such as abscesses, bruises, laminitis, or sole punctures.
Procedure: A hoof tester, a large metal tool, is used to squeeze different parts of the hoof, including the sole, frog, bars, and heel. The veterinarian or farrier carefully applies pressure in each area and monitors the horse’s response for signs of discomfort, such as flinching, lifting the hoof, or attempting to pull away.
Interpretation:
Positive Response: If the horse reacts strongly to pressure in a specific area, it indicates a potential problem, such as a hoof abscess (localized pain), laminitis (widespread sensitivity), or bruising.
Limitations: While a hoof tester can help identify pain in the hoof, it may not reveal the exact cause, so further diagnostic imaging (e.g., X-rays) is often needed to confirm the diagnosis.
3. Nerve Blocks (Local Anesthesia)
Purpose: Nerve blocks, also known as diagnostic anesthesia, are a vital tool for pinpointing the exact location of lameness in horses. By sequentially numbing specific nerves or regions, veterinarians can isolate the source of pain, narrowing down possible causes. Here’s an in-depth look at the types of nerve blocks, how they’re performed, and what their results indicate.
Why Use Nerve Blocks?
Nerve blocks are used to:
Localize the area of pain within a limb.
Rule out or confirm specific regions as the source of lameness.
Guide further diagnostic steps, like imaging (radiographs, ultrasound).
TNerve Block Locations
Typical cutaneous areas (TCAs) innervated by the medial and lateral palmar nerves (below the communicating branch). The cutaneous areas supplied by the medial and lateral palmar metacarpal nerves are represented by the white areas enclosed by dash-margin. The TCAs with grid pattern are innervated by both nerves. On the medial aspect of the proximal interphalangeal joint and coronary band between the dorsal and palmar midline, there is a skin area supplied only by the medial palmar nerve (autonomous zone of the median nerve).
1. Rest and Controlled Exercise: For mild soft tissue injuries or inflammation, rest combined with controlled exercise is crucial. Gradual reintroduction to activity helps prevent reinjury.
2. Anti-Inflammatory Medications: Non-steroidal anti-inflammatory drugs (NSAIDs) like phenylbutazone (Bute) and flunixin meglumine (Banamine) are commonly used to reduce pain and inflammation in acute and chronic lameness.
3. Joint Injections:
Corticosteroids: Intra-articular corticosteroid injections are used to reduce inflammation and pain in degenerative joint conditions like osteoarthritis.
Hyaluronic Acid: Helps lubricate the joint and promote cartilage health in horses with joint disease.
4. Supportive Therapies:
Shockwave Therapy: Extracorporeal shockwave therapy stimulates healing and reduces pain in soft tissues and bones.
Laser Therapy and Cold Therapy: These modalities promote healing by increasing blood flow and reducing inflammation.
Regenerative Therapies: Stem cell injections, platelet-rich plasma (PRP), and IRAP (Interleukin-1 Receptor Antagonist Protein) therapies are used for tendon, ligament, and joint injuries.
5. Corrective Shoeing: Horses with hoof-related lameness such as laminitis or navicular syndrome benefit from corrective shoeing and trimming. Hoof balance is restored by adjusting angles and using specialized shoes to support the affected structures.
6. Surgical Intervention:
Arthroscopy: Used to remove osteochondral fragments, cartilage damage, or joint debris in conditions like OCD or fractures.
Tendon Surgery: Severe cases of tendon injuries may require surgical repair or debridement.
Fracture Fixation: Open or closed reduction techniques are employed to stabilize fractures using plates, screws, or external fixation devices.
Hallmark Clinical Signs and Diagnosis of Common Lameness Conditions
Laminitis: Horses exhibit characteristic signs like reluctance to move, a "sawhorse" stance (leaning back to relieve pressure on the front feet), and heat in the hooves. Radiographs reveal rotation of the coffin bone (P3).
Navicular Syndrome: Chronic, intermittent forelimb lameness worsened by hard surfaces. Nerve blocks of the heel region (palmar digital nerve block) temporarily relieve lameness. Radiographs may show remodeling of the navicular bone.
Osteoarthritis (Degenerative Joint Disease): Progressive stiffness, swelling, and reduced range of motion in affected joints. Radiographs confirm joint space narrowing, osteophyte formation, and subchondral bone sclerosis.
Tendon Injuries (e.g., Superficial Digital Flexor Tendinitis): Localized swelling, heat, and pain along the tendon, often accompanied by lameness. Ultrasound confirms fiber disruption or tears.
Conclusion
Lameness in horses is a complex, multifactorial condition requiring a thorough diagnostic workup, including a detailed physical exam, imaging, and sometimes advanced procedures. Early diagnosis and appropriate treatment, whether medical, surgical, or supportive, are crucial for optimizing recovery and long-term soundness. By understanding the pathophysiology, clinical signs, and diagnostics of lameness, veterinarians can make informed decisions to improve outcomes for affected horses.
Nerve Blocks
Nerve blocks, also known as regional anesthesia or perineural anesthesia, are an indispensable diagnostic tool in equine medicine for localizing the source of lameness. By sequentially desensitizing specific regions of the limb, nerve blocks help pinpoint areas of pain and guide further diagnostic and treatment decisions. A deep understanding of the pathophysiology, indications, and application of these blocks is essential for accurate lameness evaluation and management.
Pathophysiology of Lameness and the Role of Nerve Blocks
Lameness in horses arises due to pain, mechanical dysfunction, or both. Conditions affecting the bones, joints, tendons, ligaments, and soft tissues can alter the horse's gait, leading to uneven weight distribution and compensatory strain on other limb structures. Nerve blocks function by temporarily numbing specific sensory nerves, thereby disrupting the pain signals transmitted to the central nervous system. When a block alleviates the lameness, it suggests that the desensitized region contains the source of pain.
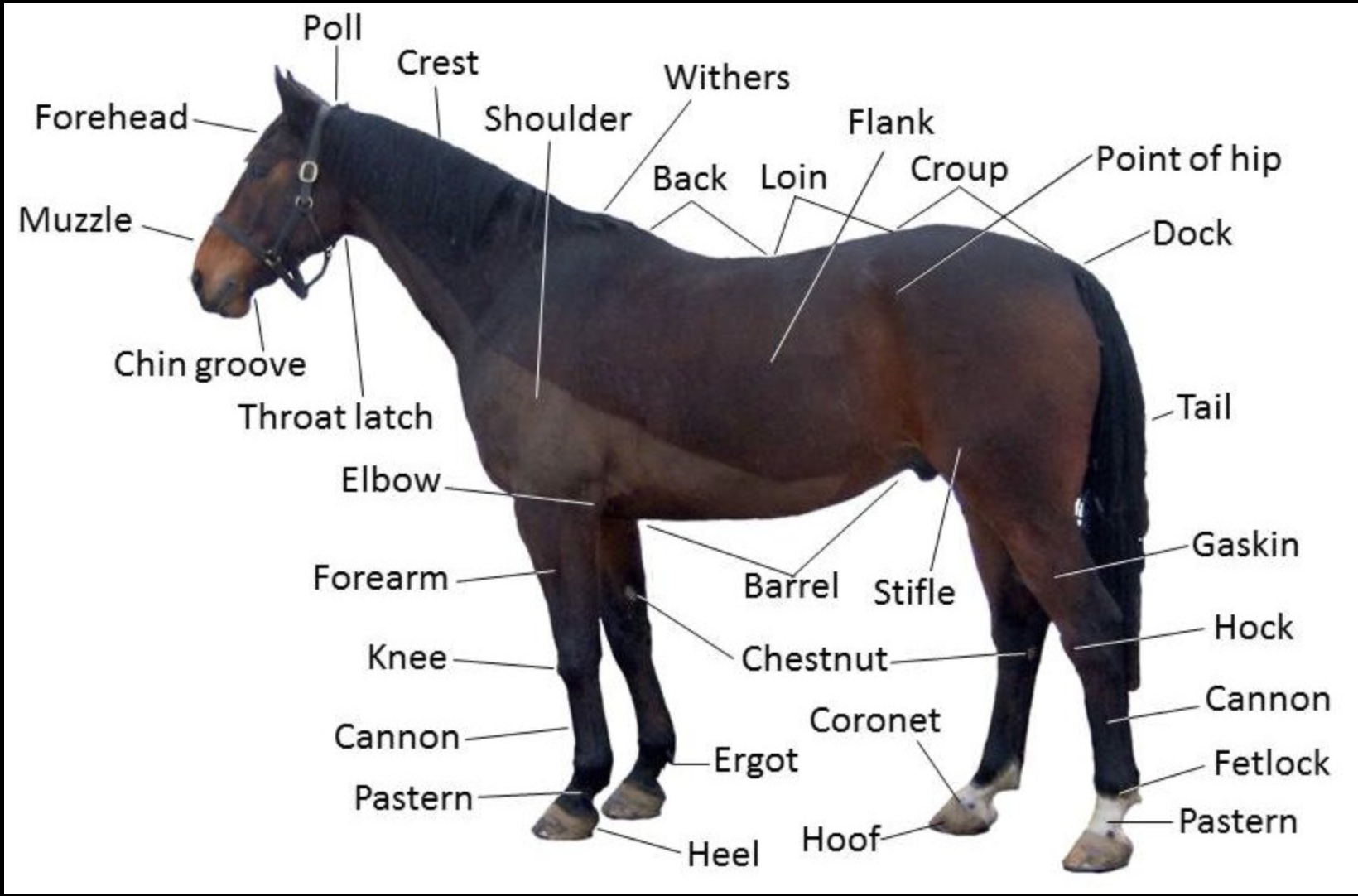
Horse anatomy
Image: Creative Commons
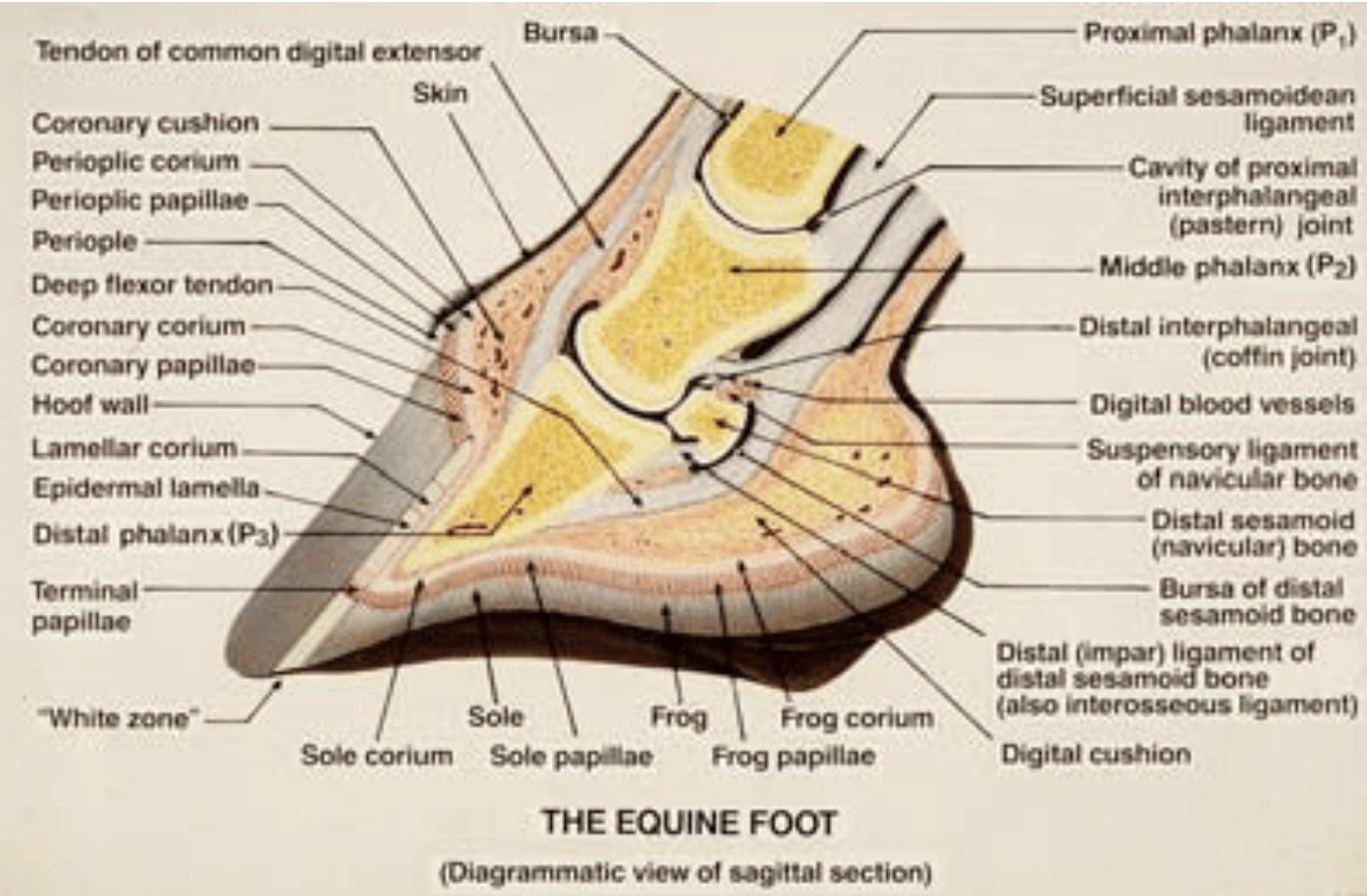
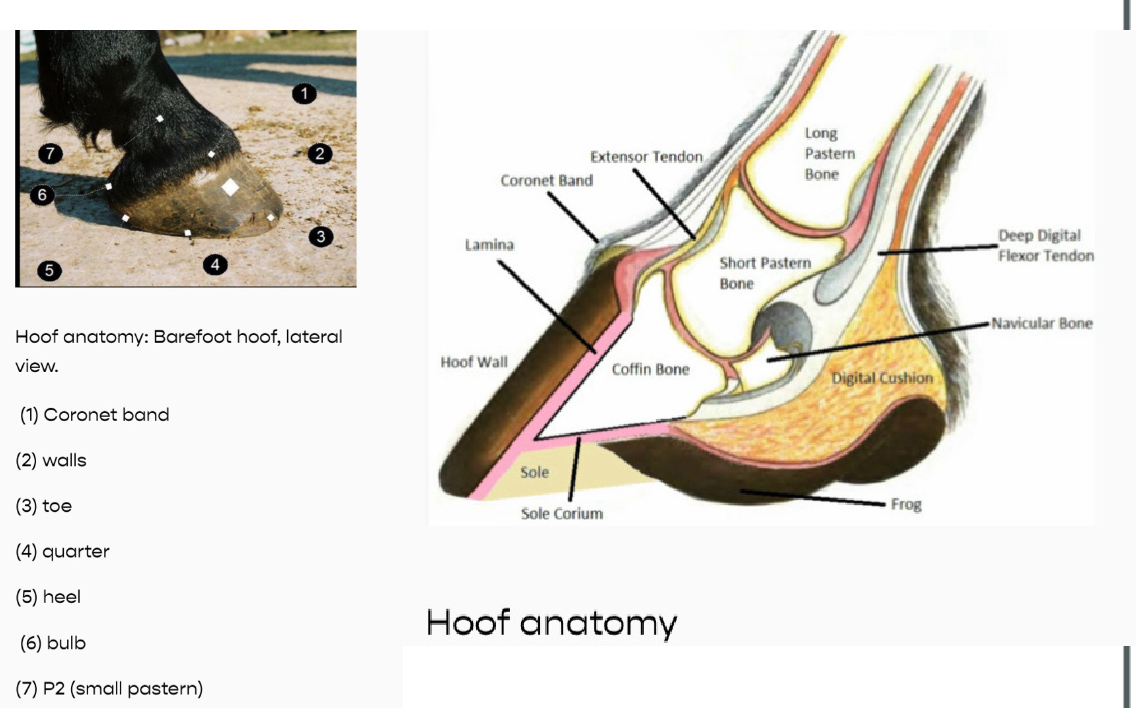
Hoof anatomy
Image: Pollitt, Chris & Kyaw-Tanner, Myat & French, Kathryn & Eps, A & Hendrikz, J. & Daradka, Mousa. (2003). Equine Laminitis. Proc. Am. Ass. equine Practnrs. 49.
Clinical Signs Indicating the Need for Nerve Blocks
Persistent or intermittent lameness that cannot be localized through physical examination alone
Lameness that worsens with exercise or flexion tests
Positive response to hoof testers indicating focal pain in the hoof
Gait abnormalities such as toe dragging, shortened stride, or uneven foot placement
Increased digital pulses or limb swelling that do not provide a definitive diagnosis
Nerve blocks allow the practitioner to systematically work through the limb, starting from the distal structures and moving proximally. The gradual numbing of sensory input helps narrow down the affected area, thus guiding further imaging and treatment.
Risk Factors for Lameness Requiring Nerve Blocks
High-performance horses (e.g., racehorses, eventers, jumpers) are prone to musculoskeletal injuries due to the increased physical demands placed on their limbs.
Aging equines often develop degenerative joint diseases or soft tissue pathologies that lead to chronic lameness.
Conformation abnormalities, such as long toes, low heels, or upright pasterns, can predispose horses to repetitive stress injuries.
Improper hoof care can result in hoof imbalances and conditions like navicular syndrome, laminitis, or sole bruising, frequently necessitating the use of nerve blocks for diagnosis.
Diagnostics: Types of Nerve Blocks and Their Application1. Palmar/Plantar Digital Nerve Block (PDN)
Anatomy Blocked: This block targets the palmar or plantar digital nerves, located just above the heel bulbs. It desensitizes the back third of the hoof, including the heel, sole, frog, digital cushion, and portions of the coffin bone.
Procedure: A small amount of local anesthetic (usually 2-3 mL of mepivacaine or lidocaine) is injected on each side of the limb at the level of the pastern, near the heel bulbs.
Clinical Use: The PDN block is primarily used to identify pain originating from structures in the hoof, such as navicular syndrome, heel pain, sole bruising, or hoof abscesses.
Interpretation: A positive response (improvement in lameness) confirms that the source of pain is localized to the caudal aspect of the hoof. This block does not desensitize the dorsal or proximal parts of the limb.

Palmar/Plantar Digital Nerve Bloc
Located just above the heel bulbs
Identifies pain originating from structures in the hoof, such as navicular syndrome, heel pain, sole bruising, or hoof abscesses.
2. Abaxial Sesamoid Nerve Block
Anatomy Blocked: Desensitizes the palmar or plantar digital nerves at the level of the proximal sesamoid bones. This numbs the entire hoof, the coffin joint, the pastern joint, and the distal portions of the deep digital flexor tendon.
Procedure: The anesthetic is injected just above the fetlock on both the medial and lateral aspects, adjacent to the base of the proximal sesamoid bones.
Clinical Use: This block is indicated when the source of pain is suspected to be in the pastern or coffin joint, deep digital flexor tendon, or lower parts of the limb.
Interpretation: A positive response indicates that the pain is likely originating from within the foot or pastern, such as coffin joint arthritis, pastern joint osteoarthritis, or deep digital flexor tendon pathology.

Abaxial Sesamoid Nerve Block
Located just above the fetlock on both the medial and lateral
Indicated when the source of pain is suspected to be in the pastern or coffin joint, deep digital flexor tendon, or lower parts of the limb.
3. Low Palmar (Low 4-Point) Nerve Block
Anatomy Blocked: Blocks the medial and lateral palmar nerves and the palmar metacarpal nerves at the distal end of the splint bones. This desensitizes the fetlock joint and structures below it, including the digital flexor tendons and suspensory ligament branches.
Procedure: An anesthetic is injected on both the medial and lateral aspects of the limb, distal to the splint bones. This involves four injection sites to block both the palmar nerves and the palmar metacarpal nerves.
Clinical Use: Used to diagnose conditions involving the fetlock, suspensory ligament branches, digital flexor tendons, and distal joints.
Interpretation: If lameness improves, the source of pain is likely in the fetlock joint, digital flexor tendons, or suspensory ligament branches. This block is particularly helpful for diagnosing suspensory branch desmitis, fetlock arthritis, or tendon sheath pathology.

Low Palmar (Low 4-Point)
Located medial and lateral aspects of the limb, distal to the splint bones
Indicated to diagnose conditions involving the fetlock, suspensory ligament branches, digital flexor tendons, and distal joints.
4. High Palmar (High 4-Point) Nerve Block
Anatomy Blocked: Desensitizes the medial and lateral palmar nerves, as well as the palmar metacarpal nerves, at the level of the proximal metacarpus. This affects the entire limb below the carpus, including the proximal suspensory ligament.
Procedure: Local anesthetic is injected on both the medial and lateral aspects of the limb, just above the splint bones, to block the palmar nerves and the palmar metacarpal nerves.
Clinical Use: Primarily used for diagnosing proximal suspensory desmitis, deep digital flexor tendonitis, and other conditions in the proximal metacarpus.
Interpretation: Improvement in lameness following this block indicates pain originating from the proximal suspensory ligament, metacarpal bones, or flexor tendons.

High Palmer (High 4 point)
Location: both the medial and lateral aspects of the limb, just above the splint bones
Indication for diagnosing proximal suspensory desmitis, deep digital flexor tendonitis, and other conditions in the proximal metacarpus
5. Tibial and Peroneal Nerve Blocks (Hindlimb)
Anatomy Blocked: These blocks desensitize the hindlimb below the hock, affecting structures such as the hock joint, fetlock joint, and distal tendons.
Procedure: The tibial nerve is blocked on the medial side of the limb, and the peroneal nerve on the lateral side, just above the hock. These two blocks are often performed together to ensure complete desensitization.
Clinical Use: Used to identify conditions within the hock, suspensory ligament, or lower hindlimb.
Interpretation: If lameness improves after both blocks, the source of pain is localized to the structures innervated by these nerves, often indicating conditions like hock arthritis, proximal suspensory desmitis, or tendon sheath inflammation.

Tibial and peroneal nerve blocks
Location: the tibial nerve is blocked on the medial side of the limb, and the peroneal nerve on the lateral side, just above the hock.
Indication: Used to identify conditions within the hock, suspensory ligament, or lower hindlimb.

Nerve Blocks
Want to learn more? Check out this video by CSU: Nerve Blocks Made Easy
Diagnostics: Hallmark Signs and Interpretation
Positive Response to Nerve Block: A marked improvement in lameness following a specific block confirms that the desensitized area contains the source of pain. For example, a positive response to a palmar digital nerve block localizes the issue to the heel or caudal hoof structures.
Sequential Blocking: By starting distally (e.g., palmar digital block) and moving proximally (e.g., high 4-point block), veterinarians can narrow down the affected region, leading to more targeted imaging (radiography, ultrasound) and treatment.
Treatment Based on Nerve Block Results
The treatment of equine lameness depends on the condition identified through nerve blocks. Common treatments include:
Corrective Farriery: Adjusting hoof balance and shoeing to alleviate pressure on the affected structures (e.g., raising heels in navicular syndrome).
Intra-articular Injections: Administration of corticosteroids, hyaluronic acid, or regenerative therapies into joints or tendon sheaths identified as sources of pain.
Rest and Rehabilitation: Prescribed periods of rest followed by controlled exercise for conditions like suspensory ligament injuries.
Surgical Intervention: Arthroscopy or other surgical procedures for conditions such as chip fractures or advanced navicular disease.
NSAIDs and Pain Management: Non-steroidal anti-inflammatory drugs for managing pain and inflammation during recovery.
Conclusion
Nerve blocks are an essential diagnostic tool for equine practitioners to localize the source of lameness in horses. A thorough understanding of the anatomical regions affected by each block and the interpretation of clinical responses is crucial for an accurate diagnosis. The use of sequential blocking, combined with advanced imaging and clinical examination, allows for a targeted and effective treatment plan, improving outcomes for equine patients.
Laminitis:C.S
Sawhosre stance
Acute pain + Lameness
Bounding digital Pulse
Hoof heat
Pain on hoof tester
@ junction of the hoof wall + the sole
Shifting weight
Laminitis:D.X
Exam
Rad
Rotation of the coffin bone
Sinking (Founder)
Venography
Contrast into digital veins to see laminae
Bloodwork
Test for insulin resistance
Laminitis:T.X
Medical Management
NSAIDs
Phenylbutazone
Flunixin meglumine (Banamine)
Vasodilators
Acepomazine(watch out) or isoxsuprine
Cryotherapy
Good for early stage
Insulin Regulation
EMS or PPID: use metformin or pergolide
Mechanical Support
Hoof trimming + Shoeing ( Heart bar or reverse shoes)
Deep bedding
Nutritional Management
Low starch diet
Reduce body weight
Surgery
Deep digital flexor tenotomy
Chronic cases not responding well to traditional treatment: deep digital flexor tendon tenotomy to relieve pull of tendon on coffin bone.
Myositis/Myopathy:C.S
Stiffness + Muscle pain + Weakness
Rapid Muscle Atrophy
Sweating
Reluctance to move: tying up
Fasiculations or tremors
^HR + RR
Myoglobinuria
Dark red/brown urine
Myositis/Myopathy:D.X
Serum Muscle enzymes
^ CK + AST: muscle damage
Urinalysis
Myoglobinuria
Muscle biopsy
For immune mediated or chronic myopathy
Genetic testing
GYS1 gene= PSSM
Selenium + Vitamin E blood levels
For nutritional myopathies
Myositis/Myopathy: T.X
Exertional Rhabdomylosis
Rest + NSAIDs
FLuid therapy
Dietary Management
Low starch High fat
Dantrolene/Methocarbomol: Muscle relaxants
Infection/Immune mediated myositis
Corticosteroids
± Immunomedulatory therapy
Nutritional myopathy
Selenium + Vitamin E supplementation
Generally good prognosis
Disruption of Suspensory Ligament:C.S for Proximal suspensory desmitis
Toes dragging gait
Common in the hindlimbs of dresage
Disruption of Suspensory Ligament:C.S for Suspensory body injury
In forelimbs
Acute to mod/severe lameness
Swelling/heat in mid canon region
Disruption of Suspensory Ligament:C.S for Suspensory Branch injury
Swelling around fetlock
± sesamoid fractures
Disruption of Suspensory Ligament:D.X
Palpation + Flexion tests
U/S:* for assesing suspensory ligament
Rads
MRI
Nerve blcks
Check which ones
Disruption of Suspensory Ligament:T.X
Rest + Controlled Exercise
NSAIDs or steroid injections
Shock wave therapy
PRP or Stem cell
Surgery
Chronic hindlimb PSD w/ fibrotic changes
Neurectomy
Exertional Rhabdomyolysis
Muscle disorder primarily affecting Thoroughbreds, Standardbreds, and other high-strung horses.
It is characterized by episodes of muscle pain and stiffness, especially after exercise.
Abnormal calcium regulation in muscle cells leads to prolonged muscle contraction, resulting in muscle cell damage and rhabdomyolysis. Horses with RER have a defect in intracellular calcium handling, which may be related to a dysfunction in the ryanodine receptor (RyR1), a calcium channel in the sarcoplasmic reticulum of muscle cells.
Clinical Signs: Signs include muscle stiffness, sweating, a reluctance to move, and myoglobinuria (dark-colored urine) following exercise. Elevated serum CK and AST levels are common post-episode.
Diagnosis: Diagnosis is based on clinical signs, exercise intolerance, and muscle biopsies revealing abnormal calcium regulation and muscle fiber damage.
1. Recurrent Exertional Rhabdomyolysis (RER)
Treatment Objectives: The primary goal is to reduce the frequency of muscle stiffness and pain episodes, manage muscle damage, and allow the horse to maintain a comfortable level of physical activity.
Dietary Management:
High-Fat, Low-Starch Diet: Feeding a diet that is low in non-structural carbohydrates (NSCs) and high in fat is crucial. High-fat diets (using sources like rice bran or vegetable oil) provide an alternative energy source, reducing the reliance on glycogen stores in muscles. This minimizes the rapid breakdown of glycogen that contributes to RER episodes.
Electrolyte Balance: Supplementing electrolytes, particularly potassium and sodium, helps support normal muscle function and reduces the risk of muscle cramping. Ensuring that the horse is properly hydrated is equally important.
Exercise Management:
Consistent, Regular Exercise: Horses with RER benefit from a consistent exercise routine that avoids periods of rest followed by sudden intense work. Daily, controlled exercise helps to keep muscle cells functioning optimally and prevent stiffness.
Warm-Up and Cool-Down: A gradual warm-up period before more intense exercise, along with a cool-down after exercise, helps to reduce muscle stiffness and the risk of muscle fiber damage.
Medications:
Dantrolene: This muscle relaxant decreases the release of calcium from the sarcoplasmic reticulum within muscle cells, helping to regulate intracellular calcium and reduce muscle contractions. It can be administered prior to exercise to prevent RER episodes.
Tranquilizers: Low-dose tranquilizers such as acepromazine may be used to reduce anxiety and stress, which are known triggers for RER.
Additional Management Strategies:
Environmental Modifications: Reducing stressors such as changes in routine, travel, or competition schedules can help minimize the frequency of RER episodes
PSSM as a Cause of ER: PSSM is one of the specific causes of exertional myopathy. Horses with PSSM are genetically predisposed to ER, making them more susceptible to episodes of "tying-up," especially after periods of inactivity followed by sudden exercise.
Not All ER is PSSM: While PSSM horses experience exertional myopathy, not all cases of ER are due to PSSM. Other causes of ER can include Recurrent Exertional Rhabdomyolysis (RER), sporadic overexertion, and electrolyte imbalances.
Equine Polysaccharide Storage Myopathy (PSSM) Types 1 and 2:
PSSM is a glycogen storage disorder in horses that comes in two forms: Type 1 and Type 2. Both types cause the abnormal accumulation of glycogen in muscle fibers, leading to exercise intolerance, muscle pain, and stiffness.
PSSM Type 1: This form is caused by a mutation in the GYS1 gene, leading to excessive glycogen synthesis. It is most commonly seen in breeds like Quarter Horses, Draft breeds, Paint Horses, and some Warmbloods.
PSSM Type 2: Unlike Type 1, PSSM Type 2 does not involve the GYS1 mutation. It occurs in a wider range of breeds, including Arabians, Warmbloods, and Thoroughbreds. The exact genetic basis for PSSM Type 2 is currently unclear.
Calcium Regulation:
PSSM Type 1: The excessive glycogen storage seen in PSSM Type 1 can disrupt normal muscle metabolism and contraction. There is some evidence suggesting that calcium regulation within muscle cells may be affected, contributing to muscle pain and stiffness during exercise.
PSSM Type 2: Abnormal calcium regulation within muscle fibers is a more prominent feature in PSSM Type 2. This dysregulation can impair muscle fiber contraction and energy utilization, leading to recurrent episodes of muscle pain, stiffness, and exercise intolerance.
Clinical Signs:
PSSM Type 1: Horses typically exhibit exercise intolerance, muscle stiffness, and pain after light work, especially when dietary management is inadequate. Signs may include sweating, reluctance to move, and muscle tremors. The condition may also result in muscle atrophy over time.
PSSM Type 2: Horses with PSSM Type 2 show similar signs of exercise intolerance, muscle stiffness, and pain after light exercise. Over time, they may develop noticeable muscle atrophy. Episodes can vary in severity and frequency depending on exercise and dietary management.
Diagnosis:
PSSM Type 1: Diagnosed through a genetic test for the GYS1 mutation using a blood or hair sample. If the mutation is present, the horse is confirmed to have PSSM Type 1.
PSSM Type 2: Since PSSM Type 2 does not involve the GYS1 mutation, it is diagnosed through a muscle biopsy. The biopsy reveals abnormal polysaccharide storage and disrupted calcium regulation in the muscle fibers. The presence of amylase-resistant polysaccharides is a characteristic finding.
Treatment Objectives:
For both PSSM Types 1 and 2, treatment focuses on reducing muscle stiffness, preventing recurrent episodes, and improving exercise tolerance.
Dietary Management:
Low-Starch, High-Fat Diet: Both types of PSSM benefit from a diet low in non-structural carbohydrates (NSCs) and high in fat. This reduces glucose fluctuations and abnormal glycogen storage in muscle fibers.
Fat Sources: Include vegetable oil, stabilized rice bran, and commercial high-fat feeds to provide an alternative energy source. This dietary approach helps manage muscle metabolism and reduces the risk of muscle pain.
High-Quality Forage: Providing high-quality hay with minimal grain further reduces starch intake and helps minimize muscle pain and stiffness episodes.
Exercise Management:
Regular, Low-Intensity Exercise: Daily, low-intensity exercise is key for both types of PSSM. Regular exercise helps utilize excess glycogen in the muscles and improves energy metabolism. It is crucial to avoid periods of prolonged rest followed by sudden intense work, which can trigger episodes of muscle pain.
Gradual Increase in Exercise: Slowly increasing the intensity and duration of exercise allows the muscles to adapt, reducing the risk of stiffness and exercise intolerance.
Medications:
For PSSM Type 1 and PSSM Type 2, there are no specific medications that directly treat the disease. However, some horses may benefit from:
Anti-Inflammatory Drugs (NSAIDs): Used during acute episodes to manage pain and reduce inflammation.
Muscle Relaxants: In some cases, muscle relaxants can be used to reduce muscle stiffness and spasms.
Monitoring and Long-Term Management:
Routine Blood Work: Regular monitoring of serum creatine kinase (CK) and aspartate aminotransferase (AST) levels post-exercise is essential for both types. Elevated levels indicate muscle damage, guiding adjustments in dietary and exercise management.
Regular Reassessment: Periodic evaluations by a veterinarian can help assess the horse’s response to management strategies and make necessary adjustments to diet and exercise routines.
Key Differences in Clinical Signs between HYPP, RER and PSSM
Muscle Trembling: A hallmark sign of HYPP that is not typically seen in RER or PSSM.
Prolapse of the Third Eyelid: Unique to HYPP and not observed in RER or PSSM.
Myoglobinuria: More common in RER and severe PSSM episodes, indicating extensive muscle breakdown. It is not a feature of HYPP.
Exercise Intolerance: Present in both PSSM and RER, but RER episodes tend to be more sudden and acute, while PSSM can present with more chronic, subtle signs.
Muscle Atrophy: Seen in PSSM over time due to ongoing muscle damage and fibrosis, but not commonly observed in RER or HYPP.
While there are some overlapping symptoms (such as muscle stiffness and reluctance to move) between RER, PSSM, and HYPP, each condition has hallmark clinical signs that set it apart. Understanding these differences is crucial for veterinarians to accurately diagnose and manage each condition. For example:
RER is characterized by acute muscle pain and stiffness, especially after exercise, often with dark urine.
PSSM presents with chronic exercise intolerance, muscle stiffness, and sometimes muscle atrophy.
HYPP involves muscle tremors, weakness, possible paralysis, and third eyelid prolapse, often triggered by changes in potassium levels.
Fistulous Withers:C.S
Localized swelling + Heat
Pain + sensitive
Fistulous tracts
Reluctance to move
Systemic signs
If infection
Chronic abscessation
If left untreated
Fistulous Withers:D.X
Exam
Rads
U/S
Guided FNA
View extent of fluid
Microbe culture
Nuclear scintigraphy
Fistulous Withers:T.X
ABX
If brucella do rifampin + doxycycline
SX Drainage
Topical + Wound care
Isolation if Brucella
Manage underlying causes
Prevent further trauma
Flexural Deformities (Club foot): Congenital causes
Intrauterine malpositioning
Genetics
Teratogenic influences (ingested while pregnant
Locoweed/Astragulus + Oxy tropis
Sudan grass + Sorghum
Fescue
Lupines

Flexural Deformities (Club foot):C.S
Congenital
Acquired
Stage 1: mild/moderate, heels remain in contact w/groudn but increase angle at fetlock or coffin joint
Stage 2: Severe, heels are raised off ground, bearing weight on toes (clubfoot), altered gait
Flexural Deformities (Club foot): Joint specific clinical signs
Coffin
Walk on toes
Fetlock
If severe, knuckle over, weight bearing on the dorsum of joint
Carpal
Limb flexed position
Flexural Deformities (Club foot):D.X
Exa
Rads
U/S
Calcium + phosphorous levels
Flexural Deformities (Club foot): T.X
Medical Management
Oxytetracycline: Calcium-chelating effects)
Analgesics + Anti-inflammatories
Nutritional management
Controlled diet
Limit excess calories for those w/rapid growth
PT + Exercise
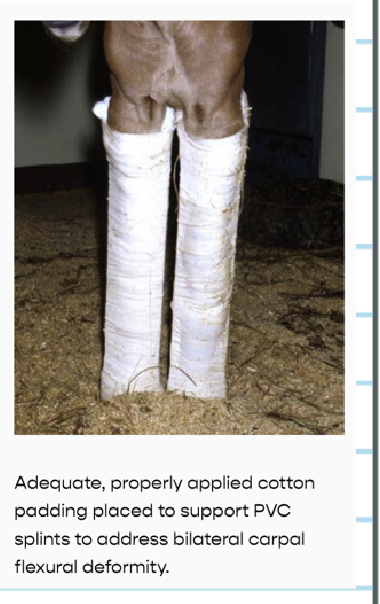
While splints/casts are applied in congenitals
Corrective shoeing
Surgery
Inferior check ligament destomy
Involving coffin joint
Superficial digital flexor tonotomy
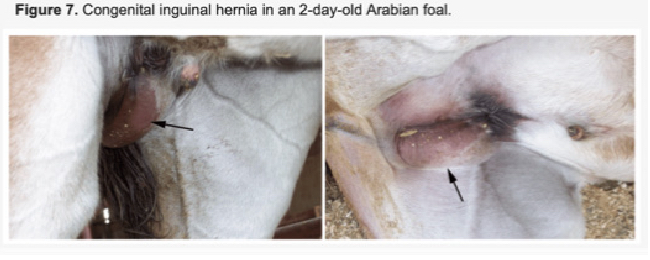
Hernias:C.S
Umbilical
Soft + palpable budge in umbilical region ± reducible
Large: ± entrapment
Inguinal/Scrotal
Swelling in the region
Foals: Reducible
Stallions: colic, pain, ^HR, decrease gut sounds
Diaphragmatic
Respiratory Distress
Exercise intolerance
Colic if abdominal organs become strangluating
Auscultation of muffled heart + lung sounds
Hernias:D.X
Exam
U/S
Rads
Abdominocentesis
Intestinal strangulation: ^TP + Lactate= bowl compromise
Blood work
For systemic causes etc
Hernias:T.X
Umbilical
Small,Reducible (<5cm): Often spontaneously resolve by 6 to 12 months
Larger: SX repair
Strangulated: SX
Inguinal
Foals w/ reducible spontaneously resolve
Stallions: ASAP SX, ± castration
Diaphragmatic
SX but prognosis is guarded
Hoof Imbalance:Types
Medio-Lateral
One side of hoof is higher: stress on coffin + fetlock joints
Dorso-Palmer/Plantar
Heel or toe s too high or low: stress on DDFT + Navicular bone + heel structures
Sheared heels
One heel higher than the other: Lameness+ Pain
Club foot
Heel is excessively high: steep hoof-paster axis
Strain on tendons + ligaments (DDFT)
Broken Hoof-Pastern Axis
Hoof Imbalance:C.S
Lameness
Uneven wear on hoof
Asymmetry in hoof growth
Abnormal stride
Increased digital Pulse
Tendon strain
Hoof Imbalance:D.X
Exam
Hoof tester
Gait analysis
Rads
Thermography + U/S
Hoof Imbalance:T.X
Corrective trimming
Corrective Shoe
Wedge: Dorsopalmer
Lat/medial support(Medio-lat)
Eggbar/Heart-bar: sheered heels or collapsed heels
Rehabilitation + Rest
NSAIDs
Navicular Disease/ Palmer Digital Pain:C.S
intermittent Lameness
Shifting short strided to stabbing gait
Bilateral lameness
Pain on palpation or hoof testing
Over heels or frog= palmer digital pain
Response to flexion test
Exacerbation of lameness following distal limb flexion (Front limb)
Toe-pointing posture
Stiffness or reluctance to turn
Navicular Disease/ Palmer Digital Pain: D.X
Exam
Lameness test + Palmer digital nerve block
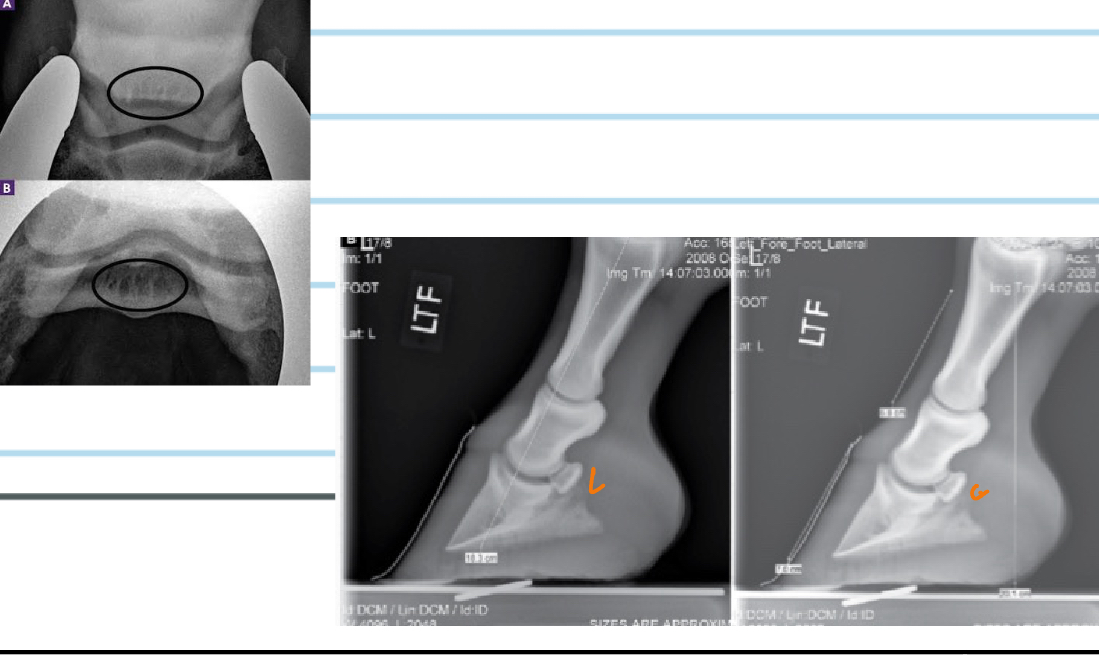
Rads
Increased radiopacity in Navicular bone
Sclerosis
Cyst-like lesions
U/S
Thickening or tearing of DDFT + Suspensory ligament of navicular bone
MRI*
Nuclear scintigraphy
Navicular Disease/ Palmer Digital Pain: T.X
Corrective shoes
Shorten toe, raise heel to decrease pressure
Egg-bar or Heart-bar shoes can provide additional support
Pharmacological Management
NSAIDs
Biphosphonate
Tiludronate, clodronate: inhibit bone resorption
Corticosteroid injections
Intra bursal
Biologic Therapies
Surgery
Palmer digital neurectomy
Bursoscopy
Nonseptic Synovitis/Bursitis: C.S
Non-septic
Swelling + Lame
Pain on palpation
± Thick/hard bursal wall
Septic
Severe swelling
Lame
Systemic signs
Purulent or sanguinous discharge
Pain
Nonseptic Synovitis/Bursitis:D.X
Exam+Imaging
Synovial Fluid Analysis
Nonseptic: Clear, mild leukocytosis
Septic: Leukocytosis, turbid fluid
Nonseptic Synovitis/Bursitis: T.X
Non-septic
Rest + Cold therapy
NSADs + Drainage
Steroid injection if SX is refractory
Septic
Systemic ABX
Bursal Lavage
SX Debridement
Pain management
Wound Care
Septic Tenosynosynovitis:C.S
Lameness + Swelling + Fever
Heat + Pain
Reduced range of motion
Septic Tenosynosynovitis:D.X
Exam
U/S*
Rads
Arthrocentesis
Septic Tenosynosynovitis: T.X
Medica
ABX: Penicillin, Gentamicin, Ceftiofur
NSAIDs
Surgical
Drainage
Tenoscopic debridement
Supportive care
Subsolar Abscess:C.S
Acute onset of severe lameness
Sensitivity to hoof testers
Heat in the hoof + Bounding digital pulse
Drainage+ Swelling above coronary band
Subsolar Abscess:D.X
Exam
Rads
To rule out coffin bone fractures
U/S
Nerve block
Palmer digital nerve block confirms te source of pain is the hoof
Subsolar Abscess:T.X
Drainage
Soak hoof w/ epsom 2-3 times per day for 10-20min
Poulticing then wrap foot
If infection spread beyond hoof
Systemic ABX
Pain Management: NSAIDs
Hoof care + Protection
What is a Temporohyoid osteopathy
Progressive debilitating dz of the middle ear, temporahyoid joint
Results in fusion of the joint
Osteoarthritis
Boney proliferation
Fractures
CnVII + CnVIII deficits
Temporohyoid osteopathy:C.S
Neurology
Facial nerve paralysis
Vestibular Dysfunction
Hearing Loss
MSK
Dysphagia
Painful chewing or swallowing
Head shake/Ear rub
Temporohyoid osteopathy:D.X
Neuro Exam
Palpate hyoid apparatus
Imaging
BAER
Temporohyoid osteopathy:T.X
Medical
NSAIDs, ABX if strep or staph ear infection
Corneal ulcer management (Facial Paralysis)
T.X
Ceratohyoidectomy*
Fracture repair
Supportive Care
Tendon/Ligament Rupture
Thrush:C.S
Foul odor
Black Discharge: Dark necrotic material in central sulcus of the frog
Lameness
Swelling
Around frog + Heel bulbs
Sensitivity to touch
Thrush:D.X
Exam
Visually seeing discharge + palpate for swelling
Hoof Tests
Microbial Culture if necessary
Fusobacterium necrophorum is the most frequently identified bacteria associated with the disease
Thrush:T.X
Thorough hoof cleaning
Antiseptic Application
Mechanical Debridement of necrotic tissue
Koppertox or Copper Sulfate
White Line
Affects the white line of the hoof
Separation of the hoof wall from the sole
Cause by bacteria, fungi or yeast
Crumbly powdery chalking appearance
± Lameness
Tx: Remove damaged/infected portion of hoof wall
Antiseptic/Antifungal
Gait Abnormalities as Indicators of Musculoskeletal Disease
Changes in a horse’s gait are often the first sign of musculoskeletal problems.
1. Lameness
Description:
Lameness is a common sign of musculoskeletal issues.
It often presents as an irregular gait
Associated Diseases:
Navicular disease,
Osteoarthritis,
Tendon injuries,
Laminitis,
Fractures.
Assessment:
Graded on scales like the AAEP lameness scale (0 to 5).
Helps localize the source of pain.
2. Short-Strided Gait
Description:
A shortened stride often indicates discomfort or pain.
Horses with a "short-strided" gait appear stiff and reluctant to move freely.
Associated Diseases:
Navicular syndrome,
Tendonitis,
Degenerative joint diseases.
Key Observations: The stride may be reduced symmetrically (e.g., laminitis) or asymmetrically (e.g., unilateral lameness).
3. Stumbling or Tripping
Description: Frequent stumbling can indicate weakness, pain, or neurological deficits. A horse that trips or knuckles over at the fetlock may be experiencing muscle fatigue, tendon injury, or proprioceptive deficits.
Associated Diseases: Navicular disease, tendon injuries, cervical vertebral malformations (wobbler syndrome).
Key Observations: Look for repeated stumbling, dragging of the toes, or failure to properly lift the limbs.
4. Dragging Toes
Description: Toe dragging is often seen in horses with hindlimb lameness or back pain. It may also occur in neurological conditions like equine protozoal myeloencephalitis (EPM).
Associated Diseases: Sacroiliac disease, EPM, laminitis (especially in the acute stage), osteoarthritis.
Key Observations: During a walk or trot, one or both hind toes may visibly scuff the ground, resulting in abnormal hoof wear.
5. Pacing or ‘Crabwalking’
Description: Pacing or crabwalking occurs when a horse moves sideways or shifts its body weight abnormally while walking, often indicating pain in the back, hips, or hindlimbs.
Associated Diseases: Sacroiliac joint dysfunction, hip dysplasia, severe hindlimb lameness.
Key Observations: The horse shifts its body to relieve pressure on the affected limb(s), leading to a characteristic sideways or "crabbing" movement.
Postural Abnormalities as Clinical Signs
How a horse stands can be just as telling as how it moves. These postures often point to specific conditions:
1. Pointing of the Forelimb
Description: Horses with forelimb pain may point the affected limb forward to relieve pressure on the hoof or lower limb.
Associated Diseases: Navicular disease, laminitis, foot abscesses.
Key Observations: Chronic cases may involve frequent weight-shifting or a constant pointing of the same limb.
2. Reluctance to Bear Weight (Lifting Limbs)
Description: In cases of severe limb pain, horses may intermittently or constantly lift the affected limb.
Associated Diseases: Acute laminitis, fractures, severe tendon injuries.
Key Observations: Horses with severe laminitis may adopt a "sawhorse" stance, where they lean back onto their hind legs to relieve forelimb pressure.
3. Cross-Legged Stance (Base-Narrow Stance)
Description: A base-narrow stance, where the horse places its feet closer together than normal, can signal discomfort in the shoulders, hips, or back.
Associated Diseases: Cervical vertebral stenotic myelopathy (wobbler syndrome), musculoskeletal pain, back pain.
Key Observations: The horse may appear unsteady or awkward, particularly when shifting weight.
4. Camped-Out or Camped-Under Posture
Description: "Camped-out" refers to extending limbs forward or backward, while "camped-under" involves pulling the limbs underneath the body.
Associated Diseases: Laminitis (camped-out), severe abdominal pain (colic), neurological conditions.
Key Observations: Horses with laminitis stand with their forelimbs camped-out to reduce weight on the front feet. Horses with back pain may adopt a camped-under stance.
5. Sawhorse Stance
Description: In a "sawhorse" stance, the horse stands with front legs extended forward and hind legs backward. This is an attempt to relieve pain in the forelimbs.
Associated Diseases: Acute laminitis, tetanus.
Key Observations: The horse may appear stiff and reluctant to move, often rocking back onto its heels.
6. Knuckling
Description: Knuckling involves abnormal flexion of the fetlock joint, where the horse "knuckles over" at the fetlock, partially folding the pastern and hoof under.
Associated Diseases: Neurological disorders (e.g., EPM), tendon injuries, muscle fatigue.
Key Observations: Knuckling may be accompanied by stumbling or toe dragging, worsening with exercise or fatigue.
7. Toe-Up Posture
Description: This posture involves flexing the fetlock joint while raising the toe off the ground, reflecting discomfort in the hoof or limb.
Associated Diseases: Laminitis (chronic), deep digital flexor tendon injury, navicular syndrome.
Key Observations: The horse may frequently shift weight, standing with the heel in contact while lifting the toe.